










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.50 n.2 Pretoria Aug. 2020
http://dx.doi.org/10.17159/2310-3833/2020/vol50no2a7
ARTICLES
Return to Work for People with Hand Injuries in South Africa: Occupational Therapy Strategies
Michelle Elizabeth UysI; Helen BuchananII; Lana van NiekerkIII
IB.OT (SU); M.OT (US). https://orcid.org/0000-0003-2565-9402; Occupational Therapist in private practice, Up & Go Occupational Therapists, Stellenbosch
IIBSc OT (UCT); MSc (UCT); PhD (UCT). https://orcid.org/0000-0001-5540-9928; Associate Professor, Division of Occupational Therapy, Department of Health & Rehabilitation Sciences, University of Cape Town
IIIB.OT (UFS); M. OT (UFS); PhD (UCT). https://orcid.org/0000-0003-0003-6006; Associate Professor, Division of Occupational Therapy, Department of Health & Rehabilitation Sciences, Stellenbosch University
ABSTRACT
INTRODUCTION: The socio-economic burden of a hand injury in South Africa is substantial, particularly for manual labourers whose job tasks are physically demanding and require hand function. Barriers to participation in work occur on an economic, social and political level, as well as on a therapist and client-specific level
AIM: This study aimed to identify the strategies and barriers encountered by occupational therapists in work-related transitions after a serious hand injury
METHODS: A descriptive cross-sectional design was utilised. A questionnaire was developed for the study through a rigorous development process that included piloting. The final instrument was disseminated as an online questionnaire to occupational therapists working within the field of return-to-work and hand injuries. As no data were available on the number of occupational therapists working within this field, convenience sampling was used with snowballing as a strategy to increase the number of possible respondents. Data were exported into Microsoft Excel and descriptive analyses were conducted
RESULTS: Forty three occupational therapists completed the questionnaire. Respondents mostly focused on treating components of function (100%), addressing activities of daily living (97.67%) and issuing home programmes (97.67%) as direct intervention strategies to facilitate work-related transitions. One of the least used strategies was issuing assistive devices for work (30.23%). The least used work-specific strategies included conducting worksite visits, observing clients (or proxies) completing work tasks in the workplace and implementing work trials. Financial support and compensation were viewed as both an asset and a barrier
CONCLUSION: Without knowledge about the representability of the study sample, the results of this study cannot be generalised. However, the therapists who responded to the questionnaire were offering a range of strategies to address work-related transitions for people with serious hand injuries, despite the numerous barriers that exist
Key words: Upper extremity, Vocational Rehabilitation, Work-related transitions
INTRODUCTION AND BACKGROUND
Injuries to the hand account for a substantial number of injuries globally. For example, more than a decade ago, Sorock et al1 reported that one million workers in the United States of America sustained hand injuries annually and a more recent study found that an estimated total of 3,468,996 upper extremity injuries occur every year across the USA2. This translates to an incidence of 1,130 upper extremity injuries per 100,000 persons per year. Canadian statistics have shown that 28% of 630,000 work-related injuries in 2003 were to the hand3, while one-fifth of cases presenting to European emergency departments were hand injuries4. While there are no accurate prevalence statistics for hand injuries in South Africa, taking the high levels of violence and road traffic accidents5 into account, we suspect they are likely to be more prevalent than in Europe and North America.
Occupational therapists play an important role in providing therapy and vocational rehabilitation to people with hand injuries. Substantial evidence for the benefits of vocational rehabilitation has been produced in the United Kingdom6. In Norway, the most effective vocational rehabilitation strategy was found to be prompt placement of clients back into work7, while an Australian study reported case management and personal counselling as the most important and most-used skills within vocational rehabilitation8. Although the reported frequency of actual and ideal use of strategies has been shown to differ9, there is a tendency for strategies used with the same frequency to overlap across all types of work-related interventions9.
Occupational therapists use a variety of strategies to facilitate work-related transitions. The range of these strategies have been explored in detail in a scoping review which is currently under review, and for which a published protocol is available10. The strategies reported in the scoping review originated from studies undertaken in high and upper-middle income countries and focused mainly on taking the prognostic factors related to successful work-related transitions into account during the transition to work process. The limited research evidence on the strategies used by occupational therapists and their frequency of use internationally, and more specifically in South Africa, pointed to the need for the current study. Of the few studies that have investigated these strategies, psychological support11 particularly for traumatic hand injuries12, the involvement of occupational therapists in the communication of the work-related transition process with the employer and employee13 and making recommendations for alternative work tasks14 were featured.
Factors impacting on work-related transitions may be an asset for some and a barrier to others. A Swedish study determined that factors related to work-related transitions and general work motivations could be grouped into three categories: individual factors, factors related to the work environment and rehabilitation factors15. A more recent study achieved consensus on 1 3 assets for work-related transitions following non-traumatic upper extremity surgery16. The assets identified were: motivation to return to work; self-efficacy for return to work and recovery; availability of alternative duties; flexible return to work arrangements; positive coping skills; limited heavy work job tasks; supportive return to work policies; supportive management; absence of catastrophic thinking; absence of fear avoidance to return to work; absence of fear avoidance to pain/activities; return to meaningful work duties and high job satisfaction16.
Barriers confronted by occupational therapists in addressing work-related transitions occur at an economic, social and political level, as well as on a therapist- and client-specific level9. An Australian study found that the barriers to ideal practice in conducting work-related assessments related to occupational therapists working in isolation, and lacking training and experience9. Client-specific barriers included a lack of motivation to return to work and clients who do not speak English as a first language. The most prominent work barriers were lack of consistency in the workplace, the work environment and the employer's attitude9. External barriers included industrial issues, delayed referrals and legislative problems among others.
