










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676XPrint version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.41 n.3 Pretoria Dec. 2025
https://doi.org/10.7196/SAJCC.2025.v41i3.3169
RESEARCH
https://doi.org/10.7196/SAJCC.2025.v41i3.3169
Noise levels in intensive care units at Charlotte Maxeke Johannesburg Academic Hospital
D BrancatoI, II; M MerIII, IV; Z JoomaV, VI
IDA; Department of Anaesthesia, Faculty of Health Sciences, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa
IIDA; Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
IIIPhD; Department of Anaesthesia, Faculty of Health Sciences, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa
IVPhD; Charlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa
VCert Crit Care Anaes; Department of Anaesthesia, Faculty of Health Sciences, School of Clinical Medicine, University of the Witwatersrand, Johannesburg, South Africa
VICert Crit Care Anaes; Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa
ABSTRACT
BACKGROUND. Noise exposure can negatively affect patients and staff. Patients may experience sleep disturbance, delirium and sympathetic stimulation. Communication may be hampered, and staff may experience alarm fatigue. The World Health Organization (WHO) recommends time-averaged sound levels of 35 dB. Prolonged exposure to noise levels >85 dB may damage hearing. Studies on noise levels in adult intensive care units (ICUs) in South Africa are lacking.
OBJECTIVES. To compare noise levels with WHO recommendations, across ICUs and between recording zones.
METHODS. A prospective cross-sectional research design was used. A class 2 sound-level meter measured noise levels in six adult ICUs at the central station and a patient cubicle for three 24-hour periods per ICU.
RESULTS. Time-weighted sound levels (L ) ranged between 48 and 65 dB. There was no statistically significant difference when comparing noise levels conditioned to ICU size, layout and between recording zones. Daytime noise levels at the central station were higher than night-time values (p<0.001) but diurnal variation was not appreciated in patient cubicles. All ICUs exceeded WHO recommendations >80% of the time. Noise levels >85 dB were very infrequent.
CONCLUSION. Noise levels consistently exceeded WHO recommendations, ranging between 48 and 65 dB. ICU size and layout do not appear to influence noise levels. Elevated daytime noise levels at central stations may result from increased daytime staff and duties. Noise-protective equipment is unnecessary as noise levels do not exceed 85 dB for >8 hours, but noise-reduction strategies should be broadly implemented to improve critical care.
Keywords: Critical care, decibels, intensive care, noise levels, sound levels
Noise levels in the hospital setting have long been a subject of interest in research because of the impact on health and well-being.[1] Both patients and staff can suffer negative physiological and psychological consequences as a result of noise exposure.[2] Noise may impair sleep quality, thereby increasing the risk of delirium and contributing to longer hospital stays.[3,4] Exposure to noise has been linked to sympathetic stimulation resulting in hypertension and tachycardia.[5] Noise may enhance the release of cortisol, increase oxygen consumption, increase the need for sedation, and disrupt circadian rhythm.[1,3-5] The effects on staff may include annoyance, alarm fatigue and barriers to communication.[6-9] Noise levels in intensive care units (ICUs) originate from a variety of modifiable and non-modifiable sources, mostly comprising noise generated by care-giving activities, equipment, and human factors.[10] In ICUs, common alarms typically reach sound levels of approximately 70 dB, comparable to noise of a vacuum cleaner.[11]
Nebulisers can produce noise levels of up to 80 dB, similar to heavy traffic, while objects falling to the floor have been recorded at levels as high as 90 dB, akin to the noise of a motorcycle.[11]
The World Health Organization (WHO) recommends stringent time-averaged sound levels of 35 dB in rooms in which patients are being treated, and a maximum of 40 dB for single noise events in hospital rooms.[12] Exposure to noise levels of 85 dB and higher for 8 hours or longer can lead to hearing impairment, hence necessitating the use of noise-protective equipment.[12]
In South Africa (SA) several studies measuring noise levels in operating theatres and neonatal ICUs (NICUs) have been done, but there is a paucity of studies assessing noise levels in adult ICUs.[13-16] This study aims to measure the noise levels in six adult ICUs at Charlotte Maxeke Johannesburg Academic Hospital (CMJAH) and to compare noise levels with international guidelines.
