










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouthern African Journal of Critical Care (Online)
On-line version ISSN 2078-676XPrint version ISSN 1562-8264
South. Afr. j. crit. care (Online) vol.41 n.3 Pretoria Dec. 2025
https://doi.org/10.7196/SAJCC.2025.v41i3.3282
RESEARCH
https://doi.org/10.7196/SAJCC.2025.v41i3.3282
A retrospective review of advanced life support interfacility transfers of the public sector emergency medical service in the Western Cape Province, South Africa
L C van RensburgI; N MajietII; C Vincent-LambertIII; W StassenIV
IPhD Emerg Med; Emergency Medicine Division, University of Cape Town, Groote Schuur Hospital, Cape Town, South Africa
IIBEMC; Western Cape Government Health & Wellness, Cape Town, South Africa
IIIPhD; Department of Emergency Medical Care, Faculty of Health Science, University of Johannesburg, South Africa
IVPhD Emerg Med; Emergency Medicine Division, University of Cape Town, Groote Schuur Hospital, Cape Town, South Africa
ABSTRACT
BACKGROUND. The need for critical care transfers (CCTs) has increased in recent years owing to the growing prevalence of high-acuity patients who require access to specialised care and/or resources that are not readily available at the facility where they find themselves. During their transfer from one facility to another, critically ill and injured patients commonly require ongoing care, monitoring and interventions that can only be provided by transfer teams with advanced training and appropriate equipment. In South Africa (SA), these transfers are undertaken mainly by advanced life support (ALS) providers with variable amounts of training. Understanding the demographics and needs of CCT patients in specific contexts is essential to inform training and policy.
OBJECTIVES. To broadly describe the population of adult patients undergoing CCTs facilitated by the public sector emergency medical service (EMS) in the Western Cape Province, South Africa. Patient demographics (age and gender), time intervals (response time, scene time, transfer time), primary diagnosis (respiratory, cardiovascular, gastrointestinal tract, and others), attachments, and clinical or pharmacological interventions.
METHODS. A retrospective descriptive analysis was conducted on electronic patient care records (ePCRs) logged in the EMS's Computer-Aided Dispatch (CAD) database from January 2018 to December 2021. As no universal criteria currently exist for distinguishing a CCT from another transfer, our focus was on cases that required ALS care during the transfer.
RESULTS. During the study period, 25 635 adult patients underwent ALS transfers, with a nearly equal gender distribution. The median patient age was 40 (range 18 - 101) years. Sixty percent of patients were triaged as orange upon arrival (for urgent management) and the remainder red (for emergency or immediate management). Average response, preparation, and transport times spent (minutes:seconds) were 7:10, 16:58, and 12:56, respectively. Respiratory disease (17.9%), cardiovascular disease (12.2%), and central nervous system disorders (12.0%) were the most prevalent clinical conditions. Non-invasive blood pressure monitors (98%) and pulse oximeters (96%) were commonly used devices. Medications were administered to 22% of patients, primarily via intravenous injection (7.5%) and continuous infusion (6.7%). Morphine (4.3%), midazolam (6.4%), and adrenaline (2.0%) were frequently utilised medications. These findings highlight the demographic profile, clinical conditions, and critical care aspects involved in ALS patient transfers, emphasising the complexity and urgency of prehospital medical transport.
CONCLUSION. This study analyses adult patients undergoing ALS transfers by a public sector EMS in the Western Cape, SA (2018 - 2021), providing insights into the transferred patient population. It highlights the importance of continuous patient monitoring, especially electrocardiograms (ECGs), and reveals inconsistencies in medication practices, indicating the need for improved training. The findings stress the necessity for standardised protocols and structured training programmes to inform educational initiatives, equipment procurement, and the critical care retrieval services (CCRS) curriculum development. Additionally, this research can help establish clinical standards for dispatching specific ALS cadres based on patient needs.
Keywords: Patient transfer, emergency medical services, patient population, South Africa
Transferring patients between healthcare facilities in South Africa (SA) is inevitable and more prominent owing to a paucity of healthcare services and specialities offered at various levels across the healthcare system.[1] Like many other low- to middle-income countries (LMICs), SA has significant healthcare service inequalities where there are limited specialised health facilities, and those that exist are often in urban areas. [2,3] In such a context the transferring of patients between healthcare facilities becomes inevitable, driven by the paucity of healthcare facilities that can offer high levels of specialist care and related services in all areas of the country.[1]
Furthermore, the frequency of transferring patients between facilities appears to be increasing in SA partly because of a tiered approach to healthcare provision based on referral, with the level of care being dependent on the capabilities of the initial receiving facility.[4] A growing and ageing population also results in an increased need for patients requiring 'upgraded care' as technology advances. This results in an increased demand for intensive care units and high-care beds.[5-8] A recent study examining the strategy of LMICs in implementing and delivering critical care predicts that, in the next decade, there will be a significant increase in demand for critical care services. This has been attributed to various factors, including a growing elderly population with complex medical needs, limited access to primary healthcare, the impact of climate change, natural disasters, and conflicts.[9]
In this context critical care retrieval and transfer (CCRT) services become essential to the functioning of the healthcare system. Dedicated critical care retrieval services (CCRS) with specialised medical staff and state-of-the-art equipment have become a feature of many international emergency medical service (EMS) systems and healthcare structures. [10,11]In the case of high acuity of patients, the need for ambulance crews with specialised training and access to appropriate equipment have become well recognised as critical in ensuring that patients being transferred between healthcare facilities continue to receive the best possible care.[12,13]
The value and benefits of dedicated CCRS is supported by evidence of decreased adverse events occuring during transfers when specialist teams are used.[14,15] That said, CCRS remains a nascent field within the SA EMS context, and limited training opportunities are available for prehospital providers who are expected to undertake these transfers, resulting in their feeling poorly prepared and lacking confidence.[16] Limited local regulation and standardisation for CCRS practices exist. And, prior to our study, there were few data describing the patient population and their care needs during transport. Such data are crucial for tailored training and decision making around what equipment needs to be provided to safely conduct a CCRT.[11,17]
Part of the challenge remains the fact that there is no locally accepted standard definition as to exactly what a CCT is and how a CCT differs from a conventional ambulance call or transfer. However, for the purposes of our study and this manuscript, we adopted Venter et al'.s [14] definition of CCR as being 'the stabilisation and transport of a critically ill or injured patient from a location where the patient's healthcare requirements outweigh the diagnostic or treatment abilities, and/or expertise available, to an appropriate facility where these are available'
Developing a deeper understanding of the demographics and needs of the patients that are being transferred to and between facilities in different contexts and regions of the country becomes important. This prompted us to investigate and broadly describe the population of adult patients undergoing transfers accompanied by advanced life support (ALS) in the public sector EMS of the Western Cape Province.
