










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Higher Education
On-line version ISSN 1753-5913
S. Afr. J. High. Educ. vol.40 n.1 Stellenbosch Mar. 2026
https://doi.org/10.20853/40-1-6534
GENERAL ARTICLES
Improving biostatistical support in a resource-constrained academic health sciences institution through 360-degree feedback
E. LibhaberI; B. KramerII; M. MabhikwaIII; J. LevinIV; M. PapathanasopoulosV; I. MaposaVI
IUniversity of the Witwatersrand, Johannesburg, South Africa. Health Sciences Research Office, Faculty of Health Sciences. https://orcid.org/0000-0002-7043-4002
IIUniversity of the Witwatersrand, Johannesburg, South Africa. School of Anatomical Sciences, Faculty of Health Sciences. https://orcid.org/0000-0002-8779-7491
IIIUniversity of the Witwatersrand, Johannesburg, South Africa. School of Public Health, Faculty of Health Sciences
IVUniversity of the Witwatersrand, Johannesburg, South Africa. School of Public Health, Faculty of Health Sciences
VUniversity of the Witwatersrand, Johannesburg, South Africa. School of Pathology, Faculty of Health Sciences
VISchool of Global Health, Faculty of Health Sciences, Stellenbosch University, Bellville, South Africa
ABSTRACT
A comprehensive biostatistical support service was established in a resource-constrained health sciences institution in sub-Saharan Africa in order to enhance its research. A 360-degree feedback survey was used to evaluate the perceptions of consultees and consultants on one-on-one biostatistics consultations in this constrained setting. Self-administered, online surveys with closed and open-ended questions were distributed to health sciences students and academic staff. A separate questionnaire was compiled for the biostatistics consultants. Responses were received from 361 consultees and 23 consultants following one-on-one biostatistical consultations. Consultations had positively assisted with understanding the direction of the research (64.3%). Both consultees and consultants concurred on the views expressed of the expectations, perspectives and weaknesses of the consultations. The level of statistical knowledge and technical skills of the biostatisticians was commended. Consultants mentioned difficulties in understanding the medical terminology of the consultees and the problem of explaining complex statistical concepts to the consultees. Recommendations from this 360-degree survey emphasizes the need to capacitate junior consultants in consultancy skills and in a basic biomedical subject, as expansion of biostatistics support in resource-constrained environments around the globe is not always possible.
Keywords: optimizing biostatistical services, one-on-one consultations, academic health sciences institution, biostatistical training, resource-constrained environment
INTRODUCTION
Research excellence is the gold standard of any academic institution in the world, whether from a high-income status or a low-income status (Kramer and Zent (2019). The enormous burden of disease (Machekano et al. 2015, Confraria and Wang 2020) continues unabated in the resource-constrained regions of the world (Perez-Iratxeta and Andrade 2002) and yet forms an important resource for research in improving patient health and quality of care. While research outputs emanating from the African continent (Perez-Iratxeta and Andrade 2002) continue to be relatively low, relevant health sciences and clinical research from this continent must be shared globally as it contributes valuable knowledge of both infectious and non-communicable diseases. Biostatistics is central to accomplishing high quality health sciences research. In resource-rich countries, Schools of Medicine and Public Health generally provide strong biostatistical support through collaboration between individuals from the disciplines of epidemiology, biostatistics and clinical medicine (Rubio et al. 2011, Strom et al. 2012, Perkins et al. 2016, Spratt, Fox, Mazumdaar 2017). These collaborations result in enhanced interdisciplinary research (Strom et al. 2012). In addition, in order to assist with developing stronger biostatistical resources, some institutions in resource-rich regions offer assistance to institutions in resource-constrained settings (Bandigwala et al. 2002, Olawale 2011). Such an example is the Translational and Clinical Sciences Institute at the University of North Carolina Chapel Hill and the Department of Statistics at Virginia Polytechnic Institute, US which provide ongoing statistical services in both theoretical and practical usage as well as applied statistics to many institutions in low and middle-income countries (Bandigwala 2002, Olaomi 2007, Olawale 2011, Goshu 2016, Spratt et al. 2017). Institutions in resource-rich countries have a robust approach to the inclusion of biostatistics as part of interdisciplinary collaboration, while in Africa more needs to be done to encourage these types of collaborations (Strom et al., 2012, Welty et al. 2016, Spratt et al. 2017, Kramer and Zent 2019). Thus building capacity in biostatistics in Africa (Omaswa 2014, Kirby 2014) and in other resource-constrained regions is important in the undertaking and dissemination of research.
In Sub-Saharan Africa (SSA), many biomedical publications are a product of international collaboration (Fonn et al. 2018). There is thus, a need to strengthen the biostatistical knowledge and training of local individuals to enable increased independent research from this region. In SSA, where the burden of disease is overwhelming and the countries are resource-constrained, physicians and registrars (internists) have had limited research training due to clinical demands, often resulting in an inability to engage in robust scholarly work (Fonn et al. 2018).
Some of the additional challenges in Africa to providing biostatistical support are internet and mobile access, limited access to technology, language barriers, financial constraints (van Zyl et al. 2021) and the lack of trained biostatisticians (Reddy et al. 2023) Thus, training and support in biostatistics would help to improve the scholarship and careers of healthcare academics (Machekano et al. 2015, Libhaber, Chirwa, Kramer 2019).
As the amount of research data is increasing in volume and complexity, the inclusion of a biostatistician as an essential member of the research team in resource-constrained countries would facilitate enhanced research excellence, translation and dissemination (Welty et al. 2013). However, there is a shortage of biostatistics expertise, a lack of biostatistical awareness and hence limited biostatistics consultation services in SSA countries (Olaomi 2007, Machekano et al. 2015, Chirwa, Kramer, Libhaber 2015). While it is important to foster biostatistical collaborations between resource-rich and resource-constrained institutions, it is more important to ensure biostatistical competence and provide ongoing biostatistical support within the communities of research-constrained institutions themselves.
