










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.55 n.3 Pretoria Dec. 2025
https://doi.org/10.17159/2310-3833/2025/vol55no3a2
RESEARCH ARTICLE
Factors influencing the utilisation of early childhood intervention services in occupational therapy
Humaria Sayed KhanI, II,; Patricia Ann de WittIII; Lindsay KochIV; Denise FranzsenV
IDepartment of Occupational Therapy, School of Therapeutic Sciences, Faculty of Health Sciences, University of the Witwatersrand, 7 York Road, Parktown, Johannesburg, Gauteng, South Africa. https://orcid.org/0009-0002-8421-5211
IIAmana Healthcare: Plot no 11-12, SE 44 Khalifa City A, Abu Dhabi, United Arab Emirates
IIIDepartment of Occupational Therapy, School of Therapeutic Sciences, Faculty of Health Sciences, University of the Witwatersrand, 7 York Road, Parktown, Johannesburg, Gauteng, South Africa. https://orcid.org/0000-0003-3612-0920
IVDepartment of Occupational Therapy, School of Therapeutic Sciences, Faculty of Health Sciences, University of the Witwatersrand, 7 York Road, Parktown, Johannesburg, Gauteng, South Africa. https://orcid.org/0000-0002-7440-2331
VDepartment of Occupational Therapy, School of Therapeutic Sciences, Faculty of Health Sciences, University of the Witwatersrand, 7 York Road, Parktown, Johannesburg, Gauteng, South Africa. https://orcid.org/0000-0001-8295-6329
ABSTRACT
INTRODUCTION: Early identification of children with or at risk of developmental delay and disability is recommended so intervention occurs within their first 1000 days, a critical period for all aspects of development. Early childhood intervention (ECI) services are provided by health and rehabilitation professionals, including occupational therapists, to identify and address developmental delay and disability in young children in South Africa. However, there are concerns about the low rate of caregivers accessing ECI for their children identified as needing this intervention.
METHODOLOGY: A survey design was used to determine the reasons caregivers did or did not utilise ECI occupational therapy services at a district hospital in Gauteng. Structured but non standardised interviews were used to collect the data from 16 caregivers who attended their appointments and three who did not. Data were analysed descriptively based on the framework by Reardon et al. in four domains: family circumstances, views and attitudes towards services, knowledge and understanding of services and treatment, as well as systemic issues in health care.
RESULTS: The 19 participants were mostly women and the mother of the child. The children were mostly males, and only 8 children fell within their first 1000 days of life. Most of the participants only sought help for their children later, when the problem was more severe. Most caregivers were unsure of their child's problem and the implications of this.
Most participants lived in low socioeconomic circumstances between 0 and 21 km from the hospital and used minibus taxis for transport. There was low awareness of the ECI services at the hospital, and participants were more familiar with the work of social workers and psychologists. Most ECI referrals were received from other rehabilitation professionals, with the fewest referrals from doctors. Most participants who did not attend the ECI service stated that this was due to their uncertainty about the extent of the child's problem and belief that it might resolve without treatment.
CONCLUSION: The results identified more barriers to accessing the ECI service at a district hospital than facilitators based on the four domains in the framework by Reardon et al. This included a lack of understanding of their child's developmental problem, what interventions the service had to offer and the service benefits, the contribution of the various health professionals, as well as issues with the health care system being far from where they lived and there being no intersectoral collaboration with other child services.
IMPLICATIONS FOR PRACTICE
• Poor awareness of ECI services and caregivers' lack of understanding of their child's need to access these services early needs to be addressed.
• Client centred services that acknowledge a service user as a partner in health care to enhance health literacy, understanding of the health condition and provide patient satisfaction need attention.
• Multidisciplinary ECI services should be offered at the primary health care (PHC) level to improve access.
• Occupational therapists promoting awareness of occupational therapy related ECI services and advocating for a defined referral pathway to ensure equitable access to ECI services
• Intersectoral collaboration between ECI, infant and toddler wellness programmes and the ECD servicesshould befacilitated.
Keywords: developmental delay, client centred service, hospital-based services, factors affecting service use, multidisciplinary intervention, referral pathway, good health and well-being.
INTRODUCTION
The World Health Organisation (WHO) and United Nations Children's Fund (UNICEF) estimate that over 50 million children under five years old have developmental disabilities, with four out of every 10 children in low middle-income countries missing critical developmental milestones1. Young children are left behind and experience occupational deprivation due to poverty, inadequate access to essential nutrition, health, water and sanitation services; lack of access to early stimulation, responsive care and learning opportunities2. In South Africa, Early Childhood Development (ECD) was introduced in 2005 as an intersectoral service between the Departments of Social Welfare, Health, Basic Education, local government, and the non-profit organisation sectors. These services aimed to ensure the promotion of child development, adequate stimulation, provision of early play-based learning opportunities, sound parenting practices, as well as behaviour management practices3. Initially, this programme was administered by the Department of Social Development (DSD) and, in 2022, was transferred to the Department of Basic Education (DoBE) as ECD was viewed more as a learning function than a child protection function4. Inherent in the approach used by the DoBE is the early identification of children with or at risk of developmental delay and disability between birth and age eight years1. These children need to be identified as early as possible since it is recommended they receive intervention in their first 1000 days, or two years, which is considered critical for optimal cognitive, physical, language, motor and social development5.
The identification of these at-risk children demands the provision of accessible services for early childhood intervention (ECI) "to promote child health and well-being, enhance emerging competencies, minimise developmental delays, remediate existing or emerging disabilities, prevent functional deterioration and promote adaptive parenting and overall family function"6:15. According to the National Integrated Early Childhood Development Policy of 2015, the Department of Health is responsible for these services at all levels of health care7. Health and rehabilitation professionals, including occupational therapists, physiotherapists, as well as speech therapists and nutritionists, thus play a role in the provision of ECI. These services address identified impairments in client factors as well as performance in developmental^ and contextually appropriate everyday activities8. However, despite policies indicating accessible free health services for children under the age of six years9, concern has been reported at the low rates of caregivers accessing ECI for their children10.
