










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.56 n.1 Pretoria Apr. 2026
https://doi.org/10.17159/2310-3833/2026/vol56no1a11
RAPID REVIEW
Evidence of occupational therapy intervention for depression: A rapid review
Madri EngelbrechtI; Hester M. van BiljonII; Janke van der WaltIII; Shaheed M. SoekerIV
IDivision of Disability and Rehabilitation Studies, Department of Global Health, Faculty of Medicine and Health Sciences, Room 4006, Education Building, Tygerberg Campus, Stellenbosch University, Francie van Zijl Drive, Cape Town, Western Cape, South Africa. https://orcid.org/0000-0002-4606-7572
IIWork-Link Vocational Rehabilitation Practice, No2 Bunting Road, Aucklandpark, Johannesburg, Gauteng, South Africa. http://orcid.org/0000-0003-4433-6457
IIIDivision Occupational Therapy, Department of Health and Rehabilitation Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Francie van Zijl Drive, Cape Town, South Africa. https://orcid.org/0000-0001-5012-0121
IVClinical and Community Engagement, Faculty of Community and Health Sciences, University of the Western Cape, 14 Blanckenberg Street, Bellville CBD, Cape Town, South Africa. https://orcid.org/0000-0001-5382-1855
ABSTRACT
INTRODUCTION: Depression is a leading cause of disability. Occupational therapy interventions address the multifaceted impact of depression by promoting participation and engagement in meaningful activities. This review examined the specific contribution of occupational therapy as part of a national initiative in South Africa to inform public healthcare practice on the role of occupational therapy in treating depressive conditions
METHOD: A rapid review methodology was used to synthesise evidence from the CINAHL and Cochrane Library databases. Systematic reviews and randomised controlled trials (RCTs) published from 2014 until 2025 on occupational therapy interventions for depressive disorders were included. The initial search yielded 265 articles. Following title and abstract of 262 articles conducted by three reviewers using predetermined inclusion criteria, 41 articles proceeded to full-text review
RESULTS: Six systematic review articles with CASP ratings ranging from 70 to 90%, were included. These synthesised evidence from between 5 and 45 RCTs conducted predominantly in high-income countries. Identified intervention themes included return-to-work and work retention after depression, healthy lifestyle interventions and suicide risk mitigation, specific therapeutic approaches and techniques, activity-based and occupational performance components, and social- and community-focussed interventions. Work-focussed interventions showed the strongest evidence base, while tele-health delivery of occupational therapy interventions remained under-explored
CONCLUSION: Occupational therapy interventions for depression span individualised, components of function, and group-based approaches, with emphasis on work and lifestyle outcomes. The evidence is heavily concentrated in high income countries. To inform South African practice, local occupational therapists should prioritise systematic documentation and generation of high quality evidence from diverse economic contexts, and address the limited exploration of tele-health interventions in current practice
IMPLICATIONS FOR PRACTICE
•Local occupational therapists working with persons with depression should prioritise the systematic documentation of interventions and outcomes to contribute to building a contextually relevant evidence base.
•Occupational therapists should develop competencies in tele-health service delivery and explore opportunities to deliver depression interventions through remote platforms while remaining mindful of digital divides and infrastructure limitations.
•Occupational therapists should strengthen community-based rehabilitation (CBR) approaches for depression, integrating with primary care services while addressing community-level stigma and accessibility barriers.
Keywords: tele-health service delivery, return to work, healthy lifestyle, suicide risk mitigation, social- and community-based intervention, good health and well-being
INTRODUCTION
Depression is a leading cause of disability worldwide. The condition, which is characterised by persistent sadness, loss of interest, and functional impairment, and a significant impact on a person's quality of life and social functioning1, also affects the person's ability to participate in daily activities and fulfil occupational roles2. Occupational therapy intervention for depression complements pharmacotherapy and psychotherapy to address the multifaceted challenges associated with this condition3.
Occupational therapy's approach to depression is to promote a person's mental health and well-being through engagement in meaningful activities4. Occupational therapy interventions for depression include activity-based strategies, cognitive-behavioural approaches, sensory modulation, and vocational rehabilitation5. Research has shown that engagement in purposeful activities improves mood, self-efficacy, and overall function6. Occupation-based interventions can be tailored to individual needs while fostering personal autonomy and social participation7.
Occupational therapy intervention and scope of practice in South Africa are governed by the National Health Act8 and the Framework and Strategy for Disability and Rehabilitation services9 which protect the rights of citizens to access the highest standard of health10. Over the past 12 years, the National Health Insurance Policy11 has spearheaded the phased implementation of universal health coverage for South Africans to realise the equal right to health for all citizens.
As the professional association for occupational therapists in South Africa, OTASA was approached to define the roles and practices of therapists within quality healthcare in the country, towards the integration of occupational therapy as rehabilitation offering into universal healthcare. In response to this request, an OTASA task team was commissioned to compile practice evidence for interventions offered in various areas of healthcare, including for occupational therapy for depression. This rapid review directly addresses that mandate by synthesising current evidence to support the articulation of occupational therapy's role in treating depression with the NHI framework.
The OTASA Standards Protocol Group provides guidance on occupational therapy interventions by developing and maintaining standard operating protocols for health conditions where therapists are involved. This rapid review reports the outcomes of a systematic search to produce evidence related to occupational therapy interventions for depressive disorders. The aim of the review was to identify Level 1 evidence-based occupational therapy practices and interventions for depression across all care settings and ages.
METHODOLOGY
Rapid review methodology was selected to provide timely, high level evidence for decision-making related to high priority, emergent, and contextual health questions12. This expedited approach was necessary given the urgent policy timeline for defining occupational therapy roles in universal healthcare. While more streamline than traditional systematic reviews, rapid review methodology promotes knowledge synthesis at an accelerated level while maintaining scientific rigour through systematic searching, critical appraisal, and transparent reporting12.
The authors of this paper conducted the review and met on a monthly basis to promote consistency and uniformity in approaches and support. The authors are occupational therapists with clinical and academic research experience, including in teaching and learning, and clinical student supervision. Subject-specific expertise was obtained from two of the authors who have practice experience in mental health rehabilitation, as well as the draft standard operating procedure (SOP) for occupational therapy depression intervention that was developed by expert therapists in South Africa13. The first author was the principal researcher and was assisted by the other authors during all phases of the review.