Understanding the context is crucial in justifying the need for, and significance of, this study. The extremely high unemployment rate in South Africa (29.1% in 2019)17, along with the substantial income inequalities that have affected the skills level of informal workers18, make the return to work process extremely challenging. Taking into account the substantial socio-economic burden of hand injuries in South Africa to individuals, families, employers and the State, identifying evidence-based interventions for successful work-related transitions is vital in contributing to reducing our unemployment rate. Low- and middle-income countries such as South Africa, have large numbers of informal workers and are strongly reliant on manual labour. Considering that manual labour requires strong and dextrous hand function, sustaining a hand injury typically requires medical intervention and rehabilitation which impacts on the person's capacity to work19. The high prevalence of unemployment within South Africa has been shown to adversely impact unskilled workers' rehabilitation as they can easily be replaced20.
Adding complexity to this picture is the lack of occupational therapists employed within the Department of Labour in South Africa which impacts on the services and resources available for addressing the final stages of rehabilitation which specifically focus on work-related transitions20. The majority of South Africans are reliant on the public sector for healthcare as they do not have healthcare insurance21. In contrast, people in higher income brackets can afford healthcare insurance and can thus access treatment in the private healthcare sector 21 which has better human resourcing, despite more people being dependent on the public sector for healthcare22. Levesque et al's23 conceptual framework provides a way of understanding the barriers many South Africans face in accessing healthcare, which includes rehabilitation. This patient-centred framework outlines five dimensions of accessibility namely, approachability, acceptability, availability, accommodation, affordability and appropriateness22. These dimensions encapsulate aspects such as financial accessibility, physical accessibility, time and resource availability22. Transport costs, travelling distances and the type of transport available are common barriers South Africans face in accessing healthcare18. Considering these contextual realities, it is of critical importance that occupational therapy interventions directed at work-related transitions are based on the best available evidence in order to make the best use of scarce resources and to achieve the best possible outcomes.
The current study was nested within a larger three-year study that explored the successful transition of people with serious hand injuries to work. This study, conducted in the second year of the larger study, followed a mixed methods approach that occurred in two-phases. The quantitative (first) phase aimed to identify the strategies occupational therapists in South Africa were using to facilitate work-related transitions for people with serious hand injuries, and to determine the barriers encountered. Obtaining this information would be useful in contributing to the development of best practice guidelines aimed at improving the occupational therapy services offered to this group of people. The qualitative (second) phase aimed to understand the strategies occupational therapists were using for this group of people from the perspective of occupational therapists and their clients. Earlier data collection sessions, prior to this phase of the study, were used as a foundation from which to develop this phase of the study. For the purposes of this study, the work-related transitional process started in the acute phase, moved through a rehabilitative phase and then to a return-to-work phase in which occupational therapists used specific work-related strategies. Therefore, the questionnaire that was developed was categorised accordingly. The questionnaire was divided broadly into direct occupational therapy treatment strategies, indirect occupational therapy treatment strategies, the provision of emotional support, specific work-related strategies and suggestions, as well as possible assets and barriers to work-related transitions.
The study had three objectives:
1. To establish which interventions occupational therapists used in each of the four categories: direct occupational therapy services, indirect occupational therapy services, work-related interventions, and return to work as a component of work-related services.
2. To determine the frequency of use of the various strategies.
3. To determine the assets and barriers influencing work-related transitions.
METHODS
The STROBE guidelines24 have been used to report this study.
Study Design
A descriptive cross-sectional research design was utilised. This particular design was appropriate to obtain descriptive data from occupational therapists in all healthcare facilities that described the work-related transition strategies they were using, and to draw comparisons between the different strategies24. Cross-sectional questionnaires are also useful to measure the frequency that various work-related transitional strategies are used25 and to determine the variety of barriers encountered by study participants.
Population and sampling
The population comprised all occupational therapists in South Africa working within the field of hand/upper limb rehabilitation and vocational rehabilitation or work practice. As no data were available on the number of occupational therapists working within this field, non- convenience sampling with snowballing was used to include as many occupational therapists as possible.
Instrumentation
A questionnaire was developed, and pilot tested prior to finalisation.
Questionnaire development
The items in the questionnaire were developed from two sources. Firstly, as part of a scoping review, a thematic analysis was conducted to identify the different types of strategies used by occupational therapists to facilitate work-related transitions for clients with hand injuries10. Questions were formulated from the codes that made up the theme "strategies that occupational therapists use to enable work-related transitions" in the scoping review. Secondly, an inductive analysis was undertaken of interview transcripts from an overarching study conducted in 2017 that explored South African occupational therapy practice related to work transitions after serious hand injury10. Codes were identified on the strategies the therapists used and questions were formulated from these codes. The questionnaire comprised two sections namely, work-related transition strategies used by occupational therapists, and demographic information (see Table 1, page 55). Within the section on work-related transition strategies, questions were grouped according to the client's stage of recovery (e.g. acute, rehabilitative and return-to-work phases) and sub-divided into: direct occupational therapy treatment strategies, indirect occupational therapy treatment strategies, provision of emotional support, specific work-related strategies, and assets and barriers to work-related transitions.
The questionnaire made use of a combination of ordinal scales and text boxes. A four-point rating scale was chosen for most questions (43 of 67) as it is known to enhance validity and reliability when measuring individuals' opinions26. Four-point rating scales are also beneficial as the repetitive style of asking the questions has been found to improve the response rate27. The text boxes contextualised the responses or contributed new considerations to the existing questionnaire. Questions with four-point rating scales were supplemented with a textbox to provide an opportunity for additional descriptive information to the frequency of strategies used to facilitate work-related transitions, which is widely regarded as complex. The questionnaire was refined during the pilot testing phase after which it was finalised.
