










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.56 n.1 Pretoria Apr. 2026
https://doi.org/10.17159/2310-3833/2026/vol56no1a3
RESEARCH ARTICLES
Content and item validity of the self-care inventory for children with cerebral palsy living in a resource-constrained context in KwaZulu-Natal
Julia BurgI, ; Gillian SaloojeeII; Patricia Ann de WittIII; Denise FranzsenIII
IMoveAbout Therapy Services: 304/14 Lexington Dr, Berkeley Vale, New South Wales, Australia. https://orcid.org/0000-0003-2653-2104
IIDepartment of Physiotherapy, Faculty of Health Sciences, University of the Witwatersrand, 7 York Rd., Parktown, Johannesburg, Gauteng, South Africa. https://orcid.org/0000-0003-1582-0151
IIIDepartment of Occupational Therapy, Faculty of Health Sciences, University of the Witwatersrand, 7 York Rd., Parktown, Johannesburg, Gauteng, South Africa. https://orcid.org/0000-0003-3612-0920; https://orcid.org/0000-0001-8295-6329
ABSTRACT
INTRODUCTION: Children with cerebral palsy (CP) usually struggle with self-care activities. Occupational therapy self-care assessment tools for children with CP may not accommodate all South African contexts. This study aimed to determine item criteria and content validity for the Self-Care Inventory for Children with Cerebral Palsy (SCICP), for use in resource-constrained contexts
METHODS: Using an instrument design methodology, the International Classification of Function, Disability and Health (ICF) was used to map items from existing self-care assessments for children, which were categorised into the SCICP. Subject matter experts completed a content validity index (CVI) on the SCICP, which was translated into isiZulu. The items were further evaluated by caregivers of children to ensure cultural relevance and the age of independence in items by typical children
RESULTS: Of the 197 items, 88 were discarded and 16 were edited due to ambiguity and contextual relevance. Adequate CVI values ranged from 1.00 to 0.82 for the six sections on the SCICP, with limited consensus on the age of independence for self-care tasks
CONCLUSION: This study presents the first stage in the development of the SCICP, which requires further testing for validity and reliability to confirm its suitability before use in the South African context
IMPLICATIONS FOR PRACTICE: This study focused on the first stage of the development of the Self Care Inventory for Children with Cerebral Palsy (SCICP), which has the potential to become a standardised, usable assessment tool for use within resource-constrained areas of South Africa. A pilot study to confirm the other psychometric properties of the SCICP as a contextually relevant assessment for use in South Africa is required before the assessment can be used clinically
Keywords: good health and wellbeing, culturally and contextually, appropriate occupational therapy assessment, self-care inventory for children with cerebral palsy (SCICP), International Classification of Function, Disability and Health (ICF)
INTRODUCTION
In South Africa, standardised occupational therapy assessments are essential due to the diverse cultural, socioeconomic and linguistic differences1,2 of the persons needing occupational therapy. Assessments developed in the Global North are commonly used, but they require adaptation and careful interpretation to be relevant and effective for South African populations3,4. Occupational therapists are increasingly aware of the need for context-specific assessments that acknowledge potential biases5. According to de Sam Lazaro, authentic assessments for young children should be more family-centred and function-based6 within the environment in which the child naturally performs skills, such as self-care7.
A critical developmental outcome in young children is independence in self-care. However, many factors influence the rate and nature of this independence, including culture, family values and expectations, environmental context, physical and psychological capacity, as well as the motivation to engage8. Independence in self-care as well as other activities of daily living (ADL), as identified in the Occupational Therapy Practice Framework VI (OTPF IV)8 from the basis of competence in occupational performance within many contexts of daily life9. Thus, an appropriate, contextually and culturally relevant and language accessible assessment is needed to determine the nature and extent of these challenges to direct intervention required to improve self-care intervention and self-care outcomes.
In many instances, occupational therapists working in resource-constrained contexts in South Africa use internationally developed standardised assessment tools10 to determine intervention needs11. However, ADL tools for children with disabilities, including the Pediatric Evaluation of Disability Inventory (PEDI)12 the Functional Independence Measure for Children (WeeFIM)13, the Bayley Scales of Infant and Toddler Development (Adaptive behaviour)14, the Independent Living Skills Assessment Tool15 and the Activities for Kids (ASK)16 are not standardised for South Africa. Thus, available assessments are not culturally relevant since they do not consider the variations in self-care activities, which are required for the assessment of ADL in resource-constrained areas1, where piped water, indoor plumbing, reliable electricity and electrical appliances are not available.
The need for a more contextually appropriate self-care assessment for children living in resource-constrained settings is supported by a number of researchers1,17. Such a multicultural assessment, which may be norm-referenced, should consider the parents' understanding and expectations of their child's ability in the assessment process. The assessment should be available in the language most appropriate for the parents and should be interpreted in relation to the child's development within the cultural expectations18. It is important for clinically useful assessments to consider an interpretation of the context, cultural differences and an analysis of the child's disability, with caregivers assisting with the evaluation, so assessments cannot simply be translated for use in South Africa.
Available assessments of self-care that have been developed to evaluate young children with disabilities also do not consider children with specific deficits based on classifications such as the Gross Motor Function Classification System (GMFCS), Manual Ability Classification System (MACS), which are specifically utilised for children with cerebral palsy (CP). Patel17 indicated the need for a context-specific self-care inventory for children with CP to provide evidence-based health care in developing countries, particularly for those living in under-resourced contexts where contextual and cultural factors influence how activities of daily living are performed and judged. Fuller19 and Avetisyan20 endorsed the need for a valid assessment for children with CP using an internationally recognized framework such as the International Classification of Functioning, Disability and Health (ICF)21. Such an occupational therapy assessment should consider activity limitations and participation restrictions as identified by the ICF19,21 which defines self-care as life tasks that are required for caring for the body and self-maintenance. Functional mobility action to complete the self-care tasks as indicated in the ICF19,21 should also be considered along with age-appropriate self-care tasks. The ICF is particularly relevant as the South African Department of Health22 has regulated that the ICF as part of the WHO-Family of Classifications, will be included in the standardised health terminology system reform for all medical coding and reporting in the country.
Thus, a new ADL assessment, the Self Care Inventory for Children with Cerebral Palsy (SCICP), was proposed, which considered young children with CP living in resource-constrained contexts in South Africa. An assessment for this group of children was considered critical in South Africa since the prevalence of CP is estimated to be higher than the global average, with rates up to 10 per 1,000 live births23. Also, due to the interaction between poverty and limited accessibility to health and rehabilitation resources, children with CP from these contexts rarely receive appropriate early and ongoing therapy19,24. Occupational therapy services are seldom provided more than once a month, thus, accurate assessment to support appropriate home programmes is required19. Since existing standardised assessments are expensive and rarely available to occupational therapists in the public sector primary health care clinics25, a valid, reliable, culturally applicable, low-cost assessment tool will support occupational therapy intervention in improving independence in self-care, specifically for children with CP, in resource-constrained South African contexts.
In line with existing Paediatric ADL assessments12,13 and suggestions for cross-cultural adaptation of outcome measures in South Africa26, a norm-referenced, caregiver report format on the child's performance was considered suitable for the assessment of self-care. Optional observation of the child completing tasks by the therapist as an adjunct to support problem formulation and intervention was suggested. The assessment would be available in languages commonly spoken in South Africa26.
