










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSA Orthopaedic Journal
On-line version ISSN 2309-8309Print version ISSN 1681-150X
SA orthop. j. vol.24 n.4 Centurion 2025
https://doi.org/10.17159/2309-8309/2025/v24n4a6
ORTHOPAEDIC ONCOLOGY AND INFECTIONS
Contemporary indications for neoadjuvant chemotherapy for conventional osteosarcoma: results from a survey of South African surgeons and oncologists
Phakamani G MthethwaI,; Leonard C MaraisII
IHead: Department of Orthopaedic Surgery, Consultant: Bone Tumours, Sepsis and Limb Reconstruction; Dr Pixley Ka Isaka Seme Memorial Hospital, Nelson Mandela School of Clinical Medicine, University of KwaZulu-Natal, Durban, South Africa
IISchool of Nelson Mandela School of Clinical Medicine, College of Health Sciences, University of KwaZulu-Natal, Durban, South Africa
ABSTRACT
BACKGROUND: This study describes the contemporary approach to using neoadjuvant chemotherapy (NACT) in high-grade conventional osteosarcoma (COS) of the extremities in South African clinical practice. Secondarily, we determine if any factors were associated with routinely using NACT.
METHODS: A cross-sectional questionnaire-based online survey was performed involving orthopaedic oncology surgeons and medical oncologists working in South Africa on the indications and use of NACT in COS. For statistical analysis, we employed Stata Version 18 and GraphPad Prism analysis to generate descriptive statistics and encode open-ended responses. We used chi-square or Fisher's exact association tests to summarise variables with medians and percentages. Univariate and multivariate logistic regression assessed associations with NACT use in COS, with significance at p < 0.05. The reliability of the survey scale was Cronbach's alpha coefficient (0.6409).
RESULTS: NACT was routinely prescribed by 69% of all respondents. Orthopaedic surgeons were less likely to recommend the use of NACT than oncologists (odds ratio [OR] 0.16; 95% confidence interval [CI] 0.02 to 0.95; p = 0.044). Notably, orthopaedic surgeons were also more likely to treat a high volume of COS cases per annum (OR 0.02; CI 0.002 to 0.25; p < 0.001). Regarding NACT administration without limb salvage, orthopaedic surgeons were less likely to prescribe NACT prior to amputation surgery than oncologists (OR 0.11; CI 0.02 to 0.73; p = 0.041). A public practice clinical setting was associated with worse outcomes regarding disease progression (DP) on NACT (OR +infinity; CI 1.364 to +infinity; p < 0.043) and NACT response rate < 50% (OR 18.33; CI 2.51 to 102.5; p = 0.005).
CONCLUSION: In South African clinical practice, we observed disparities in the approach to treating highgrade conventional osteosarcomas of the extremities among clinicians regarding the use of neoadjuvant chemotherapy. This further elucidates the need for more data pertaining to COS in South Africa to enable the development of pragmatic treatment guidelines tailored to our context to improve outcomes.
Level of evidence: 5
Keywords: high-grade conventional osteosarcoma, neoadjuvant chemotherapy, extremities, South Africa
Introduction
The standard treatment approach for central high-grade conventional osteosarcomas (COS) involves a combination of wide surgical resection and systemic multidrug chemotherapy.1-4 Neoadjuvant chemotherapy (NACT) refers to chemotherapy administered preoperatively to patients, while adjuvant chemotherapy (ACT) follows surgical intervention.1-4 Although there have been numerous studies on the use of chemotherapy in COS there remain some controversies, particularly in terms of the routine use of NACT.5-6
In the 1980s, the shift to adding NACT to treatment protocols was mostly based on anecdotal information and practical considerations rather than high-level scientific evidence.5,7 NACT allowed for assessment of the treatment effect on the primary tumour by evaluating chemotherapy-induced tumour necrosis, serving as a surrogate marker for therapeutic response.5,7 Another rationale, the expeditious initiation of systemic therapies, was viewed by treating physicians as a means to prioritise the treatment of the systemic disease rather than concentrating solely on local control of the primary tumour.5,7 Goorin et al. suggested that surgeons had an unfounded bias towards NACT in that it will improve overall survival due to immediate systemic effects of chemotherapy.5 Furthermore, during the early days of limb salvage surgery, surgeons advocated for NACT to buy time to manufacture custom-made tumour prostheses.5,7 Surgeons also preferred to conduct close-margin resections around tumours that had already undergone systemic treatment with the understanding that the chemotherapy 'sterilised' the reactive zone of microscopic tumour extensions.5,7,8 The proponents of NACT underscored several additional potential advantages, including tumour size reduction, improved visibility of peritumoral oedema in magnetic resonance imaging (MRI) scans, the development of a rind or pseudo-capsule around the tumour, and a noticeable increase in tumour firmness upon palpation.8