LITERATURE REVIEW
In South Africa, environmental factors such as poverty affect ECD, with approximately half of the children in the country living below the lower poverty line11. This context has the potential to adversely affect development, especially for children with disabilities,12 resulting in a greater need for ECI services. Children in these circumstances may be at further risk for developmental delay or increasing disability due to a lack of early identification of the problem, and a lack of referral to or an inability to access ECI13.
Screening of young children to identify those at risk occurs within education and health settings. Nationally, the developmental screening tool used in health services is the parent-held Road to Health Booklet (RtHB), revised in2018 to includete e de bbyS¡decamgn¡gn,wh ich considers access to special care needs or support for children with developmental delay or disability14. Once a child is identified as being at-risk or in need of special care, referral for ECI in the health sector should occur, where intervention includes providing diagnostic and evaluation services. Early childhood intervention is provided by a multidisciplinary team including medical, nutrition and rehabilitation services13. Occupational therapists are among the rehabilitation professionals offering ECI and play an important role in health promotion, prevention, and intervention for the development of at-risk or disabled children by facilitating participation in the occupations of childhood15. These therapists use screening tools that determine the child's ability to complete various activities to ensure an objective assessment of the child. If children present with impairments or delays in occupational performance, a full assessment based on age and culturally appropriate functional ability is completed. Family-centred intervention is offered, usually on a monthly outpatient basis16,17.
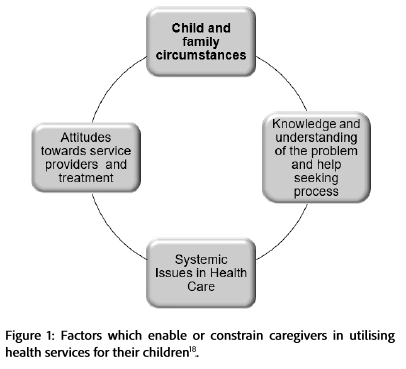
However, significant numbers of children in South Africa at-risk due to undefined developmental delay or established disabilities, do not currently access EDI10. To understand the possible factors that act as enablers and constraints to service users in utilising ECI, a framework developed by Reardon et al.18 was applied in the current study (Figure 1, below). The framework includes four domains: family circumstances, views and attitudes towards services, knowledge and understanding of services and treatment, at well at fystemic i sssieei nhhelttcate.
Family Circumstances
Reardon et al.18 identified that barriers to seeking help for the child by their caregiver are related to aspects of the family life, such as the religious and cultural views, as well as the impact of the family's financial situation. Consideration must be given to the religious and cultural beliefs of the community19,20. For example, a child who presents with developmental delay or disability in some cultures may not be considered to have "ill health" and caregivers are reported to feel that the problem will resolve spontaneously, so they do not seek health care21,22. Kyarkanaye et al.23 reported that if health care services are not offered in a culturally relevant way, it is less likely that community members will access these services.
A family's socioeconomic status and the environment in which the child lives impact not only the child's nutrition and development but also access to healthservicesintermsof aoss antjtime.
Views and attitudes towards services and treatment
Past experiences, as well as the perception of the quality of services provided at the health care facility, influence whether caregivers would seek help for their child18. Negative attitudes of staff and a lack of collaboration with caregivers and parents of children discouraged the parents and caregivers from accessing health care. This negatively impacted the number of children accessing the services23. Poor interdisciplinary team functioning, resulting in multiple appointments on different days and sites for health care, also plays a role8.
If the caregiver or parents are not aware of the child's problems, they are unlikely to access services, particularly those of ECI21. Socio-cultural factors such as a low level of education, lack of adequate understanding of health information and low levels of health literacy have been linked to the caregivers' choice of care for young children with disabilities. Research has indicated that many caregivers did not think that the child's problems were serious enough to seek help24.
Knowledge and Understanding of the services
A lack of awareness of services was identified by Reardon et al.18, as a barrier to the utilisation of healthcare. Frequently, a patient will be requested to go for follow-up at the clinic for continuation of services or will be referred up to a more specialised level of care at a hospital for further management. However, they do not always understand the reason for this and as a result, return home without having sought the necessary health care recommended25.
Systemic Issues in Health Services
Literature indicates that even when children attend ECI services, there is very little coordination with the DoBE and other sectors offering ECD services8,13. Caregivers of children, as service users, have also reported a lack of collaboration between themselves and health professionals23 and poor inclusive services for children requiring ECI in ECD13 as affecting the utilisation of ECI services.
From the first author's experience, attendance for ECI services at an urban public sector district hospital in Gauteng, South Africa, was found to be inconsistent. It was also noted that not all caregivers and their children were referred for occupational therapy when developmental delay or disabilities had been identified or made appointments or attended ECI even when appointments were made. Many caregivers only sought assistance for their children at a later stage when secondary complications had occurred or the severity of problems associated with the diagnosis had progressed significantly. Although there is literature available in the South African context on the factors (enablers and constraints) that influence access to health care, it is unclear what specific factors influence access to ECI services in an urban context. To address the poor utilisation of occupational therapy services, this study aimed to determine the factors that influenced the caregivers' decision to access ECI occupational therapy services for their child.
METHODOLOGY
A descriptive, cross-sectional, quantitative, and non-experimental survey design26 was used to determine the utilisation of occupational therapy ECI by caregivers of children referred for intervention services at a district hospital, as well as the factors that enabled or constrained access to these services.
Setting
The occupational therapy ECI service at a district hospital in Gauteng, South Africa, forms part of the specialized multidisciplinary ECI centre developed in 2014, in accordance with the Guidelines for ECD3. Services include occupational therapy, speech therapy and audiology, physiotherapy, nutrition and as from 2017, psychology and social work. Specialized services, early identification of problems and rehabilitation are included in the ECI programme. Service users were referred from the surrounding clinics and from the hospital's neonatal intensive care unit, paediatric wards, andoutpatient clkinics.