The review process was guided by the South African Department of Health's Method Guide for Rapid Reviews14 and the Cochrane Rapid Reviews Method Guide12. Occupational therapy was delineated as a client-centred discipline concerned with the promotion of health and well-being through occupation, as defined by the World Federation of Occupational Therapists (WFOT)15. The primary goal of occupational therapists is to enable the participation of their clients in activities of daily life by enhancing their ability to engage in meaningful occupations15. The levels of care (primary, secondary, and tertiary) considered in the review, was informed by OTASA's outline of where occupational therapists work in South Africa16. Simultaneously, the review considered interventions for depression across the lifespan of persons with the condition. The definition of depression proposed in the draft SOP for South African occupational therapists was used, i.e. "a mood disorder that causes a persistent feeling of sadness and loss of interest"13:2.
Topic and review refinement
The research question was developed through stakeholder involvement to ensure fit for purpose12. As such, the OTASA draft SOP informed the development of the question, i.e. What evidence exists for occupational therapy intervention for depression? The population of interest was defined as persons of all ages, genders, and cultural groups who had been diagnosed with depression, and received occupational therapy at any level of care. Interventions were considered as any occupational therapy treatment as described by WFOT15 and OTASA16, and the outcomes of concern were occupational therapy treatment that enables function in persons with depression to participate and engage in occupations of choice.
Peer reviewed, full text English articles of Level 1 evidence17 (systematic reviews and randomised controlled trials (RCTs)) that reported occupational therapy decision-making, skills, and interventions, and were published from 3 October 2014 until 2 October 2025 were considered for inclusion.
Strategy and search
Two databases, CINAHL and Cochrane Library, were searched on 7 February 2025 for evidence. A MeSH search term builder was used to develop the search string used in the Cochrane Library, namely:
("depression" OR "depressive disorder" OR "major depressive disorder") AND ("occupational therap*") AND ("treatment").
The search string used in CINAHL was:
("depression" OR "depressive disorder" OR "major depressive disorder") AND ("occupational therapy" OR "occupational therapist" OR "occupational therapists" OR "ot") AND ("treatment" OR "intervention" OR "management" OR "rehabilitation") AND ("systematic review").
The search was limited to two databases consistent with rapid review methodology which prioritises efficiency while maintaining rigour12. These databases were selected for their comprehensive coverage of occupational therapy and healthcare literature. CINAHL provides extensive allied health professional literature, while Cochrane Library offers high quality systematic reviews. The search produced respectively 55 articles (Cochrane Library) and 210 articles (CINHAL) for screening. Grey literature was excluded due to the rapid review timeframe and the focus on Level 1 evidence, which is predominantly published in peer-reviewed sources. We acknowledge this may have excluded practice-based evidence from conference proceedings or organisational reports, particularly from LMIC settings.
Screening and selection
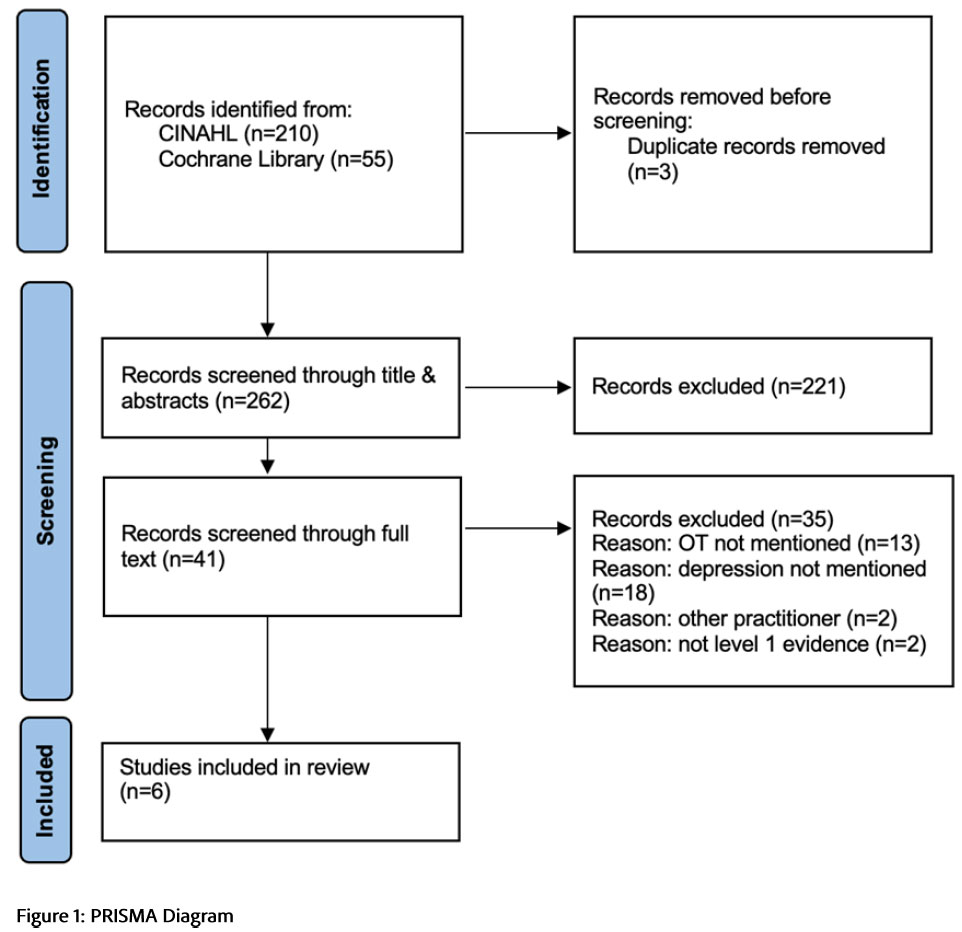
The 265 articles were uploaded into web-based Rayyan.ai18 software to assist with the organisation and coordination of reviews and knowledge synthesis. Rayyan.ai detected six (n=6) duplicates which were resolved by the first author by deleting three duplicated articles. Two hundred and sixty-two (n=262) articles remained for title and abstract screening.
