










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkCommunitas
On-line version ISSN 2415-0525
Print version ISSN 1023-0556
Communitas (Bloemfontein. Online) vol.26 Bloemfontein 2021
http://dx.doi.org/10.18820/24150525/comm.v26.6
ARTICLES
Covid-19 information gaps among disadvantaged communities: the case of the deaf and limited English proficiency communities in Zimbabwe
Paul SvongoroI; Tawanda MatendeII
IFaculty of Arts and Humanities, University of the Western Cape, Cape Town, South Africa Email: 4080786@myuwc.ac.za; ORCID: https://orcid.org/0000-0002-3186-339X
IIDepartment of Linguistics, Faculty of Arts, University of Zimbabwe, Harare, Zimbabwe Email: matendet@arts.uz.ac.zw; ORCID: https://orcid.org/0000-0003-2214-0760
ABSTRACT
Worldwide public health authorities are taking action to contain Covid-19. While the bulk of research on the pandemic focuses on understanding the spread and seeking a cure for the virus from a virology perspective, research of the same magnitude should also focus on the risks of the pandemic for society, particularly among disadvantaged groups. This study adopted a community-centred approach to information and health rights and utilised the case study approach to investigate the quality and access to Covid-19 information, care and treatment by the Limited English Proficiency (LEP) and the Deaf communities in Zimbabwe. More than 60% of Covid-19 messages communicated in Zimbabwe's mainstream media do not cater for the needs of these disadvantaged groups. Brochures, videos and infographics, for instance, appear in English, yet there is a significant LEP population in Zimbabwe. As regards the Deaf community, videos, conversations and interviews with health specialists, which rarely appear in mainstream public media, include Zimbabwean Sign Language interpretation. In this case, the choice of language and medium used to communicate vital Covid-19 messages in mainstream public media may pose language barriers to effective and equitable health information for these vulnerable groups. What this reality hints at is that public communication that does not discriminate is a necessity to allow all members of the community to fight the spread of Covid-19 and hence, reduce its potential risks.
Keywords: health communication; science communication; development communication; Covid-19 information; risk communication; disadvantaged communities; Deaf community; Limited English Proficiency
INTRODUCTION
Worldwide public health authorities are taking action to contain the spread of Covid-19. While the outbreak has prompted clinical trials of antibodies, vaccines and treatments to combat the spread of the virus, researchers from the social sciences note the paucity of research that adopts a community perspective about the virus. This study adopts a community-centred approach to information and health rights and utilises the case study approach to investigate the quality of and access to Covid-19 information, care and treatment by persons with Limited English Proficiency (LEP) and the Deaf communities in Zimbabwe.
While efforts have been made to share information with all people, there is limited and in some cases, no information being produced in accessible formats for persons with disabilities and the disadvantaged such as the Deaf and those with LEP. This is in contradiction of, for instance, Article 11 of the Convention on the Rights of Persons with Disabilities (CRPD) that calls on all states to take "all necessary measures to ensure the protection and safety of persons with disabilities in situations of risk". In the case of Zimbabwe, brochures, videos and infographics, for instance, appear in English yet there is a significant LEP population in the country. Even for citizens with good English proficiency, the technicality of medical language pertaining to Covid-19 may pose challenges to communication and hence, access to information critical for surviving the pandemic. As regards the Deaf community, videos, conversations and interviews with health specialists, which appear in mainstream public media, rarely include Zimbabwean Sign Language (ZSL) interpretation. In this case, the choice of language and medium used to communicate vital Covid-19 messages in mainstream public media may pose language barriers to effective and equitable health information for these vulnerable groups.
In view of this, the researchers realised the urgent need for research that delves into the nature of the problem with a view to finding possible ways of enhancing the provision of accessible health information. In so doing, the researchers hope for an opportunity to contribute to policy regarding access and equity in health care, while at the same time, strengthening Zimbabwe's response to this and other public health crises.
Kusters et al. (2017: 123) note that many authors use "deaf" for individuals and "Deaf" for sociocultural entities like "the Deaf community" as well as established theoretical concepts, such as "Deaf culture" (cf. Haualand 2012: 19). They argue that the convention "deaf" does not mean "oral/medical" but rather biologically corporally deaf. The d/Deaf distinction creates or perpetuates a dichotomy between deaf and Deaf people (even when trying to be inclusive by writing "d/Deaf") and has caused practices and experiences of exclusion (Kusters et al. 2017: 98). In this study the term "deaf" is used as a term to describe deaf people as well as those who are hard of hearing, while "Deaf" is use for sociocultural entities and theoretical concepts.