Sampling
This study used purposeful total population sampling and included all caregivers of children referred to the occupational therapy ECI service for the first time, regardless of age and referral source, over a period of six months27. Based on a record review of referrals, a sample size of 40 was anticipated. The recruitment of participants was hindered by the non-arrival of caregivers for booked appointments, requiring the researcher to recruit additional participants by telephoning those who missed their appointment.
Research instrument
The data were collected in non-standardised interviews using a survey questionnaire which was developed specifically for this study based on the literature. The questionnaire had three sections: demographic information of the caregiver; information about the referred child, including birth related information, medical history and the presentation of signs and symptoms of the condition that initiated the referral; and finally, factors which enabled or constrained the utilisation of the occupational therapy ECI service. The face validity of the questionnaire was evaluated by a multidisciplinary panel from the ECI team. Changes suggested were made to the questionnaire based on their critique.
A second questionnaire was developed for the caregivers who failed to attend the booked appointment for their child, to explore the reasons for not accessing the service. This questionnaire was administered telephonically and had two parts: demographic and medical history of the child, followed by the reasons for not attending the given appointment. Both questionnaires were piloted on five caregivers attending other services at the ECI centre. The purpose of the pilot study was to ensure the questions were user-friendly, understandable, and consistent with the study aim.
Both questionnaires had open-ended questions, which allowed the participants to explain their answers to questions and comment on their answers.
Research Procedure
The study was approved by the Human Research Ethics Committee at the University of the Witwatersrand (M160846) as well as the Gauteng Provincial Health Department and the Hospital where the research took place. All first-time users of the occupational therapy ECI service were invited to participate and were provided with the approved information sheet. A research assistant was trained to assist with translation if the caregiver was not proficient in English, to ensure that the caregiver understood the purpose and nature of the study. Caregivers gave informed consent prior to the structured interview.
The data were collected face-to-face with participants on the first day they accessed the occupational therapy ECI service. The researcher conducted the structured interview and recorded the caregiver's answers on the questionnaire to accommodate the low literacy rates. The questionnaire took an average of 15 minutes to complete. Telephonic interviews were conducted with caregivers who did not attendtheirappointments.
Data Analysis
Data from the questionnaires were analysed using descriptive statistics based on the domains included in the framework by Reardon et al.18. Content analysis was used to analyse comments and responses to the open-ended questions.
RESULTS
The occupational therapy ECI service received 36 referrals during the six-month research period. Only 21 caregivers (58,3%) arrived for their appointment and five refused the invitation to participate and thus, 16 participants (44%) were recruited into the study. The researcher was able to recruit a further three participants (20%) from the 15 caregivers who did not attend their given appointment for telephonic interviews. The remaining seven caregivers could not be contacted by the researcher as the call was not answered, or the number was out of service or incorrect
Demographics
Caregivers
Of the 19 caregiver participants, the majority (84.2%) were female and 15 (77.9%) were the mother of the child, while two were the grandmothers and one was the father of the child attending ECI. One child was brought to ECI by a friend of the mother,
Children referred to occupational therapy for early childhood intervention
Of the 19 children referred for occupational therapy, most were male (68.4%; n=12) and their ages ranged from six months to over five years, with only eight children (42.1%) falling into the first 1000-day category. Eleven children were over the age of 24 months and the seven children (31.5%) who were five years of age or older would be considered late referrals.
Table I (below) reports the diagnoses of the children referred for ECI, but some participants (10.5%) reported being unaware of any medical diagnosis or reasons that may have caused the child's developmental delay or disability.
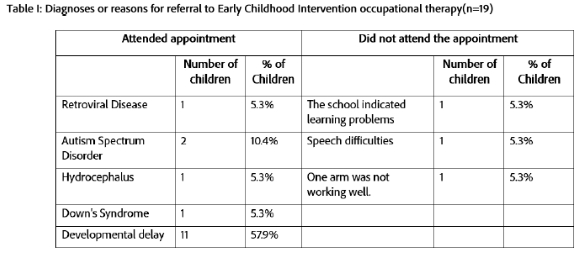
Of the children who were referred with developmental delay, caregivers reported that eight children (42.1%) had problems since birth due to prematurity (n=2) and neonatal jaundice, respiratory distress, asphyxia, and a heart condition. Six children (31.5%) had been admitted to hospital after birth for tuberculosis, seizures, a liver cyst, to insert a shunt, bronchitis and being underweight.
Eight children (42.1%) spent their day at home, seven (36.8%) went to ECD centres (creche or nursery school) and four (21.0%) went to school. It was reported that nine (81.8%) of the 11 children who went to ECD centres or school presented with the following developmental and learning problems: letter reversals, difficulties copying from the board, behavioural problems, concentration problems, poor social skills, poor appetite, difficcltieew¡thhhanwr¡t¡noaannnOsppeaino·
Factors enabling or constraining the utilisation of occupational therapy early childhood intervention services.
Family Circumstances
Two thirds (n=12) of the caregiver participants reported having a monthly income of between RO-5599, indicating a low socio-economic status, while the remaining earned between R5600-R40,000, which is considered a middle-income status. Caregiver participants reported that they lived between 0 and 21 km from the Hospital offering ECI services. Taxis were the most common mode of transport used by 14 (73.6%) participants, with one participant indicating that more than one taxi was required to access the ECI service. One participant used the train, and three (15.8%%) participants indicated that they walked to the hospital. Four (21.0%) participants reported transport problems due to a lack of finances for transport or no direct transport available for accessing the hospital. Five (26.3%) participants indicated that they did not seek help for their children earlier because of transport constraints.
Caregiver participants reported that nine (52.6%) of the primary caregivers of the children referred to occupational therapy ECI, were employed. Four (21.0%) of these participants reported that it was easy to get time off work, while two (10.5%) reported that it was difficult or somewhat difficult to get time off work to bring their child to appointments. Five (26.3%) of the working caregivers were able to send someone else to attend the appointment with the child, should they be unable to do so. In four cases, this was reported to be the father, and in one, thegrandparents.