Testing validity and utility
Face validity, content validity and specific aspects of clinical utility of the questionnaire were investigated through a piloting process.
Pilot sample: Three occupational therapists employed at three different academic institutions across the country and with a clinical background of at least five years in the field were invited to participate. These participants were chosen so as not to involve any potential respondents for the main study in this pilot phase and to obtain diverse input on the clarity and relevance of the questionnaire to the research question. Experts within the field of work-related transitions or hand injuries were involved in this process to increase the likelihood of obtaining reliable and accurate responses28.
Procedure: The three participants were recruited via email or telephonically. On agreeing to participate, each participant was emailed the questionnaire which they completed in their own time.
After receiving the completed questionnaires, responses were checked for consistency by looking for logical patterns. The first author arranged individual face-to-face or Skype meetings with each participant to systematically critique the clarity of each question. Content validity was evaluated by appraising the comprehensiveness of the questionnaire and checking that the questions represented all characteristics the authors intended to measure 29. Participants also determined whether any questions could be removed, added or reformulated, without compromising content validity30.
For clinical utility, the clarity of instructions, formatting of questions and response options, completion time interpretation of questions and clinically relevant31 were evaluated with the same three occupational therapists. Clinical relevance related to the appropriateness of the strategies for occupational therapy practice in South Africa and the likely barriers that would be encountered. Participants also commented on the conciseness and comprehensiveness of the questionnaire.
Feedback from the pilot study participants was tabulated and systematically discussed item by item. Where the feedback improved clarity, changes were made. Revisions included changing or removing words for clarity, adding a definition of case management, expanding a question to include synonyms (for example, components of function and performance skills), dividing concepts such as activities of daily living into instrumental and basic activities of daily living, providing examples for some items and adding text boxes to capture additional comments. The response options were initially in most cases, hardly ever and never. After the pilot study improvements were made. One pilot participant recommended adding a further response option to make the three-point rating scale a four-point rating scale.
The final Questionnaire
The final questionnaire consisted of two sections (details shown in Table 1, page 55) and contained an information page, consent form and inclusion criteria.
Data Collection Method
The questionnaire was developed as an online survey as the most economical way of ensuring that participants from across the country could participate in the study. Additional benefits included the flexible formatting of the questionnaire (which permitted questions that were not relevant to the respondent to remain hidden), being able to limit the number of questions on each page, allowing respondents to answer the questions at their convenience and ease of sharing the link with colleagues. The questionnaire could only be completed if the respondent met the self-selected inclusion criteria.
The electronic platform, SUrveys.sun.ac.za, was used to conduct the online questionnaire. A link to the questionnaire was distributed to the entire population of occupational therapists to recruit as many respondents as possible. The questionnaire was shared through the Occupational Therapy Association of South Africa (OTASA) and the Metropole Occupational Therapists in Health (MOTH) group mailing distribution lists. The link was also posted on social media platforms, namely LinkedIn and relevant Facebook groups (Occupational Therapy, University of Cape Town, OT Comserv 2017, ST's, PT's, OT's, DT's and Audio's!, Maties se beste OTs and 2017 Community Service Allied Health Professionals) between 27 May 2019 and 5 August 2019 and was shared with occupational therapists known to the first author for further distribution. Therapists who received the invitation to participate in the study were required to determine their eligibility by self-selecting options from the inclusion criteria. The eligibility questions asked if the participant was practicing as an occupational therapist in South Africa and if they were working in the field of upper limb and vocational rehabilitation. The questionnaire was designed to only proceed if both inclusion criteria were met. The questionnaire was available for ten weeks and 4 days (25 May 2019 to 6 August 2019). Reminders were sent via a mailing list on three occasions (llJuly 2019, 24 July 2019 and 5 August 2019).
Data management and analysis
Data from completed questionnaires were exported from SUsur-veys into Microsoft Excel for analysis. As the data were not normally distributed, medians and ranges were determined for numerical variables. Descriptive statistics were used to calculate frequencies and percentages for the different strategies used to facilitate work-related transitions. No additional analyses were conducted as the aim of the study was to describe current practice.
Ethics
The Human Research Ethics Committee of the University of Stellenbosch (HREC reference number: SI8/05/098) and the University of Cape Town (HREC reference number: 537/2018) granted permission for this study. This work is based on the research supported wholly by the National Research Foundation of South Africa (GRANT NUMBER: TTK160525166179).
The identity of research participants was anonymous as no personal information was required.
RESULTS
The SUsurvey platform showed 762 incomplete responses where the respondent either did not complete the questionnaire fully or only realised while completing it that it was not relevant to them. Forty-three occupational therapists met the inclusion criteria and completed the questionnaire. Respondent profiles are presented first, after which the results are presented according to the sections in the questionnaire, namely: direct occupational therapy treatment, indirect occupational therapy intervention, provision of emotional support, specific work-related strategies, and assets and barriers in work-related transitions.
Respondent profile
Table II presents the respondents' biographical and context-specific data. The respondents worked predominantly in the private sector, and in urban areas in Gauteng or the Western Cape. Although they were relatively experienced (median of 10 years) occupational therapists, they were less experienced in facilitating work-related transitions (median of 4 years). Slightly more than half (53.5%) did not have a postgraduate qualification in hand - or vocational rehabilitation. Of all respondents, 67.8% saw fewer than ten clients (range: 2 - 200 clients) with serious hand injuries who required assistance with a work-related transition per month.
