










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Surgery
On-line version ISSN 2078-5151Print version ISSN 0038-2361
S. Afr. j. surg. vol.62 n.2 Cape Town 2024
https://doi.org/10.36303/SAJS.00198
HPB SURGERY
Liver resection for hepatocellular and fibrolamellar carcinoma in a South African tertiary referral centre - an observational cohort analysis
Y ZiaeiI; JEJ KrigeI; EG JonasI, II; UK KotzeI, II; MM BernonI; C KloppersI; S SobnachI
IDepartment of Surgery, Faculty of Health Sciences, University of Cape Town, South Africa
IISurgical Gastroenterology and HPB Surgery Unit, Groote Schuur Hospital, Observatory, Cape Town, South Africa
ABSTRACT
BACKGROUND: More than 80% of global hepatocellular carcinomas (HCC) occur in sub-Saharan Africa (SSA) and South East Asia. Compared with the rest of the world, HCC in SSA has the lowest resection and survival rates. This study assessed outcome following liver resection for HCC and fibrolamellär carcinoma (FLC) at a tertiary referral centre in South Africa.
METHODS: A retrospective analysis was done of all liver resections for HCC and FLC at Groote Schuur Hospital and the University of Cape Town Private Academic Hospital between January 1990 and December 2021. Three groups were compared, (i) HCC occurring in normal livers, (ii) HCC occurring in cirrhotic livers, and (iii) fibrolamellar carcinoma. Postoperative complications were classified as per the expanded accordion severity grading system. Median overall survival (OS) and 95% confidence intervals (CI) were calculated.
RESULTS: Forty-eight patients were included in the study, 25 for HCC in non-cirrhotic livers, 15 in cirrhotic livers and eight for FLC. Thirty-six patients (75%) underwent a major resection. No mortality occurred but 16 patients (33%) developed grade 1 to 4 complications postoperatively. Thirty-three patients (69%) developed recurrence of HCC following their initial resection of whom 29 (60%) ultimately died. Median overall survival (OS) for the total cohort after surgery was 57.2 months, 95% CI (29.7-84.6), 64.2 months (29.7-84.6), 61.9 months (28.1-95.6), and 31.7 months (1.5-61.8) for patients with HCC in non-cirrhotic livers, FLC and HCC in cirrhotic livers respectively.
CONCLUSIONS: Liver resection for HCC and FLC was safe with no mortality, but one-third of patients had associated postoperative morbidity. The high long-term recurrence rate remains a major obstacle in achieving better survival results after resection.
Keywords: surgery, liver, HCC, fibrolamellar carcinoma, complications, survival
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy in adults and is the fifth most common solid tumour worldwide with a variable prevalence based on underlying risk factors and geography.1,2 The incidence has risen over the past several decades and HCC is now the third leading cause of cancer-related deaths globally, after lung and stomach cancers, with a 5-year survival rate less than 20% and recurrence rates as high as 88%.3,4 More than 80% of global HCCs occur in sub-Saharan Africa (SSA) and Eastern Asia where the incidence ranges from 4.8 to 8.3 per 100 000 per year in different regions of SSA with the highest incidence in western and central Africa compared to less than 3 per 100 000 in Western countries.5 HCC has become a significant public health concern in SSA and is now the second leading cancer in men and the third for women, occurring in particular in young adults.3,6 Unfortunately only a small proportion of patients in SSA with HCC are treated with curative intent. Data are scarce, but studies consistently report that curative-intended treatment is pursued in less than 1% of patients in SSA with HCC.3,6 Fibrolamellar carcinoma (FLC) was until recently regarded as a variant of HCC occurring in young patients with a relatively good prognosis but is now recognised as a distinct clinical entity with consistent chimeric fusion protein (DNAJB1-PRKACA) expression by FLC tumours.7
The optimal treatment of HCC and FLC is influenced by the stage of the disease, the degree of liver impairment, and patient performance status.3,8 Currently, the therapeutic strategy is based on international guidelines and the Barcelona Clinic Liver Cancer (BCLC) staging system in which potentially curative treatment for early-stage HCC includes resection, transplantation or ablation.3 Surgical resection is the treatment of choice in patients without cirrhosis and in those with cirrhosis and well-preserved liver function.9 Despite advances in surgical techniques and perioperative care, hepatectomy remains a high-risk surgical procedure with complications occurring in up to 40% of resections. This adds a significant burden to individual patients by adversely affecting quality of life and increasing length of hospital stay, readmission rates, and healthcare costs. Recurrence despite curative-intent treatment occurs more often in patients with tumour multifocality, tumour size > 5 cm, macroscopic vascular or microscopic lymphovascular invasion, elevated alfa-fetoprotein (AFP) levels and impaired liver function.4 Previous publications from our unit have reported earlier data on resection for HCC and FLC.10-12 In this study, we assessed the perioperative outcome and survival of patients with HCC and FLC following curative liver resection at a tertiary referral centre in South Africa.