Methods
Study design
We conducted a retrospective descriptive analysis of electronic patient care records (ePCRs) from the Western Cape Government Emergency Medical Services (WCG-EMS). All ePCRs of adult patients who were accompanied by ALS providers during transfer were sampled. Ethical approval was obtained from the Human Research Ethics Committee of the University of Cape Town (ref. no. HREC 407/2022), following which organisational approval from the Western Cape Department of Health & Wellness was obtained. This study is reported in accordance with the Reporting of studies Conducted using Observational Routinely collected health Data (RECORD) extension of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist.[18]
Setting and population
The study was conducted within the Western Cape Province, SA. The province is located in the southwest of SA, and is a diverse province known for its cultural richness and scenic beauty. With 11.9% of the national population, more than 7.2 million people live in the province on 129 462 square kilometres of land. As in the greater SA context, the healthcare system in the province is divided between the public and private sectors, each contributing differently to the overall health landscape. The public sector shoulders a substantial burden, providing healthcare services to the majority of the population, including those with limited financial means.
The service has a fleet of over 250 ambulances and provides primary emergency care, helicopter emergency medical services, interfacility transport, and rescue services.[19]
Sample and sampling
Our data set consisted of ePCRs that were logged in the EMS's Computer-Aided Dispatch (CAD) database from January 2018 to December 2021. Our focus then became to identify cases that were accompanied by ALS providers during the transfer.
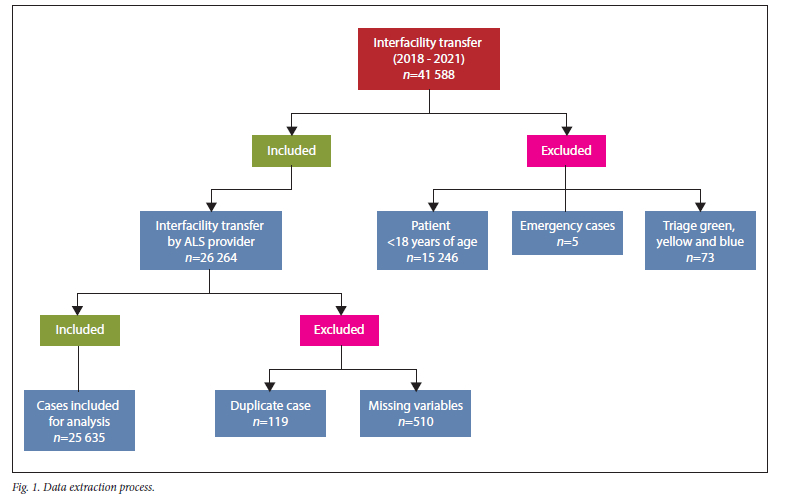
Cases meeting the inclusion criteria for this study include those transferred between January 2018 and December 2021 within the WCG-EMS. Specifically, trauma and medical interfacility transfers (IFTs) are considered, with cases involving an ALS unit comprising registered paramedics and emergency care practitioners (ECPs) attached to service them. Additionally included are IFT instances where emergency care providers requested ALS assistance/intervention.
Cases not meeting the inclusion criteria are excluded from consideration. Excluded cases were primary or emergency cases, patients triaged as green, yellow, or blue, IFTs conducted by emergency providers who are not ALS qualified, cases lacking attachments reserved for ALS providers, and instances where critical variables are missing.
Variables
The following variables were described: Patient demographics (age and gender), time intervals (response time, scene time, transfer time), primary diagnosis (respiratory, cardiovascular, gastrointestinal tract, and others), attachments, and clinical or pharmacological interventions. Based on the extracted variables we were able to describe the patient population's pathologies and needs during transfer. It is important to keep in mind that in all instances, more than one diagnosis, attachment or medication is possible for one patient. Furthermore, we quantified the types of IFTs that required ALS for transfers in and between facilities and described them accordingly.
Data extraction
After familiarising the statistician with the research aims, objectives, data variables and the contents of the WCG-EMS CAD database, the data from eligible cases were extracted. Regular meetings were held between the statistician and investigators to ensure credible extraction in line with Gilbert et al.'s[20] guidance on retrospective chart reviews in emergency care.
The ePCR system used by WC-EMS mandates completion of predefined clinical fields before case closure, ensuring that all analysed records include the required demographic, diagnostic, and clinical intervention data. Although free-text narrative fields may have been variably completed, they were not core to the study objectives and were therefore excluded from the analysis. No data imputation was performed, and only cases that met the completeness thresholds for critical variables were included in the final dataset.
Data analysis
The data were extracted onto a spreadsheet and analysed with the help of a senior WCG-EMS ECP. The cases were categorised based on the diagnosis, attachments, and medications.