The development of a new assessment tool is, however, complex27-29. Once decisions on the need for the assessment, the target population had been identified and how a construct such as self-care could be measured, several critical steps were required, which include: clearly defining the constructs and developing the items, as well as establishing response options and scoring. Item and content validity need to be established before pilot testing of the instrument's psychometric properties and determining normative data29. Davis30 emphasised that the assessment needs to be appropriate for functional clinical intervention and outcome evaluation. This study reports the initial stages in the development of a new self-care assessment tool to be used for children with CP living in resource-constrained contexts within South Africa. The purpose was thus to establish criteria for items to be included in the new assessment tool, which were contextually and culturally relevant, as well as to establish the item and content validity for the assessment tool31.
METHODS
The research design used in this study was a methodological research design that focused on systematically designing, testing, and validating a new assessment tool32, named the Self Care Inventory for Children with Cerebral Palsy (SCICP). This was completed in two stages, which covered two steps in the instrument design process:
Target population
Stage 1 of the study aimed to specify the constructs of self-care as well as the functional mobility demanded to complete the self-care tasks completed by typical preschool children from birth to 6 years 6 months. Once it was established how and at what age typical children performed activities of self-care, children with CP can be assessed to determine delay and the need for intervention. These self-care tasks will be assessed in children with CP, irrespective of their age, for all different levels of severity of CP as identified by the GMFCS and MACS to determine their skills and functional mobility relative to self-care achieved by typical children. The performance of the child with CP could be compared to the expected self-care for any age group to determine if a delay was present and intervention was required.
The assessment of functional mobility was included since CP is classified according to the predominant motor deficits33 and therefore movement such as walking, carrying and lifting, are all essential for independence in self-care tasks, and thus need to be assessed34. The amount of caregiver assistance required, as well as differences according to the socio-cultural and socio-economic context in which the tool would be used, will be considered to include self-care methods not covered by current ADL assessments, which do not accommodate cultural differences experienced in under-resourced contexts1.
Definition of Self-Care Constructs
The SCICP was based on the WHO ICF21. The ICF considers health conditions according to body functions and structures, activities and the restrictions to participation in society. The ICF also stresses the importance of the environment when considering the activities of daily living. This universal framework covers domains for the codes related to self-care (Chapter 5) and functional mobility required to achieve the self-care codes (Chapter 4), within the Activities section. Mapping of the ICF domains and codes allowed for potential items to be included or excluded within the subcategories for each self-care activity listed and the functional mobility required. The development in self-care, specifically noting the developmental sequence of independence in self-care skills of typical children35, was also considered.
Item development
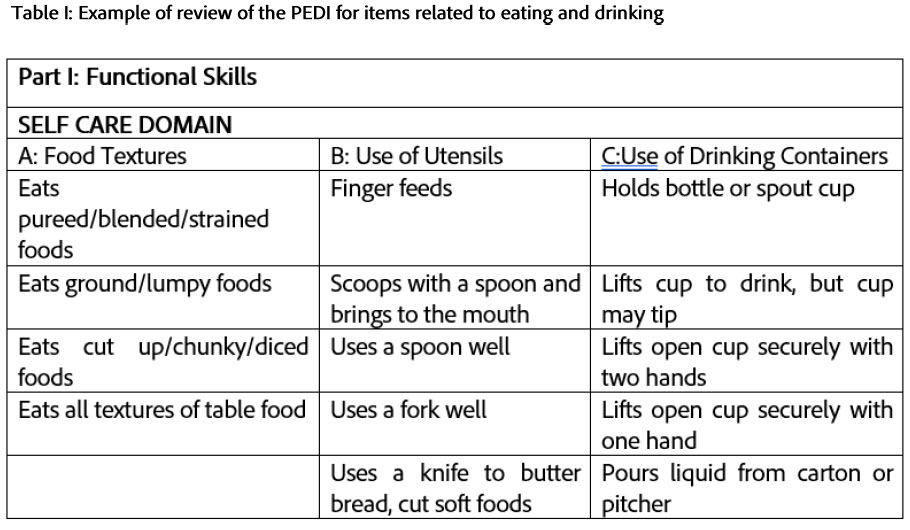
All items for the SCICP were developed by the researcher using the item domain areas based on the ICF and the codes given to relevant activities relating to self-care as per the chapters on Activities and Participation. Item subdomains within the following codes were considered for inclusion: Self-care (d5) - including washing (d510), caring for one's body parts (d520), toileting (d530), dressing (d540), eating (d550), drinking (d560); while mobility considered changing and maintaining body position (d410-429), carrying, moving, and handling objects (d430-449) and walking (d450). An initial item bank for each self-care domain was developed from the following existing assessments of self-care for children, which provided an indication of self-care tasks and the ages (summarised in 1-year intervals) at which typical children mastered these tasks.
-
Pediatric Evaluation of Disability Inventory (PEDI)12 (Table I, below).
-
Functional Independence Measure for Children (WeeFIM)13
-
Bayley Scales of Infant and Toddler Development (Adaptive behaviour)14
-
Independent Living Skills Assessment Tool15
-
Activities for Kids (ASK)16
-
Primary Progress Assessment Chart of Social Development36
-
Oregon Project for Visually Impaired and Blind Preschool Children37
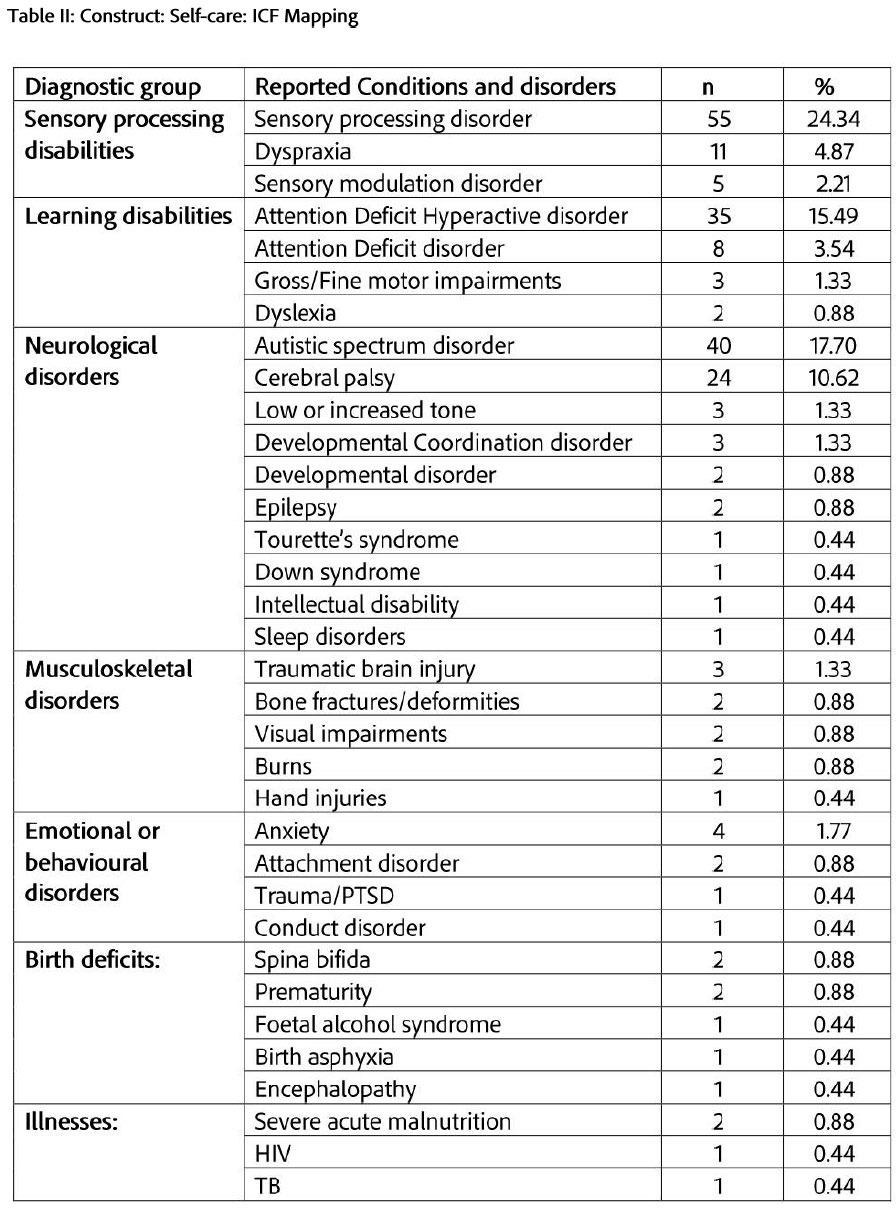
Items were included if they were identified as being achieved by typically developing preschool children between birth and 6 years 6 months, and if they required a functional mobility action to complete the self-care task, and if these two components could be linked to an ICF code. The first step in Stage 1, therefore, involved the selection of items from seven existing self-care assessment tools and categorising them according to the self-care and mobility domains of the ICF. Six domains from the ICF were found to be associated with self-care and functional mobility. For the SCICP, the ICF domains were used as it was or clustered together and renamed. Washing (d510) Eating and drinking (d550 and d 560) were combined into one section and caring for body parts was renamed as grooming (d520). The seven ICF domains (d410, d415, d420, d430, d440, d445, d 450) related to mobility were renamed Functional mobility associated with eating and drinking, washing, dressing, grooming, toileting and General functional mobility. The wording of items was carefully considered as suggested in the study by Bornman et al.38, in that many of the words used in international self-care assessments are not commonly used within South Africa. Thus, words such as "zippers", "pullover garments", "closet", "diaper", "tub" required consideration in terms of context and language. A total of 318 items from the assessments were mapped according to the ICF domains and codes. These ICF items were reduced to 206 items by excluding duplications and grouping of similar tasks (Table II, below).