The Deaf community in Zimbabwe remained relegated to the periphery in as far as access to Covid-19 information is concerned. Efforts to make sure information reaches this community are still minimal across the nation. Deaf people are exposed to serious risk because information on Covid-19 is not being presented to them in accessible formats. Covid-19 poses unique challenges to the Deaf community in Zimbabwe, many of whom rely on visual cues such as lip-reading and sign language (ZSL), which leans heavily on facial cues and expressions for communication.
RESEARCH PROBLEM
Significant gaps and challenges still exist about Covid-19; these gaps are especially evident in resource-limited settings and the challenges impact heavily on disadvantaged groups in society such as the Deaf and those with LEP. Evidence suggests that the likelihood of pandemics has increased over the past century because of increased global travel and integration, urbanisation, changes in land use, and greater exploitation of the natural environment. This implies that communicative efforts, especially those aimed at disadvantaged groups, should also be improved.
Most data regarding the risks, impacts, benefits and cost of mitigation measures against pandemics that are generally reported in the literature come from high-income countries, leading to biases and potential blind spots regarding the risks, consequences and optimal interventions specific to low-income countries such as Zimbabwe. Against this background, this study seeks to explore how access to information by disadvantaged groups in a low-income country like Zimbabwe impacts on the Deaf and the LEP community.
Since the outbreak of Covid-19 towards the end of 2019 in Wuhan, China, the World Health Organisation (WHO) has been adding the latest international multilingual scientific findings and knowledge on Covid-19 to its Covid-19 database. The global literature cited on this database is updated daily (Monday through Friday) from searches of bibliographic databases, hand searching, and the addition of other expert-referred scientific articles. This database represents a comprehensive multilingual source of current literature on the topic. While it may not be exhaustive, new research is added regularly. However, most of this global literature in the WHO Covid-19 database is drawn from medical schools and laboratories at universities, medical journals and research institutes around the developed world. The literature is generally based on clinical trials and is useful for understanding the spread and prevention of Covid-19. However, to understand the disease holistically, there is need to complement this effort by embarking on research that takes a community-centred approach to the understanding of the impact of Covid-19 on communities, particularly the marginalised in society.
SIGNIFICANCE OF THE STUDY
Access to information at the right time, in the right language, and of the right quality is critical in the fight against the social and economic impact of Covid-19. However, when disadvantaged groups are deprived of essential Covid-19 information, they are left at an increased risk of contracting the disease and exponentially spreading the disease; thereby, increasing the burden on already underfunded health facilities. Persons with LEP and the Deaf remain susceptible to contracting the disease because vital information about Covid-19 shared in mainstream media is often inaccessible to them. This presents a challenge in preventing the spread of the disease and further complicates governments' efforts at re-opening economies.
The study seeks to contribute to the understanding of social protection for disadvantaged groups, as this ultimately reduces financial burdens on the entire economy and enhances the quality of healthcare for all citizens. The study also contributes to the debate around issues regarding access and barriers to equitable information and healthcare. The researchers hope that these issues could be addressed by further interrogating policy and training for media and healthcare personnel to enable governments to effectively and systemically respond to members of the Deaf and LEP community.
RESEARCH OBJECTIVES
The study seeks to:
♦ explore the perceptions of the LED and the Deaf community on the quality and access to Covid-19 information, care and treatment;
♦ explore the factors that limit or increase access to Covid-19 information by the LEP and Deaf community in Zimbabwe;
♦ explain how these factors limit or increase access to general Covid-19 information, care and treatment by the LEP and Deaf community, and their ability to understand and comply with Covid-19 prevention and treatment options; and
♦ propose policy interventions to address information challenges faced by members of the LEP and Deaf community.
ACCESS TO COVID-19 INFORMATION AND RISKS AMONG DISADVANTAGED GROUPS
According to UNESCO, persons with disabilities remain an invisible population group, and this accentuates their vulnerability and marginalisation in times of emergency. Literature on the Spanish flu pandemic of 1918 reveals that people with poor literacy were much more likely to transmit the disease, and to die. During the H1N1 swine flu outbreak, Chinese people with limited English proficiency living in King County, Washington were reportedly unlikely to obtain information from the public health system. Similarly, Spanish speakers were found to be at the greatest risk of exposure to H1N1 during this outbreak. What these few examples suggest is that people with limited English proficiency do not receive adequate health information, which ultimately exacerbates health disparities.