However, the argument for NACT has largely diminished with the advent of modular, off-the-shelf implants and the establishment of allograft tissue repositories. While the first rationale persists, Huvos criteria of chemotherapy response offer primarily prognostic information rather than actionable treatment guidance; evidence shows that altering treatment protocols in response to a poor histological response following NACT does not lead to improved outcomes.9-11 While peritumoral oedema improves on MRI studies, osteosarcomas tumours rarely shrink with NACT.8 Importantly, the RCT by the Pediatric Oncology Group showed a similar event-free survival (EFS) rate at Ave years (69 ± 8% for immediate surgery vs 61 ± 8% for presurgical chemotherapy; p-value = 0.8).5 The treatment arms had a similar incidence of limb salvage (55% for immediate surgery and 50% for NACT).5 Approximately 45-55% of COS tumours exhibit a good response to chemotherapy.9-11 Problems with chemotherapy include multi-drug resistance and a host of complications, which include an increased risk of infection.9-11
In South Africa, clinicians generally follow treatment guidelines for NACT that originated in developed countries.12-16 However, in South Africa, good response rates to NACT using these international protocols have been reported to be as low as 21%.12 In low- and middle-income countries (LMICs) like ours, advanced tumour stages at presentation, i.e. Enneking Musculoskeletal Tumour Society stage III, have been associated with poor response to chemotherapy.12-16 The risk of disease progression (DP), defined by Response Evaluation Criteria in Solid Tumours (RECIST) and EURAMOS-1 studies as an increasing disease burden (local, systemic or combined) while patients are on NACT, has previously been identified.17-18 Furthermore, DP while a patient is on NACT confers poor outcomes.19 As a result, clinicians may elect to perform upfront surgery and omit NACT to avoid undue delay in surgical resection of the primary tumour.12-16 Despite the fact that there are only a small number of clinicians working in the field of orthopaedic oncology in South Africa, anecdotal reports suggest a high level of discordance in their approach to NACT. The multidisciplinary nature of treatment, and the fact that treating clinicians come from various specialities, may contribute to this perceived variation. Furthermore, no data currently depicts the indications and efficacy of NACT in South Africa, in contrast to the high-income countries (HICs) where preoperative chemotherapy has become a standard of care.1-4 In a limited-resource environment like ours, the indications for NACT have to be questioned in instances of COS cases where there is clear clinical and radiological evidence of DP (RECIST criteria) on first or second cycles; fungation or ulceration; tumour bleeding; limb salvage being impossible; advanced tumours treated for palliative purposes; or contraindications for immediate chemotherapy and sociocultural aspects.
This study aims to describe the clinicians' attitudes and practices with regard to the use of NACT in high-grade COS of the extremities in South African clinical practice. Secondarily, we determine if any practice setting factors were associated with routinely administering NACT.
Methods
Participants
We performed an observational, cross-sectional, questionnaire-based online survey of South African orthopaedic oncology surgeons and medical oncologists. The necessary ethical approval was obtained from our institutional ethics committee prior to the commencement of the study, and all participants provided informed consent. The study period was from June 2022 to December 2022. The questionnaire was disseminated online across South Africa through the South African Orthopaedic Association (SAOA), South African Societies for Medical Oncologists (SASMO) and the South African Society of Clinical and Radiation Oncology (SASCRO) for distribution to their members. Orthopaedic oncology surgeons and adult and paediatric medical oncologists from both the public and private healthcare sectors involved in treating patients with osteosarcoma in South Africa were considered eligible and invited to participate in the survey. Registrars, medical officers and interns were excluded. Data collection was performed using RedCAP, a secure online software platform that supports data capture in research studies.20
Demographic data collected included: a) specialist qualification, b) duration of practice as a specialist, c) practice setting (private practice/public sector/both), and d) academic affiliation. The osteosarcoma-data survey contained 14 outcome domains to be analysed: a) number of cases treated per annum; b) treatment guidelines used (EURAMOS-1, ESMO, MSTS, other, or each case treated on an individual basis); c) adherence to guidelines; d) relevance of international guidelines to the South African clinical landscape; e) ability to follow international guidelines; f) the perceived need to develop South African-relevant guidelines; g) use of NACT if limb salvage is not an option; h) the preferred NACT regimen; and i) perceived prevalence of chemoresistance to NACT. Regarding chemotherapeutic practices, the participants were also asked about: a) duration of NACT; b) whether they change or intensify their chemotherapy regimens in accordance with the responses to NACT; c) if they use second-line ACT in poor-response cases; and d) the proportion of cases that exhibited local and systemic DP while the patient was undergoing chemotherapy. Finally, the participants were asked about: a) experiences regarding the response rate to the NACT in South Africa; and b) the need for osteosarcoma research groups in South Africa.