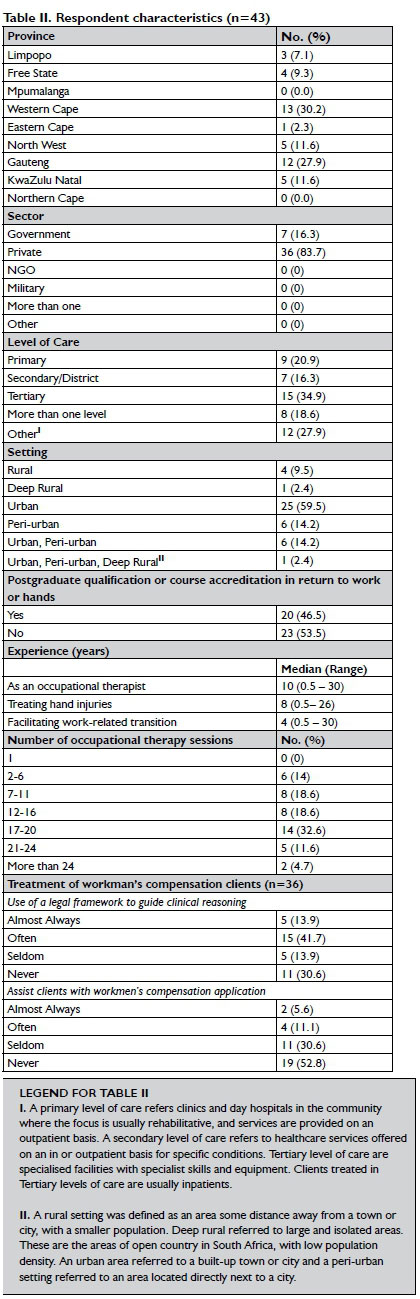
A high percentage (83.7%) of respondents treated workman's compensation clients. A legal framework was almost always used by most of the respondents (83.7%). A few respondents almost always assisted with the workman's compensation application (16.7%). Of the seven respondents working in the government sector, only two (North West and Gauteng) saw workman's compensation clients.
Occupational Therapy Strategies Direct Occupational Therapy Treatment
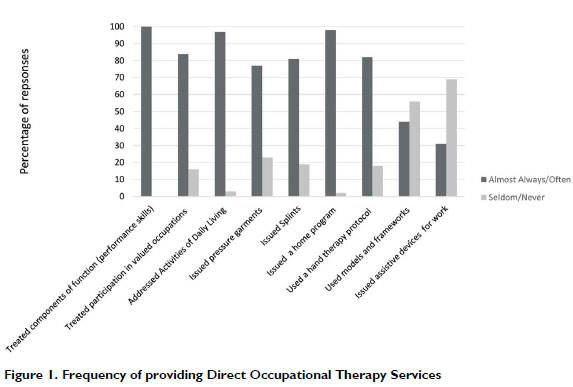
Respondents indicated how often they had used various techniques as part of a return to work protocol (refer to Figure 1 on page 57). The least used technique was issuing assistive devices for work while all respondents addressed components of function. Addressing activities of daily living and issuing clients with a home program were almost always used (by > 90%) to facilitate work-related transitions. Respondents primarily used the International Classification of Functioning (ICF) framework for clients in the acute phase of treatment and the Person, Environment and Occupation (PEO) model for those in the chronic phase. The chronic phase is generally defined as a phase starting three months after the day of the hand injury, in which the symptoms of the hand injury including the person's ability to work, are still persisting. Other models used included the Model of Human Occupation, the Model of Creative Ability, Affolter Approach and the Biopsychosocial Model.
Indirect Occupational Therapy
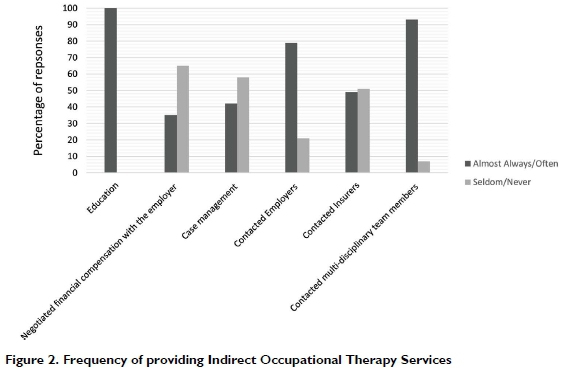
With regard to indirect occupational therapy services, every respondent provided education and almost all contacted medical and rehabilitation professionals (93.0%) (see Figure 2). The respondents also contacted their clients' employers (79.1%).
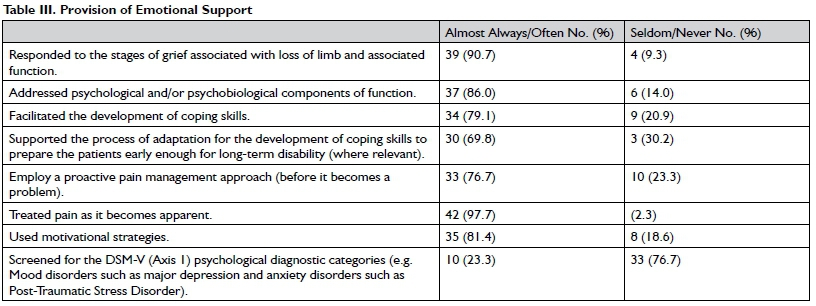
Provision of emotional support
The respondents identified how often they provided emotional support in a variety of ways (see Figure 3). Responding to their client's stage of grief (91.7%) and considering psychological and psychobiological components of function (86.0%) were almost always included in the provision of emotional support. Additionally, they used motivational interventions (81.40%) and coping strategy interventions (79.1%). The types of motivational interventions used included: identifying external and internal motivators; positive reinforcement and feedback; goal setting; measuring progress numerically with photographs and videos; re-education; motivational interviewing; the use of meaningful activities; planning a routine; choosing motivators according to a client's priorities and interests; applying principles of Vona du Toit's Level of Creative Ability; participation in fun leisure activities that require similar function as the clients work and making clients aware of their capability and feeling of accomplishment; Cognitive Behavioural Therapy (CBT); using activities with a time component to put a numerical value to progress, projects with an end-product and goals that incorporate strengthening to be able to return to a favourite activity.