Scoring and administration
Although administration guidelines were still to be developed for the caregivers, therapists and children it was planned that the caregiver would first report on whether the child was able or unable to complete an item on the SCICP on a four-point scale ranging from being unable to do the task (1) to being independently able to do the task (4). This scale is similar to other paediatric independence assessments. Then the therapists could ask the child to perform the item to observe and rate the child's actual performance on the same scale if the caregiver was unsure about the child's skills and record aspects such as speed of performance, quality of the task, compensation used, and assistance needed in the comments section. Items required for most self-care tasks are usually available in the occupational therapy department or the child's home, depending on where the assessment occurred.
The SCICP was designed for each self-care domain to be assessed separately according to caregiver concerns, and the full assessment does not need to be completed at one time, since completing all domains on the assessment requires 45 minutes to administer. It was intended that the assessment be freely accessible to occupational therapists, to be low-cost and be available in several South African languages.
Matafwali et al.31 identified that certain biases affect the usefulness of assessment tools that have not been developed for target populations, such as cross-cultural bias, method bias, construct bias, as well as sample and administration bias. Thus, to avoid biases and irrelevant and inappropriate items in the SCICP, content validity, to ensure relevance and clarity of the items, needed to be established. In addition, the item analysis of the SCICP also aimed to establish whether the sections and items selected accurately represented self-care and functional mobility applicable to typical children within resource-constrained areas of South Africa.
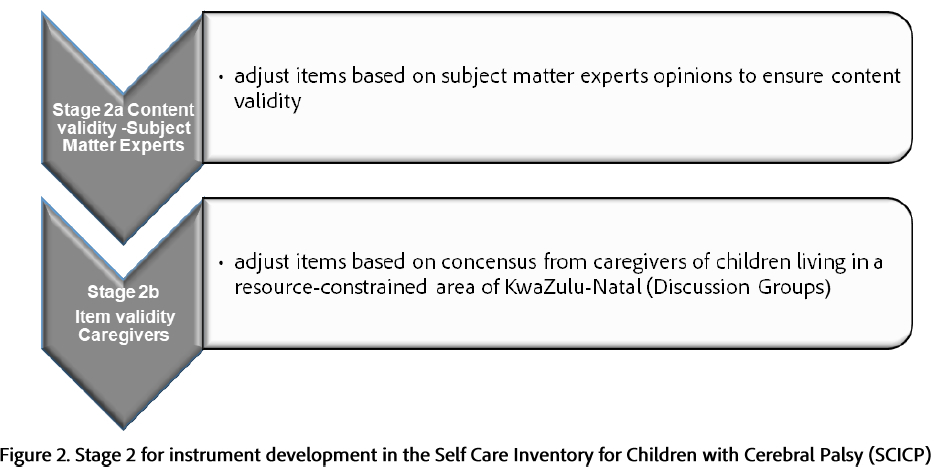
Stage 2a: Review by subject matter experts (SME)
The population for this review was paediatric occupational therapists who were all familiar with and had worked with children with CP in rural resource-constrained contexts in South Africa. They were considered experts as they had at least ten years' experience in the field39. A purposive sample of ten occupational therapists considered to be subject matter experts (SMEs) was identified using the database of Malamulele Onward, a non-profit organisation providing therapy to children with CP in resource-constrained contexts. Of the ten SMEs invited, three agreed to critically examine and suggest revisions to the items on the SCICP40 according to content relevance and clarity of items for typical children up to 6 years and 6 months, or whether the item needed rewording, or to be discarded. They were provided with a template suggested by Yusoff41 for establishing a content validity index (CVI) for each item. The process for determining a CVI was based on the method suggested by Davis30 and the level of acceptance for items was set at 0.83. Once items were analysed, the SMEs were asked to evaluate all edited items for relevance and clarity using the same content validity template.
Stage 2b: Review by Caregivers of Children Living in Resource-Constrained Areas of KwaZulu-Natal (Discussion Groups)
Study context
The study site for the review of items on the SCICP by caregivers of typical children was Nquthu, in the Umzinyathi Health District of KwaZulu-Natal. Nquthu is considered a deep rural area of the district, which has a mountainous topography and poor basic infrastructure42. The most common language and culture in this area is isiZulu. There is seldom running water and ablutions within the homes and bathing is usually done from a bucket or aluminium bath. Many homes have pit toilets in the yard. A few homes have electricity, but most cooking is over an open fire or using a paraffin stove. Meals are often eaten using the right hand or with a spoon, sitting on benches or on mats on the floor. Water also needs to be collected from communal taps in the community. Health resources are limited and usually far from homes, with limited transport options restricting access. This context is like many resource-constrained areas in South Africa where community rehabilitation services are delivered.
For stage 2b of the study, the SCICP was translated into isiZulu by a professional translator, with more than 20 years of experience in translation and was back translated by a research assistant who worked with caregivers of children with CP and who was familiar with the project. Participants were defined as caregivers if they met the inclusion criteria of being parents, grandparents, or primary caregivers of typically developing children, irrespective of their level of education, living in the study site. If they met these criteria, they were invited to participate in the discussion groups43. These individuals were considered experts due to their experience in raising children within the resource-constrained context. This methodology, although not commonly reported, was used by Abubakar et al.44 in resource-constrained areas of Kenya, for the development of their milestone monitoring assessment.