Categorical variables (gender, diagnosis, types of attachments, types of medications) are described as frequencies and proportions. Continuous variables (age) are described as mean and standard deviation (SD) if seriously deviating from a normal distribution or median and interquartile range (IQR) if deviating markedly from a normal distribution. The data are presented as frequency (n) and proportion (%). Patient demographics were presented as both frequency and proportions (%) and as a range, depending on whether the data are continuous or categorical. Patient diagnoses were depicted as proportions (%). It is important to keep in mind that in all instances, more than one diagnosis, attachment or medication is possible for one patient.
Results
Demographics and acuity of patients transferred
Of the 25 635 adult patients transferred, 12 892 (50.3%) were male and 12 718 (49.7%) females. Fig. 1 shows how the sample was derived.
The average age (range) median age for the patients was 40 (18 - 101) years, after removal of some outliers ranging from 102 to 221 years. A total of 15 379 (60.0%) were triaged as orange (for very urgent management) upon arrival at the receiving facility and the remainder as red (for emergency or immediate management) 10 231 (40.0%).
Response, preparation, and transport times for the patient transfers
We also analysed the key time intervals (response time, scene time, transfer time) involved in patient transfers. The mean (SD) time spent (minutes:seconds) response time from the initial emergency call to the arrival at the receiving facility was 07:10 (11:00). Once at the receiving facility, the mean (SD) time spent (minutes:seconds) to prepare the patient for transfer was 16:58 (23:25). Finally, the mean (SD) duration of transport from departure to the final destination was 12:56 (18:26), highlighting the overall time taken for patient relocation. These time metrics are crucial for understanding and improving the efficiency of our patient transfer process.
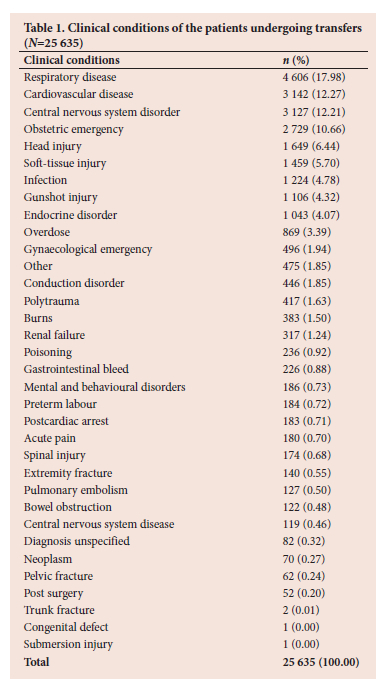
Clinical condition
Table 1 outlines the clinical condition of the patients transferred for the above-mentioned period. The most prevalent diagnosis was respiratory disease (n=4 605, 17.9 %), followed by cardiovascular disease (n=3 141, 12.3%) and central nervous system disorders (n=3 078, 12.0%).
Presence of indwelling devices and attachments
Table 2 presents the indwelling devices and attachments used during transfer. In total 72 061 attachments were reported (an average of three per patient). The most used devices or attachments were non-invasive blood pressure monitors (n=25 112, 98.0%) and pulse oximeters (n=24 600, 96.0%). A total of 4 693 patients (18.3%) were mechanically ventilated and 3 365 (13.1%) received support with passive oxygenation devices.
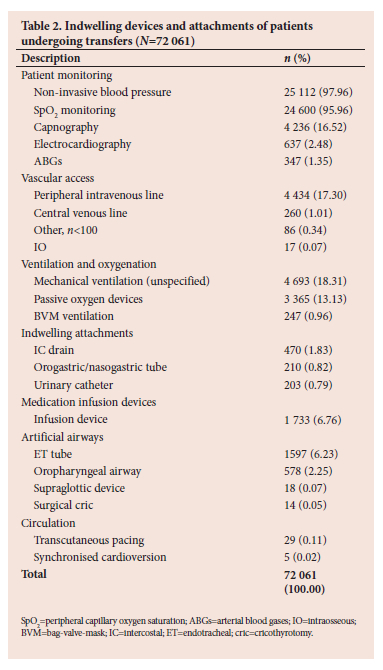
Peripheral intravenous access was noted as the most commonly used route for vascular access (n=4 434, 17.3%). The predominant indwelling catheter was an intercostal drain (n=470, 1.8%), followed by a nasogastric/orogastric tube (n=210, 0.8%).
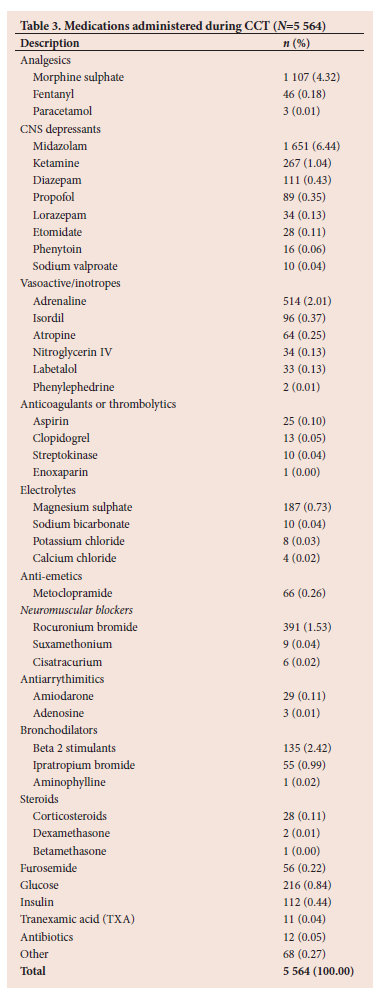
Medications and infusions
A total of 5 564 medications were recorded as being given either as bolus doses or as infusions. The overall prevalence of patients receiving medications during the transfer was 5 640 (22%). The most common route of administration was intravenous injection (n=1 944, 7.5%), followed by continuous infusion (n=1 752, 6.7%). A list of the medications recorded is presented in Table 3. Morphine was found to be the predominant analgesic administered (n=1 107, 4.3%), followed by fentanyl (n=46, 0.18%). Among central nervous system (CNS) depressants, the sedative agent most commonly used was midazolam (n=1 651, 6.4%). Adrenaline (n=514, 2.0%) was the most commonly used medication for inotropic support during transport.