Two reviewers (the first and second listed authors) independently screened all titles and abstracts according to the developed inclusion and exclusion criteria, and 221 articles were excluded. Forty-one (n=41) articles remained for full text screening which was done by two reviewers (the first and third listed authors) and a third reviewer (the fourth listed author) resolved 11 disagreements through review and discussion with the first reviewer. Only six (n=6) articles met the selection criteria and were included in the review. Articles were excluded when the service providers' delivering interventions were not identified, or were identified as other than occupational therapists, when the article reported general rehabilitative interventions without specifying occupational therapy involvement, when depression was not specifically identified as a condition in the article, and if the article did not report Level 1 evidence. One article (Natale et al.24) was included despite not explicitly mentioning occupational therapy, as it examined psychosocial interventions commonly delivered by multidisciplinary teams including occupational therapists in dialysis settings, and the interventions described fall within occupational therapy scope of practice. Figure 1 (below) shows the results of the search, screening, and selection in the form of a PRISMA diagram19
Risk of bias assessment, quality appraisal and data extraction
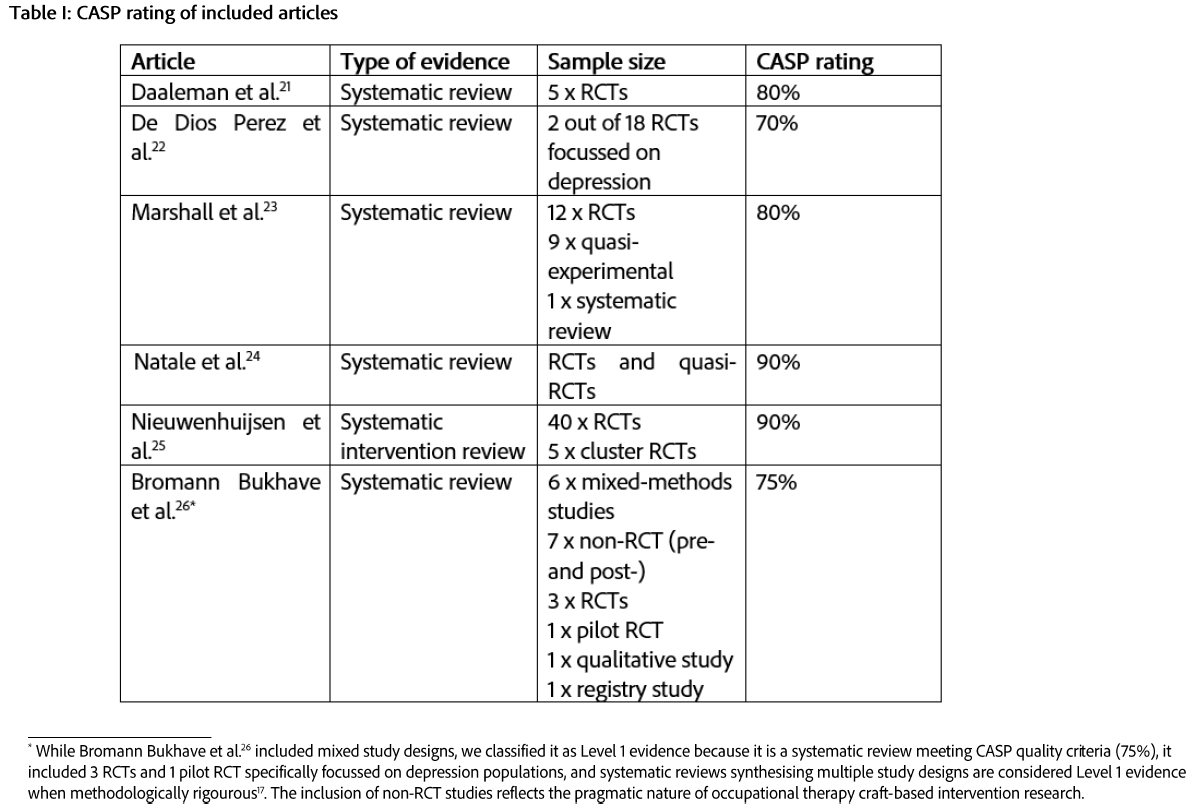
The quality of the included systematic reviews (n=6) was evaluated using the Critical Appraisal Skills Programme (CASP) appraisal tool for Systematic Reviews20, and achieved mostly high ratings from 75% and 90%, as shown in Table I, (page 4) These ratings reflect methodological rigor, reliability, and relevance of findings, and provide a foundation for drawing conclusions about the effectiveness of interventions that were examined across the included studies. All studies demonstrated strong methodological quality (>70%), with four studies achieving >80%. The primary methodological limitations identified through CASP appraisal included limited precision of results due to small sample sizes and heterogeneity22,23, and one review indicated potential incompleteness in the inclusion of relevant studies26. A limitation of the CASP analysis itself is that high overall scores may obscure uncertainties related to applicability, economic feasibility, and implementation, indicating that while the evidence is credible and suitable for informing practice and policy discussions, conclusions should be interpreted cautiously, particularly when translating findings into resource-constrained or context specific settings.
A data extraction sheet was developed in MS Excel to capture information about the type of study, the study setting and population, occupational therapy interventions, and the outcomes of interventions.
Synthesis
Analysis and synthesis of data were done by grouping studies by themes, intervention types and foci, and outcomes. Patterns and inconsistencies in the data were highlighted, and key findings summarised. Quantitative aspects of data, for example frequency of interventions, were counted and grouped, and then expressed as percentages to derive meaningful insights. Data, outcomes, and discrepancies were discussed in meetings amongst the co-researchers. The first author integrated analytical insights to synthesise the discussion and conclusions.