Views and attitudes towards services and treatment
Participants reported that family members, particularly the grandparents, were most concerned (52.6%) about the child and suggested that they received ECI. Over 20% of fathers and teachers at school also recommended the child be assessed for developmental problems.
It was reported that 57.8% of participants had been advised to seek help from the hospital and 42.2% from the clinic (Figure 2, below).
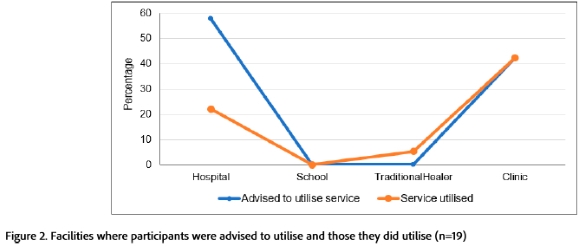
Most participants reported utilising the clinic services, since they perceived that more help would be available from the clinic, while only 22% attended the hospital. One participant (5.2%) believed the traditional healer would be of most assistance (Figure 2, page 4). Fifteen caregiver participants indicated that they were concerned about their children at or before 24 months. Five participants (26.3%) reported being concerned about their child from birth to three months, while five (26.3%) were only worried from 24 months onwards. However, nine caregiver participants who were referred to occupational therapy ECI services early only attended appointments later when the child was over 24 months old. Seven participants (36.8%) reported they thought the child would just get better, and one participant (5.2%) indicated that she was unsure if the child had a problem and was waiting for the doctor to confirm and refer her to other services (Table II below).
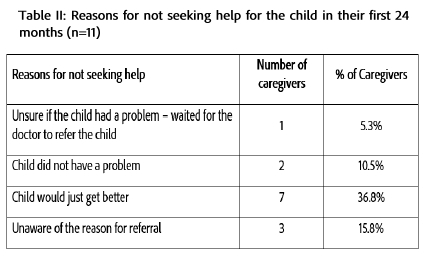
Three participants (15.8%) reported being unaware of the reason for referral to occupational therapy ECI services. Two caregiver participants with children older than 24 months, who did not attend occupational therapy ECI, one indicated that she had forgotten about the appointment and did not see any of the problems that the school had reported at the time of making the appointment. The other caregiver participant did not wish to have their appointment rescheduled, as she also did not perceive her child had a problem anymore.
Knowledge and Understanding of the services
Two thirds of the 19 caregiver participants were more aware of general hospital services than specific services, such as occupational therapy or the ECI programme in the hospital. Ten (52.6%) participants indicated that they did not seek help for their children earlier since they were unsure where to seek help. Six (31.5%) of the caregiver participants were aware of occupational therapy, while three (18.8%) of the participants were aware of the ECI programme. Of the participants who were aware of ECI services, two (10.5%) had heard about the services from other health professionals and the remaining one (5.3%) from ECI promotion and prevention talks atthehospital (Figure 3, below).
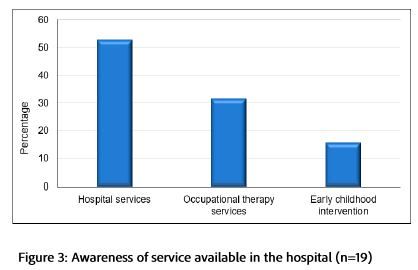
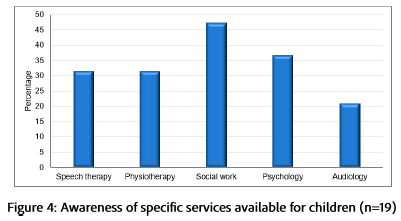
Figure 4 (below) indicates that the highest percentage of caregiver participants were aware of the other services provided by social work and psychology. Just less than a third of participants were aware of services by speech therapy and physiotherapy services, with the lowest awareness foraudiology services.
Systemic Issues in Health Services
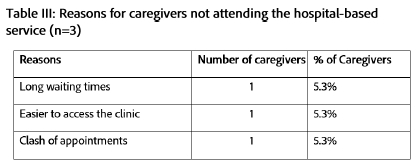
Most children were referred to the occupational therapy ECI service by other health professionals. Eight (42.1%) referrals were from other rehabilitation professionals, followed by nurses (n=5,26.3%) and doctors (n=3; 15.8%). Four (21.0%) caregiver participants were self-referred and there were no direct referrals from creches or schools Only three (15.8%) participants reported challenges in utilising the service at the hospital (Table III, below).
DISCUSSION
The study was based on a framework developed by Reardon et al.18 allowed for barriers and facilitators in attending ECI occupational therapy services to be viewed from four perspectives. While views and attitudes towards services and treatment and knowledge of services provided the most attitudinal and informational barriers, family circumstances and health service issues present greater structural barriers t oaccessing ECI.
Family Circumstances
Most families of the participants in this study could be considered as having a low socioeconomic status in terms of income and with less than half being employed. This environmental factor has been identified as significantly associated with risk for or exacerbating developmental delay28. The level of financial stress caregivers experience affects their access to assistance for the child, as well as their ability to provide a cognitive stimulating environment29 and the adequate nutrition required to prevent developmental and educational impairments30.
The socioeconomic status of the participants in the study meant most were reliant on public transport. The National Households Travel Survey in 2020 indicated that in Gauteng, minibus taxis were the most common mode of transport used by 70,9% of the population31. Transport to accessing services, including health, remains a major deterrent in the current study, with trips for health visits not included in the budget of most families, where the cost of transport is not prioritised31. A similar finding was reflected in a study in a high-income country (HIC). Canada also reported that the most significant logistical challenge in attending ECI was reliance on public transport32.
Access to health services may be affected by the location of health services as they are far from the child's home and the need to take time off work to use the services. Adedini et al.33 reported distance from services as the greatest barrier to accessing health services for children in urban South Africa. This supports the importance of moving services to their communities, which was also a recommendation made by participants in a study by Frost et al.34 on the lack of attendance at appointments in a distric thospital in the Western Cape.