Methods
A prospective cross-sectional research design was used. An ethics waiver was obtained from the Medical Human Research Ethics Committee at the University of the Witwatersrand (ref. no. W-PR-231002-01). Permission was obtained from the relevant departments. All six adult ICUs at CMJAH were included in the study, namely: multidisciplinary ICU (2), cardiothoracic ICU, neurosurgery ICU, trauma ICU and the coronary care unit.
CMJAH is a tertiary academic hospital in Johannesburg and one of the major public sector hospitals in the province. SA has a dual healthcare system comprising public and private sectors.[17] The majority of the population utilises the public sector characterised by resource-limitations, budget constraints and high patient load.[17]
Using James and Tatton-Brown's typology, the layout of ICU was classified as open or double-corridor design, alongside additional layout types used in healthcare architecture.[18] At CMJAH three ICUs are open and three are double corridor. An open layout is an open space with the central station (CS) surrounded by multiple patient beds separated by curtains.[18] At CMJAH the open ICUs housed eight to twelve beds separated by curtains. In the double-corridor layout the CS is separated from enclosed patient rooms by a corridor on either side.[18] At CMJAH the enclosed rooms typically contained multiple beds (one to four) separated by curtains.
Data were collected on weekdays from a patient cubicle (PC) and the CS at each of the six ICUs. Data were excluded if it was found that the sound-level meter was moved during the recording period, if a patient's cubicle was vacant for more than 6 hours or if a technical fault was experienced, such as loss of power supply to the meter.
Sound is measured in decibels (dB), which is a logarithmic measure of the effective pressure exerted by a sound wave.[19] When sound is measured, three frequency weightings can be applied based on the setting.[19] These frequency weightings are A, C or Z.[19] The human ear is most sensitive to frequencies between 2 kHz and 5 kHz.[19] The A-weighting is most appropriate in the context of human hearing because it reduces the influence of very low and high frequencies by boosting the mid-range frequency.[19]
The International Electrotechnical Commission (IEC) standards describe classes of sound-level meters as class 1 and class 2.[20] Class 1 sound-level meters measure sound levels more accurately across a broader range of frequencies of 20 Hz to 20 kHz with a tolerance of ±1.5 dB.[21] Class 1 sound-level meters are more expensive and are preferred for precise measurements in fields such as architectural acoustics.[21] Class 2 meters are appropriate for use in general workplace noise surveys as their frequency range is 20 Hz to 8 kHz with a tolerance of ±2.3 dB.[21] Owing to financial constraints, and in keeping with similar studies, a class 2 sound-level meter (SLM-25) was used for the study.[13,22] The sound-level meter captured noise levels from 30 to 130 dB. Particular analysis was done of noise levels exceeding 35 dB, 40 dB and 85 dB to allow for comparison with international standards.
Sound measurement terminology incorporates a variety of metrics to quantify different characteristics of sound.[23] Leq is the equivalent continuous sound level over a period of time.[23] It represents the sound level that contains the same amount of sound energy as the varying levels of noise during that time.[23] Leq is more greatly affected by outliers, especially higher sound levels, because it accounts for the total sound energy.[24] Leq aids with assessment of overall risk of exposure as duration of exposure is considered.[24] Other common terms used to describe noise levels are Lmax and Lmin which respectively refer to the highest and lowest noise levels recorded.[24] Useful terms for statistical analysis of noise levels include L50, L90 and L10.[24] These metrics indicate the noise levels surpassed for 50%, 90%, and 10% of the observation duration, respectively.[24] The L50, also considered the median noise level, is more robust against outliers and is useful to compare background noise levels.[24] The L50 was used for statistical comparison in this study.
Data collection
Data were collected from 23 January 2024 until 22 March 2024. One sound-level meter was used to record noise levels for the duration of the study. Noise-level recordings were collected on weekdays. Noise levels were measured for 24-hour periods from 07h00 until 06h59 the following day. The sound-level meter was placed by the primary researcher at the CS for three 24-hour periods and then placed in a PC for three 24-hour periods in each of the six ICUs. The PC closest to the entrance was selected in each ICU and the meter was placed at an occupied bed in the cubicle being analysed. Thirty-six samples (24-hour recordings) were required for analysis, consisting of six samples in total from each of the six ICUs.