Statistical analysis
We employed Stata Version 18 (College Station, TX, Stata Corp LLC) and GraphPad Prism. The survey responses were exported as descriptive statistics, and the responses to open-ended questions were encoded to themes. Non-parametric continuous variables were summarised as medians with interquartile range (IQR), categorical variables were expressed as percentages with counts, and associations were tested using a chi-squared or Fischer's exact test. Univariate binomial logistic regression was employed to assess the associations with the routine use of NACT for all cases of COS. Subsequently, a multivariate logistic regression model (adjusted for all explanatory variables) was constructed using repeated stepwise variable elimination. Statistically significant differences were set at p < 0.05. The reliability of the survey scale was Cronbach's alpha coefficient (0.6409).
Results
Demographic characteristics of the participants
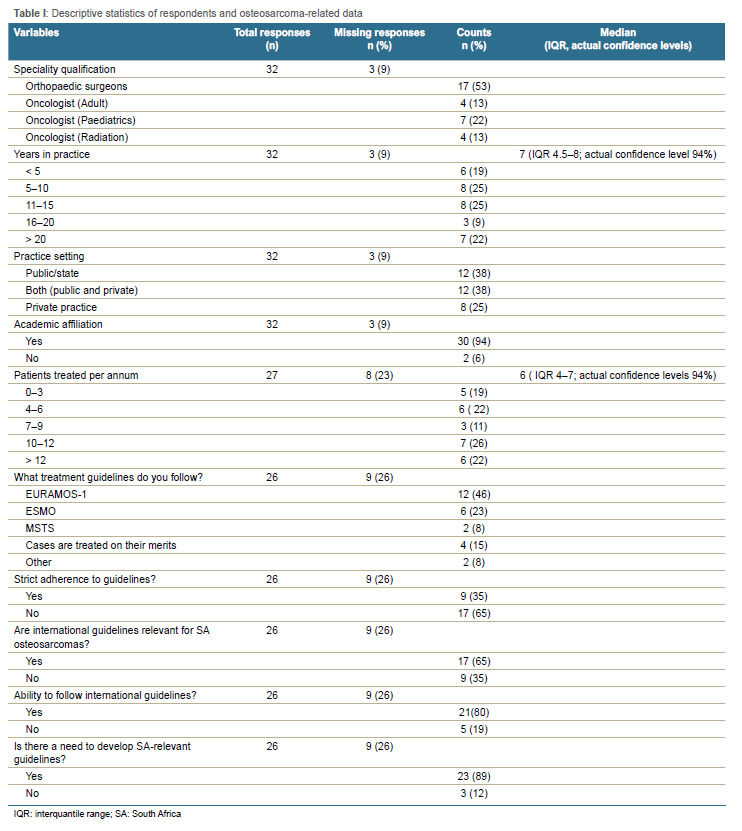
Thirty-five responses were returned; however, two were excluded from the final analysis due to missing data. Respondents comprised 17 orthopaedic surgeons (53%), four adult oncologists (13%), seven paediatric oncologists (22%) and four radiation oncologists (13%) (Table I). The median experience as a qualified specialist was seven years (interquartile range [IQR] 4.5-8.0); actual confidence level [ACI] 94%), with 19% (6 of 32) of participants being in practice for < 5 years and 25% for 5-10 years. Most participants had more than ten years of experience, with 25% (8 of 32) having 11-15 years, 9% 16-20 years, and 22% having > 20 years in practice. Their practice settings comprised private practice 25% (8/32), public practice 38% (12/32)), or both 38% (12/32). Notably, there was an increased proportion of academically affiliated specialists at 94% (30/32) compared with non-academic affiliations at 6% (2/32).