Views and attitudes towards services and treatment
Children referred to occupational therapy ECI services ranged in age from six months to over five years. Developmental delays can present at any stage in the child's life35 and thus, while it is encouraging that just over a third of the sample sought help as soon as they became aware of their children's problems, as indicated by Smythe et al.35 a large number of children with disabilities in lower-middle-income countries (LMIC) never receive ECI and thus do not maximise their developmental potential and functioning.
Participants in the current study indicated that the delay in or lack of uptake of ECI services was based on their knowledge of child development and their understanding of the child's challenges was supported by Phoenix et al.32. Although 42.1% of the children were admitted to hospital at or just after birth and most had diagnoses such as retroviral disease, hydrocephalus and Down's Syndrome associated with pre-and peri-natal risk for developmental delay36,37 over half of the children attending ECI occupational therapy did not have a diagnosis. Caregivers' lack of knowledge, particularly on developmental milestones and the lasting effects of chronic disability, was found to be an important factor that influenced whether healthcare services were accessed or not25,38. Similarly, a poor understanding of the diagnosis and its developmental implications also plays a role in the type of help that the family members may seek for the child. Alternative treatment methods or care services from traditional healers may also be sought39.
Often, it was older family members with experience of raising children who better understood developmental delay who recommended that ECI services be sought. Tomlinson et al.40 indicated family support structures as a significant factor influencing whether or not early childhood services are accessed. However, as indicated by Magnusson et al.41, the parents' beliefs about health and development are the most important factors in seeking help for their child. In their study, as in the current study, the parents' belief that the child would outgrow the concerns identified or that the child did not really have a problem affected the attendance at ECI. Magnusson et al.41 reported that mothers from low socioeconomic situations often rely on social networks to deal with the issues rather than the health system, where they feel their concerns are not heard or understood. It is therefore important that caregivers understand what to expect of their child's age band and receive training on how to implement a home programme with the child to encourage participation in occupations such as bathing, dressing, feeding, play and education42 so the child can reach their developmental potential35. Magnusson et al.41 also emphasize the importance of understanding the parents' developmental expectations and making them an equal partner in how concerns should be addressed41, rather than imposing therapy and home programmes43.
In the South African context, parents who work often leave the child with an alternative carer44 who may not be able to identify problems that the child may be experiencing. Parents also relied on carers or family members to access ECI on their behalf if they could not get time off work. This compounded the issue of the child's needs not being well understood by the parents themselves. Education campaigns on child development and recognising developmental delay should occur at the primary health care level, with involvement from a multidisciplinary team10,38.
Although only one participant in the current study forgot about the appointment, this was the most reported reason for lack of attendance for outpatient services reported by Frost et al.34 in the Western Cape. It was suggested that a messaging system with appointment reminders should be considered,allowing cancellations if necessary.
Knowledge and Understanding of the services
While 50% of participants were aware of the hospital services, only a third of the participants were aware of the various professions offering ECI and only three participants were aware of ECI services. Services offered by the psychologists and social workers were known to a higher percentage of participants, with services offered by occupational therapy being limited. These results reflect those of Kotsokoane et al.43 and Zziwa et al.45 when exploring factors influencing the utilisation of rehabilitation services in LMIC. A lack of awareness of rehabilitation services was significantly associated with utilisation of the services. In the current study, a lack of knowledge about what services are available also appears to affect most participants' understanding of what they offer and why their child would benefit if they accessed these services. In addition, health care professionals refer children to ECI but do not always explain the reason for the referral46. Many did not appear to do so, as many parents did not understand the reason for the referral, which may also affect attendance at the appointment given. Participants often did not make further enquiries on the referral, resulting in exacerbation of the developmental delay before intervention was sought. Similar findings of parent disempowerment were reported by Hohlfeld et al.47 and Lynch er al. 46 when determining parent self-efficacy in dealing with developmental delay and disabilities in pre-school children with disabilities in resource-limited settings in LMICs.
Systemic Issues in Health Services
A number of local and national health service issues were identified as impacting access to occupational therapy ECI, indicating the need to address and advocate at all levels of policy making and implementation.
The health system structure and issues with the management and service provision at the hospital did affect the access to ECI for a small number of participants. Another urban South African study by Adedini et al.33 reflects similar issues expressed by caregivers of children accessing ECI services. Although most participants were positive about the services, there were issues in terms of waiting time for appointments. When appointments were given, the child was not always seen at the appointment time, so visits were perceived as time-consuming and sometimes disorganised. They also felt the frequency of appointments was insufficient48.
The participants also mentioned that they relied on nurses at the well-baby clinics with whom they had regular contact to assist with identifying developmental problems with their child. Almost half of the participants verbalised that they could access the clinic and preferred local services rather than coming to the hospital, although referrals were made to the ECI team at the hospital. This indicates the importance of providing the ECI services at a primary health care level in the clinics or using a community outreach approach, since there are limited therapeutic services available in the clinics. This type of local service provision was identified by Richter et al.49 and the DoBE in their ECD 2030 Strategy50 as essential to providing services that support parents in addressing developmental delays49.
In the current study, workforce and training were issues highlighted by participants. A quarter of the referrals to ECI came from nurses who do developmental screening at the clinics, although this is not mandatory. The clinics are often understaffed and therefore, only children with severe and moderate problems are more likely to be referred to ECI from this source10. Even if participants were to receive ECI at the clinics in their area, they offer limited rehabilitation services, sometimes these only occur twice a month and due to workload and the children were not seen regularly. These findings were supported by literature in South Africa and a few early intervention professionals13 and in other LMIC countries, where the availability of appropriate assessment tools affected referral and treatment offered in ECI46.