Discussion
This study describes the sample of adult patients who underwent transfer by ALS emergency care providers within WCG-EMS. from January 2018 to December 2021. A total of 25 635 transfers were conducted during the study period, with 72 061 unique interventions or attachments needing monitoring in place.
Despite trauma being one of the leading causes of death in SA and being described as an epidemic in our country,[21] the majority of patients (n=20 241) who underwent ALS transfers in this sample suffered medical pathologies. Trauma and violence remain a concern, but it can be argued that many of those patients never make it to the hospital or the stage where they require CCT.[22] The shift towards a medical disease burden can be attributed to challenging socioeconomic status, lifestyle changes, and rapid urbanisation in some settings.[23,24]
The two most common clinical conditions were respiratory (n=4 606; 17.9%) and cardiovascular (n=3142; 12.3%) diseases. The disease prevalence noted in this sample comes as no anomaly, as LMICs such as SA have been seeing a significant epidemiological shift with more patients presenting with non-communicable diseases than communicable diseases, influenced by broader demographic, socioeconomic, technological, political, and cultural changes and urbanisation.[25] Further, it is important to note that a subset of our data derives from the COVID-19 pandemic, which most certainly inflated the number of patients who were suffering from respiratory emergencies/complications. A subsection of the sample, which occurred during the first and second waves of the COVID-19 pandemic in SA, could explain our results and the predominance of respiratory-related illnesses among patients undergoing ALS transfers.[26,27]
Cardiovascular diseases are the second most common clinical condition requiring CCTs in SA. This further highlights the epidemiological shift and the impact non-communicable diseases have on the healthcare system.[28] It also highlights the need for better heart healthcare facilities, preventive measures, and efficient patient referral pathways. It points to broader public health challenges, like lifestyle factors and access to timely medical care.[29,30] Improving these areas is essential for reducing the number of patients requiring transfers and those suffering deaths and continuous health issues related to cardiovascular diseases in SA.
The case distribution seen in this study coincides with data reported from Statistics SA, which also indicates a significant caseload shift towards non-communicable diseases.[23] This significant shift towards non-communicable diseases can be indicative of the need for the healthcare system to adapt to managing more chronic conditions, requiring long-term care and resource reallocation.
Caring for critically ill and injured patients is complex, as they often have multiple conditions requiring various treatment regimens. This complexity underscores the importance of specialised training and advanced equipment for healthcare practitioners. Providing them with the right skills and tools ensures effective care at the appropriate level for better patient outcomes.[12,31]
Notably, patient monitoring was the most common patient attachment in the study, with non-invasive blood pressure and pulse oximetry monitoring occurring in >95% of the ALS transfers. This finding is encouraging given the fact that related research has argued that continuous patient monitoring is of utmost importance to reduce adverse effects and to ensure continuous patient safety during transport.[11,32] Transport monitoring during inter- and intrahospital transfers improves patient care by alleviating the effects of transport stress on the patient and the EMS providers by providing real-time information and support, ensuring smoother and more efficient transfers, and ultimately improving the overall quality of patient care.[33] The implementation of routine monitoring is of paramount importance in risk mitigation and early detection of deterioration in critically ill and injured patients.
Second to non-invasive blood pressure and pulse oximetry monitoring, ventilation and vascular access were the most common attachments during transport. The high use of mechanical ventilators comes as no surprise given that part sampling frame for the study fell within the first and second waves of the COVID-19 pandemic in SA where increased use of mechanical ventilators was prevalent.[34] The pandemic not only posed a challenge to the system and healthcare providers as a result of increased patient loads but also to healthcare providers owing to abnormal management regimens and unique ventilation strategies, which often required extremely high oxygen concentration and significant adjustment from the normal ventilation strategies.[35]
To see that 90% of the patients undergoing mechanical ventilation during transport had end-tidal carbon dioxide (ETCO2) monitoring in place during transport is a positive and encouraging trend. These results concur with a study done in the SA private sector, but they have also shown that knowledge around capnography and its use was found to be good in most areas, but often lacking when dealing with more complicated patients and suggested the need for improved and ongoing training, as well as incorporation into curricula.[36]
ETCO2 serves as a valuable indicator of the effectiveness of ventilation and provides crucial information about a patient's respiratory status.[37] In the transport environment, where patients may be particularly vulnerable, continuous monitoring of ETCO2 helps healthcare providers assess the adequacy of ventilation, detect potential complications, and make timely adjustments to the ventilatory and haemodynamic support.[38]
This proactive approach enhances patient safety and contributes to better outcomes during the critical period of transport.[38] The integration of ETCO2 monitoring into routine practice reflects a commitment to delivering high-quality care in dynamic and challenging settings, ultimately fostering confidence in the management of ventilated patients during transport.[29]
When looking at analgesia and sedation in relation to mechanical ventilation, it is clear that only 4.5% of the patients received some analgesic, and 8.6% received some form of sedation. Given the fact that mechanical ventilation itself is uncomfortable, the use of analgesia and sedation in patients receiving mechanical ventilation is crucial for patient comfort, safety, and overall outcomes.[30] The clear underutilisation can be an indication of several issues.