The median distribution of osteosarcoma cases treated per annum was 6.0 (IQR 4.0-7.0; ACI 94%). Eighteen per cent (5/27) of respondents reported seeing 0-3 cases/annum, 22% (6/27) 4-6 cases/annum, 11% (3/27) 7-9 cases/annum, 26% (7/27) 10-12 cases/annum, and 22% (6/27) > 12 cases/annum, with 52% of practitioners (14 of 27) reporting seeing less than ten cases per year. Most clinicians followed the EURAMOS-1 osteosarcoma treatment guidelines (46%; 12/26), followed by 23% ESMO (6/26) and 8% MSTS (2/26). Fifteen per cent (4/26) of specialists did not follow specific guidelines, and 8% (2/26) used other unspecified guidelines. Interestingly, more clinicians did not adhere strictly to these guidelines than those who exclusively used guidelines, at 65% (17/26) and 35% (9/27), respectively. Furthermore, most clinicians (65%;17/26) believe that international guidelines still apply in South African settings compared to sceptical experts (35%; 9/26). Eighty-nine per cent (23/26) of respondents believed there was a need to develop specific guidelines for the South African clinical landscape, compared to 12% (3/26) who thought this was irrelevant.
Osteosarcoma-related data
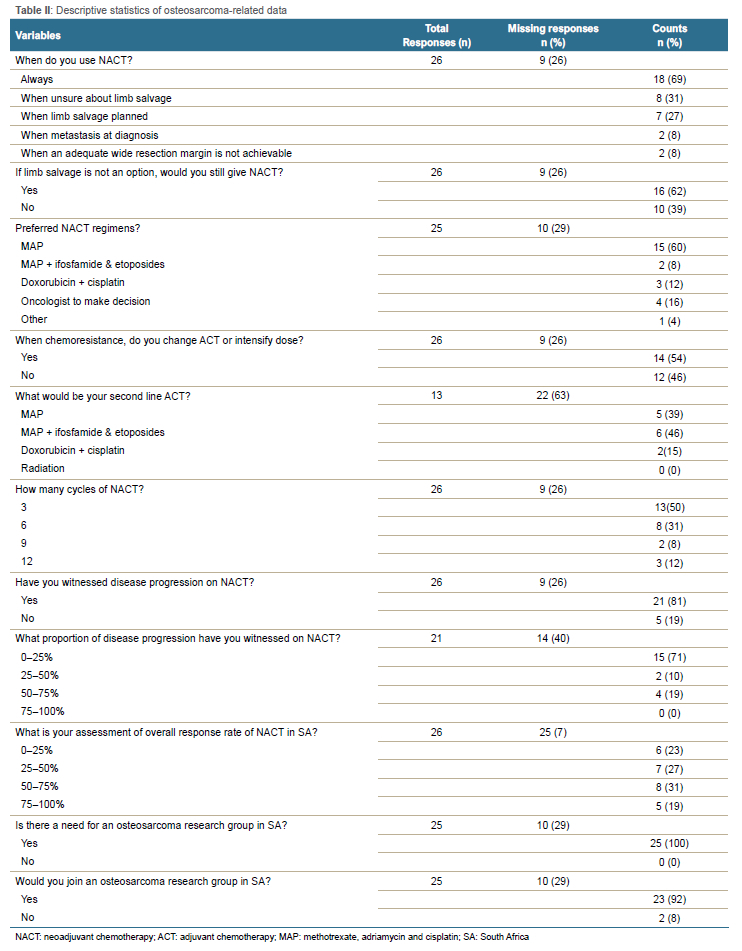
NACT was routinely prescribed to all COS cases by 69% of clinicians (18/26); in contrast, 31% (8/26) would administer it if there was uncertainty about the ability to perform limb salvage, 27% when planned limb salvage, 27% when metastasis was present at diagnosis, and 8% (2/26) when adequate wide margin resection margins were not achievable (Table II). Sixty-one per cent (16/26) of respondents still prescribed NACT if limb salvage was not an option and amputation was planned. The preferred first-line NACT regimen by 60% of respondents comprised methotrexate, adriamycin and cisplatin (i.e. MAP); 8% preferred MAP plus ifosfamide and etoposide; while 16% of respondents left the decision to the oncologist. In the instance of chemoresistance, 54% (14/26) of respondents opted for a change of agents in the ACT regimen or an intensified dose of the ACT regimen. The preferred second-line ACT regimen was either MAP at 39% (5/13), MAP plus ifosfamide and etoposide at 46% (6/13), or doxorubicin plus cisplatin at 12% (3/13). Interestingly, the number of NACT cycles prescribed varied widely, at three (50%; 13/26), six (31%; 8/26), nine (8%; 2/26), or twelve (12%; 3/26) cycles.
