










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151Print version ISSN 0038-2361
S. Afr. j. surg. vol.63 n.1 Cape Town 2025
https://doi.org/10.36303/SAJS.01082
HOW TO DO IT
Photo- and video-documentation of gastrointestinal endoscopy in under-resourced settings
MF Scriba; GE Chinnery; SR Thomson
Surgical Gastroenterology Unit, Groote Schuur Hospital, University of Cape Town, South Africa
SUMMARY
A visual record of standardised anatomical landmarks and specific pathology in gastrointestinal endoscopy is now considered by international endoscopy and gastroenterology societies as a mandatory component of the procedural report.14 Photo and video documentation of gastrointestinal endoscopy procedures accurately monitor key performance indicators (KPAs) for trainees and consultants, which are essential to assess the attainment and maintenance of competency. In addition, visual documentation is an excellent adjunct for feedback during training, enables remote teaching and mentorship, is essential for multidisciplinary teams (MDTs) and the conducting of clinical audits, and may be invaluable for medicolegal purposes.
The endoscopy equipment of all the major manufacturers in South Africa (Fuji Film, Olympus and Pentax) allows for image capturing directly from buttons on the control handle to a Universal Serial Bus (USB) flash drive. The flash drive can be used to transfer images, and in some instances video, to a reporting computer, but involves time-consuming manual transfers. Some systems have polaroid reproduction systems which are usually single-print photographs attached to reports and generally only document pathology. Commercial medical video hardware and software technology is costly. For example, one of the manufacturers has reporting software and hardware, at a cost of about ZAR 250 000 per stack, that allows direct video and image capture.5 Such major costs highlight the major hurdle to routine photo or video documentation in under-resourced settings.
We describe the development in the Groote Schuur Hospital Gastrointestinal Unit of a simple, low-cost method of still-image and video capture that can be set up on current endoscopy equipment to provide routine still-image and video capture. This system makes use of inexpensive hardware and open access software. It has been implemented and is in routine use for oesophagogastroduodenoscopy, colonoscopy, and advanced interventional endoscopy.