Pain was largely treated proactively before it became a problem (76.7%) or treated as it became apparent (81.40%). Screening for the Diagnostic and Statistical Manual of Mental Disorders (DSM-V)32. Axis 1 psychological diagnostic categories (e.g. Mood disorders, such as major depression, and anxiety disorders, such as Post-Traumatic Stress Disorder) was seldom considered (76.7%). Respondents indicated that they would use tests such as the Progressive Goal Attainment Program, the Depression, Anxiety Stress Scale (DASS) and the Beck's Depression Inventory Test to screen for psychological diagnostic categories. Table III (page 59) refers to the respondents' provision of emotional support.
Specific work-related strategies
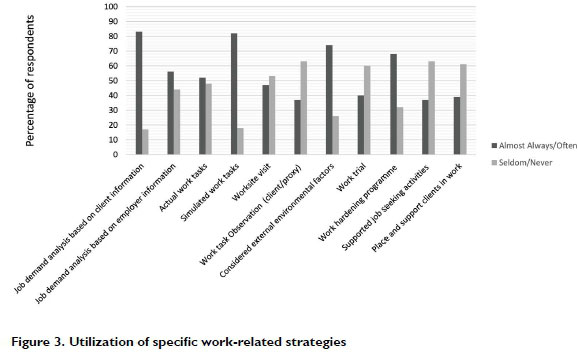
The respondents often obtained a job demand analysis based on information provided by the client (83.7%) and from the employer (55.8%). Of the respondents, 53.5% seldomly conducted worksite visits, 48.8% seldomly used actual work tasks and 62.8% seldomly observed a client (or proxy) completing actual work tasks. See Figure 4 for the frequency of specific work-related strategies used.
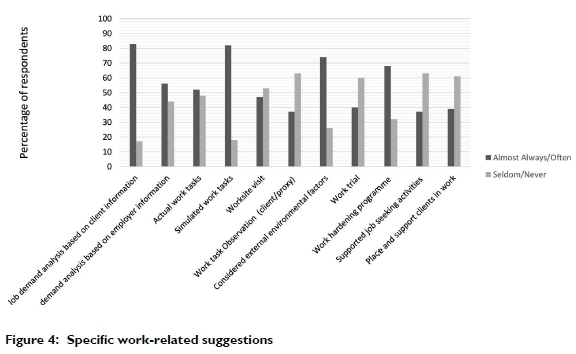
Work-related suggestions
This item requested respondents to indicate how often they were making recommendations for specific work-related strategies, such as workplace accommodations, light duty and an early return to work. The occupational therapists almost always recommended: a graded return to work (88.4%), return to work as soon as the client is medically and functionally able (88.4%) and workplace accommodations to the client (81.4%). Workplace accommodations were less often suggested to the employer (67.4%). Additional suggestions included ergonomic education and discussions with various stakeholders including the client's colleagues and employer. Four respondents explicitly noted that they would suggest job modifications or workplace accommodation and not "light duty" (see Figure 4).
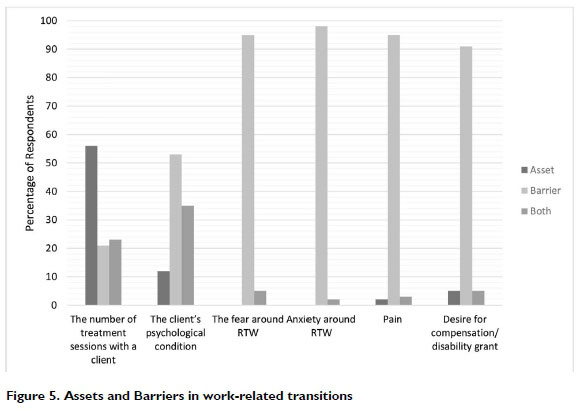
Assets and Barriers in Work-Related Transitions
Anxiety relating to return to work (97.7%), pain (95.35%), fear about returning to work (95.35%) and desire for compensation (90.7%) were the most frequent barriers identified. The number of treatment sessions with a client (55.8%) was indicated as the most common asset for work-related transitions. Figure 5 depicts the assets and barriers that respondents identified in work-related transitions. With regard to additional assets and barriers for work-related transitions in their settings, respondents identified more barriers than assets. Barriers included financial constraints, access to healthcare due to distance, the client's attitude and insight and work specific constraints. Work specific constraints included aspects such as the employer's willingness to assist, an employer's refusal to consider a graded return to work program, the type of work contract that the client had and the client's work history. One respondent commented that personal protective equipment was a challenge in many industries as the job may require wearing gloves, which may not be possible for a client with finger amputations. Furthermore, the same respondent explained that "light duty" is not feasible in specific industries due to the risks involved.
DISCUSSION
This study aimed to establish the strategies used by occupational therapists, and the assets and barriers they experienced in facilitating work-related transitions for people with serious hand injuries. The respondents in this study drew on a variety of interventions depending on the setting in which they worked and appeared to be fulfilling a central role in facilitating the successful reintegration of people with hand injuries into the work environment.