For Deaf communities around the world, communication barriers present a profound challenge to accessing critical health and safety information regarding the novel coronavirus pandemic. According to the World Federation of the Deaf, about 70 million people with auditory disabilities worldwide use more than 300 different sign languages. Deaf communities are further marginalised from public life because they do not have access to educational opportunities, which results in low literacy. In the Covid-19 context, information on the pandemic is often not available in sign language. The increased use of protective face masks because of Covid-19 compounds these communication barriers because masks block visual cues, including facial expressions, lip reading and emotions, all of which are critical for Deaf and hard-of-hearing people to communicate. In view of the above examples about how pandemics impact disadvantaged groups in society, it is imperative that people around the world learn from past mistakes. While the researchers do not make an absolute claim that people with LEP and the Deaf are more likely to contract the virus, it is imperative to ensure that this group is not disproportionately affected because of lack of access to Covid-19 information that is communicated to them in languages that exclude and hence, continue to marginalise them.
METHODOLOGY
The project adopted a community-centred approach to information and health rights and it was conducted during a period of approximately four months during the pandemic. The project applied a qualitative methodology to collect data from multiple sources. First, data was collected from both print and electronic media covering a broad spectrum of public and private media. Such data included news bulletins, government and ministerial Covid-19 addresses and updates, coronavirus infographics, leaflets, notices and brochures. Second, data was collected through semi-structured and in-depth interviews with Deaf participants on their experiences and perceptions regarding access to Covid-19 information, which appeared in both print and electronic media, and how access to information affected their health-seeking behaviour.
The data was analysed using the Socio-Pragmatic Model, which is located in the broad field of pragmatics. While no concise definition of pragmatics can be agreed upon, Agbara and Omole (2014) view pragmatics as a field of linguistic study, which deals with how a speaker conveys meaning from his/her utterances and how listeners are able to interpret speaker meaning from those utterances. Although this definition is clear about the focus of pragmatics, for the purposes of this study the researchers adopted the view shared by Crystal (2003) and Mey (2001) about pragmatics. For both Crystal (2003) and Mey (2001), pragmatics deals with the language options of interlocutors and the consequences they have on respective listeners. One of the implications is that the way speakers use language amidst a number of constraints (context, topic, speech acts, appropriateness of the language and medium used) in any communicative situation may result in misinterpretation, and hence, lack of understanding of the speaker's intended message. The second implication is that a lack of understanding of the speaker's message may have dire consequences, particularly when dealing with health matters.
Socio-pragmatics describes the ways in which pragmatic meanings are influenced by the "specific local conditions of language use" (Leech 1983: 10). This aspect makes the model relevant to the analysis of data used in this study. In the context of this study, the specific local conditions of language use, which are vital parts of any discourse, can be viewed in terms of the gender, age, social class/status (e.g. the Deaf and LEP communities), and race of the interlocutors. In this regard, Leech's (1983) view is extended by LoCastro (2012: 185), who argues, "Meaning, structure and the use of language are socially and culturally relative". Thus, the Socio-Pragmatic Model concerns itself with the "social rules of speaking, those expectations about interactional discourse held by members of a speech community as appropriate and normal behaviour" (LoCastro 2012: 187). The Socio-Pragmatic Model views communication as social action (e.g. warning or informing about coronavirus), and interaction, and borrows from a variety of schools of thought listed by Ralarala and Rodrigues (2019).
SYNOPSIS OF DATA
During the period of four months, 22 electronic and print messages about Covid-19 appeared in mainstream government-owned and private media. These messages comprised the following:
♦ Sixteen were Covid-19 brochures, infographics, leaflets, notices, Covid-19 updates and media statements collected from The Herald, Kwayedza and The Sunday Mail newspapers, which are government-owned news outlets owned by Zimpapers. These messages were meant for members of the public in Zimbabwe as part of the government's Covid-19 information dissemination efforts;
♦ Twelve were news bulletins, national addresses and updates on Covid-19, videos and infomercials collected from Zimbabwe Television (ZTV), a television station owned by the state entity, the Zimbabwe Broadcasting Corporation (ZBC); and
♦ Eighteen were Covid-19 messages in the form of brochures, infographics, leaflets, notices, Covid-19 updates and media statements collected from two privately-owned newspapers namely Daily News, owned by Associated Newspapers Zimbabwe (ANZ), and Newsday, owned by Alpha Media Holdings (AMH).
Data was collected from 12 Deaf participants about their experiences and perceptions regarding access to Covid-19 information that appeared in both print and electronic media. These interviews also assisted the researchers to elicit information from the participants about how access to information affected their healthcare-seeking behaviour. The views obtained from these interviews were then analysed according to recurring themes.
