










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.78 n.9 Johannesburg Oct. 2023
http://dx.doi.org/10.17159/sadj.v78i09.17395
RADIOLOGY CORNER
Desmoplastic Fibroma: a benign neoplasm mimicking a malignancy
L MerboldI; S ShaikII
IDepartment of Oral and Maxillofacial Pathology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa ORCID: 0000-0003-4041-127X Email: Lmerbold@gmail.com
IIDepartment of Oral and Maxillofacial Pathology, School of Dentistry, Faculty of Health Sciences, University of Pretoria, South Africa. ORCID: 0000-0002-4898-3005 Email: shoayeb.shaik@up.ac.za
CASE
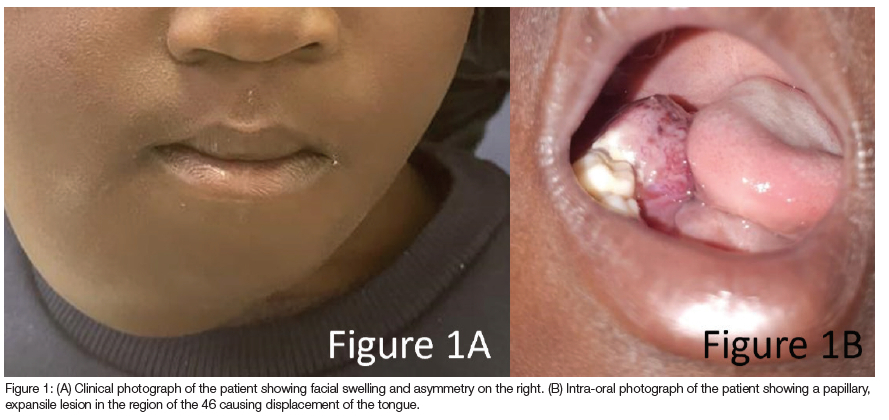
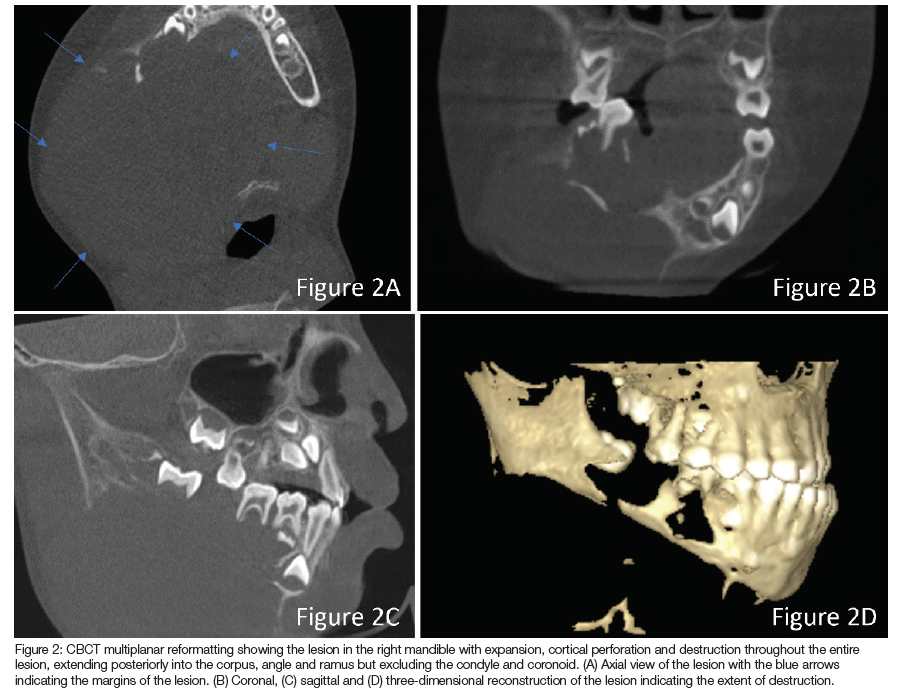
A four-year-old African male patient presented to our clinic with a two-month history of a firm, warm lesion involving the right side of his face. The lesion presented as a bleeding papillary mass in the 85/46 region that extended to the floor of the mouth, causing displacement of the tongue (Figure 1A-B). Upon cone-beam computed tomography (CBCT) examination, an expansile homogenous intermediate density lesion was noted with complete destruction of the bucco-lingual cortical bone. Discernible extensions were identified in the anteroposterior plane from the region of the 84 to the posterior mandible involving the right corpus, developing 46, angle and ramus but spared the condyle and coronoid processes. The lesion extended inferiorly below the epiglottis and showed a reduction of the hypopharynx. Marked bucco-lingual expansion with soft tissue swelling was noted (Figure 2A-D). An incisional biopsy was performed under general anaesthesia, and histological examination rendered a diagnosis of desmoplastic fibroma (DF).