The sound-level meter recorded sound levels every 3 seconds using A-weighting frequency filter and fast response mode. Staff and patients were requested not to move the device for the duration of the recording period. Additional data were collected concerning the ICU layout, the number of nursing staff present, the occupancy of the entire unit and the occupancy of the cubicle in which the meter was placed. The ICUs were de-identified and labelled ICU A - F. Data were exported to Microsoft Excel (Microsoft, USA) spreadsheets for analysis. The recordings were analysed as a continuous 24-hour period, as well as 12-hour periods with daytime being from 07h00 until 18h59 and night-time from 19h00 until 06h59 the following day. WHO guidelines were used for comparison.
All analyses were conducted using R v4.4.0. Linear quantile regression analysis was used to examine relationships between noise levels for each ICU conditioned on the number of people in each ICU, noise levels during the day and night for each recording zone (CS v. PC) and recording zones using 24-hour record data. A Mann-Whitney U test was used to compare noise levels conditioned on ICU layout (double-corridor or open). In order to assess whether noise levels exceeded recommended levels, the percentage of time spent above the respective thresholds was calculated (35 dB, 40 dB and 85 dB). Statistical comparisons of the time spent above the respective thresholds between the CS and PC recording zones were performed using Mann-Whitney U tests. A p-value of <0.05 was considered significant.
Results
Thirty-six samples were included in the final analysis, as indicated in Fig. 1.
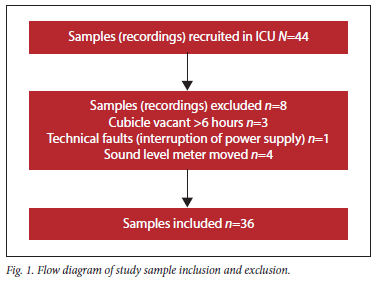
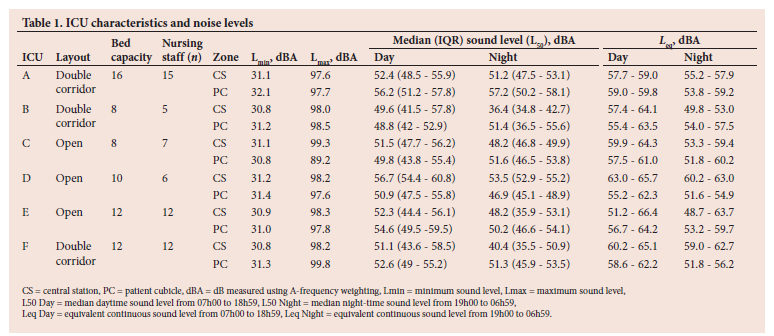
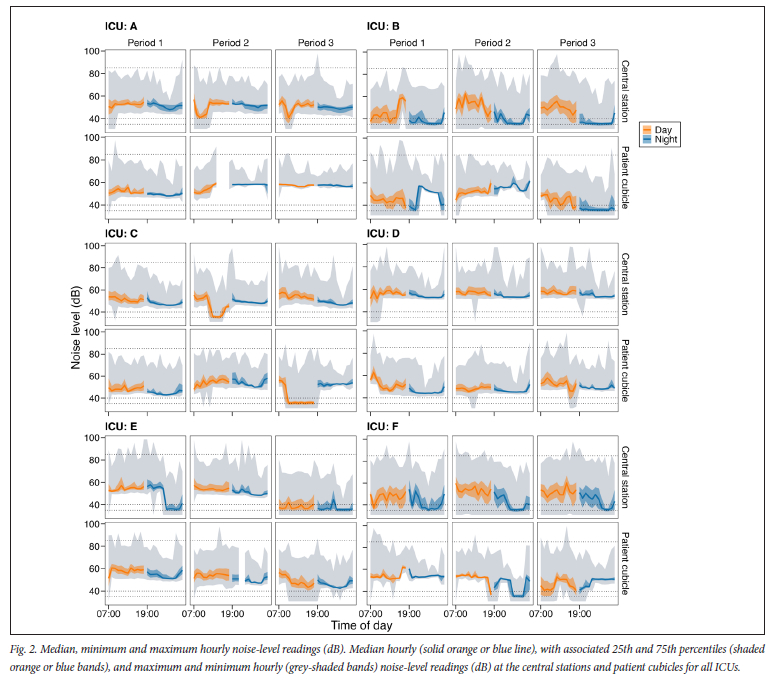
Table 1 outlines the characteristics of the ICUs and their measured noise levels. Both time-weighted averages (L ) and median sound levels (L50) exceed the WHO recommendation of 35 dB in each ICU during daytime and night-time readings. Fig. 2 illustrates the median hourly noise-level readings (dB) (solid orange or blue line), with associated 25th and 75th percentiles (shaded orange or blue bands), and maximum and minimum hourly (grey-shaded bands) noise-level readings (dB) at the CS and PC for ICUs A - F. Each period (1 - 3) represents a 24-hour recording period from 07h00 to 06h59 the following day. The dotted horizontal lines on each plot indicate the key health and safety thresholds of 35 dB, 40 dB and 85 dB.