The input from the discussion group contributed to the cultural relevance of the SCICP. A research assistant, a local disability facilitator and parent liaison officer, invited members of the Nquthu community to participate in discussion groups at the Philani Drop-In Centre. It was only possible to recruit and pay the transport costs of a total of 20 participants based on available research resources. These participants were included in two discussion groups with 10 participants as suggested by Nyumba et al.45. The research assistant was trained by the first author to facilitate the discussion groups. The research assistant presented each item verbally in isiZulu to the discussion groups. It was explained to participants that they would need to indicate if each item on the SCICP was relevant and should be retained or discarded. The wording of each item was then considered for clarity. Participants were asked to indicate in month and year intervals, the age at which independence is usually achieved for each activity as it was presented to them. This was discussed and the agreement by eight out of 10 group participants was accepted as a final decision for all aspects. Each discussion group was audio recorded for later analysis and confirmation of the data by the researcher and research assistant.
Data Analysis
Demographic data were analysed using descriptive statistics. The content validity was established for the items if the universal agreement (CVI-UA) between the experts41 and items were retained if they achieved a CVI of 0.83, which Davis30 indicated was acceptable for two to three experts. For the discussion groups, items were retained if 80% consensus46 was achieved (i.e., yes or no) on the relevance and clarity of the item and the age at which independence was reached. Following the content and item validity reviews, adjustments were made to the items that did not achieve the cutoff to be retained, and items were deleted if the CVI was below 0.75 or consensus was less than 70%. Comments made by the SMEs and discussion groups were also analysed and considered when editing and adjusting items.
Ethical considerations
Ethical clearance for the study was obtained from the Human Research Ethics Committee of the University of the Witwatersrand (ethical clearance M 20361). An approved information sheet was circulated to all participants in an appropriate home language. The information sheets, one for the experts and the other for the caregivers, indicated the purpose of the study, that participation was voluntary, and that participants could discontinue participation at any point. Consent was assumed from the participants who completed the online survey (Stage 2a) and signed consent, or a thumbprint was provided by participants of the discussion groups for participation and audio recording (Stage 2b). Participants were informed before the discussion groups that confidentiality could not be ensured in the discussion groups, but no names or identifying data would be used in the data analysis and reporting of the research.
RESULTS
Stage 2: Content validity
Stage 2a: Review by subject matter experts
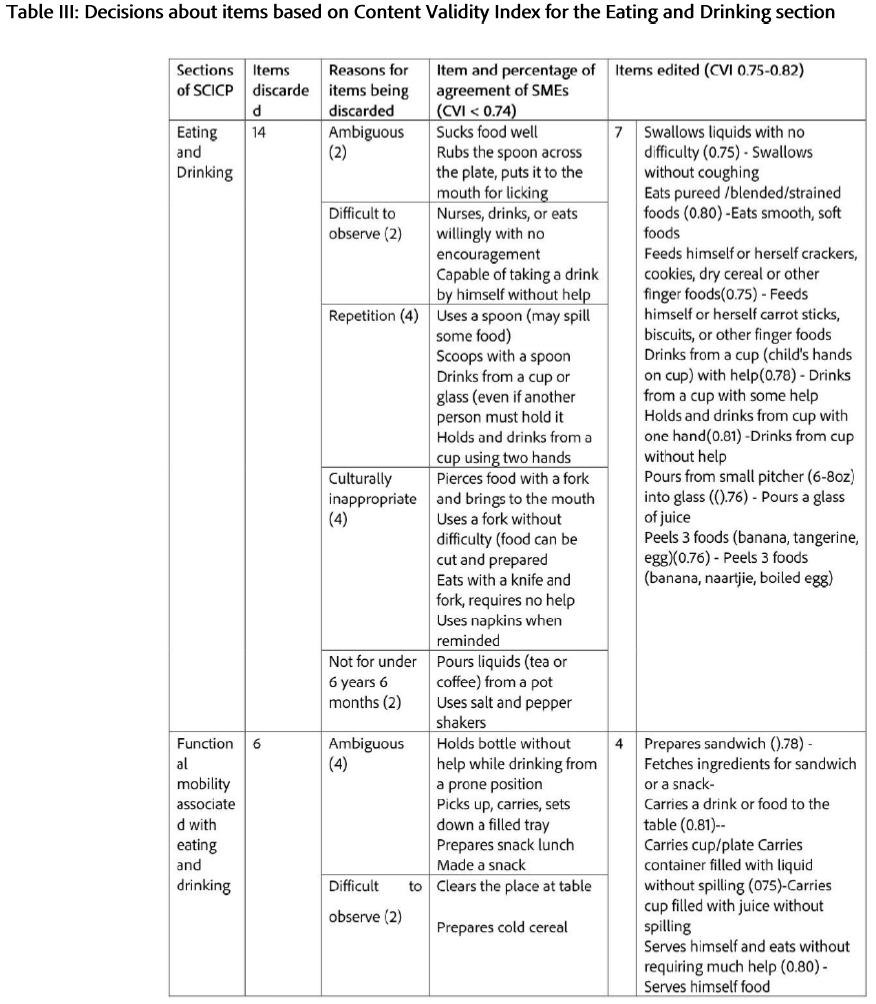
Results for all 206 items on the SCICP were analysed by three SMEs for content validity. Table III describes the results within the Eating and Drinking section. As indicated above, items were retained with a CVI at 0.83 and 14 of 36 items with a CVI of <0.74 and below were discarded. Two of these items were considered ambiguous, two were difficult to observe, four were repeated, four were culturally inappropriate, and two did not apply to typical children up to 6 years 6 months. In the Functional mobility associated with eating and drinking section, another six items were discarded for being considered ambiguous and two were difficult to observe. A total of 11 items with a CVI of between 0.75 and 0.82 were retained, of which seven were edited (Table III, below). The edited items all achieved a CVI of 0.83 when rereviewed by the SMEs.
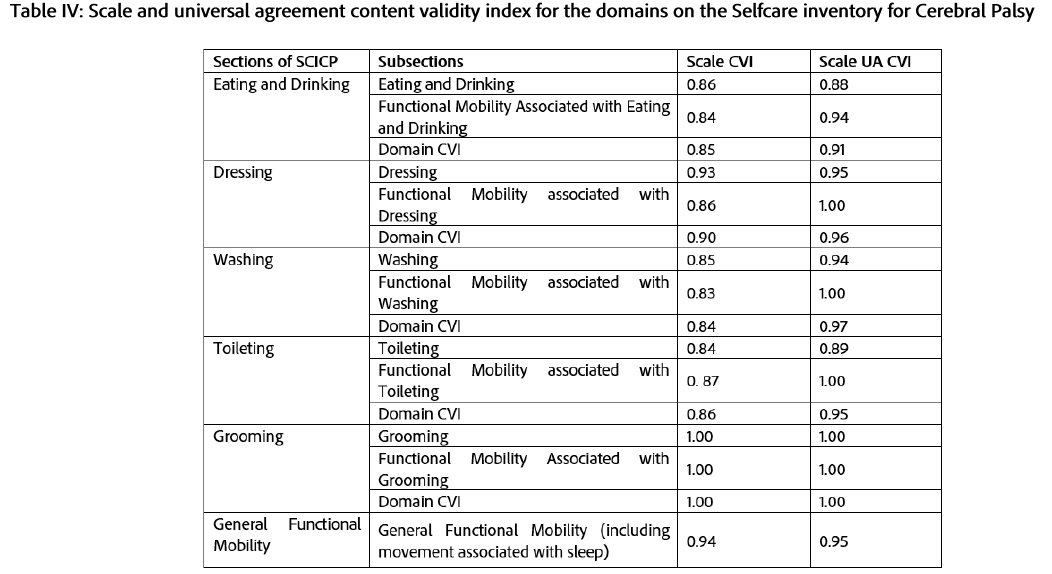
The changes to the other five sections of the SCICP followed the same process as detailed in Table III (page 6). All items were listed and either accepted, discarded or changed with a justification based on the same CVI levels. The reasons for deleting and editing items were mainly due to ambiguity, repetition, irrelevance to age or culture and difficulties in observing the item. A total of 84 of the 206 items were deleted, and 21 were edited. Many of the items discarded were for Dressing, while a few changes were made to the Washing, Toileting and Grooming sections. The General Functional Mobility section was reduced to nine items. The scale CVI and scale of universal agreement (SUA CVI) on the 122 items retained were reviewed again by the SMEs, are presented for each domain of the SCICP in Table IV (below).
