










Services on Demand
Journal

Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Dental Journal
On-line version ISSN 0375-1562Print version ISSN 0011-8516
S. Afr. dent. j. vol.80 n.7 Johannesburg Aug. 2025
https://doi.org/10.17159/sadj.v80i07.21793
CASE REPORT
A 13-Year Follow-Up of a full mouth rehabilitation using a fixed PFM bridge opposing an acrylic veneered implant supported hybrid prosthesis
SK MpungoseI; AK SinghII; LM SykesIII
IBChD, MChD (UWC), Head Clinical Unit, Department of Prosthodontics, School of Dentistry, Faculty of Health Sciences, University of Pretoria, Oral and Dental Hospital, Prinshof Campus, Riviera Pretoria, South Africa, 0002. ORCID: https://orcid.org/0000-0003-2177-7540
IIBChD, PDD, MChD (UWC), Private Practice, Suite 114, The Madison Medical Cnr Umhlanga Ridge Boulevard and Aurora Drive, Umhlanga Ridge, KZN, South Africa
IIIBSc, BDS, MDent, Dip Research Ethics (IRENSA), Dip Forensic Path, Dip ESMEA, FCD (Pros) Head of Department of Prosthodontics, Faculty of Health Sciences, University of Pretoria, Oral and Dental Hospital, Prinshof Campus, Riviera, South Africa, 0002 https://orcid.org/0000-0002-2002-6238
ABSTRACT
This case report presents a 13-year follow-up of a patient rehabilitated with maxillary and mandibular prostheses made of dissimilar materials to address the differing aesthetic and functional demands in each arch. In the maxilla a fixed telescopic crown-retained porcelain fused to metal (PFM) prosthesis was fabricated which opposed a mandibular implant-supported acrylic veneered hybrid prosthesis. A 51-year-old female initially presented with functional and aesthetic concerns as a result of a fractured maxillary provisional restoration spanning from the 13-23, pain on the 13, and failing crown and bridgework on her remaining maxillary teeth. This was opposed by an acrylic provisional immediately-loaded implant supported hybrid prosthesis that had been placed in 2009. She was rehabilitated using telescopic-crowns supporting a flxed porcelain fused to metal (PFM) bridge, and an acrylic veneered implant supported prostheses. In the 13 years of follow-up, both prostheses have shown excellent longevity with the maxillary prosthesis having had only one incident of de-cementation, and the prosthesis needing repair/replacement of the veneering material and screw-access-hole closure on two occasions in 2018 and 2022. This report highlights the efficacy and long term success of using prostheses made with different materials and techniques in each arch in complex rehabilitation cases.
INTRODUCTION
Telescopic crown-retained prostheses and implant-supported hybrid prostheses are established modalities for rehabilitating patients with compromised dentitions The choice between porcelain and acrylic veneering materials involves trade-offs between aesthetics, durability, repairability and maintenance.2 This case highlights the long-term outcomes of a maxillary porcelain fused to metal prosthesis opposing a mandibular acrylic-resin veneered hybrid prosthesis supported by five implants. It emphasises the material-specific challenges and solutions encountered in each.
Literature Review
Telescopic crowns (double crowns/crown and sleeve copings/konuskrone) are a well-established prosthodontic solution for patients with compromised dentitions allowing for the maintenance of teeth and their periodontal ligaments (PDL) enhancing proprioception, as well as bone preservation and the potential for future modifications when neccessary.1 They were initially introduced as retainers for removable partial dentures, and have since been used in fixed restorations as well. Despite their long historical use, published follow-up data on their durability remains limited. Telescopic crowns are indicated for patients with a compromised periodontium, caries, or trauma requiring splinting of mobile abutment teeth.2 They allow redistribution of occlusal forces, help preserve compromised dentition, and facilitate hygiene through removable components.3 Langer and Langer (2000) emphasised their role in rehabilitating non-parallel abutment teeth and in limiting alveolar bone loss.4 They are however contraindicated in cases where there is poor oral hygiene, insufficient abutment support, and high aesthetic demands due to the added bulkiness.5 Breitman et al. (2012) also confirmed the concerns of unaesthetic outcomes in patients who have high smile lines as well as the increased costs as disadvantages.6 Further reported complications include cement failure and marginal and/or recurrent caries in patients with poor oral hygiene. Despite these limitations, studies report 85-95% 5-year survival rates for telescopic crown-retained prostheses.7
Implant-supported acrylic veneered hybrid prostheses are indicated for edentulous patients requiring cost-effective, retrievable solutions.3 Studies report survival rates of 9095% over 5-10 years for prostheses supported by 4-6 implants.4 The use of five implants is believed to be ideal as its argued this will distribute occlusal loads more effectively, thus reducing cantilever strain and peri-implant bone loss.5 Acrylic veneering, is prone to wear of approximately of 2-3 mm over 10 years, depending on factors such as occlusion, diet, and the material in the opposing arch.6 This wear may necessitate periodic veneer replacement, typically every 5-7 years, but the process is relatively cheap and easy when compared to porcelain.7,10
Acrylic, though less aesthetic than porcelain, also acts as a good shock absorber of masticatory forces which helps protect underlying frameworks and implants.9 Porcelain prostheses on the other hand, provide superior aesthetics and wear resistance but are brittle and prone to fracture under parafunctional loads.8 In patients requiring full mouth rehabilitation, the use of a combination of porcelain in the maxilla, and acrylic resin in the mandible can address both their aesthetic and biomechanical functional needs.11
Case Report
In 2013, a 51-year-old female patient presented with a main complaint of a fractured maxillary provisional bridge spanning from 13-23, pain from the 13, and a worn mandibular implant retained provisional prosthesis (figure 1). The implant-retained prosthesis had been placed in 2009, but no definitive prosthesis was ever made. The patient was adamant that she did not want to lose any more teeth, and neither did she want to wear a removable appliance.