The lack of cross-sectoral governance and intersectoral cooperation between the Department of Health and DoBE8 is of concern due to a lack of funding, limited strategic planning for large-scale change, and uneven progress in integrating services across government departments and local structures 51. This means that despite the implementation of ECI services in the hospital, these services are not currently assisting in early intervention for barriers to learning identified by teachers, as parents are not following up on recommendations and no official referral between education and health exists. For the children referred for occupational therapy ECI, who were in school or ECD centres (nursery school and crèche) for over 80% of the child's caregivers were made aware of developmental problems by the ECD staff, who encouraged them to seek intervention for their child52. However, accessing ECI was dependent on the child's parents, a problem reported in many LMIC35.
These issues are related to policy-practice gaps. Although policies such as the WHO Nurturing Care Framework2 and the National Integrated Early Childhood Development Policy (NIECDP)7 and its 2030 Strategy50 support the provision of comprehensive ECD services, fragmented progress in South Africa has been made51. As reported by Lynch et al.46 with other LMIC country policies, the South African polices lack referral pathways from ECD to ECI to rehabilitation and occupational therapists. This lack of pathways further impedes collaboration with other services and the provision of handovers Thus. ECI occurs in isolation within the health sector, where Balton et al.8 identified poor implementation of the ECI provincial policy, with no records of children shared between services, as challenges to the provision of these services in Gauteng.
Limitations of the study
The study had a small sample size, which influences the external validity and gen e ra liability of the results to other contexts. The results may not reflect all the factors impacting attendance at ECI occupational therapy even in the current context. It was not determined in this study whether the developmental problem had been identified whilst the child was in hospital at birth and whether the child had been referred for ECI at that stage.
CONCLUSION
In conclusion, there are both barriers and facilitators influencing access to early childhood services. However, there are more barriers than facilitators and initial barriers to uptake of services were informational and attitudinal due to a lack of knowledge of childhood development and the belief that the child did not require health services. The caregiver's knowledge of the problem, as well as developmental norms was also noted as a barrier, as it influenced the time at which services were sought. Even for participants who did wish to attend ECI occupational therapy, structural barriers such as availability, cost and access to transport appeared to be significant. Systemic issues in the health system due to gaps in policy implementation, limited workforce, location of services and lack of intersectoral collaboration between government departments further limited uptake of ECI services.
Acknowledgements
We would like to acknowledge the parents and caregivers who gave their time for this study.
Author Contributions
Humaria Sayed Khan and Lyndsay Koch conceived the study and Humaría Sayed Khan carried out the research supervised by Lyndsay Koch. Pat de Witt and Denise Franzsen conceived and wrote the article based on the research The article was checked, edited and approved by Humaría Sayed Khan and Lyndsa yKoch
Conflicts of interest
None to deelare
REFERENCES
1. World Health Organization and United Nations Children's Fund. Global report on children with developmental disabilities: from the margins to the mainstream. 2023. https://www.unicef.org/media/145016/file/Global-report-on-children-with-developmental-disabilities-2023.pdf [ Links ]
2. World Health Organization and United Nations Children's Fund. Nurturing Care for Early Childhood Development: a Framework for Helping Children Survive and Thrive to Transform Health and Human Potential. Geneva; 2018. https://iris.who.int/bitstream/handle/10665/272603/9789241514064-eng.pdf?sequence=1&isAlloweedy [ Links ]
3. Republic of South Africa. The Guidelines for Early Childhood Development Services. Department of Social Development. 2006. https://www.gov.za/sites/default/files/gcis_document/201409/childhooddev0.pdf [ Links ]
4. Republic of South Africa. Implications for ECD shift to Basic Education. Department of Basic Education. 2021. https://www.education.gov.za/ECDFunctionShift2021.aspx [ Links ]
5. Cusick S, Georgieff M. The first 1,000 days of life: The brain's window of opportunity. 2013. https://www.unicef-irc.org/article/958-the-first-1000-days-of-life-the-brains-window-of-opportunity.html [ Links ]
6. Shonkoff J., Meisels SJ. Handbook of Early Childhood Intervention. 2nd ed. Cambridge: Cambridge University Press; 2000. [ Links ]
7. Republic of South Africa. National integrated early childhood development policy. Department of Social Development. 2015. https://www.gov.za/sites/default/files/gcis_document/201610/national-integrated-ecd-policy-web-version-final-01-08-2016a.pdf [ Links ]
8. Balton S, Vallabhjee A, Burger E. Early childhood intervention : the Gauteng experience. South African Health Review. 2020;1:99-106. https://journals.co.za/doi/pdf/10.10520/ejc-healthr-v2020-n1-a13 [ Links ]
9. Buchner-Eveleigh M. Children's rights of access to health care services and to basic health care services: a critical analysis of case law, legislation and policy. De Jure Law Journal. 2016,-49(2):307-325. doi:https://doi.org/10.17159/2225-7160/2016/v49n2a6 [ Links ]
10. Samuels A, Stemming W. Early Childhood Intervention in South Africa in Relation to the Developmental Systems Model. 2012;25(4):334-345. doi:https://doi.org/10.1097/IYC.0b013e3182673e12 [ Links ]