THE DEAF AND ACCESS TO COVID-19 INFORMATION
Access is a broad topic that is regularly discussed within the Deaf community. It involves access to communication, information, education and culture, as well as access to services, including health services. Understanding of ill health as well as language and communication barriers have been linked to challenging health care access in culturally and linguistically diverse populations (Komaric et al. 2012). Access to health care affects the health of deaf people and a call for action to provide better access to health services has been highlighted (Emond et al. 2015). There are no reliable estimates on the number of deaf people in Zimbabwe. According to Ndlovu (2016), there are over 200 000 persons who are deaf in Zimbabwe with most of them migrating to Harare in search of work opportunities. Many deaf people use sign language as their main form of communication. Fromkin et al. (2003: 3) state, "Sign language is established in linguistics and it is a fully and completely human language that meets every criterion that one can apply to describe language".
The researchers were spurred to conduct this research because of the common perception that deaf people are deprived of their right to access information about Covid-19 through exclusion of Zimbabwean Sign Language (ZSL) on various media platforms. In 2020, persons with disabilities sued the Zimbabwean government for failing to use accessible formats in disseminating information concerning Covid-19 (Zimeye 2020). The Executive Director and Trustee at the Centre for Disability and Development noted that the Zimbabwean President's Covid-19 lockdown national addresses on ZTV (and also broadcast on national radio stations), and Covid-19 updates by both the Ministry of Information, Publicity and Broadcasting Services and that of Health and Child Care broadcast on ZTV related to Covid-19 failed to accommodate the needs of the Deaf community.
The data analysis included a focus on the format in which the messages were presented, namely the language(s) the messages were broadcast in - whether they were oral messages, written messages, pictorial messages or messages in Zimbabwean Sign Language. The focus was further on whether the messages provided inclusive or exclusive Covid-19 messages. Finally, the focus was on whether the message sources made an effort to reduce barriers in communication by ensuring the messages were broadcast in formats accessible to the generality of the Zimbabwean population regardless of age, gender, social status and disability.
From the analysis of the Covid-19 messages shown on ZTV, it is clear that the challenges faced by the Deaf community in Zimbabwe raised more questions than answers. The platforms used to communicate Covid-19 information are not accessible to persons with disability, especially the Deaf community. Table 1 summarises the various types of Covid-19 messages, the messages communicated, the format in which the messages occurred, and how these issues affected access to Covid-19 information by the Deaf community.
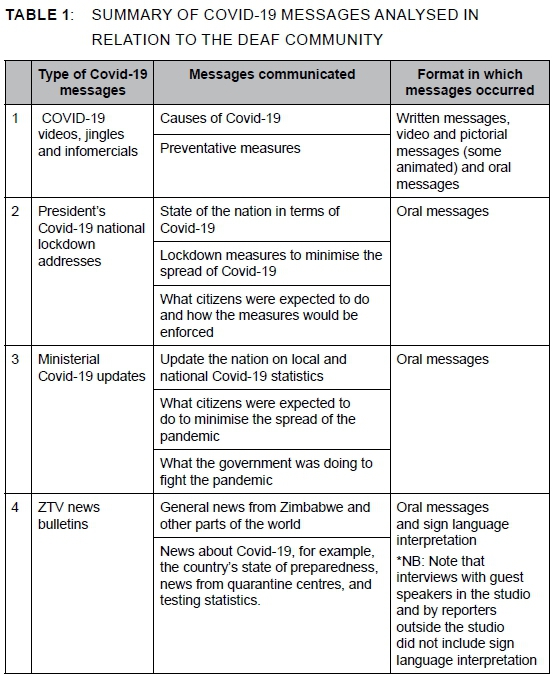
From the tabulated information, it is clear that efforts to ensure information reaches the Deaf community are still minimal in Zimbabwe. In terms of the Covid-19 pandemic, people who are deaf and hearing impaired have not been given enough information and education on how the disease is spread, how it is prevented, and on related issues. An inclusive means of communicating with people who have disabilities and other minority groups is therefore vital, as they are part of an already marginalised and vulnerable group of people.