Noise levels across the ICUs were compared using occupancy as an indicator of ICU size. The occupancy was calculated by averaging the number of people (patients and nursing staff) in each of the recording zones across the three 24-hour recording periods. There was no statistically significant relationship between the ICU noise level and their size (median (interquartile range (IQR)) 0.2 dB (-0.3 - 0.6), p=0.516). The noise levels across the ICUs were compared using the layout of the ICU (double-corridor v. open layout (n=3 for each layout)). There was no statistically significant difference between the two layouts (-0.5 dB (-7.1 - 3.3), p=0.31).
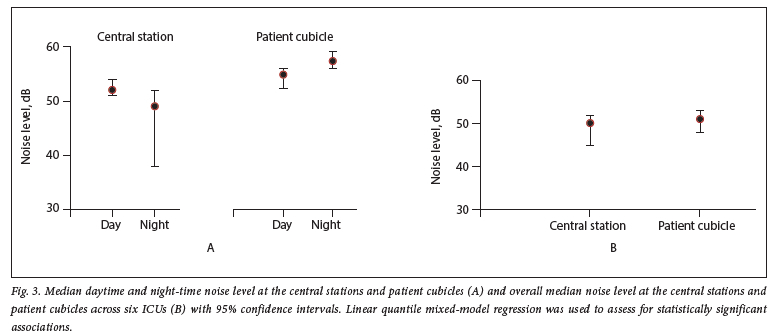
A statistically significant difference was found when comparing daytime and night-time median (IQR) noise levels at the CS with daytime levels being significantly higher (daytime = 52.8 dB (51.1 - 55.0); night-time = 48.9 dB (37.5 - 52.1); p<0.001). No significant difference was found between the daytime and night-time median (IQR) noise levels in PCs (daytime = 52.2 dB (49.3 to 54.0); night-time = 50.2 dB (48.6 to 52.8); p=0.266) (Fig. 3A). No statistically significant difference was found when comparing overall median noise levels of all PCs to overall median noise levels of all CSs across the 6 ICUs (Fig. 3B).
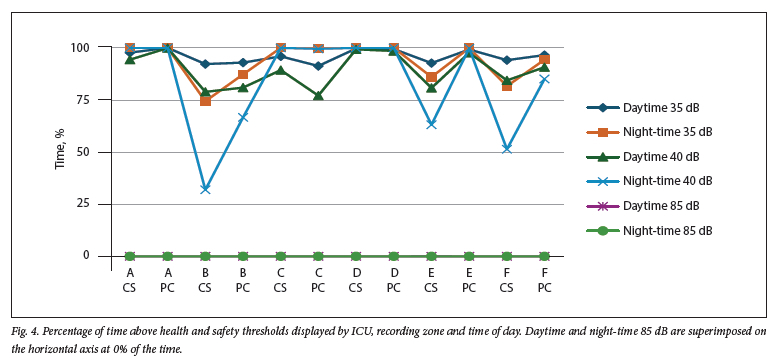
Fig. 4 depicts the average time spent above certain health and safety noise thresholds. These threshold values are 35 dB, 40 dB and 85 dB. WHO recommends time-weighted average sound levels of 35 dB. Other than the CS of ICU B, noise levels exceeded 35 dB >80% of the time. When converted to hours, the median (IQR) time above 35 dB in CSs was 22.5 hours (21.2 - 23.7), and in PCs it was 23.4 hours (22.9 - 23.9), per 24-hour period. Overall, there was no statistically significant difference between the recording zones across the ICUs when comparing the percentage of time spent above 35 dB (-1.9; -12.1 - 3.5, p=0.31).