Patients and methods
Patients who underwent a primary liver resection for HCC or FLC in the Surgical Gastroenterology Unit at Groote Schuur Hospital or the University of Cape Town Private Academic Hospital between January 1990 and December 2021 were included in the study. All patients in the study were assessed preoperatively and treatment recommendations made in a multidisciplinary team meeting. Data were retrieved from an ethics approved prospective database and analysis included patient demographics, imaging results, surgical procedures performed, postoperative morbidity and mortality and histopathology results. Three groups were compared, namely HCC occurring in normal livers, HCC occurring in cirrhotic livers, and FLC. Liver resections were classified as minor (< 2 segments) or major (> 3 segments) according to definitions of the Brisbane 2000 classification and nomenclature.13 The expanded accordion severity grading system of surgical complications was used to assess morbidity.14 Postoperative bile leaks (BL) and post-hepatectomy liver failure (PHLF) were graded according to the respective International Study Group of Liver Surgery (ISGLS) definitions.15,16 Details of the surgical technique used have been published.11,12,17,18 Four-phase contrast-enhanced computed tomography (CE-CT) was used as primary imaging modality for tumour characterisation, assessment of biliovascular anatomy and surgical planning. In patients with a marginal future liver remnant (FLR), volumetry was performed. Magnetic resonance imaging (MRI) using gadopentetate dimeglumine (Magnevist®) or Gadoxetate disodium (Primovist®) (Bayer Schering Pharma, Berlin, Germany) was used for further characterisation if needed. Patients were followed up at 3 months and then every 6 months postoperatively, which included clinical assessment, screening liver ultrasound, liver biochemistry and tumour marker measurement.
Statistical analysis
Data were analysed using Stata version 11 (StataCorp. 2009. Stata: Release 11. Statistical Software. College Station, TX: StataCorp LP). Months of survival was calculated from the day of surgery. For bivariate analysis, the Pearson chi-square or Kruskal-Wallis tests were used for categorical variables, and the non-parametric Wilcoxon rank-sum test for numerical variables. Univariate and multivariate logistic regression models were used to evaluate the odds ratios (OR) and 95% confidence intervals of clinical variables (while excluding collinearity). All statistical tests were two-tailed and a p-value < 0.05 was considered statistically significant. Descriptive statistics as appropriate were used to present clinical and treatment characteristics and outcome of the study subjects. Ethical approval was obtained.
Results
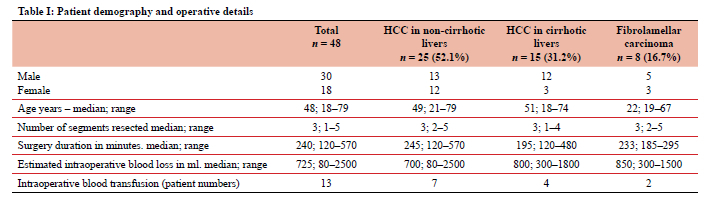
A total of 601 elective liver resections were performed during the inclusion period of which 48 (8%) were the primary operation for HCC or FLC. During the same period 529 patients with a confirmed diagnosis of HCC were assessed in the unit of whom 40 (7.6%) were resected. Twenty-five resections (52%) were performed for HCC in non-cirrhotic livers, 15 (31%) in patients with cirrhotic livers and 8 (17%) for FLC. Patient demographics and operative details are shown in Table I. The median age of the total cohort was 48 years (range 17-79), the majority of whom were men (62.5%). The viral status was known in 32 patients of whom 13 (27%) had chronic hepatitis B infection, eight in the non-cirrhotic and five in the cirrhotic groups, and one had hepatitis C. Thirty-eight (86.3%) of the 44 patients in whom complete information was available, were outside the BCLC criteria for resection (Stage 0 or A). Seven patients (15%) had preoperative radiological intervention, of whom six had trans-arterial embolisation (TAE) [bland embolisation n = 4; trans-arterial chemo-embolisation (TACE) n = 2] and one had a portal vein embolisation (PVE). Thirty-six (75%) major resections were performed. The median operating time was 240 min (range 120-570), median blood loss was 725 ml (range 80-2500) and intraoperative blood transfusion was required in 13 patients. Two of the 12 minor resections required a blood transfusion.