Key Clinical Findings:
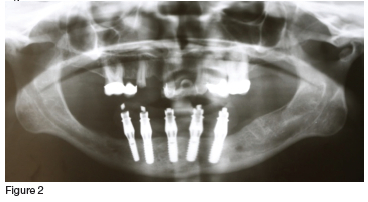
The maxilla had six remaining teeth, pain from the fractured 13 abutment tooth and grade 2 mobility of the 11 (which was expected as it had been serving as a pier abutment tooth in the provisional prosthesis (figure 3). The mandible had a severely worn acrylic hybrid prosthesis retained by five implants (figures 1 & 2).

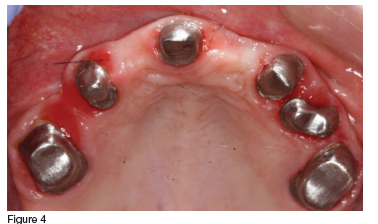
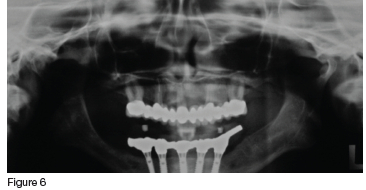
In consultation with the patient, it was decided that, although compromised, the clinician would try to save all the maxillary teeth. Initial treatment included endodontic therapy to address the pulpitis and pain in the fractured 13, followed by crown preparations on all of the remaining maxillary teeth. These were then used as abutments for the definitive prosthesis, which was a telescopic crown-retained porcelain fused to metal fixed partial denture (figures 4, 5 & 6). The mandible was restored with an acrylic veneered implant supported hybrid prosthesis (figure 7).


Follow up
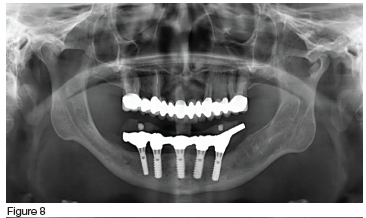
In the maxilla, the porcelain prosthesis remained intact with no fractures for 13 years (figures 8 & 9), however there was a single event of cement failure (figure 10) at year 12 in 2022. This event was easily managed through sandblasting the intaglio surface of the FPD and re-cementing it. The mandibular acrylic prosthesis also remained intact and functional for over 13 years, but did exhibit ±2.5 mm occlusal wear during this time. Additionally at year seven (2019) and year ten (2022) it had two separate events requiring replacement of the screw access hole closure material which had been lost (figures 9 & 11). No implant or framework complications were observed, nor was there any noticeable bone loss in either the maxilla or mandible (figure 8). The patient reported high satisfaction with both her aesthetics and chewing efficiency.