Assessing pain in critically ill, intubated patients can be challenging, leading to under-recognition and inadequate analgesic administration.[40] Variability in adherence to protocols and guidelines for analgesia and sedation also contributes to inconsistent practice.[41] Additionally, practitioner judgment and variability in practice, with differing thresholds for administering analgesia and sedation based on individual assessments, further exacerbate the discrepancy in providing adequate pain relief to mechanically ventilated patients.[42]
Despite routine patient monitoring being commonplace, the utilisation and reporting of electrocardiograms (ECGs) appear to be inadequate. This deficiency can be ascribed to various factors, including equipment availability, under-reporting, under-utilisation, practitioner attitudes, and motion artefacts induced by transport stressors.[43,44] Given the prevalence of cardiovascular conditions among patients, the under-reporting of ECGs may reflect clinical oversight, potentially exacerbated by recall bias and documentation errors.[45,46] In addition to the above, the lack of localised standards for patient monitoring could also contribute to the non-use of ECGs, and additional training might also be required to ensure optimal cardiac monitoring for patients undergoing CCTs.[47]
It was evident that there is no given standard for the parameters that should be monitored and recorded during transport. The parameters being monitored and reported among these patients vary greatly, and this highlights the absence of standardised monitoring parameters among healthcare providers responsible for transporting these patients. Internationally monitoring respiratory and cardiac function during transport is routinely done during prehospital, intrahospital, and interhospital transport.[32]
No literature regarding localised standards for patient monitoring during transfer could be found. However, current international guidelines provide a framework for required monitoring, but they vary slightly and need to be updated. In mechanically ventilated patients, oximetry, ECG, blood pressure, and capnography are integral to the standards of care.[32]
Non-intubated patient monitoring during transport has rarely been studied and the inclusion of early warning systems should be explored to improve patient safety among these patients.[32] The variation in monitoring standards among practitioners and the patients indicates a critical need for standardising protocols in healthcare to ensure consistent, high-quality patient care during CCTs.[36,37]
Practitioners who conducted these transfers used a wide variety of medications, the most commonly used being midazolam (n=1 651) and morphine (n=1 107). While 18.3% of the patients underwent mechanical ventilation, only 4.5% of them received some analgesia during care, which indicates a clear underutilisation or an error in reporting practices. Critical illness and injury frequently cause pain, stemming from both the underlying condition and essential medical procedures conducted for patient monitoring and care. It is imperative to ensure good analgesic and sedation practices.[48] Accurate assessment and management of pain remain crucial considerations in the care of critically ill patients, particularly among those unable to self-report, as pain is often overlooked and undertreated in this population.[49]
While most of these medications used during CCT are within the current scope of practice for ALS practitioners, many are not meant to be used for initiating care but rather for continuing care. The fact that 21.7% of patients received one or a combination of medications during these transfers suggests the complexity as it might result in multiple administration methodologies and additional equipment use such as infusion devices.[50,51] Furthermore, the medications administered during CCTs are often weight-based, requiring complex calculations under high pressure.[51]
EMS training in the current SA context is heavily guided by the scope of practice, skills and capabilities of the various cadres as outlined by the Health Professions Council of South Africa (HPCSA).[52] Owing to the variation in training and the scope-driven nature of EMS training, ALS practitioners often receive limited or no training on medications that are not listed for initiation of care within their current scope of practice.[13,53] Medications like propofol, phenytoin, phenylephrine, cisatracurium, and antibiotics are used during some ALS transfers, but practitioners may not have received adequate training on their use as these do not form part of the standard scope of practice, and EMS practitioners get trained on specific medications only, rather than classes of medications as seen in other professions. It is evident that the practitioners handling these transfers need additional training and possess limited exposure to and experience with certain medications crucial for the care of critically ill and injured patients. [54,55] Research in this field consistently highlights the substantial safety risks associated with performing procedures or administering medications when practitioners lack regular exposure to these skills or medications.[56]
Previous work has been done exploring the capabilities and scope-of-practice requirements for SA ALS practitioners undertaking CCTs, and positive consensus has been gained for many of the medications reported in this study, thus highlighting the need for structured training for CCRS practitioners.[15,53] In addition to dedicated training, it is recommended that a dedicated crew be assigned to undertake all of the transfers to ensure competency can be maintained.[14]
However, there is a consensus that additional dedicated training and specialised equipment tailored for critically ill and injured patients undergoing CCTs are necessary.[5,6,53] In SA, all ALS practitioners have the capability to carry out ALS transfers. However, the qualifications of these paramedics are not consistent and vary from a 1-year certificate to a 2-year diploma or a 4-year degree. It is unclear whether there is a standardised approach to training across these qualifications or if they are benchmarked against some criteria.[13]
Critical care retrieval resources are often the most expensive resources operated within the EMS and should be used to maximum efficiency; we should aim to optimise the cost-benefit ratio, especially for resource-limited settings such as SA.[57,58] The cost-effective use of such services can partially be achieved if we ensure that we service the appropriate patient population and cases, as advocated in the CCRS definition.[14]
From work done in the SA context, it is clear that there is a significant mismatch between the dispatch of EMS resources and actual patient needs, resulting in significantly high levels of inappropriate emergency responses and waste expenditure.[59]
As a result, there are no clear guidelines or criteria for determining which level of provider to dispatch for specific cases. To address this, we could develop standardised protocols based on patient acuity and medical needs and utilise data analytics to improve decision-making processes.[57,59] Additionally, regular training and audits could ensure adherence to these guidelines, thereby optimising resource allocation and reducing the mismatch between the dispatch of EMS resources and actual patient needs.
A recent study scrutinising the BEMC degree offerings at various SA universities revealed that upon comparing all components, the universities offering BEMC displayed more similarities than differences.[60] Whether the contents and components being taught are applicable to the SA patient population and healthcare system, or if the students are sufficiently equipped for clinical practice, remains uncertain. The majority of the patients transferred by ALS in this study population align with the concepts and/or modules being taught in the critical care transportation modules across SA bachelor's degrees; however, it is uncertain whether all the content is covered at adequate depth to meet patient needs and complexity since prehospital providers consistently feel underprepared and ill-equipped to undertake CCTs.[14,16]
Limitations
It is important to note that this study has several limitations. Firstly, the study adopted a retrospective approach, utilising clinical records for sampling and analysis. These records were not originally intended for research purposes, potentially compromising the accuracy of the diagnoses and clinical data. Additionally, since these case reports were completed by the healthcare providers caring for the patients, the research team could not independently verify the information.