11. United Nations Children's Fund (UNICEF). Country Office Annual Report 2023: South Africa. Update on the context and situation of children. 2023. https://www.unicef.org/reports/country-regional-divisional-annual-reports-2023/South-Africa [ Links ]
12. Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B. Developmental potential in the first 5 years for children in developing countries. The Lancet. 2007;369(9555):60-70. doi:https://doi.org/10.1016/S0140-6736(07)60032-4 [ Links ]
13. Karisa A, Samuels C, Watermeyer B, McKenzie J, Vergunst R. Priorities for access to early childhood development services for children with disabilities in South Africa. South African Journal of Childhood Education. 2022,-12(1):1-7. doi:https://doi.org/10.4102/sajce.v12i1.1119 [ Links ]
14. Stemming W, Bamford L. The new road to health booklet demands a paradigm shift. SAJCH South African Journal of Child Health. 2018;12(3):86-87. doi: https://doi.org/10.7196/SAJCH.2018.v12i3.1595 [ Links ]
15. American Occupational Therapy Association. Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy. 2020;74(Suppl. 2):7412410010. doi: https://doi.org/10.5014/ajot.2020.74S2001 [ Links ]
16. Maddocks S, Nakooda M, Cobbing S, Hanass-HancockJ, Chetty V. Perceptions of care and rehabilitation for children living with HIV in KwaZulu-Natal province, South Africa. https://doi.org/10.1080/17450128.2020.1830214.2021;16(2):151-165. doi: https://doi.org/10.1080/17450128.2020.1830214 [ Links ]
17. Maharaj SS, White TL, Kaka B. How are children with cerebral palsy managed in public hospitals of KwaZulu-Natal, South Africa? Physiotherapy Theory and Practice. 2021,37(11):1235-1243. doi: https://doi.org/10.1080/09593985.2019.1686791 [ Links ]
18. Reardon T, Harvey K, Baranowska M, Brien DO, Smith L, Creswell C. What do parents perceive are the barriers and facilitators to accessing psychological treatment for mental health problems in children and adolescents ? A systematic review of qualitative and quantitative studies. European Child & Adolescent Psychiatry. 2017;26(6):623-647. doi: https://doi.org/10.1007/s00787-016-0930-6 [ Links ]
19. Asa GA, Fauk NK, Mwanri L, Ward PR. Understanding barriers to the access to healthcare and rehabilitation services: A qualitative study with mothers or female caregivers of children with a disability in indonesia. International Journal of Environmental Research and Public Health. 2021;18(21). doi: https://doi.org/10.3390/ijerph182111546 [ Links ]
20. Wallace K. Early Intervention for Young Childen at Risk for Developmental Mental Health Disorders. In: Crouch R, Alers V, editors. Occupational Therapy in Psychiatry and Mental Health. London, UK: John Wiley & Sons; 2014. p. 239-347. [ Links ]
21. Merugumala SV, Pothula V, Cooper M. Barriers to timely diagnosis and treatment for children with hearing impairment in a southern Indian city: a qualitative study of parents and clinic staff. International Journal of Audiology. 2017;56(10):733-739. doi: https://doi.org/10.1080/14992027.2017.1340678 [ Links ]
22. Lehohla P. Use of health facilities and levels of selected health conditions in South Africa: Findings from the General Household Survey. 2013. http://www.statssa.gov.za/publications/Report-03-00-05/Report-03-00-052011.pdf [ Links ]
23. Kyarkanaye T, Dada S, Samuels AE. Collaboration in Early Childhood Intervention Services in Gauteng. Caregiver Perspectives. Infants & Young Children,. 2017;30(3):238-254. doi: https://doi.org/10.1097/IYC.0000000000000095 [ Links ]
24. Sekyere FO, Gyamfi CKR, Poku N. Knowledge, Attitude and Practices of Caregivers towards Disabled Children under- Five Years and It ' s Influence on Clinical Outcome. American International Journal of Business Management (AUBM). 2020;3(8):168-177. [ Links ]
25. Crabtree SA. Family responses to the social inclusion of children with developmental disabilities in the United Arab Emirates. Disability and Society. 2007;22(1):49-62. doi: https://doi.org/10.1080/09687590601056618 [ Links ]
26. Taylor RR. Kielhofner's research in occupational therapy: Methods of inquiry for enhancing practice.. FA Davis; 2017. [ Links ]
27. PolgarT. Introduction to research in the health sciences. Fifth edit. USA: Elsevier Ltd; 2008. [ Links ]
28. du Toit M, van der Linde J, Swanepoel DW. Early Childhood Development Risks and Protective Factors in Vulnerable Preschool Children from Low-Income Communities in South Africa. Journal of Community Health. 2021;46(2):304-312. doi: https://doi.org/10.1007/s10900-020-00883-z [ Links ]
29. Evans GW, Kim P. Childhood Poverty, Chronic Stress, Self-Regulation, and Coping. Child Development Perspectives. 2013;7(1):43-48. doi: https://doi.org/10.1111/cdep.12013 [ Links ]
30. Tang MN, Adolphe S, Rogers SR, Frank DA. Failure to thrive or growth faltering: medical, developmental/behavioral, nutritional, and social dimensions. Pediatrics in Review. 2021:590-603. doi: https://doi.org/10.1542/pir.2020-001883 [ Links ]
31. Statistics South Africa. National Household Travel Survey, 2020 (P0320). 2021. https://www.statssa.gov.za/publications/P0320/P03202020.pdf [ Links ]
32. Phoenix M, Jack SM, Rosenbaum PL, Missiuna C. A grounded theory of parents' attendance, participation and engagement in children's developmental rehabilitation services: Part 2. The journey to child health and happiness.,. Disability and Rehabilitation. 2020,-42(15):2151-2160. doi: https://doi.org/10.1080/09638288.2018.1555618 [ Links ]
33. Adedini SA, Sello M, Thaele D, Madhi SA. Patterns of healthcare utilisation and barriers affecting access to child healthcare services in low-income urban South African settings. SAJCH South African Journal of Child Health. 2020;14(1):34-39. doi: https://doi.org/107196/SAJCH.v14.i1.1650 [ Links ]
34. Frost L, Jenkins L, Emmink B. Improving access to health care in a rural regional hospital in South Africa: Why do patients miss their appointments? African Journal of Primary Health Care and Family Medicine. 2017;9(1):1-5. doi: https://doi.org/10.4102/phcfm.v9i1.1255 [ Links ]