In 2008, in order to develop capacity in its own researchers, the Faculty of Health Sciences (FHS), University of the Witwatersrand (Wits), Johannesburg, South Africa (which is a resource-constrained institution) developed a variety of research support services for researchers and postgraduate students (Kramer and Libhaber 2018). In addition to a comprehensive biostatistics support service, which includes one-on-one consultations, workshops in advanced statistics, sample size calculation, data management and data analysis are also provided (Chirwa et al. 2015, Kramer and Libhaber 2018, Libhaber et al. 2019 ). As part of an assessment of the biostatistical service in the Health Sciences Research Office (HSRO), a survey of the consultation platform was undertaken between 2010 - 2012 (Chirwa 2015) and again between 2013-2017 (Libhaber et al., 2019). While the platform was regarded as worthwhile by the participants, some weaknesses such as insufficient facilitators, structural difficulties with the office space in which consultations were made, insufficient slots for consultations and insufficient time for analysis were identified (Chirwa et al. 2015). It is important to develop the capacity of the consultees in the biostatistics system, as financial constraints do not allow for the expansion of the service (Chirwa et al. 2015, Kramer and Libhaber 2018, Libhaber et al. 2019).
In general, (bio)statistical consulting is defined as the interaction or collaboration of a biostatistician with health professionals in which biostatistical knowledge and expertise is applied to enable the research process (Kirk 1991, Agarwal 2020). These consultations generally begin with study design, followed by data analysis and conclude with the interpretation and publication of the results (Kirk 1991, Agarwal 2020). Authors (Gibbons and Freund 1980, Zahn and Isenberg 1983, Kirk 1991, Olaomi 2007, Agarwal 2020) have reported that (bio)statistical consulting is a complex activity that requires both statistical and non-statistical skills. Importantly both skills have been shown to lead to the success of a consultation and therefore to the outcomes of the research (Johnson and Warner 2004).
Different approaches on how to improve the quality and the efficiency of biostatistical consultations, mainly from the clients' perspective, have been reported in the literature (Johnson and Warner 2004, Pelfrey et al. 2017, McKinneyet al. 2019). However, limited information is available on how to optimize biostatistical consultations in an academic healthcare setting where human resources are scarce, funding is restricted and the burden of clinical work reduces the time for research and data analysis (Chirwa et al. 2015, Kramer and Libhaber 2018, Libhaber et al. 2019).
The current study thus, aimed to assess the perceptions of both the consultees and the consultants of one-on-one biostatistical consultations provided by the HSRO. This 360- degree feedback provides a method for continued education in biostatistical skills. Understanding these dynamics may help in identifying opportunities for further development of biostatistics consultations in this resource-constrained environment, improving knowledge and skills of consultees and consultants and as a consequence, may improve the biostatistical service and training.
METHODS
Study design and setting
The study has been performed in accordance with the Declaration of Helsinki and has been approved by the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (ref no: M1909106).
The first part of the study on the perceptions of consultees and consultants was a descriptive, cross-sectional study. Information was obtained by questionnaires administered to consultees and consultants following one-on-one biostatistics consultations, which took place in the HSRO of the FHS, Wits during 2018.
Sample
The one-on-one biostatistics consultations are comprised of one consultee and one consultant per consultation. A total of 361 responses from consultees and 23 from consultants were obtained and used in this study. Consultees were undergraduate and postgraduate students and clinical and non-clinical academic staff (some of whom were undertaking postgraduate degrees) from the FHS. These individuals required biostatistical input on one or more of research design, sample size and power calculation and data analysis. The consultants were either an academic staff member with a PhD in biostatistics, or postgraduate students undertaking a MSc or PhD degree in epidemiology and biostatistics. The staff members are all funded by the institution. The MSc and PhD students had received a scholarship and one of their duties as part of the scholarship was to provide consultations in biostatistics. All new consultants shadowed an experienced consultant prior to starting consultations and were supervised by a senior biostatistician in the HSRO. Consultations for postgraduate students, clinicians and other researchers were offered on four days of the week for 10 months of the year. The time per consultation was generally limited to 45 minutes, without scheduled appointments and were free of charge.
Instruments
In order to assess the experiences and perceptions of both consultees and consultants on the quality of the consultations, two different questionnaires were utilized. At the end of the consultation, the consultees completed an anonymous, closed questionnaire (Chirwa et al., 2015) which included a) demographic details and the nature of the consultation and b) an evaluation of the quality of the service (Chirwa et al. 2015, Libhaber et al. 2019). The survey was modified to include a question on continued ability, was optional and following completion, it was placed in a sealed box in the HSRO made available for this purpose. The consultants (n=23) received a separate anonymous questionnaire which was a self-administered, on-line questionnaire. The latter questionnaire included a section on socio-demographic information and a section on the perception of the one- on- one consultation, which consisted of four closed questions (Earnest 2016, chapter 11). In addition, both consultees and consultants responded to three open-ended questions about strengths and weaknesses of the one-on-one biostatistical consultations and suggestions for improvements of the service.