RESULTS
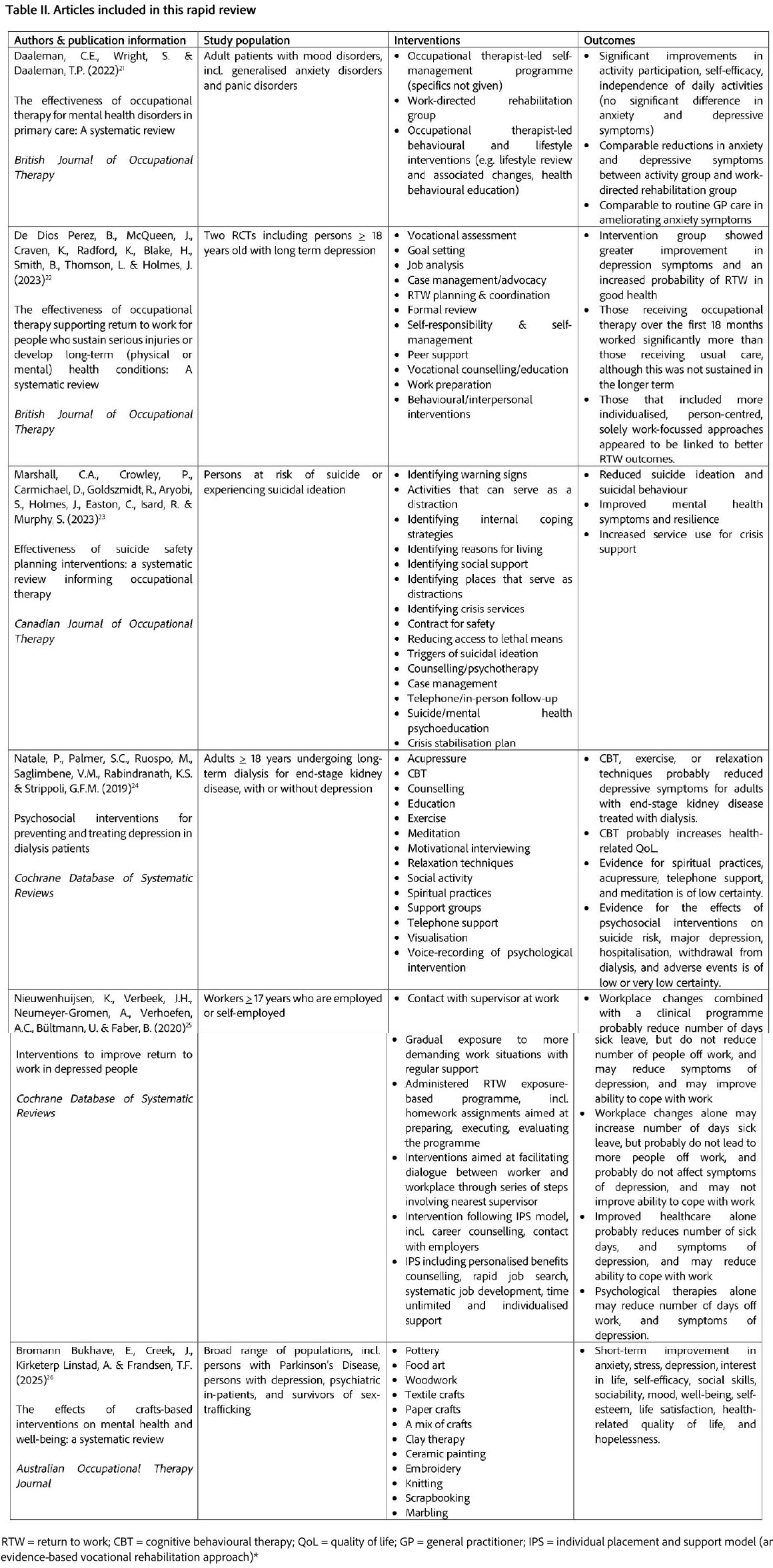
Six (n=6) articles published from 2019 until 2025 were included in the review, shown in Table II (page 5). Three (n=3) of these reported effectiveness studies21,22,23; of which two (n=2) had a focus on the effectiveness of occupational therapy intervention with clients with depression21,22 and one (n=1) focussed on the effectiveness of suicide safety planning23. All articles reported systematic reviews, of which five (n=5) reported data from high income countries, namely Sweden21,22, the United Kingdom21,22,25, the United States of America21,22,23,25, Ireland21, France22, the Netherlands22, Denmark22, Canada22,23, Switzerland22,23, Germany22, Australia22,23,26, and Taiwan23. One article included data from Europe without specifying which European countries data were obtained from25, and one article did not specify the country setting24. Only one study mentioned limited data from a low- to middle-income country, namely India23.
A third of the articles (n=2) did not report the service settings where interventions were offered24,25, but those that did included a wide range of settings. These were primary care21,26, specialised mental health/behavioural outpatient clinics23, community dwelling settings21,26, in-person clinical settings22,26, workplace settings22, community-based settings22,23,26, veteran services, refugee camps, emergency departments, and colleges/universities23. Three studies included the delivery of interventions via telephone, mail, or other virtual means22,23,26, and one study reported data gathered at a museum as intervention setting, an art gallery, an archive service, and a research institute26.
Most studies reported interventions with adult populations (older than 17 years), with the exception of one study that did not report any ages26, and all studies included populations of persons with depression. Diagnoses or conditions included were mood disorders, generalised anxiety disorder, and panic disorders each with depression present21, persons with depression who are at risk of suicide or who are experiencing suicidal ideation23, and persons with depression and end-stage kidney disease who were treated with long-term dialysis24. One study focussed on workers with depression25, and another included a wide variety of populations, including persons with physical conditions, e.g. women with hand osteoarthritis, and survivors of sex-trafficking26.
Synthesis across studies revealed a number of convergent findings, namely that work-focussed interventions with persons with depression consistently incorporated both workplace and clinical elements, and that activity-based approaches put emphasis on meaningful occupation over passive therapies. Social support was, furthermore, integrated across multiple intervention types rather than stand-alone interventions, and individualisation and person-centredness were centrally positioned regardless of intervention category. There was variable specificity in the descriptions of occupational therapy versus multidisciplinary roles in the articles, and different intensities and durations of interventions were reported, from a single session to 24 months, along with limited consensus on optimal outcomes measures.
While Bromann Bukhave et al.26 included mixed study designs, we classified it as Level 1 evidence because it is a systematic review meeting CASP quality criteria (75%), it included 3 RCTs and 1 pilot RCT specifically focussed on depression populations, and systematic reviews synthesising multiple study designs are considered Level 1 evidence when methodologically rigourous17. The inclusion of non-RCT studies reflects the pragmatic nature of occupational therapy craft-based intervention research.
Occupational therapy interventions
A broad range of occupational therapy interventions was reported in the included articles, spanning specific therapies or techniques, such as meditation, as well as psycho-education, and skills training approaches. The most extensively described areas of intervention were work-focussed interventions, healthy lifestyle practices, suicide focussed safety planning interventions, social and community-based approaches, and specific therapies.
Work-focussed interventions for depression
Two articles reported the occupational therapy focus of interventions to be on work (return to work and work retention) with persons with depression. Across these studies a pattern emerged of graded, individualised approaches that combine workplace modifications with clinical interventions. Common elements included vocational assessment, goal setting, self-management and self-responsibility, behavioural and interpersonal interventions, work hardening, vocational counselling or education, case management, return-to-work planning and coordination22.