Access to health care without barriers is a clearly defined right of people with disabilities, as stated by the UN Convention on the Rights of People with Disabilities (Kuenberg et al. 2016). Examples of approaches to improve access to health care, such as providing powerful and visually accessible communication using sign language, the implementation of important communication technologies, and cultural awareness training for health professionals, are discussed this document. According to the United Nations, enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being. The Convention is a powerful tool for working toward achieving human rights for deaf people (The World Federation of the Deaf 2019). The Convention is generally acknowledged as marking a paradigm shift concerning attitudes and approaches toward persons with disabilities, including deaf persons. It shifts from viewing them as "objects of charity, medical treatment, and social protection toward viewing persons with disabilities as subjects with rights, who are capable of claiming those rights and making decisions for their lives based on their free and informed consent, as well as being active members of society" (UN-SCRPD 2006: 178).
Information needs to be disseminated in accessible formats, such as Zimbabwean Sign Language, and consideration of these persons in resource allocation as well as priority setting. In Zimbabwe, the national news broadcasting platforms often do not reach the Deaf community because the majority cannot afford to own a television set and have limited access to the internet and electricity. In response to the Covid-19 pandemic, not all Zimbabwean government briefings were accompanied by ZSL interpreters and this provoked appreciable concern among people who are deaf and who rely solely on ZSL for information.
There was an outcry by the Deaf community after the Zimbabwean President made a public national address concerning the state of the Covid-19 national lockdown on 16 May 2020 on ZBC TV. The absence of a ZSL interpreter during the President's address raised many questions as far as inclusivity in the context of Covid-19 is concerned. A deaf person on Twitter lamented, "Where is my sign language interpreter, every time the president addresses the nation about Corona-Virus we need an interpreter please ZBC do something".
The researchers observed that in terms of access to Covid-19 information there is a significant gap between hearing people and those who are deaf. Section 62 of the Zimbabwean Constitution (Government of Zimbabwe 2013 states that "every citizen or permanent resident... has the right of access to information held by the state or by any institution or agency of government at every level, in so far as the information is required in the interest of the public accountability". However, despite these Constitutional provisions, ZSL is not prioritised and its use in the media is minimal. During the interviews as part of this study, it was revealed that despite ZSL video clips about Covid-19 awareness on ZBC TV, access to information remains a challenge for the Deaf community. The observed language practices on ZBC TV largely serve and maintain the interests of the dominant group, in this case hearing people.
According to the Zimbabwe Human Rights Bulletin (2015), most state and non-state institutions are not obliged to package services and information that has universal acceptance. Education attainment for deaf children remains much lower than for their hearing peers although the gap appears to be narrowing (Wilson & Sin 2015). Data on reading ability is dated, with the most recent research being from the 1990s. Wildon and Sin (2014) found the average reading age for a deaf school-leaver to be under nine years old. They further established that basic levels of literacy within the Deaf community are relatively low. Research confirms that the majority of deaf people are illiterate and only the partially deaf are able to lip read and write in English. This means that those who are profoundly deaf cannot communicate and express themselves in any other way than through sign language or a sign language interpreter.
Studies also confirm that deaf patients encounter severe communication barriers when accessing health services (c.f. Harmer 1999; Chaveiro et al. 2009; Pereira & Fortes 2010). Practitioners often believe that lip-reading/speech-reading and note writing provide effective health communication. In reality, these are ineffective communication modalities for health care conversations. Deaf people who have practiced lip-reading/ speech-reading for many years and who are familiar with the specific spoken language are able to understand at best 30 to 45 percent of spoken English (Lieu et al. 2007). Note writing is often constrained by deficits in health literacy and information deficits (Pollard & Barnett 2009). Smeijers and Pfau (2009) argue that treating a native use of sign language, who might not necessarily be fluent in the local written language, as if it was his/her first language, could cause serious communication problems.
While Zimbabwe continues to lag behind in terms of making vital Covid-19 information available for the Deaf community, in neighbouring South Africa efforts by the government and other stakeholders aimed at ensuring information availability for the Deaf are a top priority. The Centre for Deaf Studies (CFDS) at the University of the Witwatersrand (Wits) is contributing to society by keeping the Deaf community informed about the coronavirus pandemic through a number of initiatives that filtered information to the Deaf and hard of hearing communities in South Africa. When the President of South Africa addressed the nation to announce a national lockdown, the CFDS ensured there was a full live-stream interpreting by a Deaf person through the use of relay interpreting - a practise of translating messages from one language to another through a third language for a targeted audience. The CFDS has also increased efforts at raising awareness around Covid-19 among the Deaf by producing a video called Corona info for kids. The aim of the video was to make information accessible for deaf children in a deaf-appropriate way that would make an impact, which also included a fun hand-washing alphabet clip. Since the onset of the pandemic in South Africa, the CFDS has been offering and sharing information through these videos in South African Sign Language (SASL) to ensure the Deaf community could access information in their first language.