Stage 2b: Review by Caregivers of Typical Children Living in a Resource-Constrained Area of KwaZulu-Natal (Discussion Groups)
The 122 items retained in the SCICP, which had been translated into isiZulu were presented to the participants in the discussion groups, who verbally reviewed each item and reached consensus within the group as to whether the item was appropriate or not for evaluating self-care of children living in a resource-constrained context. The groups included 12 mothers, five grandmothers and three primary caregivers of the children who resided in the area. The participants were between the ages of 22 and 58 years. The results for the Items from the discussion groups were analysed and those that obtained 80% consensus as relevant were retained46. Items that obtained 80% agreement for relevance but were unclear were edited and the items that participants agreed were irrelevant for children up to 6 years and 6 months, culturally inappropriate, were not observed by caregivers, or the same as other items were deleted. Comments recorded in the discussion groups were analysed and the items were edited and adjusted according to participants' input.
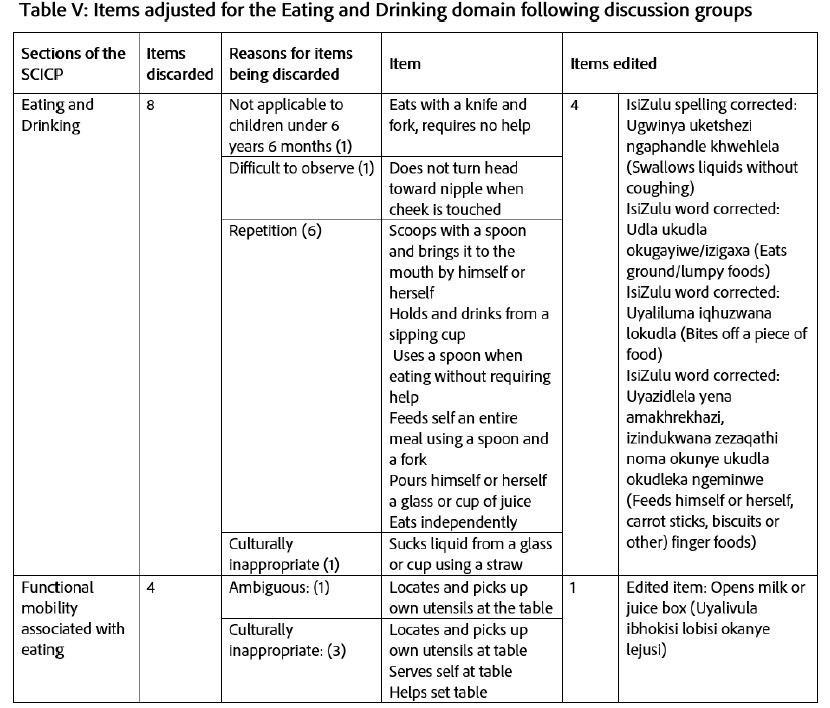
As indicated in Table V (below), eight further items within the Eating and Drinking section and four from the functional mobility associated with these aspects of self-care were discarded. Over the entire eating and drinking and functional mobility for eating and drinking, one item was not considered applicable to children under 6 years 6 months, one was ambiguous, one was difficult to observe, six were found to be repeated and four were culturally inappropriate.
Other items were adjusted in terms of cultural relevance, and the wording of certain items in IsiZulu was modified. The adjustments were verified by the local disability facilitator research assistant, who was Zulu-speaking. A similar process of analysis was followed for the other four sections of the SCICP, and following the discussion groups, no other deletion was made, so the final number of items in the SCICP was 109.
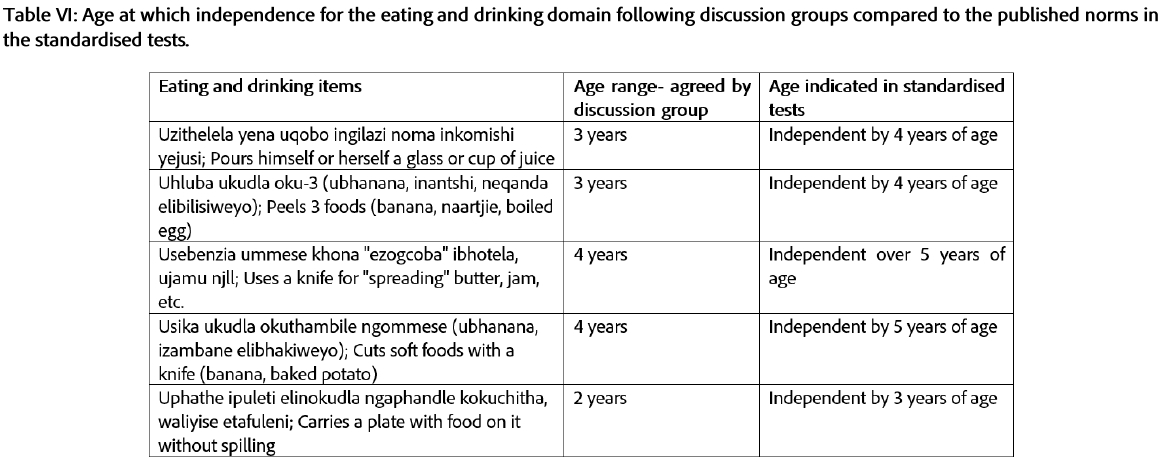
The consensus reached on the age of independence for the items by the participants in the discussion groups differed from the norms published in the assessments on which the SCICP was based. Table V indicates examples of the ages at which independence occurred according to the caregivers in the discussion groups. For some Eating and Drinking items on the SCICP, caregivers indicated independence as either earlier or later than the published norms in the standardised tests.
The same age within six months for independence in self-care tasks described on the SCICP was identified for 58 of the 109 items (53%) by the discussion group participants when compared to the age indicated in standardised tests. Twenty-one of the 109 items (19%) were identified as having independence achieved a year earlier by the discussion group participants. Standardised tests indicated that children achieved independence in the other 30 items (28%) up to a year earlier than was indicated by discussion group participants.