Both studies emphasised the importance of employer engagement and workplace dialogue, though Nieuwenhuijsen et al.25 provided more detail on specific facilitation techniques. Furthermore, the intervention elements of job analysis, ergonomics, formal review, work modification, adaptations, and adjustment, and emotional adjustment interventions were included in the occupational therapist's approaches22.
The Individual Placement and Support (IPS) model appeared in two instances25, suggesting that this structured approach has gained traction in occupational therapy practice for depression-related work disability.
Interventions towards healthy lifestyle practices
Two studies reported on occupational therapy interventions that promote healthy lifestyle practices with persons with depression, with exercise emerging as an intervention element across different populations and contexts. Physical exercise interventions ranged from supervised strength exercises for reducing work-related sickness absence25, to broader exercise programmes incorporated within psychosocial interventions for adults undergoing long-term dialysis24.
A methodological limitation across studies was the lack of clarity regarding professional discipline boundaries. Nieuwenhuijsen et al.25 examined multidisciplinary interventions without distinguishing between occupational therapist-specific and other team member contributions, while Natale et al.24 reported exercise as part of psychosocial interventions without explicit attribution to occupational therapy practice.
Beyond exercise, spiritual practices were identified as an additional intervention element within psychosocial approaches24, though operational definitions and implementation details were limited across the reviewed literature. This pattern of incomplete intervention descriptions limited the ability to determine specific occupational therapy contributions and replicate interventions in clinical practice.
Suicide safety planning and risk mitigation interventions
Interventions geared towards preventing suicide of persons with depression, or reducing the risk of suicide, featured prominently in one of the reviewed articles. Marshall et al.23 conducted a systematic review to ascertain the effectiveness of suicide safety planning (SSP) interventions, with the aim of informing occupational therapy practice. Intervention elements noted were the identification of warning signs of a suicide crisis, and utilising meaningful activity engagement as a distraction. Other SSP elements comprised the identification of internal coping strategies, identification of reasons for living, identification of social support, identification of places that could serve as distractions, and the identification of crisis services.
Contracting for safety, where the person with depression makes a verbal contract with the practitioner to reach out for professional support, was a component highlighted to occupational therapists. Furthermore, interventions included reducing access to lethal means, identifying triggers of suicidal ideation, counselling and psychotherapy, case management, telephonic or in-person follow-up, suicide or mental health psychoeducation, and devising crisis stabilisation plans.
Therapies and techniques for intervention
Therapeutic techniques reported across four studies revealed both discipline-specific and shared approaches within multidisciplinary contexts. Occupational therapists working in clinical mental health environments reported the use of art therapy, breathing exercises, calming techniques, mindfulness practice, and discussion in interventions for depression26. The use of cognitive behavioural therapy and relaxation techniques within occupational therapy scope were reported in another study24. However, professional boundaries remained ambiguous for interventions such as counselling and psychotherapy which appeared in multidisciplinary protocols without clear attribution to specific disciplines. In Marshall et al.'s review23 psychotherapy was identified as part of suicide safety planning protocols, while Natale et al.24 described it within broader psychosocial interventions for dialysis patients with depression.
A pattern emerged in interventions for dialysis patients with depression, where complementary and alternative approaches supplemented conventional techniques. These included acupressure, techniques of meditation, motivational interviewing, visualisation, and clients listening to the voice recording of psychological interventions were recorded as interventions with this group24.
Activity-based and component-focussed interventions
The literature revealed some distinct yet complementary approaches to activity-based and component-focussed occupational therapy interventions for depression. Meaningful activity engagement served dual purposes; firstly, as distraction for persons with suicidal ideation23, and secondly, as social participation vehicles for persons with depression who are undergoing dialysis24. Craft-based interventions represented the most extensively documented activity modality, with Bromann Bukhave et al.26 identifying six craft types (pottery, food art, woodwork, textile crafts, paper crafts, and mixed crafts) employed across diverse populations. Outcomes from craft interventions extended beyond the reduction of symptoms of anxiety, stress, and depression, and encompassed enhanced psychosocial functioning. These included improved self-efficacy, social skills, mood, well-being, self-esteem, life satisfaction, quality of life, as well as reduced hopelessness. Bromann Bukhave et al.'s26 findings suggest that craft activities address multiple dimensions of recovery simultaneously.
Beyond activity-based approaches, the literature identified key intervention elements integrated into occupational therapy practice. Psychoeducation appeared consistently in both suicide prevention protocols23,24 and depression treatment programmes23,24. Goal setting further emerged as intervention element for persons with long-term mental health conditions22 returning to work, suggesting that element selection may be context-dependent rather than universally applied across all depression interventions.
Social- and community-focussed intervention
Social support interventions emerged as a universal intervention element regardless of population or practice setting. However, the operationalisation of social support varied. Peer support appeared in vocational contexts where return-to-work was a focus22, as well as in the context of suicide prevention (crisis contexts)23, and in medical contexts through support groups for persons undergoing dialysis24. Delivery modalities ranged from face-to-face formats to remote telephone support24, indicating flexibility in intervention implementation.
A notable difference existed between passive social support identification and active case management. While most studies described social support as an element to be identified or established, Marshall et al.23 positioned case management as a broader community-focussed intervention that integrates social support needs assessment with ongoing care coordination and monitoring for suicide prevention. This suggests a continuum from specific social support interventions to comprehensive case management functions within occupational therapy practice, though only one study addressed this expanded scope23.
DISCUSSION
This review found evidence of occupational therapy interventions for depression that span individualised and component-focussed approaches to groups and interventions aimed at the occupational performance areas of work and lifestyle. However, the scope of this review omitted evidence of assessments performed and approaches to assessment to plan occupational therapy intervention with persons with depression. Assessment procedures form part of a comprehensive occupational therapy approach with this condition. The draft Depressive Disorders Protocol for Occupational Therapists13, developed for South African occupational therapists, addresses this gap by elaborating assessment procedures used in the local context. A complementary review of evidence to support occupational therapy assessment practices would expand the evidence-base further.