The results may be inaccurate because ePCRs were used as the primary data source. This may result in some inaccuracies and potential recall bias, which, in some instances, limit the comprehensiveness and overall accuracy of the study. Additionally, the study only considered patients who underwent ALS transfers and did not consider the level of patient acuity or analyse their conditions before and after the transfers.
Finally, because only patients who underwent ALS transfers were included, it is possible that some cases that required ALS or where ALS was requested but not available because of resource constraints were missed.
Conclusion
This study is the first to analyse adult patients undergoing ALS transfers within the WCG-EMS in SA from 2018 to 2021, offering a better understanding of the patient population being transferred.
The study underscores the importance of continuous patient monitoring, highlighting encouraging trends and improvement areas, particularly in ECG monitoring. Medication practices during transfers revealed inconsistencies and the need for better training. These findings emphasise the necessity for standardised protocols and structured training programmes, which could inform educational initiatives, equipment procurement, and the development of the CCRS curriculum in SA. Additionally, this research could help establish clinical standards for dispatching specific ALS cadres based on patient needs.
Data availability. The data used for this study are available from the authors on request.
Declaration. None.
Acknowledgements. None.
Author contributions. LCvR: conceptualisation,methodology, data curation, formal analysis, investigation,writing - original draft, writing - review and editing. NM: data analysis, writing - original draft (results and discussion), writing - review and editing. CV-L: protocol development, supervision, writing - review and editing.WS: conceptualisation, protocol development, supervision, writing - review and editing.
Funding. None.
Conflicts of interest. None.
References
1. Dunn MJG, Gwinnutt CL, Gray AJ. Critical care in the emergency department: Patient transfer. Emerg Med J 2007;24(1):40-44. https://doi.org/10.1136/emj.2006.042044 [ Links ]
2. Neely AH, Ponshunmugam A. A qualitative approach to examining health care access in rural South Africa. Soc Sci Med 2019;230:214-221. https://doi.org/10.1016/j.socscimed2019.04.025 [ Links ]
3. Gumede DM, Taylor M, Kvalsvig JD. Engaging future healthcare professionals for rural health services in South Africa: Students, graduates and managers' perceptions. BMC Health Serv Res 2021;21(1):220 https://doi.org/10.1186/s12913-021-06178-w [ Links ]
4. Ashokcoomar P. Inter-healthcare facility transfer of critically ill neonates: The development of a programme for emergency medical care in the South African context. Durban University of Technology, South Africa, 2018. http://hdl.handle.net/10321/3245 (accessed 20 January 2024). https://doi.org/10.51415/10321/3245 [ Links ]
5. Puchalski Ritchie LM, Khan S, Moore JE, et al. Low- and middle-income countries face many common barriers to implementation of maternal health evidence products. J Clin Epidemiol 2016;76:229-237. https://doi.org/10.1016/j.jclinepi.2016.02.017 [ Links ]
6. Scribante J, Bhagwanjee S. National audit of critical care resources in South Africa: Unit and bed distribution. S Afr Med J 2007;97(12):1311. [ Links ]
7. Kautzky K, Tollman SM. A perspective on primary health care in South Africa: Primary health care: In context . South African Health Review 2008;1. https://doi/10.10520/EJC35514 (accessed 3 October 2023). [ Links ]
8. Corke C, de Leeuw E, Lo SK, George C. Predicting future intensive care demand in Australia. Crit Care Resusc J Australas Acad Crit Care Med 2009;11(4):257-260. https://doi.org/10.1016/S1441-2772(23)01284-X [ Links ]
9. Komashie A, Ward J, Bashford T, et al. Systems approach to health service design, delivery and improvement: A systematic review and meta-analysis. BMJ Open 2021;11(1):e037667. https://doi.org/10.1136/bmjopen-2020-037667 [ Links ]
10. Droogh JM, Smit M, Absalom AR, Ligtenberg JJ, Zijlstra JG. Transferring the critically ill patient: Are we there yet? Crit Care 2015;19(1):62. https://doi.org/10.1186/s13054-015-0749-4 [ Links ]
11. Alabdali A, Fischer JD, Trivedy C, Lilford R. A systematic review of the prevalence and types of adverse events in interfacility critical care transfers by paramedics. Air Med J 2017;36(30:116-121. https://doi.org/10.1016/j.amj.2017.01.011 [ Links ]
12. Bourn S, Wijesingha S, Nordmann G. Transfer of the critically ill adult patient. BJA Educ 2018;18(3):63-68. https://doi.org/10.1016/j.bjae.2017.11.008 [ Links ]
13. Venter M, Stanton D, Conradie N, Jordaan L, Venter C, Stassen W. The need for setting standards in critical care transfers. South Afr J Crit Care 2017;33(1):32-39. https://doi.org/10.7196/SAJCC.2017.v33i1.319 [ Links ]
14. Venter C, Conradie N, Venter M, et al. A proposed definition of Critical Care Retrieval in the South African context. S Afr J Pre-Hosp Emerg Care 2021 Jul;2(1). https://www.journals.ac.za/index.php/sajpec/article/view/4477. https://doi.org/10.24213/2-1-4477 [ Links ]
15. Andrews S, Catlin S, Lamb N, Christensen M. A dedicated retrieval and transfer service: The QUARTS Project. Nurs Crit Care 2008;13(3):162-168. https://doi.org/10.1111/j.1478-5153.2008.00272.x [ Links ]