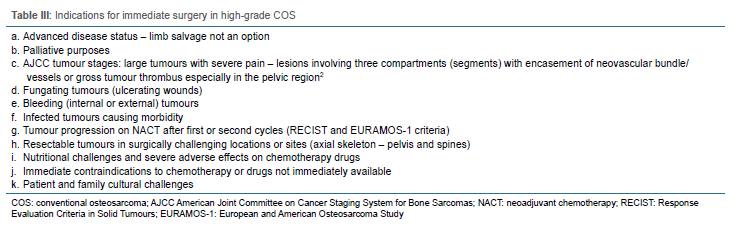
Eighty per cent (21/26) of clinicians had witnessed DP as per RECIST criteria while the patients were on NACT.12 Of those, 15 of 21 (71%) observed 0-25% of DPs. Meanwhile, 2 of 21(10%) observed 25-50% of DPs, and 4 of 21 (19%) estimated the prevalence to be 50-75%. In contrast, the perceived response rate to NACT, defined as a proportion of observed responders (> 90% tumour necrosis) to NACT compared to non-responders (< 90% tumour necrosis) according to Huvos criteria in practice, was reported to be 0-25% (6/26; 23%), 25-50% (7/26; 26.9%), 50-75% (8/26; 31%), and 75-100% (5/26; 19.2%). All clinicians, 100% (25/25), agreed on the need for an osteosarcoma consensus group in South Africa. Furthermore, Table III describes clinicians' opinions on circumstances where NACT may be unnecessary for COS.
Factors associated with prescribing NACT
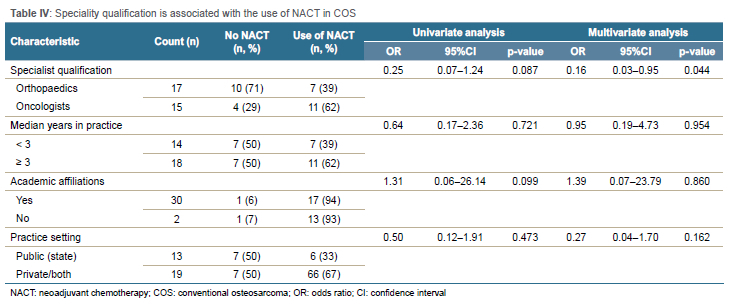
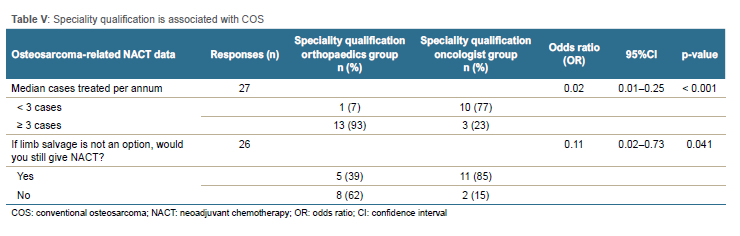
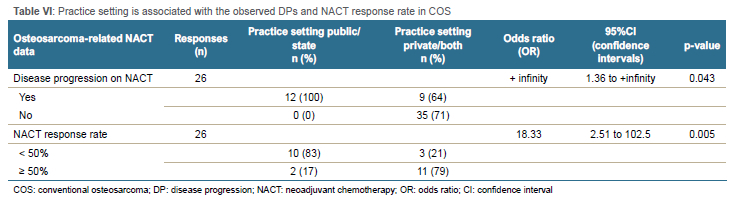
In the univariate analysis, specialist qualification (orthopaedic or oncology), time in practice, academic affiliation, and practice setting were not associated with the routine use of NACT in all cases (Table IV). However, in the multivariate analysis, specialty qualification was significantly associated with the use of NACT (odds ratio [OR] 0.16; 95% confidence interval [CI] 0.03 to 0.95; p = 0.044), with orthopaedic surgeons 84% less likely to use NACT compared to oncologists. Regarding case volume, 93% of orthopaedic surgeons (13 of 14) treated three or more cases per annum compared to 24% of oncologists (3 of 13). Thus, specialist qualification was associated with the number of cases seen per annum (OR 0.02; CI 0.002 to 0.25; p < 0.001) (Table V). In addition, speciality qualification was associated with prescribing NACT when limb salvage was not an option, with orthopaedic surgeons being less likely to recommend NACT if amputation was indicated (OR 0.11; CI 0.02 to 0.73; p = 0.041). Practitioners working in the public sector were more likely to observe DP on NACT (OR +infinity; CI 1.36 to +infinity; p = 0.043) (Table VI). Similarly, the practice setting was associated with observing a poor response to NACT (OR 18.33; CI 2.51 to 102.5; p = 0.005).