Data management and analysis
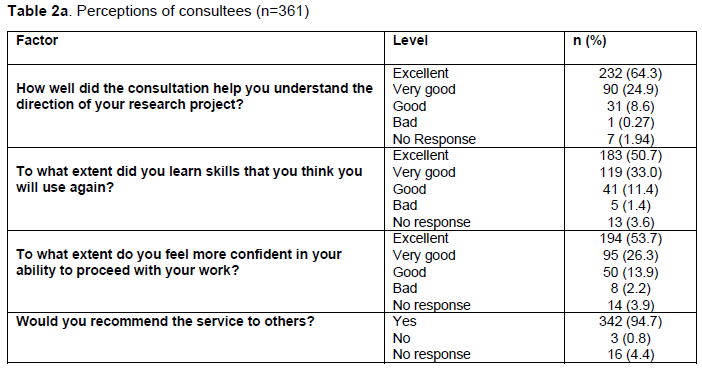
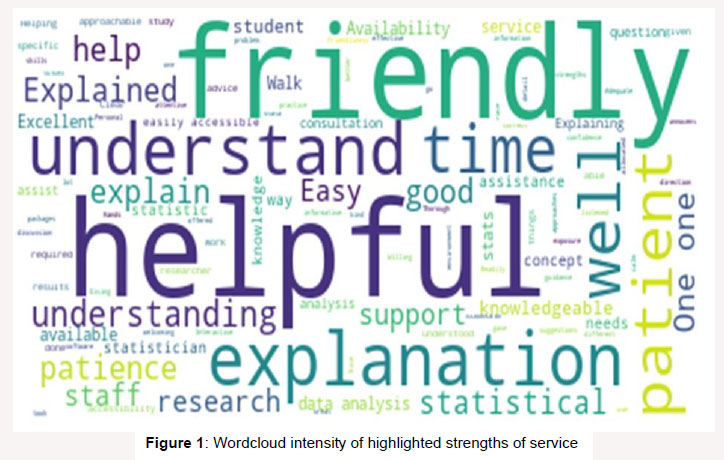
Data from the consultees' questionnaires were entered into a Microsoft Excel spreadsheet and transferred to Stata SE v15.0 for Windows (Stata Corp, College Station, Texas, USA) for analysis. The results were presented as frequencies with corresponding percentages. Perception on the service was assessed by three questions: "How well did the consultation help you to understand the direction of your project?", "To what extent did you learn skills you think you will use again" and "To what extent do you feel confident to proceed in your work". A Likert scale was used to categorise the responses as excellent, very good, good, bad and very bad. Data from the self-administered online questionnaire for consultants were captured into REDCap (Research Electronic Data Capture), a web-based application (Harris et al. 2019). Open-ended responses from both consultees and consultants were captured into a Microsoft Excel spreadsheet for further management and qualitative analysis. The three open-ended questions were used to qualitatively analyse the consultees' perceptions on strengths, weaknesses and improvements by means of thematic analysis. An initial set of codes was developed based on the responses. Two authors (EL and IM) coded the responses independently to ensure validity using an inductive approach. The authors then discussed the codes to achieve consensus and then grouped the codes into themes. The responses were imported into Python for text analysis and results were presented as word-cloud intensity figures. The word-cloud intensity analysis was compared to generated themes and codes, and figures were reported.
RESULTS
Characteristics of the consultees and consultants
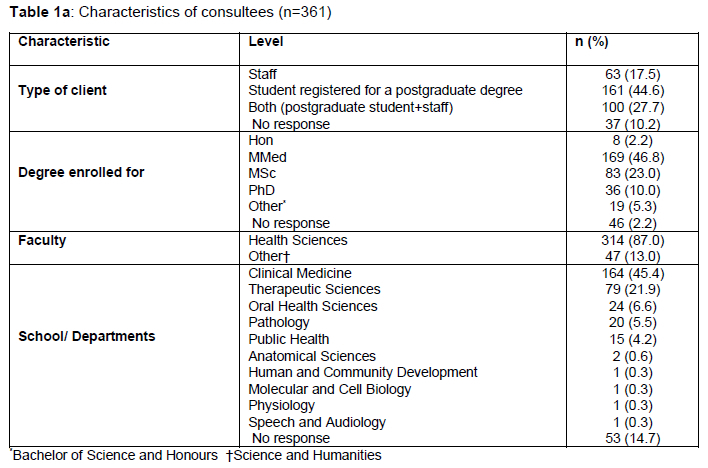
Of the 761 consultees who attended one-on-one consultations in 2018, 361 answered the questionnaire, of which 44.6 per cent were postgraduate students and 27.7 per cent were staff members who were also registered for a postgraduate degree (Table 1a). Registrars (internists) enrolled for a Master of Medicine (MMed) degree made up the bulk of the consultees (46.8%).
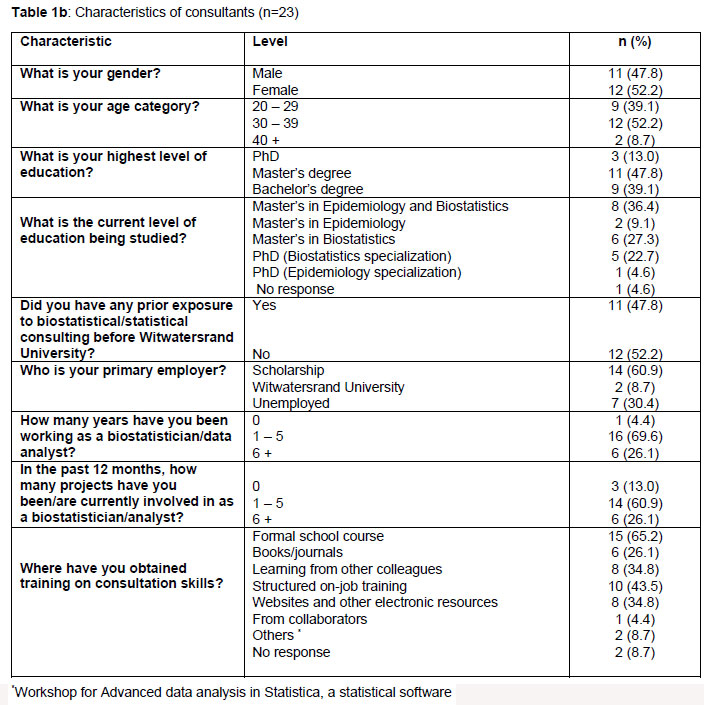
Of the 23 consultants, most were female (52.2%) and were aged 30-39 years (Table 1b). Only 13 per cent held a PhD and the majority were studying towards a Master's degree in Epidemiology and Biostatistics. Almost half of the consultants (47.8%) had prior exposure to conducting biostatistical consultations, with 15 (65%) individuals indicating that they obtained training for consultation skills through a formal course. All consultants except one had more than one year of experience as a biostatistician (Table 1b)
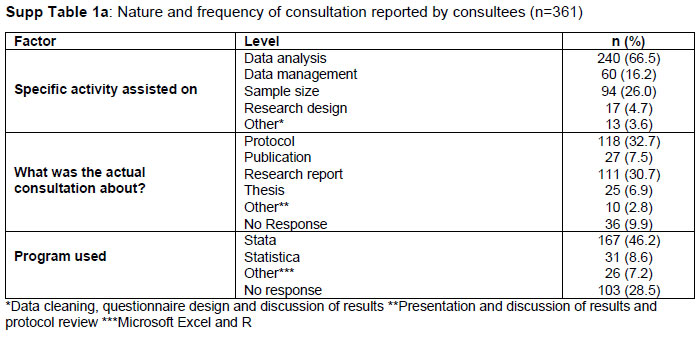
Of the 361 questionnaires answered by the consultees, 66.5 per cent individuals had received input on data analysis and 26 per cent had consulted about sample size related calculations (Sup Table 1a). Most consultations were on the statistical aspect of the development of research protocols (32.7%), while 30.7 per cent were on research reports/theses. The STATA statistical package was generally used (46.2%) by consultees. Only 7.5 per cent of the consultations were related to statistical assistance for publications not related to research towards a postgraduate degree.