Single noise events should not exceed 40 dB as per WHO guidelines. Four ICUs had noise levels >40 dB for >75% of the time. When converted to hours, the median (IQR) time >40 dB in CSs was 20.8 hours (18.0 - 23.9), and in PCs it was 22.5 hours (20.2 - 24.0), per 24-hour period. Overall, there was no statistically significant difference between the recording zones across the ICUs when comparing the percentage of time spent above 40 dB (-4.9; -32.1 - 9.2, p=0.31).
An important threshold to consider is 85 dB because of the potential to cause hearing damage if exposure exceeds 8 hours. Excursions in noise levels >85 dB were very infrequent. When converted to seconds, the median (IQR) time >85 dB in CSs was 16.8 (7.5 - 20.4) seconds, and in PCs it was 9.6 (3.6 - 14.4) minutes, per 24-hour period. Overall there was no statistically significant difference between the recording zones across the ICUs when comparing the percentage of time spent >85 dB (0.01; -0.007 - 0.027, p=0.18).
Discussion
In this study, we found that noise levels in the six ICUs at CMJAH consistently exceeded the WHO recommended time-weighted average of 35 dB. The time-weighted average noise levels ranged from 48 to 65 dB. There was no statistically significant relationship between the noise levels and the ICU size or the ICU layout. At the CS, daytime noise levels were significantly higher than night-time values, but the PC did not reveal the same diurnal variation. No statistically significant difference was found in the overall median noise levels between the recording zones, suggesting that neither the CS nor the PC zone was notably louder or quieter. Analysis of health and safety noise thresholds revealed the majority of ICUs exceeded 35 dB >80% of the time, exceeded 40 dB >75% of the time and excursions >85 dB were very infrequent.
Busch-Vishniac et al.[9] reviewed literature on noise levels in hospitals and state that none of the published results are compliant with WHO recommendations for noise levels in hospitals with average levels exceeding WHO guidelines by approximately 20 - 40 dB. This suggests that the guidelines may be excessively stringent and unattainable in the ICU environment.[91 The review identifies a clear trend of increasing hospital noise since 1960 and notably little variation across a wide variety of hospitals and units.[9]
SA has a dual healthcare system comprising public and private sectors. [171 The vast majority of the population utilises the public sector, characterised by resource-limitations, budget constraints and high patient load.[17] This study was conducted in ICUs at a tertiary referral centre in the public sector. Average noise levels in low-middle-income countries (LMICs), notably Columbia, Brazil and India range between 58 and 80 dB.[25-27] Average noise levels in high-income countries (HICs), notably Germany, England and the USA, range between 55 and 62 dB.[28-30] The average Leq sound levels measured in this study range from 48 to 65 dB, in keeping with HICs, but still up to 30 dB higher than the WHO recommendations.[12]
Studies investigating noise levels in adult ICUs in SA are lacking. A study conducted in an NICU revealed noise levels ranging from 62.3 to 66.7 dB.[15] The higher noise levels may result from the unique equipment and environmental dynamics found in NICUs. Such equipment may include incubators, apnoea monitors and oscillators. Unique environmental factors may include infant crying and prolonged visitation periods for parents. It is common for studies in paediatric ICUs to quote the American Academy of Pediatrics (AAP) guideline that Leq sound levels should not exceed 45 dB, which is 10 dB higher than the WHO recommendations in adult ICUs.[31]
Comparing studies can be challenging because of the lack of consistency in both measuring and reporting strategies. Several studies state 'average' noise levels but fail to clarify if the average refers to the Leq, L50 or arithmetic mean. The arithmetic mean is inappropriate for noise levels because the dB scale is logarithmic.[23] We chose to report both Leq and L50. Leq levels are appropriate to assess compliance with WHO recommendations and enable assessment of overall risk because the duration of exposure is taken into account.[24] Reporting Leq levels enables comparison with international studies.[9,22] Median sound levels, L50, were used for statistical comparisons and are found frequently in the literature.[22]
This study measured noise levels in various ICUs which differ in terms of size, occupancy, typical patient pathology and typical equipment, yet no statistically significant differences were discovered among the ICUs. The relative consistency of noise levels suggests that the problem of elevated noise levels is universal and noise-reducing strategies should be applied broadly.