DISCUSSION
Content and Item Validity
The content of items on the SCICP was undertaken using a SME review47. The input of the SME's considered both self-care tasks and appropriateness for resource-constrained contexts. The SCICP was reduced from 206 to 122 items based on the comments and opinions of the SMEs were accepted in the adaptation and development of assessments for different contexts in low-middle-income countries (LMIC) in other studies31,38. Matafwali et al.31 indicated that bias might be introduced when an assessment is administered across different cultures if there is a lack of accommodation for accepted practices in the performance of ADLs, as in the current study. In this study, many items were deleted as they were considered inappropriate for the isiZulu culture and resource-constrained settings where the study was carried out. Some items were reworded because, as indicated by Bornman38 the participants did not use some items, such as a knife and fork, or they were inappropriate in the local language and resource-constrained settings. Items that were identified as repetitive or assessing the same aspects of an activity were discarded. This occurred as the description of certain activities like eating with a spoon was assessed in slightly different ways, such as "Scoops with a spoon and brings to the mouth by himself or herself", "uses spoon when eating without requiring help", or "feeds self an entire meal using a spoon".
The discussion groups were also used to ensure validity for the items on the SCICP by consulting with those caring for typical children in the target population. Parents, grandparents, or primary caregivers with experience of raising children from the context in which the assessment would be used were recruited as participants with expert knowledge of child development. This supported the suggestion by Abubakar et al.44 that different types of experts were useful in establishing the validity of test items. The consultation with the caregivers of children, although not common, has been described to enhance item development. The use of the discussion groups in contributing a view on the cultural relevance and age appropriateness of items on the SCICP was supported by Vogt et al.48 who advocated for the use of groups rather than individual interviews in reaching consensus.
The caregiver discussion yielded valuable information that contributed to the item review and validity of the SCICP. The participants commented on the cultural relevance and whether the items would be valid within the resource-constrained South African context. Items inappropriate to culture included: "Sucks liquid from a glass or cup using a straw", "Uses a fork without difficulty", "Helps set table", "Takes a bath or shower without help" and "Steps into and out of adult-sized bath". The reason behind this was that within the isiZulu culture and the resource constraints in their context, these items described actions that the children do not do, and/or included equipment/ facilities they do not have.
Participation in the two discussion groups varied, which affected the input received from all participants. The caregivers within the first group felt more comfortable expressing their opinions to the translator and researcher and the opinions of the quieter caregivers had to be facilitated so all members could come to a conclusion on the items. Comparatively, the second group of caregivers was more cohesive and able to discuss their opinions and come to a conclusion independently. Although there were concerns about the first group in the first session, the cohesion attained in the second session and in the second group of caregivers made the process valid, with discussion and decision-making shared in providing the information required.
A concern in the groups was that ambiguity about the items may have arisen through the translation of the SCICP into isiZulu, even though this was done using the approved back translation method. It appears at times that the action, such as holding the washcloth to achieve the task, rather than the task of washing, was described. Words used by the translator were not always the words commonly used within Nquthu, or the specific dialect of isiZulu used in this context. The caregivers explained the need for language changes, including: "kokukhohlela" changed to "khwehlela". Both words mean cough or coughing, but "khwehlela" is the word used within this specific community, highlighting the importance of obtaining comments from those in the context where the assessment will be used.
Validity - age of independence
Many factors influence a child's performance of self-care and how and when it develops, resulting in variance seen in the age of independence. These factors can include the child's physical environment, specific demands of the activity, parents' expectations and caregiver responsiveness, cultural values and social routines49,50. This is because the achievement of developmental milestones and acquisition of new skills are dependent on the sensory and motor systems, cognitive, emotional and social development49.
In developing the domains, items and structure of the SCICP, the developmental level of children was considered as indicated in the standardised assessments12,13-37 and analysed for item development in the study. The SMEs and caregivers of typical children were also asked to comment on the appropriateness of the items for children 6 years and 6 months or younger. The SMEs aided in establishing the content validity of the SCICP's items due to their contribution in terms of knowledge of the theory of child development and self-care and their experience in working in resource-constrained contexts. They identified items that were deemed inappropriate due to age, such as: "Pour liquids (tea or coffee) from a pot" and "Styling hair". These items were expected of children older than 6 years and 6 months, which was why they were excluded.
Even within a specific culture and similar physical environment, variation in the achievement of independence of self-care skills was evident. Development of independence in a self-care skill is achieved through many hours of practice49. Therefore, although there was agreement between the ages of independence for more than half the items reviewed in the discussion groups, age differences were reported for numerous other items. These items were given an earlier or later age for expected independence and may reflect variation expected in achieving independence in ADLs, confirmed by this information. Other research in Africa by Abubakar et al.44 and Gladstone et al.51, that used caregiver reports of independence in ADLs can be considered reliable and valid. However, further validity needs to be ensured by observations of typical children in their context to confirm the age of independence for items on the SCICP.
Independence was reportedly achieved earlier for items such as putting on and fastening clothes, cleaning up spills, carrying plates of food, peeling and eating fruit, using a knife to spread or cut fruit and general functional mobility. Caregivers reported achieved independence at an older age for doing up fastenings on clothes, putting on shoes, brushing hair, washing the whole body, emptying the basin after washing, cleaning the basin and using an adult toilet and toilet paper. The only item considered inappropriate to age, which was excluded, was "Eats with a knife and fork, requires no help". Caregivers explained that within their culture, they use their hands and spoons to eat a meal. They felt that it was inappropriate to expect their children to eat with a knife and fork, however, this is only expected later in the child's life when they may be in situations that have other cultural norms.
The SCICP aimed to identify the unique profile of each child's functional ability cognisant of their under-resourced and cultural context, allowing for intervention of their functional abilities over time52. Contrary to other assessments, such as the Peabody Developmental Motor Scales (PDMS-3)53 which are reflected within intervals of one month for the first one or two years and then in bigger intervals of six or twelve months, the SCICP accommodated changes in function that occur initially on a 12-month basis. This reflected independence in self-care items, most of which do not develop in the first year of life and which require being able to move and fetch items in the environment. Functional mobility items were included for all domains on the SCICP. The importance of assessing functional mobility in the SCICP was confirmed by Kim et al.54 who indicated the lack of independence in self-care in children with CP is often dependent on assistance for mobility. They found that on the PEDI, mobility was the only factor that significantly influenced self-care in children with CP aged younger than 6 years 6 months54.
Limitations to the study
This content validity study was limited to three SME occupational therapists, which was the minimum number acceptable for this part of the study. The items were based on existing standardised tests from the Global North, and the age for independence provided may differ in the SCICP due to different occupational forms in carrying out ADLs and the broad age intervals of 1 year used to determine independence in self-care tasks.
CONCLUSION
This study described the first stage in the development of a tool to measure self-care performance in children with CP living in resource-constrained settings in South Africa. The sections and items included in the SCICP were conceptualised and specified through a literature review and analysis of existing standardised assessments of ADL for children. The SCICP sections align with occupational therapy domains, which include the functional ability to engage in and master the development process associated with ADL, such as self-care and grooming and functional mobility, which was included since CP is defined as a condition permanently affecting body movement33. This is the first measure of its kind and, once complete, offers the potential for a useful assessment tool with the ability to draw meaningful inferences regarding self-care independence in children with CP living in resource-constrained contexts. The results of this study highlight the initial content validity of the assessment to be used to correctly identify occupational therapy intervention goals for children with CP who have challenges in the independence of self-care.
Recommendations
For the SCICP to become a standardised, usable assessment tool for use within resource-constrained areas of South Africa, further testing of other forms of validity and reliability is necessary. A pilot study using a larger sample of both typically developing children and children with CP will allow a better understanding of the criterion validity of the SCICP for children on each level of the GMFCS and the MACS. This will provide an understanding of the assessment of self-care in this highly diverse group, with variations in the type and severity of their motor, manual and other associated disabilities.