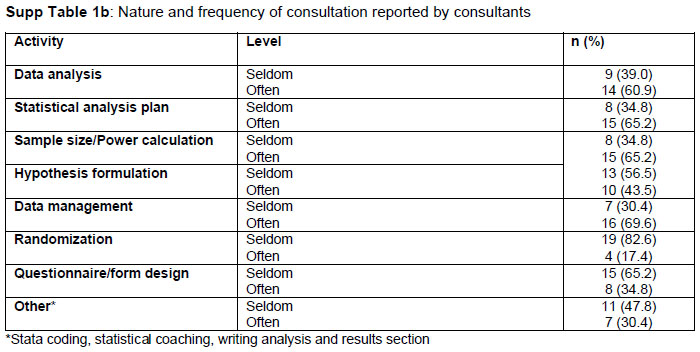
The distribution and frequency of the nature of the consultations reported by consultants are depicted in Sup Table 1b. The items on which consultations were most often recorded were data analysis, statistical analysis plans, sample size/power calculation and data management consultations.
Perceptions of consultées and consultants on services
Over half of the consultées (n=232, 64.3%) reported that the consultation was "excellent" and assisted them in "understanding the direction of the research project" (Table 2a). Almost all the consultees mentioned that they would recommend the service to others (94.7%). Only eight consultees indicated that they did not "feel more confident in their ability to proceed with their work" and five selected "bad" as the extent of their learning, use of biostatistical skills and their ability to use them again.
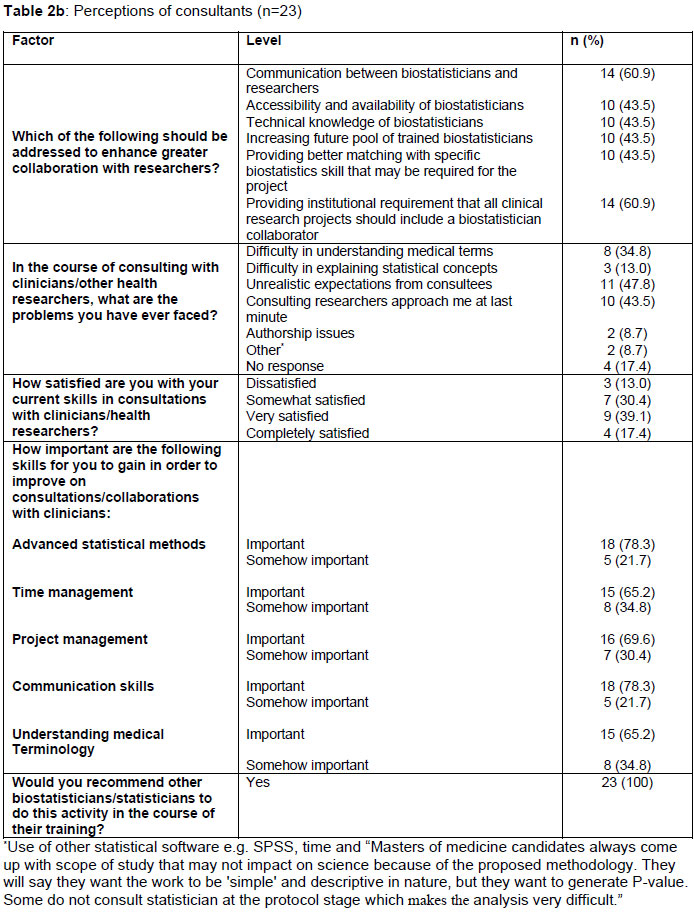
Of the 23 consultants, 60.9 per cent felt that the level of communication between biostatisticians and consultees was warranted (Table 2b). The same percentage of consultants also felt that that all clinical research projects should include a biostatistician to enhance greater collaboration with researchers (Table 2b). Challenges, which consultants remarked on, were difficulty with understanding medical terms, unrealistic expectations from consultees (47.8%) and "researchers approaching the consultant at the last minute" (43.5%). Only three (13%) of the consultants were dissatisfied with their current skills at the time of the consultation. Advanced statistical methods, time management, project management, proficiency in communication and understanding medical terminology were skills ranked as "important" by the consultants in order to improve the service (Table 2b). All consultants agreed that they would recommend other biostatisticians who were currently in training to participate in this activity.
Identified strengths, weaknesses and proposed improvements
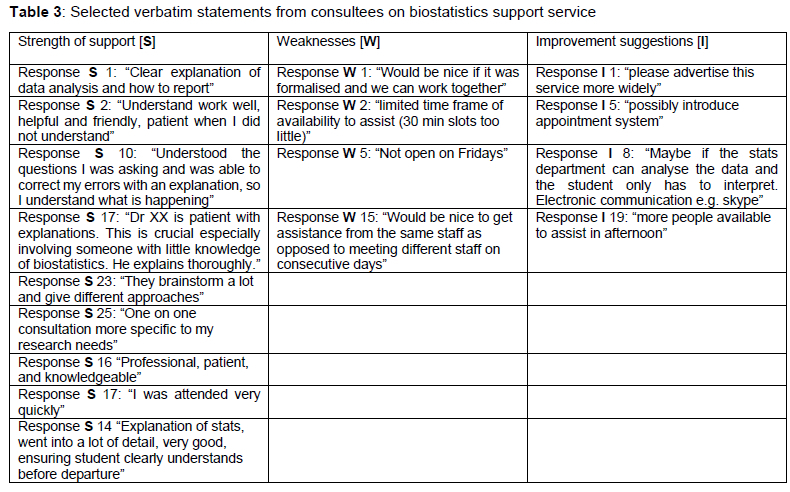
The major strengths of the biostatistics consultancy services highlighted by consultees included the friendliness of consultants, the professionalism (understanding consultees and their research problems, as well as taking time to explain the statistical solutions) and also the technical prowess and knowledge of solving statistical problems (Figure 1; Table 3).