35. Smythe T, Zuurmond M, Tann CJ, Gladstone M, Kuper H. Early intervention for children with developmental disabilities in low and middle-income countries - The case for action. International Health. 2021;13(3):22–2231. doi: https://doi.org/10.1093/inthealth/ihaa044 [ Links ]
36. Kaviani M, Ranjbaran Z, Janghorban R. Relationship between perinatal period problems and developmental delay in children aged 4-24 months. Acta Facultatis Medicae Naissensis. 2020;37(4):337-348. doi: https://doi.org/10.5937/AFMNAI2004337K [ Links ]
37. Thomaidis L, Zantopoulos GZ, Fouzas S, Mantagou L, Bakoula C, Konstantopoulos A. Predictors of severity and outcome of global developmental delay without definitive etiologic yield: A prospective observational study. BMC Pediatrics. 2014;14(1). doi: http://dx.doi.org/10.1186/1471-2431-14-40 [ Links ]
38. Ñores M, Barnett SW. Benefits of early childhood interventions across the world: (Under) investing in the very young. Economics of Education Review. 2012;2012(1):200-228. doi: https://doi.org/10.17323/1814-9545-2012-1-200-228 [ Links ]
39. Goudge J, Gilson L, Russell S, Gumede T, Mills A. Affordability, availability and acceptability barriers to health care for the chronically ill: Longitudinal case studies from South Africa. BMC Health Services Research. 2009;9:1-18. doi: https://doi.org/10.1186/1472-6963-9-75 [ Links ]
40. Tomlinson M, HuntX, Rotheram-Borus M. Diffusing and scaling evidence-based interventions: eight lessons for early child development from the implementation of perinatal home visiting in South Africa. Annals of the New York Academy of Sciences. Annals of the New York Academy of Sciences. 2018,-1419(1 ):218-229. doi: https://doi.org/10.1111/nvas.13650 [ Links ]
41. Magnusson DM, Minkovitz CS, Kuhlthau KA, Caballero TM, Mistry K. Beliefs regarding development and early intervention among low-income African American and Hispanic mothers. Pediatrics, 140(5). Pediatrics. 2017,-140(5):1-6. doi: https://doi.org/10.1542/peds.2017-2059 [ Links ]
42. O'Brien JC, Kuhaneck H. Case-Smith's Occupational Therapy for Children and Adolescents. 8th editio. Elsevier Mosby; 2019. [ Links ]
43. Kotsokoane F., Tshabalala M., Skaal L. Factors influencing the utilisation of community-based rehabilitation services by people with disability in Tshwane, Gauteng Province, South Africa: utilization of primary health care services. African Journal for Physical Health Education, Recreation and Dance. 2015;21(supp 2):287-295. https://hdl.handle.net/10520/EJC184406 [ Links ]
44. Mkhwanazi N, Makusha T, Blackie D, Manderson L, Hall K, Huijbregts M. Negotiating the care of children and support for caregivers. South African Chikld Gauge. 2018:70-80. http://childrencount.uct.ac.za/uploads/publications/South_African_Child_Gauge_2018_Children_Families_and_the_State.pdf#page=72 [ Links ]
45. Zziwa S, Babikako H, Kwesiga D, Kobusingye O, Bentley JA, Oporia F, Nuwematsiko R, Bachani A, Atuyambe LM, Paichadze N. Prevalence and factors associated with utilization of rehabilitation services among people with physical disabilities in Kampala, Uganda. A descriptive cross sectional study. BMC Public Healthealth. 2019,-19(1):1-11. doi: https://doi.org/10.1186/s12889-019-8076-3 [ Links ]
46. Lynch P, Nabwera HM, Babikako HM, Rasheed M, Donald KA, Mbale EW, Stockdale E, Chand P, Van den Heuvel, M., Kakooza Mwesige A, Gladstone M. Experiences of identifying pre-school children with disabilities in resource limited settings-an account from Malawi, Pakistan and Uganda. Disability & Society. 2024;39(8):2053-2073. doi: https://doi.org/10.1080/09687599.2023.2181769 [ Links ]
47. Hohlfeld ASJ, Harty M, Engel ME. Parents of children with disabilities: A systematic review of parenting interventions and self-efficacy. African Journal of Disability. 2018;7:1-12. doi: https://doi.org/10.4102/ajod.v7i0.437 [ Links ]
48. Mlenzana NB, Eide A., FrantzJ. Perceptions and satisfaction of caregivers regarding rehabilitation services from selected rehabilitation centres in the Western Cape. African Journal of Disability. 2018;7(1):1-5. doi: https://doi.org/10.4102/ajod.v7i0.415 [ Links ]
49. Richter LM, Daelmans B, LombardI J, Heymann J, Boo FL, Behrman JR, Lu C, Lucas JE, Perez-Escamilla R, Dua T, et al. Investing in the foundation of sustainable development: pathways to scale up for early childhood development. Lancett. 2018;389(10064):103-118. doi: https://doi.org/10.1016/S0140-6736d6te1698-1 [ Links ]
50. Republic of South Africa. South Africa's 2030 Strategy for Early Childhood Development mêmes. Department of Basic Education. 2023. https://www.education.gov.za/Portals/0/ODGWorkspace/2024Lekgotla/South_Africas_2030_Strategy_for_EarlyChildhood_Development_Programmes_FINAL.pdf?ver=2024-03-13-105446-230 [ Links ]
51. Erasmus L. ECD Diagnostic: Evaluation of findings and implementing changes. DPME/DSD Roundtable. 2015. https://www.dpme.gov.za/keyfocusareas/evaluationsSite/Evaluations/ECD_Diagnostic_15_04_28.pdf [ Links ]
52. Vargas-Baron, E, Small, J, Wertlieb, D, Hix-Small, H, Gomez Botero, R, Diehl, K, Vergara, P. & Lynch, P 2019, Global survey of Inclusive Early Childhood Development and Early Childhood Intervention programs. RISE Institute, Washington. https://pureoai.bham.ac.uk/ws/portalfiles/portal/68263167/Global_Survey_IECD_ECI_Programs_2019_Accessible.pd [ Links ]
 Correspondence:
Correspondence:
Denise Franzsen
Email: denise.franzsen@wits.ac.za
Submitted: 4 November 2024
Reviewed: 3 September 2025
Revised: 7 September 2025
Accepted: 8 September 2025
* Post Graduate Student at the University of the Witwatersrand at the time of the study.
EDITOR
Blanche Pretorius
https://orcid.org/0000-0002-3543-0743
DATA AVAILABILITY
Upon reasonable request, from the corresponding author
FUNDING
No funding was received for this study