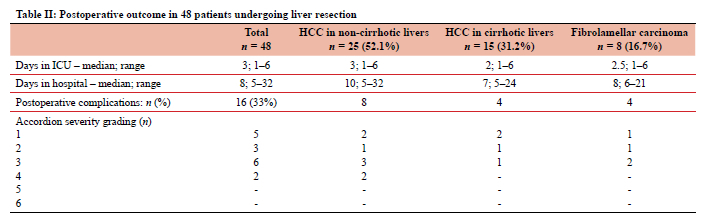
Postoperative outcomes are summarized in Table II. The median postoperative hospital stay for the whole cohort was eight days (range 5-32 days), nine days (range 6-32 days) in patients with complications compared to eight days (range 5-24 days) in patients without complications. Sixteen patients (33%) developed Accordion grade 1 to 4 complications. The highest complication rate (50%) occurred in resections for FLC. The most frequent complications were bile leaks (n = 5) and intra-abdominal collections (n = 4), followed by wound infection (n = 3), pneumonia (n = 2), and acute kidney injury (n = 2). Two of the patients with bile leaks were treated conservatively with spontaneous resolution, two underwent ERCP and stenting and one had percutaneous aspiration of a biloma. Two patients required re-exploration, one for bleeding and another for a subphrenic collection which was not amenable to ultrasound-guided percutaneous drainage. There was no in-hospital or 30-day mortality.
Review of the histology showed that 37 patients had R0 resections, two had R1 and four had R2 resections while the margin status was not recorded in six patients. Thirty-three patients (69%) developed recurrence of HCC following their initial resection of whom 29 ultimately died. The most common site of recurrence was the liver which occurred in 29 (60%) patients, five of whom also had extra-hepatic metastatic disease (lung, lymph nodes, omentum, abdominal wall and vertebrae). Four patients (8.3%) had only extra-hepatic metastatic recurrence. One patient had a repeat resection of a segment 4 recurrence one year after the initial right hemi-hepatectomy. A year later, she had percutaneous US-guided microwave ablation of a left liver recurrence and remains disease free five years later.
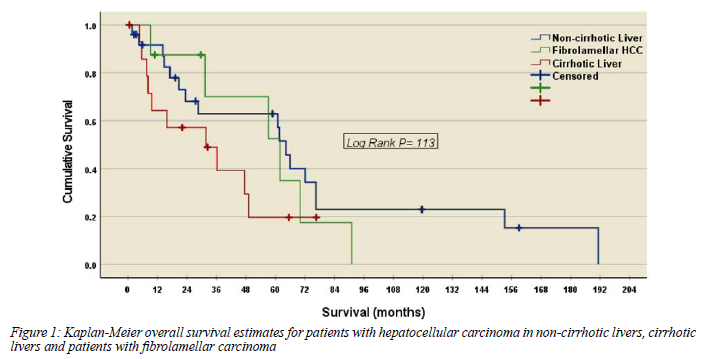
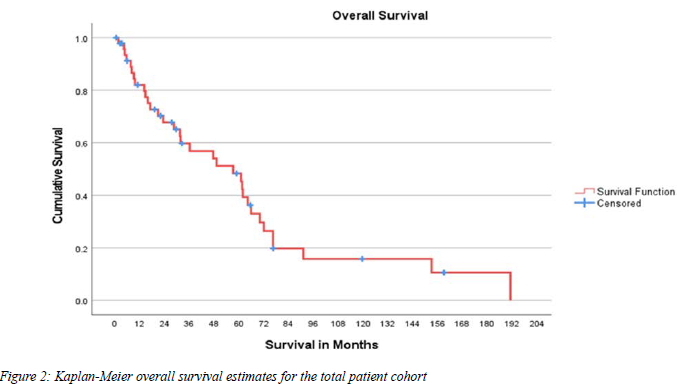
Thirty-three (69%) patients died (29 due to recurrence and four due to other causes) at a median of 952 days (range 51-5740). Median overall survival (OS) for the total cohort after surgery was 57.2 months, 95% CI (29.7-84.6). At three years the OS was 58%, and at 5 years 48% (Figures 1 and 2). Patients with a normal liver had a median OS of 64.2 months, 95% CI (29.7-84.6), for patients with FL HCC 61.9 months, 95% CI (28.1-95.6) and patients with a cirrhotic liver 31.7 months 95% CI ((1.5-61.8). There were no statistically significant differences in survival between the three groups, p = 0.113 (Figure 1).