Importantly, the identification of only six studies that met the inclusion criteria of this review invites critical examination. This limitation may reflect a genuine scarcity of Level 1 occupational therapy-specific depression research, or database limitations in the capturing of occupational therapy literature. Moreover, the integration of occupational therapy approaches in multidisciplinary mental health teams may make it difficult to identify profession-specific interventions, while overly restrictive inclusion criteria in this review may have excluded potentially relevant studies. The limited database search likely contributed to the exclusion of occupational therapy-specific journals that are not comprehensively indexed in these databases. Future reviews should include OTDBASE, OTSeeker, and manual searches of core occupational therapy journals to capture the full scope of occupational therapy depression intervention research.
The reviewed evidence included CBT, counselling, and psychotherapy as interventions, although we acknowledge that not all included studies explicitly identified occupational therapists as the sole service provider. Some interventions were delivered within multidisciplinary teams, making it difficult to isolate occupational therapy-specific contributions. In South Africa, entry-level occupational therapy training includes basic cognitive-behavioural strategies, activity-based counselling, and psychoeducation13. However, formal psychotherapy and specialised CBT typically require postgraduate training and may represent scope expansion rather than core occupational therapy practice. Although the OTASA draft Standard Operating Protocol13 includes these approaches, which may suggest scope evolution in local practice, we caution against overstating occupational therapy's role as primary provider of psychological therapies, and recognise that these are often shared or collaborative functions within mental health teams. Occupational therapy's distinct contribution lies in occupation-focused application of psychological principles rather than traditional talk therapy. Such clear boundaries benefit both professional identity and interprofessional collaboration.
The gathered evidence further reflects the current state of occupational therapy depression intervention research, where high quality RCTs remain limited. As such, some included systematic reviews synthesised heterogeneous study designs and populations. In such cases, we focussed our analysis on depression-specific findings within broader reviews while noting this limitation in interpreting effect sizes and applicability.
The concentration of evidence from high-income countries has important implications for LMIC practice. HIC contexts more typically feature comprehensive healthcare systems, established occupational therapist roles, resources for intensive interventions, and populations with different cultural conceptualisations of depression. Despite such geographic disparities, South African occupational therapy practice correlates strongly with the evidence13. Notable areas of alignment include the emphasis on work-focussed interventions after depression, the centrality of psycho-education as a treatment modality across all phases of intervention, and the re-establishment of occupational roles, habits, routines, and rituals after diagnosis13. However, direct translation of HIC interventions to LMIC settings risk overlooking resource constraints that are prevalent in LMICs, the imposition of Western depression models onto diverse cultural frameworks, de-prioritising community-based and family-centred approaches that are more feasible in LMICs, and underestimating barriers created by stigma in some settings.
Beyond South Africa, occupational therapy practices with persons with depression across Southern Africa similarly emphasise vocational rehabilitation and supported employment, including elements of client-centred approaches, illness self-management education, and adapted behavioural therapies27,28. However, Level 1 evidence from these contexts remains notably absent, demonstrating a gap in the research literature.
The reviewed evidence displayed, furthermore, an emphasis on the application of therapies and techniques, for example, counselling, CBT, and mindfulness, that are not traditionally considered core occupational therapy interventions. This integration, however, reflects contemporary occupational therapy practice rather than a departure from the profession's scope. South African occupational therapists acquire a basic level of skill in these techniques as part of their undergraduate training, and the draft Standard Operating Protocol of OTASA describes these approaches as integral elements of local occupational therapy interventions for persons with depression13.
In mental health settings where occupational therapists form part of multi-disciplinary teams, the adoption of psychological therapies within occupational therapy constitute common practice29. These psychological approaches tend to become integrated into occupational therapy frameworks to enhance therapeutic outcomes30, representing an evolution of the profession rather than a deviation from its foundational principles.
The South African draft Standard Operating Protocol identifies several interventions that were absent from the reviewed studies. These include home programmes, assistive devices and technology, cognitive interventions (encompassing remediation, cognitive hardening, and ergonomics), time management strategies, and approaches addressing community-level stigma13. This distinctive focus may reflect South African occupational therapists' emphasis on community-level services, a practice orientation further evidenced by the Protocol's description of risk assessments before discharge and occupational therapy's focus on home, work, and school adjustments during community reintegration13. This community-based mental health approach align with broader patterns observed in low- to middle-income countries, where mental health services frequently involve psychoeducation, skills training, rehabilitation, and psychological treatments delivered in community settings like homes and schools31. Such community-context interventions prioritise accessibility, acceptability, ongoing contact with trusted local providers, family involvement, and economic benefits to persons with depression. However, substantial variations exist in how these elements integrate with primary care services31, suggesting the need for context specific implementation frameworks.
Finally, the review revealed a notable gap in reporting on tele-health use in depression intervention, similarly limited in its consideration in the South African Protocol. This omission is surprising considering the development and uptake of tele-health interventions in the past decade and their proven advantages, which include increased accessibility, cost-effectiveness, feasibility, privacy protection, and facilitation of integrative care with primary providers32. Even before the COVID-19 pandemic accelerated the growth of tele-health services, remote delivery of mental health services had become integrated across both high income and low- to middle-income countries. Evidence indicates that videoconferencing, in particular, achieves high patient satisfaction, improves clinical outcomes, and has the potential to promote cost-effectiveness33. Nevertheless, the challenges of digital divides, infrastructure limitations, and the need for ongoing care and culturally sensitive programme design in low- to middle-income countries and rural communities may contribute to the persistent under-utilisation of tele-mental health services33. Addressing these barriers represents a frontier for expanding access to occupational therapy interventions for depression, particularly in resource-constrained contexts.
Implications and recommendations
Practice implications
Given the lack of documented evidence from low- to middle-income countries, it is important that occupational therapists working with persons with depression prioritise the systematic documentation of both assessment procedures, interventions, and outcomes. This documentation will contribute to building an evidence base with local and contextual relevance.
Research priorities
Along with practice information, there is a need for high quality research that examines occupational therapy interventions for depression in low- to middle-income countries, particularly in Southern Africa. Future studies must investigate the effectiveness of locally adapted interventions, including vocational rehabilitation, community-based services, and interventions addressing stigma and home- or work adjustments. This research would provide evidence-based support for practices already implemented in these contexts.
Tele-health service delivery
Occupational therapists are encouraged to explore opportunities to deliver depression interventions through remote platforms. Developing competencies in tele-health service delivery is recommended, for example virtual home assessments for routine and activity pattern evaluation, digital craft-based interventions, and tele-health vocational counselling and workplace consultation. Tele-health development should, however, remain mindful of digital divides and infrastructure limitations when serving rural or under-resourced populations. Future research should investigate the effectiveness, feasibility, and acceptability of tele-health delivered occupational therapy interventions for depression across diverse settings. Studies should, specifically, examine implementation in low to middle-income countries and rural areas, identify barriers to uptake, and develop culturally sensitive tele-health protocols that maintain therapeutic effectiveness while addressing contextual challenges.