Keywords: upper gastrointestinal endoscopy, photo documentation, low-resource setting, routine documentation
Description
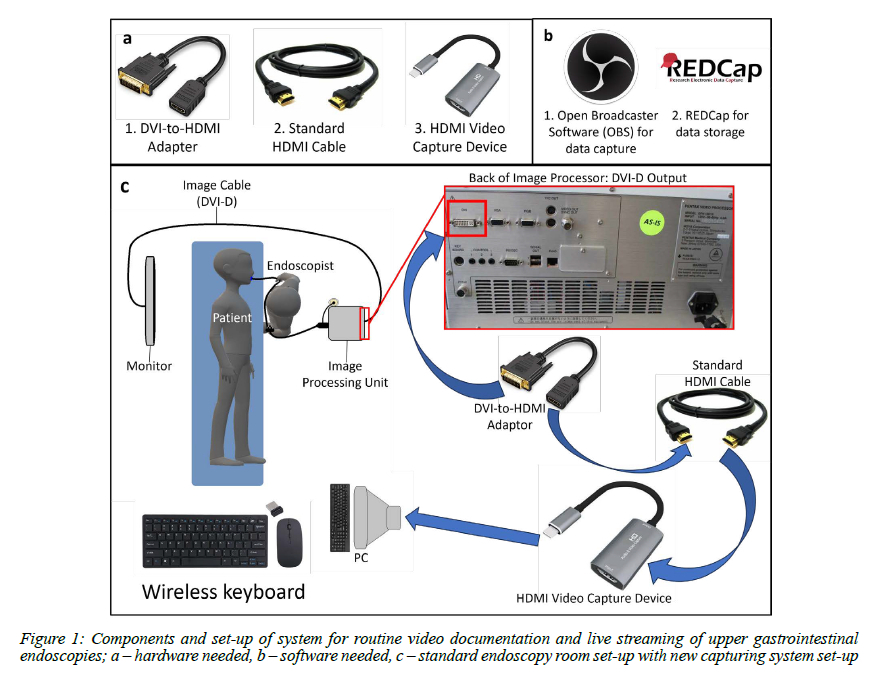
The endoscopy unit at Groote Schuur Hospital has five endoscopy rooms with flexible endoscopy towers equipped with image-processing units and output monitors. Each room has a computer with a Microsoft Windows operating system. This computer is used to create an electronic endoscopy report based on locally developed software for the documentation of all endoscopies and allows the integration of images into the database. In order to allow for photo and video capturing and digital storage, the images needed to be relayed from the image processor or monitor to the computer. The hardware and software components and connections required are shown in Figures 1a and 1b. This requires knowledge of the video output connectors present on the image processor or the monitor as either can be used for capture. The monitor can only output the same signal type as its input. Common analogue outputs include Composite, Component, Video Graphics Array (VGA), and Separate Video (S-Video). Their image quality transmission is poorer than direct digital outputs. Digital Visual Interfaces were originally used for analogue transmission (DVI-A) but are now used for digital transmission (DVI-D: digital, DVI-I: integral). DVI-D is the most common output from modern endoscopy processor and monitor units.
This output requires only a connection adapter to be cabled via a High-Definition Multimedia Interface (HDMI) to a Universal Serial Bus (USB) video capture device as detailed in Figure 1. All hardware needed is easily obtainable online and the approximate cost of these connections is:
• DVI-to-HDMI adaptor: R100
• Five-metre HDMI cable: R100
• HDMI video capture card: R400-R600.
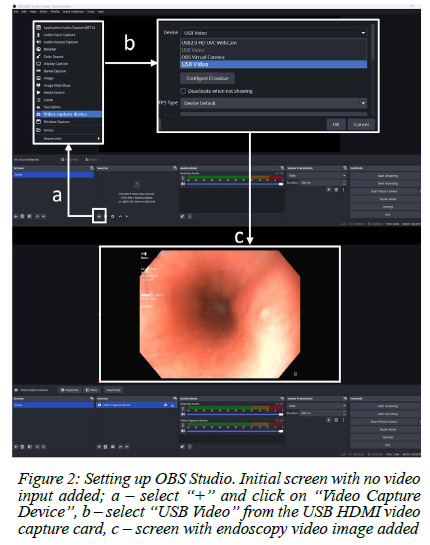
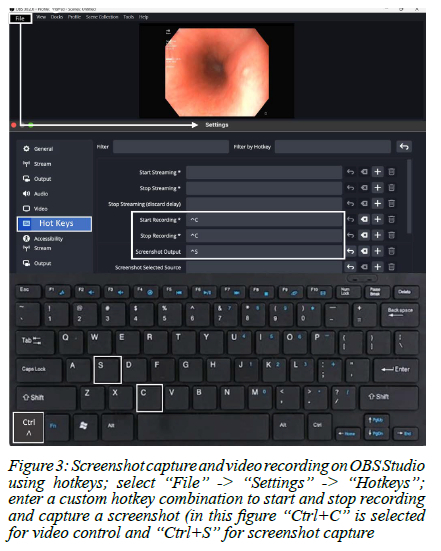
Open Broadcaster Software (OBS Studio) is an open source free download from https://obsproject.com. OBS Studio, once installed, allows for both continuous video capture and screenshots for still photo documentation. Step-by-step details on how to add a Video Capture Device, start and stop video recording and capture a still-image using OBS software are shown in