16. Senekal ACG, Vincent-Lambert C. Experiences of emergency care providers conducting critical care transfers in Gauteng Province, South Africa. South Afr J Crit Care 2022;37(3):92-96. https://doi.org/10.7196/SAJCC.2021.v37i3.487 [ Links ]
17. Gimenez FMP, de Camargo WHB, Gomes ACB, et al. Analysis of adverse events during intrahospital transportation of critically ill patients. Crit Care Res Pract 2017:6847124. https://doi.org/10.1155/2017/6847124 [ Links ]
18. Cuschieri S. The STROBE guidelines. Saudi J Anaesth 2019;13(Suppl 1):S31-4. https://doi.org/10.4103/sja.SJA_543_18 [ Links ]
19. Western Cape Government. Medical emergency transport and rescue. https://www.westerncape.gov.za/service/medical-emergency-transport-and-rescue-metro. (accessed 22 January 20201. [ Links ]
20. Gilbert EH, Lowenstein SR, Koziol-McLain J, Barta DC, Steiner J. Chart reviews in emergency medicine research: Where are the methods? Ann Emerg Med 1996;27(3):305-308. https://doi.org/10.1016/s0196-0644(96)70264-0 [ Links ]
21. Seggie J. Editor's choice. Trauma: South Africa's other epidemic. S Afr Med J 2013;103(9):589-590. [ Links ]
22. Finn J, Dixon JM, Moreira F, et al. Patterns of on-scene and healthcare system trauma deaths in the Western Cape of South Africa. World J Surg 2024;48(2):320-330. https://doi.org/10.1002/wjs.12043 [ Links ]
23. Statistics South Africa. Rising non-communicable diseases: A looming health crisis. Statistics South Africa. 2023 https://www.statssa.gov.za/?p=16729. (accessed 22 February 2024). [ Links ]
24. Mayosi BM, Lawn JE, van Niekerk A, Bradshaw D, Karim SSA, Coovadia HM. Health in South Africa: Changes and challenges since 2009. Lancet 2012;380(9858):2029-2043. https://doi.org/10.1016/S0140-6736(12)61814-5 [ Links ]
25. Kabudula CW, Houle B, Collinson MA, et al. Progression of the epidemiological transition in a rural South African setting: Findings from population surveillance in Agincourt, 1993-2013. BMC Public Health 2017;17(1):424. https://doi.org/10.1186/s12889-017-4312-x [ Links ]
26. Maslo C, Friedland R, Toubkin M, Laubscher A, Akaloo T, Kama B. Characteristics and outcomes of hospitalised patients in South Africa during the COVID-19 omicron wave compared with previous waves. JAMA 2022;327(6):583-584. https://doi.org/10.1001/jama.2021.24868 [ Links ]
27. Mbunge E. Effects of COVID-19 in South African health system and society: An explanatory study. Diabetes Metab Syndr Clin Res Rev 2020;14(6):1809-1814. https://doi.org/10.1016/j.dsx.2020.09.016 [ Links ]
28. Hadian M, Mozafari MR, Mazaheri E, Jabbari A. Challenges of the health system in preventing non-communicable diseases: Systematised review. Int J Prev Med 2021; 12:71. https://doi.org/10.4103/ijpvm.IJPVM_487_20 [ Links ]
29. Douglas M, Kgatla N, Sodi T, et al. Facilitators and barriers in prevention of cardiovascular disease in Limpopo, South Africa: A qualitative study conducted with primary health care managers. BMC Cardiovasc Disord 2021;21:492. https://doi.org/10.1186/s12872-021-02290-1 [ Links ]
30. Cappuccio FP, Miller MA. Cardiovascular disease and hypertension in sub-Saharan Africa: Burden, risk and interventions. Intern Emerg Med 2016;11:299-305. https://doi.org/10.1007/s11739-016-1423-9 [ Links ]
31. Martin T. Transporting the adult critically ill patient. Surg Oxf 2021;39(1):15-21. https://doi.org/10.1016/j.mpsur.2020.11.006 [ Links ]
32. Branson RD, Rodriquez D. Monitoring during transport. Respir Care 2020;65(6):882-893. https://doi.org/10.4187/respcare.07796 [ Links ]
33. Mindray North America. Monitoring patients during transport. https://www.mindraynorthamerica.com/monitoring-patients-during-transport (accessed 23 January 2024). [ Links ]
34. Dar M, Swamy L, Gavin D, Theodore A. Mechanical-ventilation supply and options for the COVID-19 pandemic. Leveraging all available resources for a limited resource in a crisis. Ann Am Thorac Soc 2021;18(3):408-416. https://doi.org/10.1513/AnnalsATS.202004-317CME [ Links ]
35. Möhlenkamp S, Thiele H. Ventilation of COVID-19 patients in intensive care units. Herz 2020;45(4):329-331 https://doi.org/10.1007/s00059-020-04923-1 [ Links ]
36. Wylie C, Welzel T, Hodkinson P. Waveform capnography in a South African prehospital service: Knowledge assessment of paramedics. Afr J Emerg Med 2019;9(2):96-100. https://doi.org/10.1016/j.afjem.2019.01.010 [ Links ]
37. Nagler J, Krauss B. Capnography: A valuable tool for airway management. Emerg Med Clin North Am 2008;26(4):881-897. https://doi.org/10.1016/j.emc.2008.08.005 [ Links ]
38. Kupnik D, Skok P. Capnometry in the prehospital setting: Are we using its potential? Emerg Med J 2007;24(9):614-617. https://doi.org/10.1136/emj.2006.044081. [ Links ]
39. Patel SB, Kress JP. Sedation and analgesia in the mechanically ventilated patient. Am J Respir Crit Care Med 2012;185(5):486-497. https://doi.org/10.1164/rccm.201102-0273CI [ Links ]
40. Hylén M, Akerman E, Alm-Roijer C, Idvall E. Behavioral Pain Scale - translation, reliability, and validity in a Swedish context. Acta Anaesthesiol Scand 2016;60(6):821-828. https://doi.org/10.1111/aas.12688 [ Links ]
41. Ayasrah SM, O'Neill TM, Abdalrahim MS, Sutary MM, Kharabsheh MS. Pain assessment and management in critically ill intubated patients in Jordan: A prospective study. Int J Health Sci 2014;8(3):287-298. https://doi.org/10.12816/0023981 [ Links ]