Author Contributions
Julia Burg conceived the study and carried out the research supervised by Gillian Saloojee and Denise Franzsen. Pat de Witt and Denise Franzsen conceived and wrote the article based on the research The article was checked and edited by Julia Burg and Gillian Saloojee. All authors approved the final version of the manuscript.
Conflict of interest
There are no conflict of interests to declare.
Funding
No funding was received for the study.
AI declaration
AI was not used in the creation or review of this article.
REFERENCES
1. McAdam JC, Franzsen D, Casteleijn D. Identification of occupations in a South African rural less-resourced community. Journal of Occupational Science, 26(3), pp.379-393. Journal of Occupational Science. 2019;26(3):379-393. doi: https://doi.org/10.1080/14427591.2019.1614476 [ Links ]
2. Oakland T, Wechsler SM, Maree K. Test use with children across cultures: A view from three countries. In: Geisinger K, Bracken B, Carlson J, Hansen J-I, Kuncel N, Reise S, Rodriguez C, editors. APA handbook of Testing and Assessment in Psychology, Vol. 3. Testing and assessment in school psychology and education. American Psychological Association; 2013. p. 231-257). doi: https://doi.org/10.1037/14049-011 [ Links ]
3. Naude S, Uys CJE, Bekker BM. Cross-Cultural Adaptation of the Administration Instructions of the Developmental Test of Visual Perception 3rd Edition for isiZulu-Speaking Children. South African Journal of Occupational Therapy. 2023;53(3):54-64. doi: https://doi.org/0.17159/2310-3833/2023/vol53n3a7 [ Links ]
4. Pretorius B. Standardised assessment: The crucial first step towards evidence-based practice. South African Journal of Occupational Therapy. 2023;53(3):1-2. doi: https://doi.org/10.17159/2310-3883/2023/volS3n3a1 [ Links ]
5. Rossier J, Duarte M. Testing and assessment in an international context: Cross-and multi-cultural issues. In: Athanasou H, Perera A, editors. International handbook of career guidance. Springer; 2019. p. 613-637. doi: https://doi.org/10.1007/978-3-030-25153-6_28 [ Links ]
6. de Sam Lazaro SL. The Importance of Authentic Assessments in Eligibility Determination for Infants and Toddlers. Journal of Early Intervention. 2017;39(2):88-105. doi: https://doi.org/10.1177/1053815116689061 [ Links ]
7. Bagnato S, Neisworth J, Pretti-Frontczak K. Linking authentic assessment and early childhood intervention: Best measures for best practices. 2nd ed. Baltimore: Paul H. Brookes Publishing Co; 2010. [ Links ]
8. American Occupational Therapy Association. Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy. 2020;74(Suppl. 2):7412410010. doi: https://doi.org/10.5014/ajot.2020.74S2001 [ Links ]
9. Chien CW, Brown T, Mcdonald R, Yu ML. The contributing role of real-life hand skill performance in self-care function of children with and without disabilities. Child: Care, Health and Development. 2014;40(1):134-144. doi: https://doi.org/10.1111/j.1365-2214.2012.01429.x [ Links ]
10. Akbas AN. Assessments and Outcome Measures of Cerebral Palsy. Cerebral Palsy - Current Steps. 2016. https://doi.org/doi:10.5772/64254 [ Links ]
11. Burgess A, Boyd RN, Chatfield MD, Ziviani J, Sakzewski L. Self-care performance in children with cerebral palsy: a longitudinal study. Developmental Medicine and Child Neurology. 2020;62(9):1061-1067. doi: https://doi.org/10.1111/dmcn.14561 [ Links ]
12. Haley S, Coster W, udlow L, Haltiwanger J, Andrellos P. Pediatric Evaluation of Disability Inventory (PEDI). Boston, Mass: New England: Trustees of Boston University, Health and Disability Research Institute; 1992. [ Links ]
13. Hamilton B, Granger C. Functional independence measure for children (WeeFIM). . Buffalo: Research Foundation of the State University of New York; 1991. [ Links ]
14. Bayley N. Bayley Scales of Infant and Toddler Development- Third Edition. San Antonio: Harcourt Assessment; 2006. [ Links ]
15. Washington State Department of Social & Health Services. Life Skills Inventory Independent Living Skills Assessment Tool. 2000;2016(24/04/2016). https://sites.google.com/site/transitionresourcesforteachers/home/--life-skills-inventory-assessment-tool [ Links ]
16. Young N. ASK Activities Scale for Kids. 2015;2016(24/04/2016). http://www.activitiesscaleforkids.com [ Links ]
17. Patel V. The need for treatment evidence for common mental disorders in developing countries. Psychological medicine. 2000;30(4):743-746. doi: https://doi.org/10.1017/S0033291799002147 [ Links ]
18. El-ghoroury NH, Krackow E. Enhancing the Identification of Autism Spectrum Disorders via a Model of Culturally Sensitive Childhood Assessment. 2012;43(3):249-255. doi: https://doi.org/10.1037/a0027354 [ Links ]
19. Fuller L. Occupational therapy for children with severe cerebral palsy in government healthcare facilities in the Western Cape: an overview of current services. University of Cape Town; Masters 2021. https://open.uct.ac.za/server/api/core/bitstreams/70007a2e-d66f-47ad-b219-a6517e01dc4a/content [ Links ]
20. Avetisyan M. WHO ICF as an assessment tool for evaluation of selfcare activities of the child with Cerebral Palsy. Armenian Journal of Special Education. 2021;5(1):49-65. doi: https://doi.org/10.24234/se.2021.3.1.259 [ Links ]
21. World Health Organization. The International Classification of Functioning, Disability and Health. 2001. doi: https://doi.org/10.1097/01.pep.0000245823.21888.71 [ Links ]
22. Rebublic of South Africa. Notice of intention to introduce health terminological systems in terms of section 74 of the National Health Act, 2003 (act no. 61 of 2003): coordination of National Health Information Systems. Government Gazette No 51362. https://gazettes.africa/akn/za/officialGazette/government-gazette/2024-10-01/51362/eng@2024-10-01 [ Links ]
23. Donald K, Katangwe TJ, Springer PE, Solomons RS, Van Toorn R, Steel S, Kruger M. A South African cerebral palsy registry is needed. South African Medical Journal. 2020;110(5):353-354. [ Links ]
24. Saloojee G, Phohole M, Saloojee H, Ijsselmuiden C. Unmet health, welfare and educational needs of disabled children in an impoverished South African peri-urban township. Child: Care, Health and Development. 2007;33(3):230-235. doi: https://doi.org/10.1111/j.1365-2214.2006.00645.x [ Links ]
25. Moosa A, Gurayah T, Karim SB, Govender P. Occupational therapy assessment and interventions for young autistic children in South Africa. African Health Sciences. 2023;23(1):725-735. https://doi.org/doi:10.4314/ahs.v23i1.77 [ Links ]
26. de Klerk S, Lesch HM. Community translation in the context of the translation and cross-cultural adaptation of patient reported outcome measures: a South African perspective. South African Journal of Occupational Therapy. 2021;51(2):104-106. doi: https://doi.org/10.17159/2310-3833/2021/vol51n2a14 [ Links ]