Discussion
Hepatic resection is the most widely used method for curative intended treatment of HCC and FLC.3,6,8 In this retrospective cohort analysis of 40 liver resections performed for HCC and eight for FLC, there was no in-hospital or 30-day mortality, although one-third of patients had one or more postoperative complications. Major resections were performed in 75% of patients, a quarter of whom required an intraoperative blood transfusion. Median OS was best in patients who had HCC in non-cirrhotic livers, followed by patients with FLC and worst in patients with HCC in cirrhotic livers. Of salient interest in this series was that more than 60% of the resected HCCs were in patients with non-cirrhotic livers, likely due to the oncogenic pathway of chronic HBV infection causing HCC in younger patients, which differs from the predominantly cirrhosis pathway seen in low incidence regions.19,20 Most patients in SSA present late with advanced disease when cure is not possible and there is evidence that HCC in SSA follows a more aggressive course than elsewhere.21
Eight (16%) patients in this study had FLC, a tumour typically affecting a younger age group without underlying liver disease. These tumours display a unique histological pattern distinctly different from HCC and were designated with a unique WHO classification number in 2010.7,22 Several factors in FLC are associated with a poor prognosis including lymph node metastases, multiple tumours, metastatic disease at presentation, and vascular invasion.7
Despite advances in surgical technique and perioperative management which have reduced mortality and morbidity rates for HCC and FLC resection, one third of patients in our study had postoperative complications. In large published series from high-volume referral centres operative mortality rates of less than 3% are reported, however postoperative complication rates remain substantial and exceed 35%.23,24 Risk factors for postoperative morbidity include underlying liver dysfunction, a small liver remnant volume, major blood loss, perioperative transfusion and underlying comorbidities. In most series, a blood transfusion was necessary in less than 10% of resections.23,24
The 69% recurrence rate in this study is in line with previous reports of recurrence rates of up to 80%.4,8 Fourteen per cent of patients in whom complete data were available had a positive resection margin. Although those patients with positive resection margins are likely to account for disease recurrence, most recurrences were due to new tumours in the remaining liver. The 5-year OS following surgical resection within the Barcelona Clinic Liver Cancer (BCLC) criteria is around 70% compared to the three- and five-year rates in our study of 58% and 48% respectively. The results in terms of long-term survival, however, vary considerably among series because of the variation in resection criteria. Resection outside these criteria result in lower survival rates, but some patients will benefit from 5-year OS rates in excess of 50%.8,9,25 The majority of patients in this study fell outside the resection criteria of the BCLC staging system. In our cohort OS for FLC and HCC occurring in non-cirrhotic livers were similar, with a trend of worse survival in HCC occurring in cirrhotic livers. In our study HCC recurred in 33 patients, most commonly involving the liver, but five had associated extra-hepatic metastases. The most powerful predictors of recurrence are the presence of vascular invasion and/or additional tumour sites besides the primary lesion. Risk factors for poor survival after HCC recurrence include histologically poorly differentiated tumours, tumour multifocality, large size (> 5 cm), vascular invasion, high preoperative AFP levels, R1 resection, and the presence of impaired liver function.
Accurate data on outcome after HCC resection in SSA are scant. A literature search for HCC in PubMed, PubMed Central, Scopus Web of Science, AfricaWide and the Cochrane databases up to September 2022 identified only four papers that provided specific outcome after HCC resection apart from the published studies from our unit.10-12 Of these four, two were from Nigeria,26,27 and one each from Sudan28 and Uganda.29 The Muhammad study from Nigeria included 35 patients all of whom had ruptured HCCs and only 3 had a major liver resection.26 In the Enwezor study, five of 60 HCC patients underwent a resection with a 60% operative mortality and 0% survival at 26 months.27 The Harrison study from Uganda reported that only ten of 120 patients underwent resection with a 20% operative mortality rate.29 In the study from Sudan 44 patients with HCC had resections [major (> 3 liver segments) n = 8; moderate (1-3 segments) n = 4; minor < 1 segments n = 32)] with a major complication rate of 36.4% and a 30-day operative mortality of 9.1%.28
This study has several specific limitations. Despite the fact that the data generated are from a high volume tertiary academic centre, patient numbers are small and may reflect an inherent referral, selection and treatment bias. A further limitation is that our study included patients who underwent a liver resection over a period of 30 years, during which time changes in operative techniques and perioperative management may have affected postoperative morbidity rates, and data on Child-Pugh score and performance status were not available for all patients. A strength of this study is the prospective documentation of a robust dataset conducted in a single centre using uniform criteria in consecutive patients providing reliable granular data. Although this study may not completely reflect the population of patients treated at all tertiary referral centres, the analysis provided data not typically collected or available in large administrative databases. Because data about resections for HCC in SSA and reports on outcome after surgery are limited, this study provides important and very relevant information.
