










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562
Print version ISSN 0011-8516
S. Afr. dent. j. vol.71 n.9 Johannesburg Oct. 2016
CASE REPORT
Double Dens In Dente: A rare anomaly
N SisodiaI; MK ManjunathII
ISenior Resident PGIMER and Dr RML Hospital New Delhi-01
IIProfessor and Head JSS Dental College and Hospital, Mysore ,Karnataka
ABSTRACT
Dens in dente refers to a developmental anomaly associated with an abnormal infolding of the inner enamel epithelium into the dental papilla. This in turn gives rise to a possible communication between the pulp and the oral environment, increasing the susceptibility of the tooth to caries, pulpitis, and pulpal necrosis, which highlights the need to detect and seal these pits early. This case report documents an unusual case of double dens invaginatus affecting maxillary central incisors.
Keywords: Dental caries, dens invaginatus, developmental anomaly, surgical operating microscope
INTRODUCTION
Dens in dente, dilated composite odontome, gestant anomaly, and dens telescope are terms commonly used to refer to dens invaginatus and are considered to reflect variations in its presentation.1
It is observed in 0.25% - 5% of individuals2 and is most commonly associated with maxillary lateral incisors (1.7% - 38.5%). It is more frequent in the maxilla than the mandible3 and is seen most often in Caucasians and Asians. Although mostly asymptomatic, dens in dente has been reported to be associated with various syndromes such as Ekman-Westborg-Julin syndrome, Williams syndrome, and Nance Huran syndrome.4,5
The aetiology of dens in dente remains unclear; however, various studies have reported genetics and a variable growth rate as possible causative factors. Mechanical factors, such as growth pressure leading to buckling of the tooth germ and trauma, infection, and a twin theory suggesting the fusion of two tooth germs, are also suggested as causative factors.6-8
Based on the location and extent of invagination, the anomaly can be divided into coronal and radicular types. The depth may vary from being only a lingual pit to a situation giving the appearance of a tooth within a tooth. These factors affect prognosis and treatment. This article reports a case of double dens invaginatus in maxillary central incisors and the management of the anomaly.
CASE HISTORY
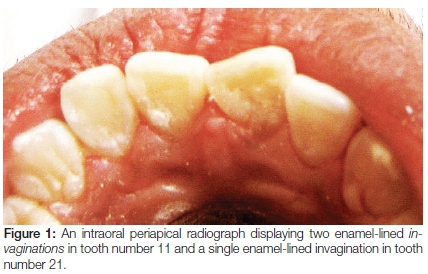
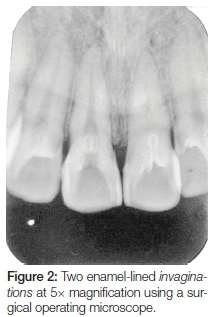
An 18-year-old boy reported to the dental outpatient department with the chief complaint of discolouration of the front teeth and sensitivity on water consumption. No history of pain, swelling, or pus discharge was reported. The patient reported no history of systemic diseases. On examination, the patient exhibited palatal caries in maxillary incisors (tooth numbers: 11, 21, 12, and 22), with extensive carious lesions associated with the right maxillary incisor. All teeth gave a positive response to vitality testing. No pain was elicited on palpation or percussion. Oral hygiene was good. Other active carious lesions were not noted. An intraoral periapical radiograph (Figure 1) revealed the presence of a single type I dens invaginatus in the left maxillary central incisor (21) and a double dens invaginatus in the right maxillary central incisor (11). The tooth anatomy otherwise appeared normal (Figure 2).
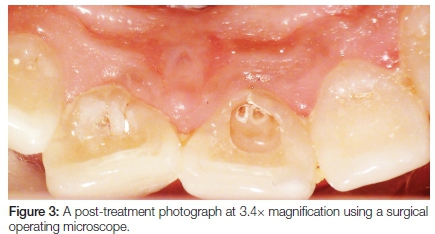
Caries excavation was performed using a number two steel round bur, followed by the placement of a calcium hydroxide liner (Dycal, Dentsply, Tulsa, USA) and temporisation with zinc polycarboxylate cement (Poly F, Dentsply, UK). The patient was recalled after eight weeks. At the second visit, the symptoms had subsided and a positive response was elicited to vitality testing. The temporary restoration was removed, and the tooth was observed under a surgical operating microscope (OPMI-Pico, Carl Zeiss, Germany) at 8X magnification to rule out the presence of remnants of the temporary restoration (Figure 3).