27. McCoach D, Gable R, Madura J. Instrument development in the affective domain. . New York: Springer; 2013. [ Links ]
28. Laver Fawcett A. Principles of Assessment and Outcome Measurement for Occupational Therapists and Physiotherapists: Theory, Skills andFawcett A: Principles of Assessment and Outcome Measurement for Occupational Therapists and Physiotherapists: Theory, Skills and Applicati. 2nd Editio. New York: John Wiley & Sons; 2013. [ Links ]
29. Davis SL, Morrow AK. Creating usable assessment tools: A step-by-step guide to instrument design. Hamsonburg; 2004. [ Links ]
30. Davis LL. Instrument review: Getting the most from a panel of experts. Applied Nursing Research. 1992;5(4):194-197. doi: https://doi.org/10.1016/S0897-1897(05)80008-4 [ Links ]
31. Matafwali B, Serpell R. Design and Validation of Assessment Tests for Young Children in Zambia. In: Serpell K. R. M, editor. Child development in Africa: Views from inside. Vol. 146. Wiley Periodicals, Inc.; 2014. p. 77-96. [ Links ]
32. Polit D, Beck C. Essentials of nursing research: appraising evidence for nursing practice. . 9th ed. Philadelphia Wolters Kluwer: Wolters Kluwer; 2018. [ Links ]
33. Baxter P, Morris C, Rosenbaum P, Paneth N, Leviton A, Goldstein M, Bax M, Colver A, Damiano D, Graham HK, et al. The Definition and Classification of Cerebral Palsy Contents Foreword Historical Perspective Definition and Classification Document. Developmental Medicine & Child Neurology. 2007;49(109):1-44. [ Links ]
34. Edemekong PF, Bomgaars D, Sukumaran S, Levy SB. Activities of Daily Living. Dordt Digital Collections; 2019. doi:https://doi.org/https://digitalcollections.dordt.edu/faculty_work/1222 [ Links ]
35. Hayase D, Mosenteen D, Thimmaiah D, Zemke S, Atler K, Fisher AG. Age‐related changes in activities of daily living ability. Australian Occupational Therapy Journal. 2004;51(4):192-8 doi: https://doi.org/10.1111/j.1440-1630.2004.00425.x [ Links ]
36. Gunzburg H. Progress assessment chart of social and personal development manual. 4th ed. Stratford-upon-Avon: SEFA Publications; 1976. [ Links ]
37. Southern Oregon Education Service District. OR Project. 2016;(24/04/2016). http://www.soesd.k12.or.us/sectionindex.asp?sectionid=132 [ Links ]
38. Bornman J, Sevcik RA, Romski M, Pae H. Successfully Translating Language and Culture when Adapting Assessment Measures. Journal of Policy and Practice in Intellectual Disabilities. 2010;7(2):111-118. doi: https://doi.org/10.1111/j.1741-1130.2010.00254.x [ Links ]
39. Schell B, Schell J. Clinical and professional reasoning in occupational therapy. 2nd ed. Philadelhpia : Wolters Kluwer Health/Lippincott Williams & Wilkins; 2017. [ Links ]
40. Lynn MR. Determination and quantification of content validity. Nursing Research. 1986;35:382- 385. [ Links ]
41. Yusoff MSB. ABC of Content Validation and Content Validity Index Calculation. Education in Medicine Journal. 2019;11(2):49-54. doi: https://doi.org/10.21315/eimj2019.11.2.6 [ Links ]
42. Besada D, Eagar D, Rensburg R, Shabangu G, Hlahane S, Daviaud E. Resource requirements for community-based care in rural , deep-rural and peri-urban communities in South Africa: A comparative analysis in 2 South African provinces. PLoS One. 2020;15(1):p.e0218682. doi: https://doi.org/10.1371/journal.pone.0218682 [ Links ]
43. Brewer MB, Crano WD. Research Design and Issues of Validity. In: Reis HT, Judd CM, editors. Handbook of Research Methods in Social and Personality Psychology. Cambridge: Cambridge University Press; 2014. p. 11-26. doi:https://doi.org/10.1017/CBO9780511996481.005 [ Links ]
44. Abubakar A, Holding P, Van de Vijver F, Bomu G, Van Baar, A. A. Developmental monitoring using caregiver reports in a resource‐limited setting: the case of Kilifi, Kenya. Acta Paediatrica. 2010;99(2):291-297. [ Links ]
45. Nyumba TO, Wilson K, Derrick CJ, Mukherjee N. The use of focus group discussion methodology : Insights from two decades of application in conservation. 2018;2018(January):20-32. doi: https://doi.org/10.1111/2041-210X.12860 [ Links ]
46. Pleasant A, McKinney J. Coming to consensus on health literacy measurement: An online discussion and consensus-gauging process. Nursing Outlook. 2011;59(2):95-106.e1. http://dx.doi.org/10.1016/j.outlook.2010.12.006. doi:10.1016/j.outlook.2010.12.006 [ Links ]
47. Young Williams, J.I., Yoshida, K.K., Wright, J.G. NL. Measurement properties of the Activities Scale for Kids. Journal of Clinical Epidemiology . 2000;53:125-137. [ Links ]
48. Vogt DS, King DW, King LA. Focus groups in psychological assessment: Enhancing content validity by consulting members of the target population. Psychological Assessment. 2004 [accessed 2020 Aug 1];16(3):231-243. https://pubmed.ncbi.nlm.nih.gov/15456379/. doi:10.1037/1040-3590.16.3.231 [ Links ]
49. Ohrvall Eliasson, A., Lowing, K., Odman, P. A. Self-care and Mobility Skills in Children with Cerebral Palsy, Related to their Manual Ability and Gross Motor Function Classifications. Developmental Medicine & Child Neurology. 2010;52:1048-1055. doi:https://doi.org/10.1111/j.1469-8749.2010.03764.x [ Links ]
50. Majnemer M.; Law, M.; Poulin, C.; Rosenbaum, P. A. S. Level of Motivation in Mastering Challenging Tasks in Children with Cerebral Palsy. Developmental Medicine & Child Neurology. 2010;52(1120-6). doi: https://doi.org/10.1111/j.1469-8749.2010.03732.x [ Links ]
51. Gladstone Lancaster, G., Umar, E., Nyirenda, M., Kayira, E., van den Broek, N., Smyth, R.L. M. Perspectives of normal child development in rural Malawi - a qualitative analysis to create a more culturally appropriate developmental assessment tool. Child: Care, Health and Development,. 2009;36(3):346-353. doi:https://doi.org/10.1111/j.1365-2214.2009.01008.x [ Links ]
52. Gunzburg H. The Progress Assessment Chart (P-A-C) of social and personal development. Stratford on Avon: SEFA Publications; 1977. [ Links ]
53. Folio MR, Fewell RR. Peabody Developmental Motor Scales 3rd Edition - PDMS-3. San Antonio: Psychological Corporation; 2023. [ Links ]
54. Kim K, Kang JY, Jang D-H. Relationship between mobility and self-care activity in children with cerebral palsy. Annals of Rehabilitation Medicine. 2017;41(2):266. doi:https://doi.org/10.5535/arm.2017.41.2.266. [ Links ]
 Correspondence:
Correspondence:
Denise Franzsen
denise.franzsen@wits.ac.za
Received: 29/118/2024
Reviewed (1st Round): 19/02/2025
Revised: 26/05/2025
Reviewed (2nd Round): 27/08/2025
Revised: 22/09/2025
Accepted: 29/09/2025
* Postgraduate student at the University of the Witwatersrand at the time of the study.
EDITOR: Adele Ebrahim https://orcid.org/0000-0002-5018-980x
DATA AVAILABILITY: Upon reasonable request, from corresponding author
FUNDING: No Funding was received for the study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}