Conclusion
Hepatic resection is the treatment of choice in patients with resectable HCC. A major concern in this study is the low resection rate of 7.6% of all patients presenting with HCC. Resection was safe with no mortality, but despite applying optimal surgical techniques and perioperative care, one-third of patients had associated postoperative morbidity. The high long-term recurrence rate remains a major obstacle in achieving better survival results after liver resection.
Conflict of interest
The authors declare no conflict of interest.
Funding source
None.
Ethical approval
The study was approved by the University of Cape Town Human Research Ethics Committee HREC REF: 131/2022.
ORCID
Y Ziaei https://orcid/org/0009-0003-5107-3736
JEJ Krigehttps://orcid/org/0000-0002-7057-9156
EG Jonashttps://orcid/org/0000-0003-0123-256X
UK Kotze https://orcid/org/0000-0003-1405-474X
MM Bemon https://orcid/org/0000-0002-7967-8548
JC Kloppershttps://orcid/org/0000-0003-2438-6879
S Sobnachhttps://orcid/org/0000-0002-4456-2115
REFERENCES
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209-49. https://doi.org/10.3322/caac.21660. [ Links ]
2. McGlynn KA, Petrick JL, London WT. Global epidemiology of hepatocellular carcinoma: an emphasis on demographic and regional variability. Clin Liver Dis. 2015;19:223-38. https://doi.org/10.1016/j.cld.2015.01.001. [ Links ]
3. Jonas E, Bernon M, Robertson B, et al. Treatment of hepatocellular carcinoma in sub-Saharan Africa: challenges and solutions. Lancet Gastroenterol Hepatol. 2022;7:1049-60. https://doi.org/10.1016/S2468-1253(22)00042-5. [ Links ]
4. Papaconstantinou D, Tsilimigras DI, Pawlik TM. Recurrent hepatocellular carcinoma: patterns, detection, staging and treatment. J Hepatocell Carcinoma. 2022;9:947-57. https://doi.org/10.2147/JHC.S342266. [ Links ]
5. Kedar Mukthinuthalapati VP, Sewram V, Ndlovu N, et al. Hepatocellular carcinoma in sub-Saharan Africa. JCO Glob Oncol. 2021;7:756-66. https://doi.org/10.1200/GO.20.00425. [ Links ]
6. Spearman CW, Dusheiko G, Jonas E, et al. Hepatocellular carcinoma: measures to improve the outlook in sub-Saharan Africa. Lancet Gastroenterol Hepatol. 2022;7:1036-48. https://doi.org/10.1016/S2468-1253(22)00041-3. [ Links ]
7. Aziz H, Brown ZJ, Madani SP, Kamel IR, Pawlik TM. Fibrolamellar hepatocellular carcinoma: comprehensive review of diagnosis, imaging, and management. J Am Coll Surg. 2023;236:399-410. https://doi.org/10.1097XCS.0000000000000476. [ Links ]
8. Vogel A, Meyer T, Sapisochin G, Salem R, Saborowski A. Hepatocellular carcinoma. Lancet. 2022;400:1345-62. https://doi.org/10.1016/S0140-6736(22)01200-4. [ Links ]
9. Villanueva A. Hepatocellular carcinoma. N Engl J Med. 2019;380:1450-62. https://doi.org/10.1056/NEJMra1713263. [ Links ]
10. Lemmer ER, Krige JE, Hall PM, et al. Surgical resection for hepatocellular carcinoma in Cape Town: a clinical and histopathological study. S Afr Med J. 1998;88(12):1575-80. [ Links ]
11. Bhaijee F, Krige JE, Locketz ML, Kew MC. Liver resection for non-cirrhotic hepatocellular carcinoma in South African patients. S Afr J Surg. 2011;49(2):68-74. [ Links ]
12. Bhaijee F, Locketz ML, Krige JE. Fibrolamellar hepatocellular carcinoma at a tertiary centre in South Africa: a case series. S Afr J Surg. 2009;47(4):108-11. [ Links ]
13. Terminology Committee of the International Hepato-Pancreato-Biliary Association. The IHPBA Brisbane 2000 terminology of liver anatomy and resections. HPB Surg. 2000;2:333-9. https://doi.org/10.1016/S1365-182X(17)30755-4. [ Links ]
14. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205-13. https://doi.org/10.1097/01.sla.0000133083.54934.ae. [ Links ]
15. Koch M, Garden OJ, Padbury R, et al. Bile leakage after hepatobiliary and pancreatic surgery: A definition and grading of severity by the International Study Group of Liver Surgery. Surgery. 2011;149:680-8. https://doi.org/10.1016/j.surg.2010.12.002. [ Links ]
16. Rahbari NN, Garden OJ, Padbury R, et al. Post-hepatectomy liver failure: A definition and grading by the International Study Group of Liver Surgery (ISGLS). Surgery. 2011;149:713-24. https://doi.org/10.1016/j.surg.2010.10.001. [ Links ]
17. Terblanche J, Krige JE, Bornman PC. Simplified hepatic resection with the use of prolonged vascular inflow occlusion. Arch Surg. 1991;126(3):298-301. https://doi.org/10.1001/archsurg.1991.01410270038006. [ Links ]
18. Krige JE, Thomson SR, Bornman PC. Choosing the optimal tools and techniques for parenchymal liver transection. S Afr J Surg. 2013;51(1):2-4. [ Links ]
19. Spearman CW, Afihene M, Ally R, et al. Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets. Lancet Gastroenterol Hepatol. 2017;2:900-9. https://doi.org/10.1016/S2468-1253(17)30295-9. [ Links ]
20. Kew MC. Hepatocellular carcinoma in Africa. In: Malignant liver tumours - current and emerging therapies, 2nd ed. Clavien PA, editor. Boston: Jones and Bartlett; 2003. p. 439-48. [ Links ]
21. Kew MC. Hepatocellular carcinoma in African Blacks: Recent progress in aetiology and pathogenesis. World J Hepatol. 2010;2:65-73. https://doi.org/10.4254/wjh.v2.i2.65. [ Links ]
22. Kew MC. Epidemiology of hepatocellular carcinoma in sub-Saharan Africa. Ann Hepatol. 2013;12:173-82. https://doi.org/10.1016/S1665-2681(19)31354-7. [ Links ]
23. Li J, Huang L, Yan J, Qiu M, Yan Y. Liver resection for hepatocellular carcinoma: personal experiences in a series of 1330 consecutive cases in China. ANZ J Surg. 2018;88(10):E713-E717. https://doi.org/10.1111/ans.14381. [ Links ]
24. Capussotti L, Muratore A, Amisano M, et al. Liver resection for hepatocellular carcinoma on cirrhosis: analysis of mortality, morbidity and survival - a European single centre experience. EJSO. 2005;31:986-93. https://doi.org/10.1016/j.ejso.2005.04.002. [ Links ]
25. Guglielmi A, Ruzzenente A, Conci S, et al. Hepatocellular carcinoma: Surgical perspectives beyond the Barcelona clinic liver cancer recommendations. World J Gastroenterol. 2014;20(24):7525-33. https://doi.org/10.3748/wjg.v20.i24.7525. [ Links ]
26. Muhammad I, Mabogunje O. Spontaneous rupture of primary hepatocellular carcinoma in Zaria, Nigeria. J R Coll Surg Edinb. 1991;36(2):117-20. [ Links ]
27. Enwezor CJ. Sixty cases of primary hepatocellular carcinoma in one year: a preliminary appraisal. Int Surg. 1992;77(4):277-9. [ Links ]
28. Elsanousi OM, Mohamed MA, Salim FH, Adam EA. Selective devascularisation treatment for large hepatocellular carcinoma: Stage 2A IDEAL prospective case series. Int J Surg. 2019;68:134-41. https://doi.org/10.1016/jijsu.2019.06.014. [ Links ]
29. Harrison NW, Dhru D, Primack A, Bhana D, Kyalwazi SK. The surgical management of primary hepatocellular carcinoma in Uganda. Br J Surg. 1973;60(7):565-9. https://doi.org/10.1002/bjs.1800600719. [ Links ]
 Correspondence:
Correspondence:
email: jej.krige@uct.ac.za

{kind=link}
{kind=link}
{kind=link}
{kind=link}