Discussion
Our results demonstrated that a substantial number of clinicians in South Africa based their treatment strategies on guidelines from HICs, mainly EURAMOS-1 (46%), ESMO (23%), and MSTS (8%).1-4 However, many did not strictly adhere to any guidelines (15%). These guidelines are derived from extensive clinical trials advocating for treating central high-grade COS with NACT, wide surgical resection, and ACT.1-4 The criteria for upfront or immediate surgery, as opposed to NACT, have not been fully clarified in most LMICs, where studies frequently show advanced COS (Enneking stage III).14
Historically, surgeons in the 1980s, as mentioned by Goorin et al., supported NACT anecdotally.5 Contemporary orthopaedic oncology surgeons, however, have identified specific situations for immediate surgery. These include locally advanced tumours encasing neurovascular structures, extensive metastatic disease, tumours with skin defects causing fungation or bleeding, ongoing internal or intra-tumoral bleeding during NACT, DP despite one or two cycles of NACT, and adverse effects of chemotherapy (Table IV). Recently, the ICONIC prospective study in the UK (2024) randomised patients with COS to either chemotherapy first or surgery first. Although their criteria are not clearly defined, upfront surgery appears to have a role in clinical practice.21
Additionally, contraindications for NACT include axial skeleton osteosarcomas, encompassing craniofacial, spinal, and pelvic tumours. A 2018 study by Xu et al., involving 146 patients with non-metastatic high-grade pelvic osteosarcoma, found no difference in survival outcomes between those treated with and without NACT.6 Histological subtypes, such as the chondroblastic osteosarcoma variant known for its chemoresistance, further question the utility of NACT in these cases, suggesting that primary surgery might be more advantageous.3,22 Sociocultural factors also significantly influence treatment decisions in South Africa. Chemotherapy-induced improvements in peritumoral oedema, highlighted by Shipley et al. in 2012, can make patients reluctant to choose surgical treatments, especially when amputation is recommended.15 In South Africa, amputation is a socially challenging option, often leading to hesitancy in following clinical advice, which results in poorer outcomes.14 Culturally sensitive approaches to treatment planning for COS have been previously elucidated by Brown et al. in 2018 in KwaZulu-Natal province.23
Despite these factors, 69% of clinicians routinely prescribed NACT, even in situations where immediate surgery could be considered, particularly when limb salvage was uncertain, planned, or in cases of metastasis. Orthopaedic surgeons were less inclined to prescribe NACT than oncologists, likely understanding that it may not alter survival outcomes or be necessary in cases requiring amputation. The indications for NACT versus immediate surgery in COS within South African clinical practice warrant further clarification. Large clinical trials have previously investigated factors associated with DP in COS; this comprises older age, axial skeleton, positive surgical margins, poor chemotherapy response, multiple site metastases, and incomplete surgical remission.17-18,24-26
In this study, clinicians reported that they commonly observed DP on NACT in practice, with varying perceived progression rates. The response rates to NACT also varied, with a wide range in the perceived proportion of tumour necrosis. In 2023, Halalsheh et al. reported that 16% of cases in their series (31/95) exhibited DP while the patients were on NACT before local control was achieved.19 Of concern in their series was that DP conferred a poor prognosis.19 Furthermore, the value of NACT in cases where wide surgical resection can be achieved with ease has been questioned.5 If local progression occurs while the patient is on NACT limb salvage, it might become impossible or may result in close margins. The worst-case scenario is that the patient may develop distant metastasis while awaiting surgery.