"They brainstorm a lot and give different approaches." (Respondent: S 23)
"Professional, patient and knowledgeable" (Respondent: S 16)
"Explanation of stats went into a lot of detail, very good, ensuring student clearly understands before departure" (Respondent: S 14)
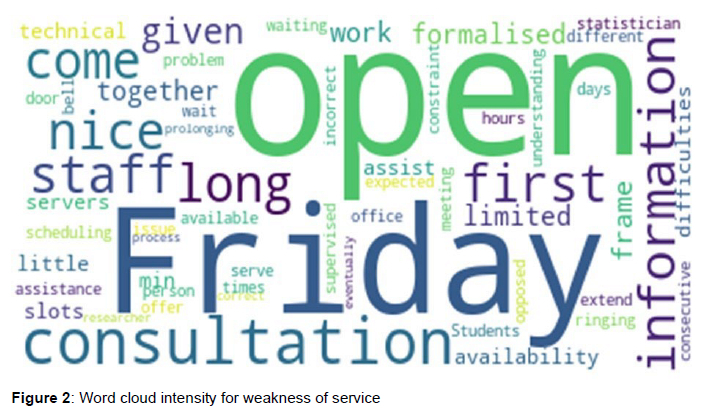
Suggestions to improve the service mirrored the weaknesses reported by the consultees (Fig. 2). The principal weakness of the consultation system was that the service is generally closed on one day a week (Friday) (Fig. 2). Consultees felt the service should be open throughout the week. The other highlighted issues included broader communication of the service to all departments and Schools in the FHS. Consultees also requested that the same consultant should assist them in ongoing consultations, rather than seeing different consultants on different days.
"Would be nice to get assistance from the same staff as opposed to meeting different staff on consecutive days." (Respondent: W 15)
Time allocation per consultation was also raised as a weakness. Some consultees felt the time allocation of 45 minutes was not sufficient to assess the analysis of the data to completion. Consultees also requested increased length of time of the consultation, more allocation of slots for consultations throughout the day, broader advertising and the ability to make bookings either telephonically and/or online (Table 3).
DISCUSSION
There are already a number of systems in the Wits FHS for biostatistical training, such as courses in basic and advanced biostatistics and a biostatistics consultation hub in Global Surgery (NIHR Global Health Research Unit, 2023) where young statisticians are mentored and trained through hands-on supervision. However, feedback on service is important for strengthening our training and hence a quantitative and qualitative survey was promoted to provide feedback/criticism/opinion on consultation procedures specifically.
Both consultees and consultants revealed a high level of concordance of their expectations and perspectives of the consultations. In addition, consultees and consultants expressed similar views on the weaknesses and recommended improvements of one-on-one statistical consultations. There was little difference between the nature of the strengths and weaknesses mentioned in the current study to that in previous surveys carried out in the HSRO (Chirwa et al. 2015, Libhaber et al. 2019) except that the consultants' perceptions concurred with that of the consultees. Despite improvements made to the platform up to 2017, the consultees still persisted in their requests for "more" - more time, more slots and more advertising.
Johnson and Warner 2004, and Niland et al. 1995. described the reported strengths of consultations undertaken at various universities in USA as friendliness, helpfulness, detailed explanations and understanding the research problem. Statistical skills such as the ability to understand the research involved in the consultation, the willingness to explain how and why to apply specific statistical methods and also the interpretation of the results (Olaomi 2007); are essential for a consultant. Consultants should also demonstrate collaborative skills and personal qualities such as establishing rapport with the client (Niland et al. 1995, Zahn and Isemberg 1983, Johnson and Warner 2004). All these aspects were positively highlighted by the consultees in the current study drawing similarities to international institutions.
In order to efficiently conduct a consultation, two aspects of the process need to converge: the client's expectation and the consultant's competency and personality (Johnson and Warner 2004, Olaomi 2007, Agarwal 2020,). However, sometimes the expectation of consultees are considered unrealistic, mainly because of their limited of statistical knowledge, or not understanding the time required for analysis of data (Kirk 1991, Agarwal 2020). In the present study, unreasonable expectations by the consultees were interpreted as a weakness of the consultation, which resulted in a dissatisfied client and consultant.
Similarly to what was found in the current study, Johnson and Warner 2004 and Agarwal 2020 also showed that consultants felt that communication between the parties (consultants and consultees) was an important aspect that needed attention, while understanding medical terminology and advanced statistical methods were some of the key attributes (Earnest 2016, chapter 11). The consultant may not have sufficient content expertise and thus may sometimes find themselves frustrated in their efforts to assist clinicians who struggle to formulate a testable research question (McKinney et al. 2019). A possible challenge for the consultant is the lack of understanding of medical terminology. When reviewing the curricula for the training of biostatisticians in health sciences academic institutions, consideration for the inclusion of training in a basic biomedical subject may thus be necessary. An alternative is for the consultant to extend the consultation and ensure that the consultee carefully explains the discipline in which the research problem resides. Our approach has been to implement a step-wise increment in training for the consultees based on the feedback received from consultations (Kramer and Libhaber 2018).
In addition, consultees in the present study remarked on "availability" as the initial attribute of a satisfactory consultation. Consultees required that the consultation be provided without a delay. Almost half of the consultees who were pursuing a postgraduate degree were from clinical medicine (47%). Usually postgraduates from clinical disciplines where clinical workloads are substantial, demand immediate assistance when they are available. In our institution, the HSRO "walk-in" biostatistical consultations accommodate these requirements as the appointments are not scheduled, but are on a "first-come, first-served" basis. However, in order to cater for all consultees arriving at the HSRO, the time per consultation has been limited and particular days of the week were dedicated to the consultations. This was highlighted in the questionnaire as a weakness. Both the current consultants and consultees surveyed agree that the time allocations for the service should be improved through the provision of additional time slots. This could be achieved by adding on-line scheduled bookings, telephonic consultations, extending the time per consultation and also adding an extra day of consultations. In addition to the existing modalities such as a walk-in consultation facility, the biostatistical consultation service in the Wits HSRO could be improved by inclusion of further options such as scheduling appointments online, via email, telephonic (WhatsApp) and Zoom meetings. The format of the one-on one consultation could be extended to consist of a brief consultation to determine the nature of the problem, followed-up by a consultation to address the problem and then a final telephonic / email outcome of the process.