The impact of the noise levels on critically ill patients was not explored as it is beyond the scope of our study. Research has demonstrated that assessing the impact of noise levels on critically ill patients is challenging because of multiple confounding factors.[35] A systematic review estimated that approximately 30% of sleep arousals can be attributed to nvironmental noise, indicating that many other factors influence the quality of sleep of critically ill patients.[35] Bundled interventions incorporating noise-reduction strategies are associated with reductions in the incidence of delirium, supporting the need to address noise levels to optimise patient care.[36]
The authors identified a paucity of studies in adult ICUs looking at the effectiveness of interventions to reduce noise in ICUs. This should be the focus of future research in the field, with particular attention to cost-effective strategies that can be easily implemented in resource-constrained environments. Acoustics and sound levels should also be taken into consideration when hospitals are built or renovated to incorporate insulation and soundproofing in the structure.[10]
Interpretation
Revolutionary changes in healthcare have enabled a variety of life-sustaining therapies and procedures to be done in ICU. These procedures involve a myriad of noise-generating equipment, alarms and healthcare workers, which are all likely to contribute to such rising noise levels. The elevated daytime noise levels at CS may result from an unaccounted increase in medical staff, medical ward rounds, visitors and generally increased activity around the CS during the day. ICU size and layout do not appear to influence noise levels and recording zones showed insignificant variation. This emphasises the need for generalised noise reduction strategies in the ICU.
Limitations
Noise levels were only recorded on weekdays so variations between weekdays and weekends were not explored. Generalisability is limited by the small sample size, short recording period and heterogeneity of ICUs. Noise levels were measured in one PC, which may not be representative of noise levels throughout the unit. The impact of noise levels on patients and staff was not explored. We did not investigate patient acuity, clinical diagnoses, and care intensity; these factors may help explain apparent differences in noise levels.
Strengths
Noise levels were recorded for three 24-hour periods in each recording zone to attain robust data less affected by random events. The data were collected by one researcher using one sound-level meter to limit bias.
Recommendations
It is recommended that ICUs implement cost-effective noise-reducing strategies such as staff education, signage and quiet-time protocols. Future studies should explore the effects of noise levels on patients and staff and should assess the effectiveness of noise-reduction strategies.
Conclusion
The findings of this study demonstrate that regardless of variations in ICU type, size and occupancy, noise levels consistently exceeded WHO recommendations by up to 30 dB. Despite differences in layout and function, median noise levels showed minimal variation across different ICU units, suggesting that elevated noise levels are a universal problem in our cohort. These findings highlight the need for broad application of noise-reducing strategies.
Data availability. The data used for this study are available from the authors on request.
Declaration. Registration: The National Health Research Database (NHRD): GP_202310_017
Acknowledgements. Peter Kamerman is acknowledged for his invaluable assistance with biostatistical analysis.
Author contributions. DB contributed substantially to the study design, data collection, data analysis and interpretation, and the writing of the final manuscript. MM and ZJ contributed substantially to the study design, data analysis and interpretation, and revision of the final manuscript.
Funding. None.
Conflicts of interest. None.