Tumour response to chemotherapy has emerged as one of the most important prognostic factors for COS of the extremities.1-4 Internationally, approximately 45-55% of tumours exhibit a good response to chemotherapy.7-11 Eighty-three per cent of the clinicians working in public/state practice settings, and 21% of those in private/both practice settings, estimated their NACT response rates to be below 50%. In 2017, Hart and Parkes observed a 21% good tumour response rate, with necrosis > 90%; and 79% had a poor response, with necrosis < 90%, among patients treated with NACT in Cape Town.12 The phenotypical aggressive disease in our geographic region, with a preponderance for DP and multidrug chemoresistance in COS, may be underpinned by novel genetic instability patterns.27 This could also explain the high prevalence of metastatic disease at presentation in our geographic area.12-16
The small sample size is a significant shortcoming, and our findings should be interpreted cautiously. The final sample size required was 88 participants; however, we had 35 respondents (40%). Our study exhibits participation bias, also known as nonresponse bias, which is common in clinical trials and survey studies. A dataset may be skewed because participants disproportionately possess certain traits that affect participation, attrition or outcomes. The resulting sample does not truly represent the population as a whole, and the results cannot be generalised. Additionally, our study may be prone to self-selection bias, with disproportionately fewer responses from medical oncologists than orthopaedic surgeons (group selection bias). Therefore, the analysis of associations with the routine use of NACT may be underpowered. Furthermore, when fewer data points are available in cases of small sample size, ask in our study, each observation has a larger impact on the estimate, resulting in less precision and, therefore, wider confidence intervals. High variability or inconsistency in the data can also contribute to wide confidence intervals, as shown in our Cronbach's alpha scale of 0.6409. However, COS is a rare disease, and there are only a small number of clinicians with experience in managing it in South Africa. We believe the survey still sheds light on the current opinion of clinicians towards NACT, particularly regarding the risk of DP and the need for specific treatment guidelines. The request for participation was sent out via the relevant professional societies and personal networks, but this may have introduced a bias as some experts in the field may have not received the invitation. Furthermore, the data presented here should not be seen as high-level evidence to guide treatment but rather as an expert's opinion (level 5 evidence). When it comes to the management of COS, it is still best that cases are individualised and treated in accordance with the decisions taken by a multidisciplinary team.
Conclusion
In South African clinical practice, we observed disparities in the approach to treating high-grade COS of the extremities among clinicians regarding the use of NACT. NACT was routinely prescribed by 69% of clinicians. Orthopaedic oncology surgeons were less likely to recommend the routine use NACT, when compared to oncologists. This further elucidates the need for more data pertaining to COS in South Africa to enable the development of pragmatic treatment guidelines tailored to our context to improve outcomes through actionable recommendations consensus or modified Delphi methods.
Ethics statement
The authors declare that this submission is in accordance with the principles laid down by the Responsible Research Publication Position Statements as developed at the 2nd World Conference on Research Integrity in Singapore in 2010. Before the commencement of the study, ethical approval was obtained from the following ethical review board: UKZN BREC, reference number BREC/00002737/2021.
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all the participants.
Declaration
The authors declare authorship of this article and that they have followed sound scientific research practice. This research is original and does not transgress plagiarism policies.
Author contributions
PGM: conceptualisation, formal analysis, investigation, methodology, project administration, writing of original draft
LCM: conceptualisation, methodology, writing of original draft
ORCID
Mthethwa PG https://orcid.org/0000-0001-6432-1899
Marais LC https://orcid.org/0000-0002-1120-8419
References
1. Soares do Brito J, Santos R, Sarmento M, Fernandes P, Portela J. Chemotherapy regimens for non-metastatic conventional appendicular osteosarcoma: a literature review based on the outcomes. Curr Oncol. 2023;30(7):6148-65. [ Links ]
2. Strauss S, Frezza AM, Abecassis N, et al. Bone sarcomas: ESMO-EURACAN-GENTURIS-ERN PaedCan Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(12):1520-36. [ Links ]
3. Smeland S, Bielack SS, Whelan J, et al. Survival and prognosis with osteosarcoma: outcomes in more than 2000 patients in the EURAMOS-1 (European and American Osteosarcoma Study) cohort. Eur J Cancer. 2019;109:36-50. [ Links ]