The tooth was etched using 35% phosphoric acid for 20 seconds, rinsed and dried. A dentin bonding agent (Curex, DPI, Mumbai) was applied and light cured for 20 seconds. Flowable composite resin (Tetric N flow, Ivoclar Vivadent) and a capping layer of micro-hybrid composite (Esthet X HD, Dentsply, Tulsa, USA) were used to restore the tooth.
DISCUSSION
Various classifications have been proposed for dens invaginatus. However, the most commonly accepted classification was proposed by Oehler (based on the extent of coronal invagination).3
Type I: An enamel lined minor form occurs within the crown of the tooth and does not extend beyond the cemento- enamel junction.
Type II: An enamel lined form which invades the root as a blind sac. It may or may not communicate with the dental pulp.
Type III: A severe form that extends from the root and opens into the periodontium. It is further divided into two sub-types:
a: An invagination that runs into the root, and communicates laterally with the periodontal ligament, without pulpal involvement.
b: An invagination into the root that communicates with the periodontal ligament at the apical foramen, which is usually lined usually by enamel and rarely by cementum.
Most authors report the presence of a single dens within the tooth. However, double or triple dens in dente have been noted, but rarely. A recent review claimed that only nine case reports of 'double dens invaginatus' have been published.4,5 This anomaly refers to the condition in which two enamel-lined invaginations are present within the tooth. It is most commonly seen in relation to the maxillary anterior and supernumerary teeth6 and may on occasion lead to pulpal involvement.
The clinical importance of this condition cannot be overemphasised because it may contribute to pulpal disease. Researchers have noted that enamel in the region of the dens may be hypomineralised, which allows the easier spread of microbes. In addition, because of the tortuous lingual anatomy of the anterior teeth, subsurface caries may develop within the dens invaginatus, without a breakdown of the external tooth surface.7 This facilitates the progression of caries, which may lead not only to external cavitations but may also enter the main pulp chamber through intercommunications between the dens and pulp cavity. The rarity of Type III (5%) anomaly compared with that of Types I (79%) and II (15%) anomalies highlights the need for a careful radiological and clinical assessment of each case.9
Treating the pulpal involvement of teeth with the dens invaginatus may require special endodontic techniques because of the complexity of the anatomy.8 Therefore, a careful examination of teeth with an enlarged palatal cingulum, conical morphology, and increased labiolingual size is advocated because these signs reveal increased chances of a dilated composite odontome. Methylene blue dye can be used to distinguish the foramen caecum (clinically dilated opening of the dens) from normal fissures.6
With the advent of microdentistry, the surgical operating microscope is an invaluable tool for visualising the anatomy and extent of the dens. It allows for a more conservative preparation, thereby reducing the chances of pulpal exposure. In cases of Type I dens in dente (such as the present case), prophylactic sealing of the potentially problematic region is recommended.
CONCLUSION
Dens in dente, a developmental anomaly, could lead to dental caries which may communicate with the pulp cavity, resulting in pulp necrosis. Its management requires a prompt detection of the anomaly and prophylactic intervention. With delayed detection and subsequent pulpal involvement, more advanced endodontic interventions may be required because of the complexity of the pulp anatomy.
Conflict of Interest: None declared.
References
1. Alani A, Bishop K. Dens invaginatus. Part 1: classification; prevalence, and aetiology. Int Endod J 2008; 41: 1123-36 [ Links ]
2. Pindborg JJ. Pathology of the Dental Hard Tissues. Philadelphia; WB Saunders, 1970: 58 [ Links ]
3. Oehlers FA. Dens inavaginatus: variations of the invagination process and associated anterior crown form. Oral Surg Oral Med Oral Pathol 1957; 10: 1204-18 [ Links ]
4. Serrano J. Triple dens invaginatus in a mesiodens. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1991; 648-9 [ Links ]
5. Mupparapu M, Singer SR, Pisano D. Diagnosis and clinical significance of dens invaginatus to practicing dentists. NY State Dent J 2006; 72: 42-6 [ Links ]
6. Alani A. Dens invaginatus; a problem from the outside. Intl Dent Journal 2009; 59(6): 343-8 [ Links ]
7. Mupparapu M, Singer SR. A rare presentation of dens invaginatus in a mandibular lateral incisor occurring concurrently with bilateral maxillary dens invaginatus: case report and review of literature. Aust Dent J 2004; 49: 90-3 [ Links ]
8. Hulsmann M. Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J 1997; 30: 79-90 [ Links ]
9. Kallianpur S. Dens invaginatus (Type III-B) J Oral Maxillofac Pathol 2012; 16(2): 262-5 [ Links ]
 Correspondence:
Correspondence:
Neha Sisodia
PGIMER and RML Hospital.
E-mail: nehasisodis86@gmail.com