Discussion
The 13-year success of the maxillary telescopic crown-retained PFM prosthesis (for aesthetics) and mandibular acrylic veneered hybrid prosthesis (for function) aligns with biomechanical principles. The mandibular prosthesis exhibited moderate occlusal wear (±2.5 mm over 13 years), necessitating two minor repairs. It may be argued that there is a need for the complete replacement of the veneering material, but in this instance, the patient was not keen to be without her prosthesis, and thus the wear was managed with minimal intervention, and the prosthesis was repaired and not replaced. The wear was anticipated as it aligns with studies showing acrylic's susceptibility to wear compared to porcelain, with average wear rates of 0.2-0.3 mm annually under functional loading.5 The rate may have been accelerated in her case due to the harder porcelain material in the opposing arch. Acrylic's reduced wear resistance is a well-documented trade-off for its shock-absorbing properties, which protect implants from overload and potential peri-implant bone loss.3,6 Notably, a four or five-implant support system distributed forces effectively, preventing framework fractures or implant mobility despite wear, consistent with protocols advocating >4 implants for cantilevered prostheses.2,4 The loss of screw access hole closure material in the fourth quadrant was a minor complication, and has also been reported in the literature to occur in 15-20% of screw-retained hybrid prostheses over time.5,8 These issues are attributed to cyclic masticatory forces and do not indicate prosthetic failure but rather routine maintenance needs.7
The maxillary telescopic crown-retained prosthesis has remained intact and in good condition for over a decade without fractures or caries recurrence. This underscores the durability of porcelain in splinted systems, its wear resistance and maintenance off aesthetic requirements.9 However, one incident of debonding occurred at year 7, resolved by recementation. Cement failure in telescopic systems is reported in 5-10% of cases, often due to parafunctional habits or suboptimal cement selection, and does not compromise long-term success if promptly addressed.10,11
The combination of a maxillary porcelain prosthesis (prioritising aesthetics and rigidity) and a mandibular acrylic hybrid prosthesis (prioritising shock absorption and protective functions as well as reparability) reflects evidence-based principles for arch-specific rehabilitation.3,12
While acrylic requires periodic veneer replacements, its ease of repair and cost-effectiveness make it ideal for the mandible, where functional demands outweigh aesthetic concerns.5,13 Key clinical implications are that patients should be informed of the need for acrylic veneering material replacement every 5-7 years, and plan to have this carried out in order to maintain their occlusal relations and prosthesis efficiency.6 The screw access holes composite material may require replacements which can be carried out during the advocated follow-up hygiene and maintenance appointments.8 Cement selection is also important, resilient temporary cements (e.g., zinc oxide eugenol) are recommended for telescopic crowns to provide for retention and retrievability.11
Conclusion
This case illustrates that moderate acrylic wear and minor screw access hole complications are inherent to hybrid prostheses but do not equate to failure. Similarly, a single debonding event in the maxilla reflects routine maintenance needs rather than prosthetic inadequacy. The favourable 13-year outcome validates the strategic decision to use dissimilar materials in each arch to address biomechanical and aesthetic demands in complex mouth rehabilitations.
Patient Consent
Informed consent was obtained for use of illustrations for presentation and publication purposes.
Conflict of Interest:
None declared.
REFERENCES
1. Langer Y Langer A. Telescopic retainers for removable dentures. J Prosthet Dent. 2000;83(4):439-43. [ Links ]
2. Breitman N, Nakamura S, Freedman M. Telescopic retainers: A modern approach to an old concept. J Prosthodont. 2012;21(8):650-5. [ Links ]
3. Gallucci GO, et al. Five-year results of fixed implant-supported rehabilitations. Clin Oral Impl Res. 2009;20(6):601-7. [ Links ]
4. Carlsson GE. Dental occlusion: Modern concepts in implant prosthodontics. Odontology. 2009;97(1):8-17. [ Links ]
5. Jemt T. Failures and complications in implant prosthodontics. Int J Oral Maxillofac Implants. 1991;6(3):270-6. [ Links ]
6. Al-Fadda SA, et al. CAD/CAM vs. conventional frameworks. Int J Prosthodont. 2007;21(5):575-80. [ Links ]
7. Kapos T, et al. CAD/CAM in implant dentistry. Int J Oral Maxillofac Implants. 2009;24:110-7. [ Links ]
8. Sahin S, Cehreli MC. Passive fit in implant prosthodontics. J Dent. 2001;29(4):257-64. [ Links ]
 Correspondence:
Correspondence:
Dr SK. Mpungose
Email: sandile.mpungose@up.ac.za / Tel: 012 319 2388