Figures 2 and 3. Minimum system requirements to allow this video capture system to work are mainly determined by the OBS Studio requirements. OBS Studio requires Microsoft Windows 10 or 11 but is also compatible with macOS and Linux/Unix operating systems. Further software and hardware requirements depend on what encoder is chosen, the needed resolution and frames per second.6
Video/image saving and documentation
Written documentation and reporting of all upper gastrointestinal endoscopies performed at Groote Schuur Hospital is performed using an ethically approved and password-protected electronic registry (the Upper Gastrointestinal Surgery Registry, HREC R031/2015) with the Research Electronic Data Capture (REDCap) tool hosted at the University of Cape Town.7,8 REDCap allows for uploading of images or videos directly onto the registry as part of the routine digital endoscopy report, which is remotely stored and subsequently accessible from any device with an internet connection. Figure 4 shows how images are uploaded onto the REDCap registry. Images or videos captured using the OBS System do not contain patient identifying data, but once added to the endoscopy report on REDCap are then linked to the specific patient. Images or videos stored on the computer (separately from the password-protected and ethically approved registry) thus do not contain patient identification data, allowing for compliance with the Protection of Personal Information
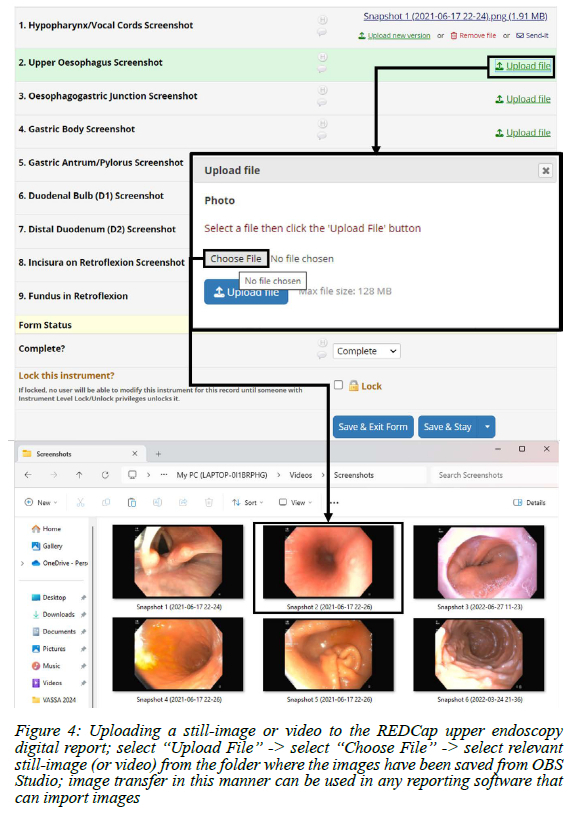
Act (POPIA) and the set-up of this image-capturing system thus would not require specific ethical approval. The use of an electronic registry which stores patient identifiers (for routine note-keeping or for research) would of course require ethical approval and the system used at Groote Schuur Hospital has been approved by the University of Cape Town Human Research Ethics Committee.
Set-up and implementation
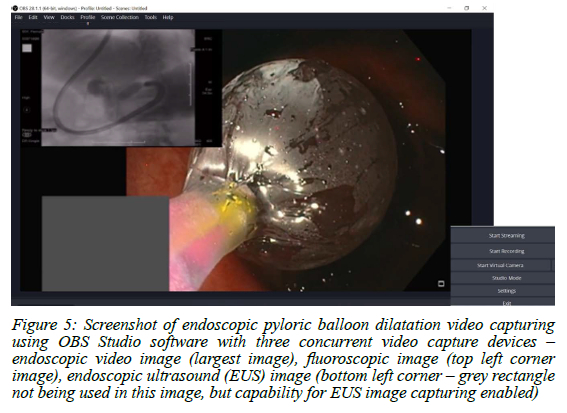
Once the system was set up, it allowed for immediate image and video-capturing. However, during interventional endoscopy procedures where fluoroscopy and/or endoscopic ultrasound (EUS) were used, separate DVI-HDMI adaptors, HDMI cables and HDMI video capture cards were used to import each modality into OBS Studio, which can handle up to four simultaneous video capture devices as shown in Figure 5.