4. van Ewijk R, Herold N, Baecklund F, et al. European standard clinical practice recommendations for children and adolescents with primary and recurrent osteosarcoma. EJC Paediatr Oncol. 2023; 2:100029. [ Links ]
5. Goorin AM, Schwartzentruber DJ, Devidas M, et al. Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for nonmetastatic osteosarcoma: Pediatric Oncology Group Study POG-8651. J Clin Oncol. 2003;21(8):1574-80. [ Links ]
6. Xu J, Xie L, Guo W. Neoadjuvant chemotherapy followed by delayed surgery: is it necessary for all patients with nonmetastatic high-grade pelvic osteosarcoma? Clin Orthop Relat Res. 2018;476(11). [ Links ]
7. Huvos AG, Rosen G, Marcove RC. Primary osteogenic sarcoma: pathologic aspects in 20 patients after treatment with chemotherapy en bloc resection, and prosthetic bone replacement. Arch Pathol Lab Med. 1977;101(1):14-18. [ Links ]
8. Jones KB, Ferguson PC, Lam B, et al. Effects of neoadjuvant chemotherapy on image-directed planning of surgical resection for distal femoral osteosarcoma. JBJS. 2012;94(15):1399-405. [ Links ]
9. Bielack SS, Smeland S, Whelan JS, et al. Methotrexate, doxorubicin, and cisplatin (MAP) plus maintenance pegylated interferon alfa-2b versus MAP alone in patients with resectable high-grade osteosarcoma and good histologic response to preoperative MAP: First results of the EURAMOS-1 Good Response Randomized Controlled Trial. J Clin Oncol. 2015;33(20):2279-87. [ Links ]
10. Marina NM, Smeland S, Bielack SS, et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): an open-label, International, randomised controlled trial. Lancet Oncol. 2016;17(10):1396-408. [ Links ]
11. Meyers PA, Schwartz CL, Krailo MD, et al. Osteosarcoma: the addition of muramyl tripeptide to chemotherapy improves overall survival--a report from the Children's Oncology Group. J Clin Oncol. 2008;26(4):633-38. [ Links ]
12. Hart H, Parkes JD. Long-term outcomes in osteosarcoma patients in the Groote Schuur Hospital patient population: A retrospective review. 2017. 2017;1. [ Links ]
13. Lisenda L, Linda ZA, Snyman FPJ, et al. Osteosarcoma patient outcomes at a South African tertiary hospital. S Afr Med J. 2017;107(9):754-57. [ Links ]
14. Mthethwa PG, Marais LC, Aldous CM. Prognostic factors for overall survival of conventional osteosarcoma of the appendicular skeleton. Bone Jt Open. 2024;5(3):210-17. [ Links ]
15. Shipley J, Beukes C. Outcomes of osteosarcoma in a tertiary hospital. SA Orthop J. 2012;11(1):18-22. [ Links ]
16. Ferreira N, Marais LC. Osteosarcoma presentation stages at a tumour unit in South Africa. S Afr Med J. 2012;102(8):673-76. [ Links ]
17. Guenther LM, Rowe RG, Acharya PT, et al. Response Evaluation Criteria in Solid Tumors (RECIST) following neoadjuvant chemotherapy in osteosarcoma. Pediatr Blood Cancer. 2018;65(4): e26896. [ Links ]
18. Hazewinkel AD, Lancia C, Anninga J, et al. Disease progression in osteosarcoma: a multistate model for the EURAMOS-1 (European and American Osteosarcoma Study) randomised clinical trial. BMJ Open. 2022;12(3): e053083. [ Links ]
19. Halalsheh H, Amer S, Sultan I. Progression before local control in osteosarcoma: Outcome and prognosis-predictive factors. Pediatr Blood Cancer. 2023;70(11): e3064912. [ Links ]
20. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019 July 1;95:103208. [ Links ]
21. Childs A, Gerrand C, Brennan B, et al. A prospective observational cohort study for newly diagnosed osteosarcoma patients in the UK: ICONIC study initial results. Cancers. 2024;16(13):2351. [ Links ]
22. Tsagozis P, Laitinen MK, Stevenson JD, et al. Treatment outcome of patients with chondroblastic osteosarcoma of the limbs and pelvis. Bone Joint J. 2019;101-B(6B):739-44. [ Links ]
23. Brown O, Goliath V, van Rooyen DRM, et al. Cultural factors that influence the treatment of osteosarcoma in Zulu patients: Healthcare professionals' perspectives and strategies. Health SA. 2018;23:1095. [ Links ]
24. Thebault E, Piperno-Neumann S, Tran D, et al. Successive osteosarcoma relapses after the first line O2006/sarcoma-09 trial: what can we learn for further phase-II trials? Cancers. 2021;13(7):1683. [ Links ]
25. Palmerini E, Torricelli E, Cascinu S, et al. Is there a role for chemotherapy after local relapse in high-grade osteosarcoma? Pediatr Blood Cancer. 2019;66(8): e27792. [ Links ]
26. Isakoff MS, Bielack SS, Meltzer P, Gorlick R. Osteosarcoma: current treatment and a collaborative pathway to success. J Clin Oncol. 2015;33(27):3029-35. [ Links ]
27. Mthethwa PG, Arumugam T, Ramsuran V, et al. Unique gene expression profiles within South Africa are associated with varied chemotherapeutic responses in conventional osteosarcoma. Cancers. 2024;16(18):3240. [ Links ]
Received: October 2024
Accepted: March 2025
Published: November 2025
* Corresponding author: mthethwap@ukzn.ac.za
Editor: Prof. Theo le Roux, University of Pretoria, Pretoria, South Africa
Funding: No funding was received for this study.
Conflict of interest: The authors declare they have no conflicts of interest that are directly or indirectly related to the research.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}