Direct occupational therapy services
Respondents mostly focused on treating components of function, addressing activities of daily living and issuing home programmes as direct strategies to facilitate work-related transitions. This focus is well established with the underpinning rationale that hand injuries that limit engagement in activities of daily living such as work, require rehabilitation to restore functional components or to make adaptations where function cannot be restored30. Studies have indicated that focusing on aspects of hand therapy, such as range of motion, are essential for a successful work-related transition13. As adaptations occur over a long duration, they require the integration of both physical and psychosocial components30. One of the least used interventions was issuing assistive devices for work. This may be because assistive devices (which include assistive technology in the workplace), have been found to be an expensive option for some people and may lead to feelings of isolation33.
Indirect occupational therapy services
The fact that all respondents provided education is supported by evidence since it has been established that informing clients of their diagnosis, precautions and adequately preparing them for what to expect in the return to work process contributes to successful work-related transitions30. This is supported by another study in which occupational therapists were reported to often discuss these aspects with their clients during a consultation or to provide their clients with educational handouts as a method to improve compliance13.
Provision of emotional support
Pain complicates functional outcomes in the short and long-term33. It is therefore noteworthy that most respondents in this study treated pain proactively and seldom addressed pain only as it became apparent. It is also well-documented that psychiatric comorbidities and psychosocial factors are of paramount importance for clients with pain and traumatic hand injuries33. People with serious hand injuries require worker role adaptations recommended by an occupational therapist to consider psychological factors in addition to workplace modifications and traditional biomechanical approaches34. Our study is supported by a previous study35 as most respondents in this study seldomly screened for DSM-V (Axis 1) psychological diagnostic categories with their hand injured clients. Despite this, respondents focused on their client's stages of grief associated with the loss of hand and limb function, addressed psychological and psychobiological components of function and facilitated the development of coping skills. This emphasis is supported by an American study that suggested that using psychosocial perceptions may assist occupational therapists to identify counterproductive factors that could negatively impact on their client's rehabilitation outcomes36.
Return to work as a component of work-related services The least used work-specific strategies were conducting a worksite visit, observing a client (or proxy) completing work tasks in the workplace and implementing a work trial. This could be related to cost implications and time-constraints; however, this will need further investigation. It would also be useful to determine the barriers to worksite visits to better understand how they could be addressed in future research. A noteworthy factor to consider is the reported negative perceptions of employers in South Africa towards healthcare workers. This may be due to a lack of understanding of what occupational therapists are able to contribute to productive work function19, an aspect that needs to be addressed in order to build collaboration between employers and therapists in negotiating work-related transitions.
Assets and Barriers
While we did not categorise the barriers identified in the current study by sector of work, it is likely that occupational therapists treating workmen's compensation clients in the private sector may experience similar barriers to those found in the government sector, such as the distance clients have to travel to receive occupational therapy and the cost implications to access occupational therapy among other economic and social challenges18. In addition to the direct costs incurred by clients, there are various indirect costs which may include a reduction in wages, time away from the workplace, transport costs to attend healthcare appointments and costs to the employer37.
For clients who are breadwinners, the indirect costs to their family and community are extensive. In a study conducted in a tertiary hospital in South Africa, 85% of the hand injury clients interviewed earned less than 600US$ monthly (between Rl,000 and R9,000 per month), despite being the breadwinners of their family38. It is likely that a breadwinner in South Africa who is earning minimum or close to minimum wage, will experience significant financial stress if they are unable to work for any length of time, which highlights the need for further studies to understand the value of financial compensation for breadwinners who have been injured. Financial support and compensation were viewed as both an asset and a barrier. It is important to note that although occupational therapists identified a client's desire to obtain a disability grant as a barrier to their intervention, many South Africans are dependent on grants to survive and to access healthcare21. Therefore, these clients need financial support to attend occupational therapy and to alleviate the financial pressure of not being able to work. However, given the high rates of unemployment and the competitive labour market in the country, some people with hand injuries may want to receive compensation to ease their financial burden, which may affect their motivation and compliance with occupational therapy treatment. There may also be barriers linked to personal expectations. For example, a South African study found that in some communities an injured person's motivation to regain functional independence was affected by an expectation that they should be cared for21.
Strengths and Limitations to the Study
A thorough procedure was used to develop the questionnaire with inclusion of expert-driven pilot testing to assess face and content validity. The questionnaire was only available electronically which may have prevented some therapists from participating. The number of questionnaire responses is a limitation to the generalisability of the study, with some provinces not being represented at all. As we did not have information about the number of occupational therapists in the population, the results cannot be generalised nationally. Furthermore, as the respondents primarily worked in the private sector and much of the treatment they provided related to workmen's compensation, the findings cannot be generalised across the public and private healthcare sectors. This study aimed to identify the interventions that were being used; it did not attempt to explore the evidence to support these interventions. Therefore, it may be useful to conduct a systematic review to evaluate the quality of evidence to support the work-related transitional interventions that are being used for people with hand injuries. The questionnaire used a four-point rating scale which is known to produce results that are clustered around extremes; this may have resulted in polarised results. In addition, the barriers considered in the questionnaire related only to the client and their context. Additional barriers such as the occupational therapist's level of experience and employer-related aspects were not considered.
CONCLUSION
The occupational therapists in this study offered a range of strategies which included direct services (incorporating aspects of hand therapy), indirect services (such as case management and client education), provision of emotional support, and specific work-related strategies. The work-related strategies comprised completing a job demands analysis, work simulation, conducting work-site visits, observing clients at work, work trials and work hardening programmes. The therapists made essential work-place recommendations which they felt contributed to their clients' successful return to work.