While statistical services across different fields of study are firmly entrenched in many institutions in resource-rich countries, in recent years a number of programs in statistics training have been initiated in Africa, Asia and South America with North American counterparts (Bandigwala et al. 2002, Johnson and Warner 2004, Olaomi 2007, Deutsch et al. 2007, Olawale 2011, Perkins et al. 2016, Goshu 2016).
In recent years there has been a renewed focus on education in biostatistics in Africa and the development of partnerships and consortia to sustain this training (Gezmu et al., 2011, Machekano et al. 2015, Chirwa et al. 2020, Shepherd et al. 2023). The challenges faced throughout Africa with respect to strengthening biostatistics are largely the same. There remains a strong need to strengthen health systems in response to infectious diseases (Gezmu et al. 2011, Machekano et al. 2015) to increase research capacity (Machekano et al. 2015), and for young researchers insufficient access to biostatistical support (Shepherd et al. 2023]. As a result of the common challenges facing health sciences researchers in Africa, large Consortia such as the Sub-Saharan Africa Consortium for Advanced Biostatistics (SSACAB) are attempting to drive changes in collaborative masters and doctoral supervision in biostatistics training by pooling of financial and supervisory resources (Chirwa et al. 2020). These consortia focus mainly on the training of individuals in their role as future biostatisticians and not on the institutional support systems which are needed to sustain the training, research and dissemination of information produced by academics. The current study focuses on developing sound institutional support for academics.
There are important mechanisms that could be introduced to strengthen consultation services across Africa. Statistical consultation skills should be incorporated into postgraduate curricula of (bio)statisticians (Olaomi 2007, Olawale 2011, Deutsch et al. 2007), similar to the training, which occurs in institutions of resource-rich countries. As evidence-based information plays an important role in both training and research, there is also a pressing need to introduce biostatistics training at undergraduate health sciences level (Willie et al. 2012, Vasudevan 2016). This could be done as short online courses. The introduction of basic statistical terminology for the undergraduate students and biological terms for the biostatisticians in-training are also recommended and could be arranged through online courses from published material. A health sciences research project, limited in scope, would also expose the biostatistician in-training to aspects of biomedical research such as critical appraisal of research methodology into which statistics is incorporated, and ensure an understanding of biomedical research. A regional approach across Africa, communicating and collaborating on the existing challenges as elucidated in this study, such as the understanding of biomedical terminology by biostatisticians, and the need to capacitate junior consultants in consultancy skills, would assist in the alleviation to some of the challenges. These recommendations can be introduced without major cost implications.
Many publications from resource-rich countries refer to the skills, scope, areas of expertise of biostatisticians or strategies of centralizing biostatistics resources (Niland et al. 1995, Deutsch et al. 2007, Welty et al. 2013, Vance 2015, Perkins et al. 2016, Spratt et al. 2017). In our institution, a biostatistical research unit is centralised only in the FHS, where biostatistical support has been ongoing since 2008 (Kramer and Libhaber 2018). Training of the junior consultants who assist researchers has been a priority to ensure adequate levels of skill when undertaking consultations on their own. This has been supported by the supervision, shadowing and mentoring of a junior consultant by a senior biostatistician as is highlighted by institutions such as Yale, Cambridge and North Carolina (Bandigwala 2002, Olaomi 2007, Welty et al. 2013). Therefore, the approach to "teaching" consultancy following graduation with a degree in biostatistics should be by first shadowing experienced biostatistical consultants and later conducting supervised consultations (Libhaber et al. 2019). Alternatively, a course in consultancy could be incorporated in the biostatistics curriculum (Olaomi 2007). Receiving additional exposure to medical or health-related projects will ensure optimal consultation skills for the junior consultant (Olaomi 2007).
One of the difficulties in the Wits FHS has been to ensure that researchers, particularly from the clinical disciplines, include a biostatistician in the initial stages of the process of their research (planning stage) (Spratt et al. 2017). Early collaboration with a (bio)statistician should become a priority in all the disciplines of health sciences (Spratt et al. 2017, LeBlanc et al. 2022) and may ensure better-planned research and promote research excellence. The value of biostatisticians goes well beyond assisting researchers in calculating sample size and doing the data analysis (Ciolino 2021). They should be viewed as full collaborators who are incorporated into studies ab initio.
Generally, the importance of biostatistical services as described in the current setting, assist with the formulation, analysis and writing of quality health sciences research for international dissemination and the production and completion of quality postgraduate degrees. Biostatistical services such as these also create an awareness of the role that the biostatistician and biostatistics play in the generation of research. Thus, existing biostatistical services should be strengthened to provide adequate support to researchers and where a service does not exist in a health sciences facility, it should be initiated.
Overall, the outcome of the study indicates the need to implement changes to the current format of the biostatistical consultations. As in any business, the long-term goal is to have satisfied customers (Parker 2000, Glickman et al. 2010). This applies equally to the biostatistical consultation service being provided to health sciences academics. The direction and advice provided by a biostatistician during consultations both prior to and throughout the analysis of research should lead to a robust output. Ongoing collaborations between biostatisticians and researchers, which may result from these consultations, will strengthen the quality of the research through multidisciplinary involvement.
STUDY LIMITATIONS
Some of the limitations of this study included the moderate response rate (47.3 %), the cross-sectional nature of the study design and the non-responses to some questions in the survey by the consultees, which may have skewed the appreciation of the consultations. Lastly each "consultation" was analysed and interpreted as unique, and was not adjusted for continuance of the consultation with the same/different consultant.
CONCLUSIONS
This study analysed both the perceptions of the consultees and the consultants, thus enabling a holistic view and 360-degree feedback of the one-on-one biostatistics consultation process, and provided insights to further optimize consultations and training of the consultants in a resource-constrained environment. Biostatisticians could work individually performing consultations and/or collaborating in a research team depending on the status and experience of the consultants (junior or senior). Training of junior consultants in consultancy, biomedical terminology and collaborative skills is imperative and could occur during formal training in biostatistics (Esterhuizen et al. 2021, LeBlanc et al. 2022).
The formal training of junior biostatisticians is important and should become mandatory in our setting in order to enhance and sustain the biostatistical consultation service. Having already moved to online platforms during 2020, future work will focus on introducing a tracking system (Pelfrey et al. 2017). In the future, the research productivity of the FHS could be used as an indicator of the effectiveness of the biostatistical service provided. A systematic and reliable approach to analysing publication output and graduations per biostatistical consultation over time should be sought.