Similar to the South African example above, to mitigate against the compounded barriers the Deaf community face in accessing information, Tunisia, through the International Foundation for Electoral Systems (IFES), developed a video in Tunisian Sign Language to share information about the pandemic. The video, which features Deaf Tunisians as actors, describes the risks of the virus and provides critical information on how deaf people can protect themselves against Covid-19.
However, in Zimbabwe deaf people continue to face difficulties in accessing health information. Deaf sign language users do not have access to incidentally occurring information about health issues in public transport, or on the radio or television, and there is a general lack of health information and education materials provided in sign language. Limited English literacy and a lack of available information in sign language reduce access to preventative health care information for deaf people in Zimbabwe. What is paradoxical about the situation in Zimbabwe is that the Constitution of the country provides for the promotion and advancement of the use of ZSL. Thus, the Constitution embraces language as a basic human right and multilingualism as a national resource.
Many barriers that restrict deaf people from accessing Covid-19 information and health services are unfortunately a result of a lack of deaf awareness. According to Watkins (2010: 16),
Deaf awareness refers to a knowledge and awareness of the terms and characteristics of deafness, what it means to be deaf, how deaf people communicate and what is the best practice when communicating and working with deaf people. From a service provider's perspective, to be highly Deaf aware would be to understand how a deaf person would access their service and what provisions they would need so that they were able to access the service fully. To not be Deaf aware is to not consider or care how a deaf person would access a service, to be unaware of their needs and to not take any special measures to account for their needs.
From the discussion above regarding access to Covid-19 information by the Deaf community, it is clear that in Zimbabwe and other parts of the world a high lack of Deaf awareness compounded by a general lack of language resources for deaf people are creating barriers for deaf people's access to Covid-19 information and health services.
ACCESS TO COVID-19 INFORMATION AMONG THE LEP
According to UNESCO, Zimbabwe has an adult literacy rate of 88.69%. While Zimbabwe's literacy rate is among the highest in Africa, there are questions about the number of people who are proficient in English because for most Zimbabweans English is spoken as a second or even third language. The majority of Zimbabweans who speak English learn it as an additional language. Those who are not proficient in English are disadvantaged because the language is the main medium of instruction throughout the education system, a measure of educational achievement, and an important qualification for higher education and employment. One area in which people who are not proficient in English are disadvantaged pertains to access to health information.
Marginalised people, including those with LEP, have a right to clear, accurate and accessible information about Covid-19 and response efforts. Such persons need information in a language and format they understand. It must also be presented in a way that is relevant to them, and available in a channel they can access and trust. However, this is rarely the case with people with LEP, especially in Zimbabwe's mainstream media, as shown in Table 2.
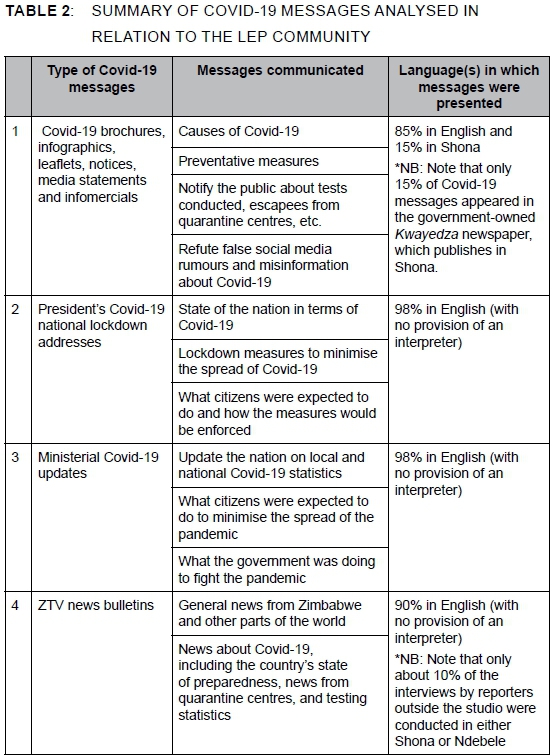
From Table 2 it is clear that Zimbabwe still faces information gaps regarding the Covid-19 pandemic. Most vital information about the pandemic is presented to citizens in English without due consideration for those with LEP. This means that people with LEP experience Covid-19 information gaps and hence are exposed to greater risk than those who are fluent in English.