This study has uncovered the importance of identifying barriers to work-related transitions in terms of their influence on work-related outcomes, particularly within South Africa with its economic, political and social complexities. The occupational therapists in this study appreciated the importance of emotional and psychological support in relation to managing work-related transitions early in the intervention process. Furthermore, financial compensation was recognised as important in alleviating some of the financial stress associated with a loss of income and in providing clients with every opportunity to receive treatment.
While some strategies for work-related transitions described in international studies (such as issuing assistive devices for work) may not be feasible in contexts such as South Africa, others (such as facilitating early work-related transitions) are relatively easy to implement and were therefore used regularly by participants in this study. The occupational therapists in this study were contributing in a variety of ways to offer comprehensive services to support work-related transitions and addressed the barriers as best they could.
FUNDING STATEMENT
This work was supported by the National Research Foundation of South Africa (GRANT NUMBER: TTK160525166179). Opinions expressed and conclusions arrived at, are those of the authors and are not necessarily to be attributed to the NRF.
AUTHOR CONTRIBUTIONS
All three authors agree to be accountable for this manuscript. All authors conducted the scoping review and the first author conducted the data analysis which contributed to the development of the survey questions used within this part of the study. The second and third authors guided the data analysis process, assisted with conceptual and editorial revisions for all phases of data collection, analysis and manuscript preparation. All researchers contributed to all drafts of the manuscript.
REFERENCES
1. Sorock, G., Lombardi, D., Courtney, J., Mittleman, M. Epidemiology of occupational acute traumatic hand injuries: a literature review. Safety Sciences. 2001; 38(3): 241 - 256. http://doi.org/10.1016/S0925-7535(01)00004-2 [ Links ]
2. Ootes, D., Lambers, K. T., & Ring, D. C. The epidemiology of upper extremity injuries presenting to the emergency department in the United States. Hand (New York, N.Y). 2012; 7(1): 18 - 22. http://doi.org/10.1007/s11552-011-9383-z [ Links ]
3. Statistics Canada Study: Work Injuries; 2007. Retrieved from: https://www150.statcan.gc.ca/n1/daily-quotidien/070710/dq070710a-eng.htm. [ Links ]
4. Ammann, B., Satink, T., & Andresen, M. Experiencing occupations with chronic hand disability: narratives of hand-injured adults. Hand Therapy. 2012; 17(4): 87 - 94. https://doi.org/10.1177/1758998312471253. [ Links ]
5. Norman, R., Matzopoulos, R., Groenewald, P, Bradshaw, D. The high burden of injuries in South Africa. Bulletin World Health Organization. 2007; 85(9): 695 - 702. https://doi.org/10.2471/BLT.06.037184. [ Links ]
6. Waddell, G., Burton, A., Kendall, N. Vocational Rehabilitation What Works, For Whom, And When? Retrieved from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/209474/hwwb-vocational-rehabilitation.pdf. [ Links ]
7. Markussen, S., Roed, K. The impacts of vocational rehabilitation. Labour Economics; 2014. http://dx.doi.org/10.1016/j.labeco.2014.08.0010927-5371/© 2014 Elsevier B.V All rights reserved. [ Links ]
8. Matthews, L., Buys, N., Randall, C., Biggs, C., Hazelwood, Z. Evolution of vocational rehabilitation competencies in Australia. International Journal of Rehabilitation Research. 2010; 33(2): 124 -133. [ Links ]
9. Innes, E., Straker, L. Strategies used when conducting work-related assessments. Work. 2002; 19(2): 149 - 65. [ Links ]
10. Uys, ME., Buchanan, H., Van Niekerk, L. Strategies occupational therapists employ to facilitate work-related transitions for persons with hand injuries: a study protocol for a scoping review. BMJ Open. 2019; 19: e027402. http://doi.org/10.1136/bmjopen-2018-027402corr2. [ Links ]
11. Chen, Y, Hsu, C., Lien, S., Yu, S., Chang, J., Su, S., & Chao, Y Entry into vocational rehabilitation program following work-related hand injury: Potential candidates. International Journal of Occupational Medicine and Environmental Health. 2016; 29(1), 101 - 111. http://dx.doi.org/10.13075/ijomeh.1896.00419 . [ Links ]
12. Marom, B., Ratzon, N., Carel, R., & Sharabi, M. Return-to-work barriers among manual workers after hand injuries: I-year follow-up cohort study. Archives of Physical Medicine and Rehabilitation. 2018; 100(3): 422 - 432. https://doi.org/10.1016/j.apmr.2018.07.429. [ Links ]
13. Cabral, L. H., Sampaio, R. F., Figueiredo, I. M., & Mancini, M. C. Factors associated with return to work following a hand injury: a qualitative/quantitative approach. Revista Brasileira de Fisioterapia. 2010; 14(2): 149 - 157. https://www.ncbi.nlm.nih.gov/pubmed/20464167 [ Links ]
14. Hwang, Y, Chen-Sea, M., & Chen, C. Factors related to return to work and job modification after a hand burn. Journal of Burn Care & Research. 2009; 30(4): 661 - 667. https://doi.org/10.1097/BCR.0b013e3181abfabf . [ Links ]