ACKNOWLEDGEMENTS
We thank Ms Shae Lazarus for assisting with the data collection.
FUNDING
The present research did not receive any funding on design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
DISCLOSURE STATEMENT
All authors (EL, BK, MM, JL, MP and IM) declare that they have no competing interests
ETHICAL APPROVAL
Ethical approval has been granted by the Human Research Ethics Committee (Medical) of the University of the Witwatersrand (ref no: M1909106).
DISCLAIMERS
None
PREVIOUS PRESENTATIONS
None
AUTHOR STATEMENT
EL and IM: conceptualization, study design, analysis, literature review, writing, editing of the manuscript and substantial revision; MM: data acquisition, data analysis and literature review; BK: result interpretation, writing of the manuscript, editing and substantial revision; MP and JL: result interpretation and substantial revision of the manuscript All authors read and approved the manuscript
DATA AVAILABILITY
The datasets used and analysed during this study are available from the corresponding author on reasonable request
REFERENCES
Agarwal, G.G. 2020. "Statistical consulting and its challenges. Review article". IJCMCR, 1(1) open access https://doi:10.46998/IJCMCR2020.01.000015 [ Links ]
Bangdiwala, S.I., M. L. Amarillo, S. Ughade, et al. 2002. "Teaching consultancy through direct experience in research: The Approach of the department of Biostatistics at the University of North Carolina at Chapel Hill". ICOT, 6 (9),1689-1699. [ Links ]
Ciolino, J.D., C. Spino, W. T. Ambrosius, et al. 2021. "Guidance for biostatisticians on their essential contributions to clinical and translational research protocol review". J Clin Transl Sci, 5, e161, 1-13. https://doi.10.1017/cts.2021.814 [ Links ]
Chirwa, T., B. Kramer, and E. Libhaber. 2015. "Developing a biostatistical support system in a resource-restricted academic institution in Africa: making it happen". BMC Medical Education, 15, 209. https://doi.:10.1186/s12909-015-0493-0 [ Links ]
Chirwa T. F, Z. Matsena Zingoni, P. Munyewende , et al. 2020. "Developing excellence in biostatistics leadership, training and science in Africa: How the Sub-Saharan Africa Consortium for Advanced Biostatistics (SSACAB) training unites expertise to deliver excellence". AAS Open Res. 3:51. doi: 10.12688/aasopenres.13144.2. PMID: 33501413; PMCID: PMC7802118. [ Links ]
Confraria, H., and L. Wang. 2020. "Medical research versus disease burden in Africa". Research Policy, 49(3), 103916. doi.org/10.106/jrespol.2019.103916. [cited 26 Jan 2021] [ Links ]
Deutsch, R., S. Hurwitz, J. Janosky, et al . 2007. "The role of education in The role education in biostatistical consulting". Stat Med, 26 (4), 709-720. Doi:10.1002/sim.2571 [ Links ]
Earnest, A. 2016. "Essentials of a successful biostatistical collaboration. Views from the ground". Taylor and Francis Group. New York: Chapman and Hall/CRC; chapter 11. [ Links ]
Esterhuizen, T.M., G. Li, T. Young, et al. 2021. "Advancing collaborations in health research and clinical trials in Sub-Saharan Africa: development and implementation of a biostatistical collaboration module in the Masters in Biostatistics Program at Stellenbosch University". BMC Research, Open Access, 22-478. doi.org/10.1186/s13063-021-05427-x [ Links ]
Fonn, S., L. P. Ayiro, L. Cotton, et al.. 2018. "Repositioning Africa in global knowledge production". Lancet, 392, 1163-1166. doi.org/10.1016/s0140-6736(18)31068-7 [ Links ]
Gezmu M, V. DeGruttola, D. Dixon, et al. 2011.. Strengthening biostatistics resources in sub-Saharan Africa: research collaborations through U.S. partnerships. Stat Med. 2011 Mar 30;30(7):695-708. doi: 10.1002/sim.4144. Epub 2011 Jan 12. PMID: 21394746; PMCID: PMC4562470. [ Links ]
Gibbons, J.D., and R. J. Freund. 1980. "Organizations for Statistical Consulting at Colleges and Universities". Am Stat, 34(3), 140-145. https://www.jstor.org/stable/2683870 [ Links ]
Glickman, M., R. Ittenbach, T. G. Nick, et al. 2010. " Statistical consulting with limited resources: Applications to practice". CHANCE, 23 (4), 35-42. doi.org/10.1080/09332480.2010.10739834 [ Links ]
Goshu, A.T. 2016. "Strengthening statistics graduate programs with statistical collaboration- The case of Hawassa University, Ethiopia". International Journal of Higher Education, 5(3), 217-221. doi.org/10.5430/ijhe.v5n3p217 [ Links ]
Harris, P.A., R. Taylor, B. L. Minor, et al.. 2019. "The REDCap consortium: Building an international community of software platform partners". J Biomed Informats, 95,103208. doi:10.1016/j.jbi.2019.103208. [Cited January 2021] [ Links ]
Johnson, H.D., and D. A. Warner. 2004. "Factors relating to the degree to which statistical consulting clients deem their consulting experiences to be a success". Am Stat Assoc, 58, 280-289. doi.org/10.1198/000313004x5806 [ Links ]
Kirby, T. 2014. "Profile: NIHs Fogarty International Centre". Lancet. 384 (9938), 0140-6736(18)31068-7121.10.1016./S0140-6736 (14)61149-1 [ Links ]
Kirk, R.E. 1991. "Statistical consulting in a University: Dealing with people and other challenges". Am Stat, 45, 28. [ Links ]
Kramer, B., and E. Libhaber. 2018. "Closing the barrier between disease and health outcomes in Africa through research and capacity development". Global Health Action, 11, 1425597. doi.org/10.1080/16549716.2018. [ Links ]
Kramer, B. and R. Zent. 2019. "Diaspora linkages benefit both sides: a single partnership experience". Global Health Action. 12, 1. doi.org/10.1080/16549716.2019.1645558 [ Links ]