References
1. Pal J, Taywade M, Pal R, Sethi D. Noise pollution in intensive care unit: A hidden enemy affecting the physical and mental health of patients and caregivers. Noise Health 2022;24(114):130-136. https://doi.org/10.4103/nah.nah_79_21 [ Links ]
2. Stansfeld SA, Matheson MP. Noise pollution: Non-auditory effects on health. Br Med Bull 2003;68(1):243-257. https://doi.org/10.1093/bmb/ldg033 [ Links ]
3. Patel J, Baldwin J, Bunting P, Laha S. The effect of a multicomponent multidisciplinary bundle of interventions on sleep and delirium in medical and surgical intensive care patients. Anaesthesia 2014;69(6):540-549. https://doi.org/10.1111/anae.12638 [ Links ]
4. Weinhouse GL, Schwab RJ, Watson PL, et al. Bench-to-bedside review: Delirium in ICU patients - importance of sleep deprivation. Crit Care 2009;13(6):234. https://doi.org/10.1186/cc8131 [ Links ]
5. Lusk SL, Gillespie B, Hagerty BM, Ziemba RA. Acute effects of noise on blood pressure and heart rate. Arch Environ Health 2004;59(8):392-399. https://doi.org/10.3200/AEOH.59.8.392-399 [ Links ]
6. Ryherd EE, Waye KP, Ljungkvist L. Characterizing noise and perceived work environment in a neurological intensive care unit. J Acoust Soc Am 2008;123(2):747-756. https://doi.org/10.1121/1.2822661. [ Links ]
7. Morrison WE, Haas EC, Shaffner DH, Garrett ES, Fackler JC. Noise, stress, and annoyance in a pediatric intensive care unit. Crit Care Med 2003;31(1):113-119. https://doi.org/10.1097/00003246-200301000-00018 [ Links ]
8. Lewandowska K, Weisbrot M, Cieloszyk A, Mçdrzycka-Dsbrowska W, Krupa S, Ozga D. Impact of alarm fatigue on the work of nurses in an intensive care environment: A systematic review. Int J Environ Res Public Health 2020;17(22):8409. https://doi.org/10.3390/ijerph17228409 [ Links ]
9. Busch-Vishniac I, West J, Barnhill C, Hunter T, Orellana D, Chivukula R. Noise levels in Johns Hopkins Hospital. J Acoust Soc 2006;118:3629-3645. https://doi.org/10.1121/L2118327 [ Links ]
10. Konkani A, Oakley B. Noise in hospital intensive care units - a critical review of a critical topic. J Crit Care 2012;27(5):522-529. https://doi.org/10.1016/j.jcrc.2011.09.003 [ Links ]
11. Stafford A, Haverland A, Bridges E. Noise in the ICU. Am J Nurs 2014;114(5):57-63. https://doi.org/10.1097/01.NAJ.0000446780.99522.90 [ Links ]
12. World Health Organization. Guidelines for community noise. Geneva: WHO, 1999. https://apps.who.int/iris/handle/10665/66217 (accessed 15 February 2024). [ Links ]
13. Carbonari A. Noise levels in the operating theatres at a central hospital. MMed. University of the Witwatersrand, 2021. https://wiredspace.wits.ac.za/server/api/core/bitstreams/bab38a25-df15-4d64-9817-fbc290a92524/content (accessed 12 February 2024). [ Links ]
14. Ismail S, Panday S. An analytical investigation into noise levels in public health sector neonatal intensive care units in the eThekwini District. S Afr J Child Health 2023;17(4):190-194. https://doi.org/10.7196/SAfrJChildHealth.2023.v17i3.1994 [ Links ]
15. Nathan L, Tuomi S, Muller A, Kirsten G. Noise levels in a neonatal intensive care unit in the Cape Metropole. S Afr J Child Health 2008;2(2):50-54. https://www.ajol.info/index.php/sajchh/article/view/41841 [ Links ]
16. Neille J, George K, Khoza-Shangase K. A study investigating sound sources and noise levels in neonatal intensive care units. S Afr J Child Health 2014;8(1):6-10. https://doi.org/10.7196/sajch.676 [ Links ]
17. De Villiers K. Bridging the health inequality gap: An examination of South Africa's social innovation in health landscape. Infect Dis Poverty 2021;10(1):19. https://doi.org/10.1186/s40249-021-00804-9 [ Links ]
18. Rashid M. A decade of adult intensive care unit design: A study of the physical design features of the best-practice examples. Crit Care Nurs Q 2006;29:282-311. https://doi.org/10.1097/00002727-200610000-00003 [ Links ]
19. Moore B. An Introduction to the Psychology of Hearing. 6th ed. Leiden, Boston: Brill, 2013:225 [ Links ]