In some parts of the world, the Covid-19 pandemic has seen changes in expectations for translation and interpreting services. In the USA, the government and various language bodies now provide information in various languages to help communicate during the pandemic. An example is a publication by the Centres for Disease Control and Prevention titled CDC Communication Toolkit for Migrants, Refugees, and Other Limited-English-Proficient Populations. Translators Without Borders (TWD) also released another publication, titled TWB's Global Response to Covid-19 (Velasquez et al. 2020).
These bodies do not only provide interpretation services in healthcare for those with LEP but also provide the same service in other areas of need, including the provision of information about lockdowns and stay-at-home rules; instructions for wearing face coverings on public transport; restricted hours at supermarkets; guidance for home schooling; access to emergency financial aid programmes or mortgage "holidays"; and help lines for mental health. All these services would be rendered unavailable when someone with LEP does not understand the language in which the content is offered. Thus, the CDC and TWB provide language services for those who need these in order to curb the possible long-term effect of the pandemic in those parts of the community not fluent in the local language. In Zimbabwe no similar efforts have been made regarding meeting the language needs of the LEP community. The current state of affairs regarding language access among the LEP in Zimbabwe could be attributed to a lack of resources to fund language research and language services provision. Apart from this, lack of commitment on the part of the government aimed at ensuring that a citizen's right to information is respected at all times could be another cause for the continued disregard of the LEP community's needs.
IMPLICATIONS AND RECOMMENDATIONS
Global Covid-19 responses identify risk communication and community engagement as a priority. This means that all responses should communicate effectively with communities, counter misinformation and make sure that all people, regardless of age, gender, status and class can take the necessary steps to protect themselves and their communities.
To achieve the above, the researchers propose that all Covid-19 messages be presented in an appropriate language and format and be relevant in content and medium depending on the purpose of the message and the target audience. From a socio-pragmatic point of view (Agbara & Omole 2014), when a speaker conveys meaning from their utterances, he/she should do so in a way that allows listeners to interpret meaning from those utterances and take the necessary actions. In the context of this study, the necessary actions may include taking preventative measures against Covid-19, getting tested or receiving treatment, or even self-isolating when one suspects he/she has Covid-19.
Communicating in international lingua francas or national (official) languages like English, in the case of Zimbabwe, makes marginalised people more vulnerable. While English is the official language of government business in Zimbabwe, it is spoken by the majority of Zimbabweans as a second or even third language. For the Deaf and other disadvantaged groups, most of whom often have fewer educational opportunities and are less likely to speak or read English as a second language, marginalisation in the face of Covid-19 is exacerbated.
The format in which information is presented affects how well it is understood. While even those who cannot read value written text, many people find pictorial, audio and video content easier to understand. Accessibility for older and semi-literate people depends on design considerations, such as larger fonts and good contrast. To convey the correct information, pictorial messaging should also reflect local culture and practices. Misinformation and mistrust flourish when communication does not clearly answer people's questions. To be useful, the information must be tailored to the intended audience. It must respond to people's questions and concerns. Covid-19 messages must be clearly expressed using concepts, sentence structures and terminology that audiences are familiar with. Experience from previous disease outbreaks shows this is a key factor for communities' trust in and uptake of health guidance, including health-seeking behaviour.
For communication to be successful, the researchers propose locally preferred and trusted communication channels to ensure the two-way flow of information. Since Covid-19 infection control limits face-to-face communication, social media, SMS services, call centres, television and radio are essential. However, these channels carry the risk of exacerbating inequalities and feelings of exclusion for some marginalised groups (the Deaf and LEP, for instance).
In view of the above, the researchers suggest a few practical actions. First, all risk communication regarding Covid-19 and community engagement that arise from it, should be based on language data. This means stakeholders should always prioritise the identification of the most effective languages, formats and channels for communicating about Covid-19. This also means that stakeholders need to value the critical role language and literacy maps can play in information dissemination and access. While language and literacy maps are vital tools in some parts of the world, such as Malawi, Mozambique, Nigeria and Zambia, such tools are rarely used in Zimbabwe.
Secondly, stakeholders should provide coordinated, timely two-way communication in the right languages, formats, and channels. The government and relevant organisations in the fight against Covid-19 should develop content in the widest possible range of relevant languages and include formats suitable and accessible for the most vulnerable individuals. All communication, whether in written, pictorial or audio format, should follow accepted plain-language principles designed to minimise reading effort. In addition, efforts should also be taken to ensure that there is agreement and a common understanding on the use of words and phrases that best describe difficult concepts. In a rapidly evolving situation like the Covid-19 pandemic, this means going beyond a static message bank and engaging in active quality control of communication efforts.