Policy implications
Occupational therapy as a profession that addresses depression must be recognised explicitly in the care pathways within universal health coverage. As such, prioritised funding for community-based occupational therapy positions and telehealth infrastructure becomes imperative in the planning and development of the Department of Health's strategy.
Community-based interventions
Finally, research is needed to examine the effectiveness of community-based occupational therapy interventions for depression, including their integration with primary care services. Studies should identify best practices for community reintegration support, evaluate the impact of addressing community-level stigma, and explore sustainable models for delivering ongoing community-based care in resource-constrained settings.
Ethical consideration declaration
Ethical clearance was not required for this review as no primary data collection was done. The quality and bias of selected articles were tested to ensure quality results to inform the question of this review.
CONCLUSION
This review identified evidence of occupational therapy interventions for depression across individualised, component-focussed, and group-based approaches, with emphasis on work and lifestyle performance areas. Among intervention categories, work-focussed approaches demonstrated the strongest evidence base, with consistent findings across multiple systematic reviews supporting graded return-to-work programmes that combine workplace modifications and clinical interventions. Craft-based activity interventions showed promising short-term outcomes, while suicide safety planning protocols provide clear frameworks for occupational therapy contribution to crisis intervention. Evidence for lifestyle interventions and specific therapies was more variable and often embedded within multidisciplinary delivery.
Evidence gaps emerged, most notably the geographic concentration of evidence in high income countries. This represents a critical limitation for South African and Southern African practice, where contextual factors such as resource constraints, cultural conceptualisations of depression, community-based care models, and stigma differ from HIC settings. South African and Southern African occupational therapists demonstrate practices consistent with international evidence, yet operate without locally generated Level 1 evidence. Additionally, unique intervention foci, such as community-based services, reflect contextually responsive practices that remain undocumented in the international literature.
The most urgent research priorities are effectiveness studies of occupational therapy depression interventions in LMIC settings, particularly in South Africa, clear documentation of occupational therapy-specific contributions within team-based care, development of tele-health intervention and testing, and cultural adaption processes for occupation-based approaches.
For South African occupational therapy practice, this review supports a continued emphasis on work-focussed rehabilitation, integration of craft and meaningful activity approaches, suicide safety planning competency development, and systematic documentation as foundation for local evidence generation. The profession must prioritise rigorous documentation of assessment and interventions practices, generate high quality evidence from diverse economic contexts, and address the notable absence of tele-health interventions in current practice.
Conflict of interest declaration
The authors declare they received remuneration from the Occupational Therapy Association of South Africa (OTASA) for this review. They declare that this did not affect their decision making in the review and results were not skewed. They have no bias to declare.
Author contributions
All listed authors planned and participated in the review. Shaheed Soeker initiated the review, and Madri Engelbrecht led the writing of the article. All authors approved the final version of the manuscript.
REFERENCES
1. American Psychological Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). 5th ed., Washington D.C.: American Psychological Association Publishing; 2022. Available from https://doi.org/10.1176/appi.books.9780890425787 [ Links ]
2. World Health Organisation. International classification of functioning, disability and health: ICF. Geneva: WHO; 2001. Available from http://www.who.int/classifications/icf/en/ [ Links ]
3. Argentzell, E., Bäckström, M., Lund, K. & Eklund, M. (2020). Exploring mediators of the recovery process over time among mental health service users, using a mixed model regression analysis based on cluster RCT data. BMC Psychiatry, 20(1), 520. https://doi.org/10.1186/s12888-020-02924-2 [ Links ]
4. American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and process fourth edition, Am J Occup Ther. 2020;74:1-87. Available from https://doi.org/10.5014/ajot.2020.74S2001 [ Links ]
5. Wisenthal, A., Krupa, T., Kirsh, B.H. & Lysaght, R. Cognitive work hardening for return to work following depression: an intervention study. Can J Occup Ther. 2018;85(1):21-32. https://doi.org/10.1177/0008417417733275 [ Links ]
6. Wilcock, A.A. & Hocking, C. (2015). An occupational perspective of health (3rd Ed.). Thorofare, NJ: SLACK Incorporated [ Links ]
7. Ikiugu, M.N. & Pollard, N. (2015). Meaningful living across the lifespan: occupation-based intervention strategies for occupational therapists and scientists. London: Whiting & Birch Ltd [ Links ]
8. South African Government. National Health Act 61 of 2003. South Africa; 2003; [Accessed 2023 Jun 10]. Available from https://www.gov.za/sites/default/files/gcis_document/201409/a61-03.pdf [ Links ]
9. National Department of Health. Framework and Strategy for Disability and Rehabilitation services [homepage on the internet]. 2015 [Accessed 2023 Jun 10]. Available from http://ilifalabantwana.co.za/wp-content/uploads/2016/07/Framework-25-may_1_3.docx [ Links ]
10. South African Government. The Constitution of the Republic of South Africa. The Bill of Rights Republic of South Africa: https://www.gov.za/documents/constitution/chapter-2-bill-rights; 1996 p.243. [ Links ]
11. National Department of Health. White Paper: National Health Insurance Policy - Towards Universal Health Coverage. Dep Heal. 2017;1-67. Available from https://www.health.gov.za/wp-content/uploads/2023/11/NHI-Policy-2017.pdf [ Links ]