20. International Electrotechnical Commission. IEC 61672-1:2013: Electroacoustics - Sound level meters - Part 1: Specifications, 2013. 43. https://cdn.standards.iteh.ai/samples/17900/df52d949fc904f329404e965b6268258ZIEC-61672-1-2013.pdf (accessed 1 September 2025). [ Links ]
21. Murphy E, King E. Environmental Noise Pollution: Noise Mapping, Public Health, and Policy. 2nd ed. Amsterdam: Elsevier, 2014. [ Links ]
22. De Lima Andrade E, da Cunha e Silva DC, de Lima EA, de Oliveira RA, Zannin PHT, Martins ACG. Environmental noise in hospitals: A systematic review. Environ Sci Pollut Res Int 2021;28(16):19629-19642. https://doi.org/10.1007/s11356-021-13211-2 [ Links ]
23. Kinsler LE, Frey AR, Coppens AB, Sanders JV. Fundamentals of Acoustics. Hoboken, NJ: Wiley, 2000:242. [ Links ]
24. Beranek L, Mellow T. Acoustics: Sound Fields, Transducers and Vibration. 2nd ed. Academic Press 2019. https://doi.org/10.1016/c2017-0-01630-0 [ Links ]
25. Galindo APG, Caicedo YC, Vélez-Pereira AM. Noise level in intensive care units of a public university hospital in Santa Marta (Colombia). Med Intensiva (English Edition) 2016;40(7):403-410. https://doi.org/10.1016/j.medine.2015.11.004 [ Links ]
26. Vieira EM, da Silva LB, de Souza EL. The influence of the workplace indoor environmental quality on the incidence of psychological and physical symptoms in intensive care units. Build Environ 2016;109:12-24. https://doi.org/10.1016/j.buildenv.2016.09.007 [ Links ]
27. Das A, Kishore J. Noise levels and annoyance among staff in a tertiary care hospital in North India: A cross-sectional study. Arch Environ Occup Health 2023;78(9-10):471-482. https://doi.org/10.1080/19338244.2023.2286388 [ Links ]
28. Luetz A, Weiss B, Penzel T, et al. Feasibility of noise reduction by a modification in ICU environment. Physiol Meas 2016;37(7):1041-1055. https://doi.org/10.1088/0967-3334/37/7/1041 [ Links ]
29. Darbyshire J, Young D. An investigation of sound levels on intensive care units with reference to the WHO guidelines. Crit Care 2013;17:187-195. https://doi.org/10.1186/cc12870 [ Links ]
30. Xie H, Kang J, Mills GH. Clinical review: The impact of noise on patients' sleep and the effectiveness of noise reduction strategies in intensive care units. Crit Care 2009;13(2):1-8. https://doi:10.1186/cc7154 [ Links ]
31. Committee on Environmental Health. Noise: A Hazard for the Fetus and Newborn. Pediatrics 1997;100(4):724-727. https://doi.org/10.1542/peds.100.4.724 [ Links ]
32. Van Rompaey B, Elseviers MM, van Drom W, Fromont V, Jorens PG. The effect of earplugs during the night on the onset of delirium and sleep perception: A randomised controlled trial in intensive care patients. Crit Care 2012;16(3):73-82. https://doi.org/10.1186/cc11330 [ Links ]
33. Ramesh A, Suman Rao PN, Sandeep G, et al. Efficacy of a low cost protocol in reducing noise levels in the neonatal intensive care unit. Indian J Pediatr 2009;76(5):475-478. https://doi.org/10.1007/s12098-009-0066-5 [ Links ]
34. Da Souza RC, Calache ALSC, Oliveira EG, do Nascimento JC, da Silva ND, de Poveda V. Noise reduction in the ICU: A best practice implementation project. JBI Evid Implement 2022;20(4):385-393. https://doi.org/10.1097/xeb.0000000000000311 [ Links ]
35. Horsten S, Reinke L, Absalom AR, Tulleken JE. Systematic review of the effects of intensive-care-unit noise on sleep of healthy subjects and the critically ill. Br J Anaesth 2018;120(3):443-452. https://www.sciencedirect.com/science/article/pii/S0007091217539811 [ Links ]
36. Van de Pol I, van Iterson M, Maaskant J. Effect of nocturnal sound reduction on the incidence of delirium in intensive care unit patients: An interrupted time series analysis. Intensive Crit Care Nurs 2017;41:18-25. https://www.sciencedirect.com/science/article/pii/S0964339717300319 [ Links ]
 Correspondence:
Correspondence:
D Brancato
daniela.brancato@gmail.com
Received 22 February 2025
Accepted 5 August 2025
Contribution of the study
This is the first study in South Africa to measure sound levels in adult intensive care units and provides baseline data which can be used to implement interventions aimed at reducing noise levels to improve care of critically ill adult patients.

{kind=link}
{kind=link}
{kind=link}
{kind=link}