LeBlanc, M., C. S. Rueegg, N. Bekiroglu, et al. 2022. "Statistical advising: Professional development opportunities for the biostatistician". Stat Med, 41, 847-859. doi: 10.1002/sim.9290 [ Links ]
Libhaber, E., T. Chirwa, and B. Kramer. 2019. "A biostatistical support system in health sciences: is this sustainable in a resource-restricted environment?" Health Res Policy Syst, 17(1), 66. doi:10.1186/s12961-019-0470-x [ Links ]
Machekano, R., T. Young, S. Rusakaniko, et al. 2015. "The Africa Center for Biostatistical Excellence: A proposal for enhancing biostatistics capacity for Sub-Saharan Africa". Stat Me,. 34(27), 3481-3489. doi:10.1002/sim.6572.h [ Links ]
McKinney, C.M., S. Mookherjee, S. D. Fihn, and T. H. Gallagher. 2019. "An academic research coach: An innovative Approach to increasing scholarly productivity in medicine". J Hosp Med, 14, 457-461. doi.org/10.12788/jhm.3194 [ Links ]
NIHR Global Health Research Unit on Global Surgery. Johannesburg Hub. Available from: https://www.globalsurgeryunit.org, [accessed April 2023] [ Links ]
Niland, J.C., T. L. Odom-Maryon., J. Lee, and B. C. Tilley. 1995. "A survey of biostatistical consulting units through North America". Am Stat, 49 (2), 183-189. [ Links ]
Olaomi, J.O. 2007. "Statistical Consulting and the Econometrician". 12th Annual Conference of the African Econometric Society in Cape Town, South Africa between 4th and 6th July, 2007, (March). Retrieved from www.africametrics.org/conference-papers.html [Cited December 2020] [ Links ]
Olawale, A.O. 2011. "Fostering the practice and teaching of statistical consulting among young statisticians in Africa". Journal of Education and Practice, 2(8),13-18. 155N 2222-288x (online) [ Links ]
Omaswa, F.G. 2014. "The contribution of the Medical Education Partnership Initiative to Africa's renewal". Acad Med, 89, S16-S18.doi.:101186/1478-4491-12- S1-I1 [ Links ]
Parker, R.A. 2000. "Estimating the value of an internal biostatistical consulting service". Stat Med, 19 (16), 2131-2145. [ Links ]
Pelfrey, C.M., K. D. Cain, M. E. Lawless, et al. 2017. "A Consult Service to Support and Promote Community-Based Research: Tracking and Evaluating a Community-based Research Consult Service". J Clin Transl Sci, 1(1), 33-39. doi;10.1017/cts.2016.5 [ Links ]
Perez-Iratxeta, C., and M. A. Andrade. 2002. "Worldwide scientific publishing activity". Science, 297, 519. Doi: 10.1126/science.297.5581.519b. PMID: 12143877 [ Links ]
Perkins, S.M., P. Bacchetti, C. S. Davey, et al and the Biostatistics, Epidemiology and Research design (BERD) Key Function Committee of the Clinical and Translational Science (CTSA) Consortium. 2016. "Best practices for biostatistical consultation and collaboration in academic health centers". Am Stat, 70(2), 187-194. doi.org/10.1080/00031305.2015.1077727 [ Links ]
Reddy T, R. N. Nsubaga, T. Chirwa, et al. 2023. "Sustainable Statistical Capacity-Building for Africa: The Biostatistics Case. Annual Reviews. 10, 97-117 https://doi.org/10.1146/annurev-statistics-033021-015609 [ Links ]
Rubio, D.M., D. J. del Junco, R. Bhore, et al. and the Biostatistics", Epidemiology and Research Design (BERD) Key Function Committee of the Clinical and Translational Science Awards (CTSA) Consortium. 2011. "Evaluation metrics for biostatistical and epidemiological collaborations". Stat Med, 30(23), 2767-2777. doi:10.1002/sim.4189 [ Links ]
Shepherd BE, Hussaini NN, Ingles DJ, et al. 2023. Training the next generation of Biostatisticians in West Africa: The Vanderbilt Nigeria Biostatistics Training Program (VN-BioStat). J Glob Health Rep.7:e2023067. doi: 10.29392/001c.88939. [ Links ]
Spratt, H., E. E. Fox, and M. Mazumdar. 2017. "Strategies for success: Early-stage collaborating biostatistics faculty in an academic health center". Am Stat. 7(3), 220-230. doi: 10.1080 / 00031305.2016.12777 157 [ Links ]
Strom, B.L., T. O. Kelly, J. R. Landis, and H. I. Feldman. 2012. "The Center for Clinical Epidemiology and Biostatistics of the Perelman School of Medicine at the University of Pennsylvania: An organizational model for clinical research in a School of Medicine". Acad Med, 87(1), 60-65. doi:10.1092/ACM.06013e31823ab5eI [ Links ]
Vance, E.A. 2015. "Recent developments and their implications for the future of academic statistical consulting centers". Am Stat., 69 (2), 127-137. [ Links ]
van Zyl C, M. Badenhorst, S. Hanekom, M. Haine. 2021. "Unravelling 'low-resource settings': a systematic scoping review with qualitative content analysis". BMJ Global Health, 6: e005190. [ Links ]
Vasudevan S. 2016. "Biostatistics teaching to the undergraduate medical students through research-oriented medical education posting program in a Teaching Medical Institute in Coastal Area of Pondicherry: An experience of a biostatistician." J Pharm Bioallied Sci. 8(1):78-9. doi: 10.4103/0975-7406.171693. PMID: 26957876; PMCID: PMC4766786. [ Links ]
Welty, L.J., R. E. Carter, D. Finkelstein, et al. 2013. "Perspective: Strategies for developing biostatistics resources in an academic health center". Acad Med. 88 (4), 454-460. doi:10.1097/ACM.0b013e31828578ed. [ Links ]
Willie D, T. Ferguson, M. Tulloch-Reid, A. McCaw-Binns. 2012. "Teaching biostatistics and epidemiology: medical students' views on the content and instructional strategies of an introductory course". Caribbean Teaching Scholar 2(2), 103-114. [ Links ]
Zahn, D.A., and D. J. Isenberg. 1983. "Nonstatistical Aspects of Statistical Consulting". Am Stat. 37(4), 297-302. [ Links ]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}