12. Garritty, C., Gartlehner, G., Nussbaumer-Streit, B., King, V. J., Hamel, C., Kamel, C., et al. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J Clin Epidemiol. 2021;130:13-22. https://doi.org/10.1016/j.jclinepi.2020.10.007 [ Links ]
13. OTASA (2026) Depressive disorders standard operating protocol for occupational therapists (OT). Unpublished. Available at https://www.otasa.org.za/wp-content/uploads/2025/12/OTASA-Draft-Protocol-for-Depression-.pdf [ Links ]
14. Department of Health. (2022). NEMLC-Protocol Template for rapid reviews of COVID-19_v4.0_12March2022 1 Methods guide for rapid reviews for covid-19 medicine reviews Rationale for rapid reviews. https://www.health.gov.za/wp-content/uploads/2022/03/Protocol-Template-for-rapid-reviews-of-COVID-19_v4.0_12March2022.pdf [ Links ]
15. WFOT. WFOT Definition of Occupational Therapy [Internet]. 2012. Available from https://wfot.org/resources/definitions-of-occupational-therapy-from-member-organisations [ Links ]
16. OTASA. O.T.A. of S. (2017). Occupational Therapy Association of South Africa Position statement on rehabilitation. South African Journal of Occupational Therapy, 47(3), 63-64. https://doi.org/10.17159/2310-3833/2017/v47n3a9 [ Links ]
17. Forrest, J.L. and Miller, S.A. Translating evidence-based decision making into practice: EBDM concepts and finding the evidence. J Evid Based Dent Pract. 2009;9:59-72. https://doi.org/10.1016/j.jebdp.2009.03.017 [ Links ]
18. Rayyan Systems I. (2020) Rayyan Intelligent Systematic Review. Rayyan https://rayyan.qcri.org/. 2020. [ Links ]
19. King, V.J., Stevens, A., Nussbaumer-Streit, B. Kamel, C. and Garritty, C. (2022). Paper 2: Performing rapid reviews, Systematic Reviews, 11(1):1-10. https://pubmed.ncbi.nlm.nih.gov/35906677/ [ Links ]
20. Critical Appraisal Skills Programme. CASP Systematic Review [Internet]. 2018. Available from https://casp-uk.net/casp-tools-checklists/systematic-review-checklist/ [ Links ]
21. Daaleman, C. E., Wright, S. T., & Daaleman, T. P. The effectiveness of occupational therapy for mental health disorders in primary care: A systematic review. Br J Occup Ther. 2022;85(4): 224-30. https://doi.org/10.1177/03080226211058362 [ Links ]
22. De Dios Perez, B., McQueen, J., Craven, K., Radford, K., Blake, H., Smith, B., Thomson, L., Holmes, J. The effectiveness of occupational therapy supporting return to work for people who sustain serious injuries or develop long-term (physical or mental) health conditions: A systematic review. Br J Occup Ther. 2023;86(7): 467-81. https://doi.org/10.1177/03080226231170996 [ Links ]
23. Marshall, C. A., Crowley, P., Carmichael, D., Goldszmidt, R., Aryobi, S., Holmes, Easton, C., Isard, R., Murphy, S. Effectiveness of Suicide Safety Planning Interventions: A Systematic Review Informing Occupational Therapy. Can J Occup Ther. 2023;90(2): 208-36. https://doi.org/10.1177/00084174221132097 [ Links ]
24. Natale, P., Palmer, S.C., Ruospo, M., Saglimbene, V.M., Rabindranath, K.S., Strippoli, G.F.M. (2019). Psychosocial interventions for preventing and treating depression in dialysis patients. Cochrane Database of Systematic Reviews 2019, Issue12. Art. No.: CD004542. https://doi.org/10.1002/14651858.CD004542.pub3 [ Links ]
25. Nieuwenhuijsen, K., Verbeek, J.H., Neumeyer-Gromen, A., Verhoefen, A.C., Bültmann, U., Faber, B. (2020). Interventions to improve return to work in depressed people, Cochrane Database of Systematic Reviews (10). Art. No.: CD006237, DOI: https://doi.org/10.1002/14651858.CD006237.pub4 [ Links ]
26. Bromann Bukhave, E., Creek, J., Kirketerp Linstad, A. & Frandsen, T.F. The effects of crafts-based interventions on mental health and well-being: a systematic review, Australian Occupational Therapy Journal. 2025;72:e70001. https://doi.org/10.1111/1440-1630.70001 [ Links ]
27. Chimara, M., Van Niekerk, L., & van Biljon, H. M. Scoping review exploring vocational rehabilitation interventions for mental health service users with chronic mental illness in low-income to upper-middle-income countries. BMJ Open. 2022; 12(5): e059211. https://doi.org/10.1136/bmjopen-2021-059211 [ Links ]
28. Mavindidze, E., Nhunzvi, C., & Van Niekerk, L. Supported employment interventions for workplace mental health of persons with mental disabilities in low-to-middle income countries: A scoping review. PLoS ONE. 2023;18(9 September), 1-18. https://doi.org/10.1371/journal.pone.0291869 [ Links ]
29. Eklund, M., Parsonage-Harrison, J. & Argentzell, E. Occupation- and lifestyle-based mental health interventions - A hallmark for the occupational therapy profession? British Journal of Occupational Therapy. 2024; 87(7): 395-97. https://doi.org/10.1177/03080226241228750 [ Links ]
30. Walker, N., Vernon-Smith, M., & Townend, M. A feasibility study of a novel work-focused relational group CBT treatment programme for moderate to severe recurrent depression. Mental Health Review Journal. 2021;26(4): 328-52. https://doi.org/10.1108/MHRJ-01-2021-0005 [ Links ]
31. Kohrt, B. A., Asher, L., Bhardwaj, A., Fazel, M., Jordans, M. J. D., Mutamba, B. B., et al. The role of communities in mental health care in low-and middle-income countries: a meta-review of components and competencies. Int J Environ Res Public Health. 2018;15(6). https://doi.org/10.3390/ijerph15061279 [ Links ]
32. Hand, L.J. The role of telemedicine in rural mental health care around the globe, Telemedicine journal and e-health. 2022;28(3): 285-294. https://doi.org/10.1089/tmj.2020.0526 [ Links ]
33. Richardson, L. K., Frueh, B. C., Grubaugh, A. L., Egede, L., & Elhai, J. D. Current directions in videoconferencing tele-mental health research. Clinical Psychology: Science and Practice. 2009;16(3): 323-38. https://doi.org/10.1111/j.1468-2850.2009.01170.x [ Links ]
 Correspondence:
Correspondence:
Madri Engelbrecht
Email: madrieng@sun.ac.za
Submitted: 27 October 2025
Reviewed: 12 December 2025
Revised: 19 January 2026
Accepted: 20 January 2025
Published: April 2026
EDITOR: Blanche Pretorius, https://orcid.org/0000-0002-3543-0743
DATA AVAILABILITY: Upon reasonable request, from Corresponding Author
FUNDING: The Occupational Therapy Association of South Africa (OTASA) requested the authors to do this rapid review and they were remunerated by the association

{kind=link}
{kind=link}
{kind=link}