15. Ramel, E., Rosberg, H-E., Dahlin, L., & Cederlund, R. Return to work after a serious hand injury. Work: A Journal of Prevention. Assessment & Rehabilitation. 2013; 44(4): 459 - 469. https://doi.org/10.3233/WOR-2012-1373 [ Links ]
16. Peters, S, Johnston V., Hines S, Ross M, & Coppieters M. Prognostic factors for return-to-work following surgery for carpal tunnel syndrome: a systematic review. JBI Database of Systematic Reviews and Implementation Reports. 2016; 14(9): 135 - 216. https://doi.org/10.11124/JBISRIR-2016-003099 [ Links ]
17. Statistics South Africa. http://www.statssa.gov.za. (17 June 2020) [ Links ]
18. McLaren, Z., Ardington C., & Leibrandt, M. Distance as a barrier to health care access in South Africa. Southern Africa Labour and Development Research Unit. 2013. Retrieved from: http://www.opensaldru.uct.ac.za/handle/11090/613 [ Links ]
19. de Klerk Susan, Badenhorst Elretha, Buttle Amy, Mohammed Fairuz, Oberem Jeanette. Occupation-based hand therapy in South Africa: challenges and opportunities. SAJOT. [Internet]. 2016; 46( 3 ): 10 -15. [cited 2020 Feb 25] Available from: http://www.scielo.org.za/scielo.php?script=sci_arttext&pid=S23l0-383320l6000300003&lng=en. http://dx.doi.org/10.17159/2310-3833/2016/v46n3a [ Links ]
20. Hoosain, Munira, de Klerk, Susan, & Burger, Marlette. (20l9). Workplace-based Rehabilitation for Upper Limb Conditions in the South African context. SAJOT. 49(2): 57 - 60. https://dx.doi.org/10.l7159/2310-3833/2019/vo149n2a9 [ Links ]
21. Harris, B., Goudge, J., Ataguba, J. et al. Inequities in access to health care in South Africa. J Public Health Pol. 2011; 32: S102 - S123. https://doi.org/10.1057/jphp.2011.35 [ Links ]
22. Coovadia, H., Jewkes, R., Barron, P., Sanders, D., Mcintyre, D. The health and health system of South Africa: historical roots of current public health challenges. Lancet. 2009; 374(9692): 817 - 834. https://doi.org/10.1016/S0140-6736(09)60951-X . [ Links ]
23. Levesque, J., Harris, M.F. & Russell, G. Patient-centred access to health care: conceptualising access at the interface of health systems and populations. Int J Equity Health. 2013; 12: 18. https://doi.org/10.1186/1475-9276-12-18 [ Links ]
24. von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vanden-broucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008; 61(4): 344 - 9. https://doi.org/10.1016/jclinepi.2007.11.005 [ Links ]
25. Setia M. S. Methodology Series Module 3: Cross-sectional Studies. Indian journal of dermatology. 2016; 61(3): 261 - 264. http://doi.org/10.4103/0019-5154.182410 [ Links ]
26. Shing-On Leung. A Comparison of Psychometric Properties and Normality in 4-, 5-, 6-, and 11- Point Likert Scales. Journal of Social Service Research. 2011; 37(4): 412 - 421. https://doi.org/10.1080/01488376.2011.580697 [ Links ]
27. Treiblmaier, Horst and Filzmoser, Peter. Benefits from Using Continuous Rating Scales in Online Survey Research. ICIS 2011 Proceedings. 2011. https://aisel.aisnet.org/icis2011/proceedings/researchmethods/1 . [ Links ]
28. Greco L, Walop W, McCarthy. Questionnaire development: 2. Validity and reliability. CMAJ. 1987; 136: 699 - 700. [ Links ]
29. Law, M. Outcome measure rating form guidelines. Can Journal of OT. 1897; 54: 133 - 138. canchild.ca/system/tenon/assets/attachments/000/000/371/original/measguid.pdf?license=yes. [ Links ]
30. Melvin, J. Roles and functions of Occupational Therapy in hand rehabilitation. The American Journal of Occupational Therapy. 1985; 39(12): 795 - 798. [ Links ]
31. Chan, J., & Spencer, J. Adaptation to hand injury: an evolving experience. American Journal of Occupational Therapy. 2004; 58: 128 - 139. https://doi.org/10.5014/ajot.58.2128 . [ Links ]
32. DeCleene, Kate E.; Ridgway, Angelia J.; Bednarski, Julie; Breeden, Lori; Mosier, Gina Gabriele; Sachs, Deborah; and Stephenson, Donna. Therapists as Educators: The Importance of Client Education in Occupational Therapy. The Open Journal of Occupational Therapy. 2013; 1(4). https://doi.org/10.15453/2168-6408.1050. [ Links ]
33. Koestler, A. Psychological Perspective on Hand Injury and Pain. Journal of Hand Therapy. 2010; 23(2): 199 - 210. http://doi.org/10.1016/j.jht.2009.09.001 . [ Links ]
34. American Occupational Therapy Association. The Unique Role of Occupational Therapy in Rehabilitation of the Hand. 2016. Retrieved from https://www.aota.org//media/Corporate/Files/AboutOT/Professionals/WhatIsOT/RDP/Facts/Hand%20Therapy%20fact%20sheet.ashx . [ Links ]
35. Diagnostic and Statistical Manual of Mental Disorders: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Association; 2013. [ Links ]
36. Keough JL, Fisher TF. Occupational-psychosocial perceptions influencing return to work and functional performance of injured workers. Work. 2001; 16(2): 101 - 110. [ Links ]
37. Dias, J., & Garcia-Elias, M. Hand injury costs. Injury. 2006; 37: 1071 - 1077. https://doi.org/10.1016/j.injury.2006.07.023 [ Links ]
38. Stewart A, Biddulph G, Firth GB. The aetiology of acute traumatic occupational hand injuries seen at a South African state hospital. SA orthop. j. 2017; (4): 49 - 53. [cited 2019 No 26]; http://www.scielo.org.za/pdf/saoj/v16n4/09.pdf [ Links ]
 Correspondence:
Correspondence:
Michelle Uys
Email: michelleelizabethues@gmail.com


{kind=link}
{kind=link}