Discussion
The system initially came about as a mechanism to provide undergraduate remote exposure to live endoscopy during the COVID-19 pandemic and has serendipitously come into general usage. A similar system using low-cost streaming capabilities for urological surgery at our institution highlights the importance of this type of innovation in low-resource settings.9 Compared to commercially available medical video capture devices and systems, which may be prohibitively expensive, this system is extremely low-cost, totalling only R600.
As a routine connection for image and video capturing is now always available, it has not only enhanced our undergraduate teaching but allowed us to create a library of high-quality endoscopic videos portraying a myriad pathologies and interventions for postgraduate teaching. Image and video storage and recall has also benefitted our practice by reducing unnecessary repeat endoscopies and enhanced our oncology multidisciplinary team (MDT) meetings.
Though it is feasible to take and upload the required screenshots for photo documentation on REDCap, the system has limitations with regard to routine video storage, particularly of interventional procedures, due to a maximum file size of 128 MB, which equates to about 4-5 minutes of video. At present, endoscopists will only video-capture interesting or important pathologies, not to the reporting system but to the computer hard drive, which itself has limited storage. The latest endoscopy processor output images are in DICOM file format, which can be integrated into hospital informatic storage systems or can be cloud based.
Conclusion
This low-cost and easy-to-set-up system confirms that image and video documentation for gastrointestinal endoscopy is feasible and implementable in low-resource settings. It allows for compliance with current electronic endoscopy reporting guidelines and has led to an improvement in clinical care and endoscopy training in our institution. We believe this system can be set up in other low-resource centres and integrated into a variety of endoscopy reporting systems. We encourage endoscopists and endoscopy unit managers to take the necessary steps to achieve this.
Conflict of interest
The authors declare no conflict of interest.
ORCID
MF Scriba https://orcid.org/0000-0001-8903-0510
GE Chinnery https://orcid.org/0000-0002-9097-8648
SR Thomson https://orcid.org/0000-0002-9485-997X
REFERENCES
1. Rey JF, Lambert R; ESGE Quality Assurance Committee. ESGE recommendations for quality control in gastrointestinal endoscopy: Guidelines for image documentation in upper and lower GI endoscopy. Endoscopy. 2001;33(10):901-3. https://doi.org/10.1055/s-2001-42537. [ Links ]
2. Beg S, Ragunath K, Wyman A, et al. Quality standards in upper gastrointestinal endoscopy: a position statement of the British Society of Gastroenterology (BSG) and Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland (AUGIS). Gut. 2017;66(11):1886-99. https://doi.org/10.1136/gutjnl-2017-314109. [ Links ]
3. Park WG, Shaheen NJ, Cohen J, et al. Quality indicators for EGD. Am J Gastroenterol. 2015;110(1):60-71. https://doi.org/10.1038/ajg.2014.384. [ Links ]
4. Emura F, Sharma P, Arantes V, et al. Principles and practice to facilitate complete photodocumentation of the upper gastrointestinal tract: World Endoscopy Organisation position statement. Dig Endosc. 2020;32(2):168-79. https://doi.org/10.1111/den.13530. [ Links ]
5. Olympus. EndoWorks 7 - Endoscopy Information Management Solution. Interface Compatibility. Available from: https://content.medical.olympusamerica.com/sites/default/files/pdf/EW_interface_compat.pdf. Accessed 18 September 2024. [ Links ]
6. Open Broadcaster Software - Basic System Requirements. Available from: https://obsproject.com/kb/system-requirements. Accessed 4 December 2024. [ Links ]
7. Harris PA, Taylor R, Thielke R, et al. Research electronic data capture (REDCap)-a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-81. https://doi.org/10.1016/jobi.2008.08.010. [ Links ]
8. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208. [ Links ]
9. Lazarus J, Thomson S. Video transmission of urology surgeries - proof of concept in a resource-constrained environment. Afr Urol. 2022;2(1):1-6. https://doi.org/10.36303/AUJ.0035. [ Links ]
 Correspondence:
Correspondence:
Email: matthias.scriba@gmail.com

{kind=link}