INTERPRETATION
Aetiology and pathogenesis
Desmoplastic fibroma is a rare benign tumour of connective tissue origin with low to variable cellularity. The tumour is a locally aggressive, invasive, benign neoplasm accounting for less than one percent of bone tumours.1 The aetiology of DF is still unknown.2 DF is usually similar to other intraosseous fibrous lesions that mainly occur in the mandible (69.4%) followed by the femur (15%), pelvis (13%), radius (12%) and tibia (9%).1,3,4 The lesion commonly presents as a painless swelling that causes facial asymmetry, tooth displacement and mobility.2
Clinical presentation
DF generally occurs during the first two decades of life with a mean age of 16 and an equal male-to-female ratio.1 It has been reported in patients as young as one year old. Clinically, most DFs present as painless, slow-growing swellings.5 A differential diagnosis of DF is difficult purely based on clinical and radiological examination and, therefore, histopathological examination is required for a definitive diagnosis.1 Histologically, DF generally resembles a soft tissue desmoid tumour.5 According to the World Health Organization (WHO), the pathognomonic histological features for DF are the presence of mature fibrous connective tissue, spindle-shaped fibroblasts (that are separated by abundant collagen fibres) and the absence of cellular mitoses or atypia.6 It is important to distinguish it from other benign spindle cell tumours such as non-ossifying fibroma, myofibroma, odontogenic fibroma, fibrous dysplasia and low-grade fibrosarcoma.1
Diagnosis
DF is a very challenging tumour to diagnose due to the slow onset and unremarkable/variable findings. The radiographic features of DF are not very specific.1 It may present as a uni- or multilocular lesion with well or ill-defined borders.5 Additionally, cortical expansion, perforation or destruction (because of rapid expansion) may cause new bone formation with a "sunburst" appearance. These features may then be mistaken for osteogenic sarcoma or Ewing's sarcoma.2 It commonly presents with a so-called soap bubble appearance and may be misinterpreted as an ameloblastoma, aneurysmal bone cyst or odontogenic myxoma.1 Diagnostic imaging is a vital step in assessing bone lesions. Panoramic radiography is usually the first imaging modality, but three-dimensional imaging, like CBCT, CT and MRI, are the imaging modalities of choice if the lesion presents with suspected cortical perforation and extra-osseous growth.2
Treatment
Due to the aggressive nature and high recurrence rate, the treatment of choice is complete surgical resection with wide margins or enucleation in selective cases.4 The recurrence rate is between 40-47% if the lesion is treated via conservative methods such as curettage. Radiation therapy can be used if the lesion is close to vital structures but should be avoided in children due to post-operative complications.1 Long-term follow-up will be needed for all patients with DF.4 Bone reconstruction is essential for patients' quality of life.2
CONCLUSION
DFs can present very early in life, grow rapidly and have a destructive nature to the extent that they can mimic a malignancy; and thus it is important to manage appropriately. Early diagnosis, comprehensive clinical and radiographic examinations, adequate biopsy site selection, histological
evaluation and appropriate treatment can result in a better prognosis and expectation for the patients.2
DECLARATIONS
Conflict of interest
The authors declare that they have no conflict of interest.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Ethics approval
This study was approved by the University of Pretoria Ethics Committee (Reference no: 456/2023). All procedures followed the ethical standards of the Helsinki Declaration of 1975, as revised in 2008.
REFERENCES
1. Karimi A, Derakhshan S, Khiavi M, Mosavat F, Mirjalili F. (2020). Desmoplastic fibroma of the jaws: a case series and review of literature. Iranian Journal of Pathology, 15(2), 134-143. https://doi.org/10.30699/ijp.2020.103833.2049 [ Links ]
2. Motevasseli S, Yousefi Z, Dalili Kajan Z, Modanlou R, Roudbari N. (2022). Periosteal reaction as a crucial radiographic finding for desmoplastic fibroma of the jaw bone in children: A case report. Imaging science in dentistry, 52(3), 319-326. https://doi-org.uplib.idm.oclc.org/10.5624/isd.20220014 [ Links ]
3. Stelter GO, Rodrigues WN, Schuch LF, Loureiro FJA, Silveira FM, Martins MAT Martins MD. (2023). Desmoplastic fibroma of gnathic bones: a systematic review, Oral Surg, Oral Med, Oral Path and Oral Rad, 136(1), 35. https://doi.org/10.1016/j.oooo.2023.03.081 [ Links ]
4. Mohammadi F, Shirani G, Derakhshan S, Faghihi T. (2020). Desmoplastic fibroma of the lower jaw in a 2-year-old patient; report of a rare case, 17(3), 231-234. https://doi.org/10.4103/1735-3327.284725 [ Links ]
5. Kahraman D, Karakoyunlu B, Karagece, U, Ertas, U, Gunhan O. (2021). Desmoplastic fibroma of the jaw bones: a series of twenty-two cases. Journal of Bone Oncology, 26. https://doi.org/10.1016/j.jbo.2020.100333 [ Links ]
6. El-Naggar AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ. World Health Organization classification of head and neck tumours. 4th ed. 2017 [ Links ]


{kind=link}
{kind=link}