42. Taylor DM, Chen J, Khan M, et al. Variables associated with administration of analgesia, nurse-initiated analgesia and early analgesia in the emergency department Emerg Med J 2017;34:13-19. https://emj.bmj.com/content/34/1/13. https://doi.org/10.1136/emermed-2016-206044 [ Links ]
43. Hiilcrom. Three factors that could be impacting your ECG interpretation. https://www.hillrom.eu/en/knowledge/article/three-factors-that-could-be-impacting-your-ecg-interpretation/. (accessed 4 October 2023). [ Links ]
44. Milligan JE, Jones CN, Helm DR, Munford BJ. The principles of aeromedical retrieval of the critically ill. Trends Anaesth Crit Care 2011;1(1):22-26. https://doi.org/10.1016/j.cacc.2010.07.019 [ Links ]
45. Elliott M, Endacott R. The clinical neglect of vital signs' assessment: An emerging patient safety issue? Contemp Nurs 2022;58(4):249-252. https://doi.org/10.1080/10376178.2022.2109494 [ Links ]
46. Moreno-Serra R, Anaya-Montes M, León-Giraldo S, Bernal O. Addressing recall bias in (post-) conflict data collection and analysis: Lessons from a large-scale health survey in Colombia. Confl Health 2022;16:14. https://doi.org/10.1186/s13031-022-00446-0 [ Links ]
47. Giusti ACBD, Cornélio ME, de Oliveira EM, Giguère JF, Gallani MCBJ. Standard practices in cardiac monitoring: Training needs of intensive care unit nurses. BMC Nurs 2024;23:82. https://doi.org/10.1186/s12912-024-01742-1 [ Links ]
48. Pota V, Coppolino F, Barbarisi A, et al. Pain in intensive care: A narrative review. Pain Ther 2022;11(2):359-367. https://doi.org/10.1007/s40122-022-00366-0 [ Links ]
49. Nordness MF, Hayhurst CJ, Pandharipande P. Current perspectives on the assessment and management of pain in the intensive care unit. J Pain Res 2021;14:1733. https://doi.org/10.2147/JPR.S256406 [ Links ]
50. Moyen E, Camiré E, Stelfox HT. Clinical review: Medication errors in critical care. Crit Care 2008;12(2):208. https://doi.org/10.1186/cc6813 [ Links ]
51. Bourne RS, Phipps DL, Jennings JK, et al. Medication safety for intensive care patients transferring to a hospital ward: A hierarchical task analysis. Hum Factors Health 2022; 2:100030. https://doi.org/10.1016/j.hfh.2022.100030 [ Links ]
52. Health Professions Council of South Africa. Clinical Practice Guidelines for Emergency Care Providers. Health Professions Council of South Africa, 2018. https://www.hpcsa.co.za/Uploads/EMB/CLINICALPRACTICEGUIDELINESPROTOCOLS-JULY 2018.pdf (accessed 17 September 2025). [ Links ]
53. Venter M, Stassen W. A national retrospective descriptive analysis of critical care transfers in the private sector in South Africa. S Afr Med J 2023;113:e672. https://doi.org/10.7196/SAMJ.2023.v113i8.672 [ Links ]
54. Laws S, Wang C, Halter M. Knowledge, attitudes and practices of UK paramedics regarding pharmacology and the legal, management and administration aspects of medicines: A cross-sectional online quantitative survey. Br Paramed J 2020;5(2):1-9. https://doi.org/10.29045/14784726.2020.09.5.2.1 [ Links ]
55. Leggio WJ, Grawey T, Stilley J, Dorsett M. EMS curriculum should educate beyond a technical scope of practice: Position statement and resource document. Prehosp Emerg Care 2021;25(5):724-729. https://doi.org/10.1080/10903127.2021.1925793 [ Links ]
56. Alanazi A. Intubations and airway management: An overview of hassles through third millennium. J Emerg Trauma Shock 2015;8(2):99-107. https://doi.org/10.4103/0974-2700.145401 [ Links ]
57. Laatz D, Welzel T, Stassen W. Developing a South African Helicopter Emergency Medical Service Activation Screen (SAHAS): A Delphi study. Afr J Emerg Med 2019;9(1):1-7. https://doi.org/10.1016/j.afjem.2018.09.001 [ Links ]
58. Murdoch I, Sajjanhar T, Tibby S, Hatherill M, Marsh M. Cost-effectiveness of a paediatric retrieval service. Crit Care 1997;1(1):P126. https://doi.org/10.1186/cc97 [ Links ]
59. Newton PR, Naidoo R, Brysiewicz P. The appropriateness of emergency medical service responses in the eThekwini district of KwaZulu-Natal, South Africa. S Afr Med J 2015;105(10):844-847. https://doi.org/10.7196/SAMJnew.8273 [ Links ]
60. Conradie NJ, Vincent-Lambert C, Stassen W. A comparison of the content taught in critical care transportation modules across South African bachelor's degrees in emergency medical care. South Afr J Crit Care. 2022 May 6;38(1):10.7196/SAJCC.2022.v38i1.498. https://doi.org/10.7196/SAJCC.2022.v38i1.498 [ Links ]
 Correspondence:
Correspondence:
L C van Rensburg
louis.vanrensburg1@outlook.com
Received 24 March 2025
Accepted 21 July 2025
Contribution of study
This study provides the first large, system-wide description of 25 635 adult advanced life support (ALS) interfacility transfers in the Western Cape public emergency medical service (2018 - 2021), detailing patient profiles, monitoring, devices, and medications. By mapping real-world care patterns, especially gaps in electrocardiograph monitoring and analgesia/sedation for ventilated patients, it generates the empirical baseline needed to standardise protocols and formally develop a critical care retrieval services (CCRS) curriculum aligned to local needs. The findings also support evidence-based equipment planning and ALS cadre dispatch criteria.

{kind=link}