Finally, the government of Zimbabwe should also improve resourcing for language support across the response. In this regard, the researchers propose that universities and language institutes should be allocated resources to meet the information and communication needs of marginalised people. It could ensure that the right tools to communicate accurate information in local languages and with the appropriate terminology are accessible to all. Language technology could also support multilingual communication at speed.
CONCLUSION
This study adopted a socio-pragmatic approach to interrogate how language choices by various forms of print and electronic media affect access to Covid-19 information by the Deaf and LEP communities in Zimbabwe. The article has shown that the way mass media messages are packaged in relation to context, topic, language and medium in any communicative situation may result in misinterpretation and hence, a lack of understanding of the speaker's intended message. In the context of this study, a lack of understanding of the speaker's message may have dire consequences, particularly when dealing with a pandemic like Covid-19. It is clear that continuing to marginalise people by failing to address their information and communication needs will prevent the global response from being as effective as it could and should be. State actors, local agencies and health systems should adapt in the midst of this crisis and develop collaborations with social service organisations, media outlets and other stakeholders that allow for the prompt development and distribution of Covid-19 health information to the Deaf and people with LEP. Only then can we bridge the gap in health information access, which continues to drive longstanding health disparities.
REFERENCES
Agbara, C.U.B. & Omole, K. 2014. A pragmatic analysis of speech acts strata in Nigeria's legislative discourse. International Journal of Research in Arts and Social Sciences 7(2): 172-180. [ Links ]
Chaveiro, N., Porto, C.C. & Barbosa, M.A. 2009. The relation between deaf patients and the doctor. Brazilian Journal of Otorhinolaryngology 75: 147-150. https://doi.org/10.1016/S1808-8694(15)30846-6 [ Links ]
Crystal, D. 2003. A dictionary of linguistics and phonetics. (Fifth edition). Oxford: Blackwell. [ Links ]
Emond, A., Ridd, M., Sutherland, H., Allsop, L., Alexander, A. & Kyle, J. 2015. Access to primary care affects the health of deaf people. British Journal of General Practice 65: 95-96. https://doi.org/10.3399/bjgp15X683629 [ Links ]
Fromkin, V., Rodman, R. & Hyams, N. 2003. An introduction to language. (Seventh edition). Boston: Wadsworth. [ Links ]
Government of Zimbabwe. 2013. Constitution of Zimbabwe. Amendment No. 20 Act. Harare: Government Printers. [ Links ]
Harmer, L. 1999. Health care delivery and deaf people: Practice, problems, and recommendations for change. Journal of Deaf Studies and Deaf Education 4: 73110. https://doi.org/10.1093/deafed/4.2.73 [ Links ]
Haualand, H. 2012. Interpreting ideas and relaying rights. A comparative study of video interpreting services in Norway, Sweden and the United States. Unpublished doctoral thesis. University of Oslo. [ Links ]
Komaric, N., Bedford, S. & Van Driel, M.L. 2012. Two sides of the coin: Patient and provider perceptions of health care delivery to patients from culturally and linguistically diverse backgrounds. BMC Health Services Research 12: 322. https://doi.org/10.1186/1472-6963-12-322 [ Links ]
Kuenberg, A., Fellinger, P. & Fellinger, J. 2016. Health care access among deaf people. Journal of Deaf Studies and Deaf Education 2016: 1-10. https://doi.org/10.1093/deafed/env042 [ Links ]
Kusters, A., De-Meulder, M. & Brien, D.O. 2017. Innovations in Deaf Studies. The Role of Deaf Scholars. Oxford: Oxford University Press. [ Links ]
Leech, G.N. 1983. Principles of pragmatics. London: Longman. [ Links ]
Lieu, C.C., Sadler, G.R., Fullerton, J.T. & Stohlmann, P.D. 2007. Communication strategies for nurses interacting with patients who are deaf. Dermatology Nursing/Dermatology Nurses' Association 19: 541-551. [ Links ]
LoCastro, V. 2012. Pragmatics for language educators: A sociolinguistic perspective. Abingdon: Routledge. https://doi.org/10.4324/9780203850947 [ Links ]
Mey, J.L. 2001. Pragmatics: An introduction. Oxford: Wiley-Blackwell. [ Links ]
Ndlovu, S.B. 2016. The Deaf and Education in Zimbabwe. Harare: Deaf Trust Zimbabwe. [ Links ]
Pereira, P.C. & Fortes, P.A. 2010. Communication and information barriers to health assistance for deaf patients. American Annals of the Deaf 155: 31-37. https://doi.org/10.1353/aad.0.0128 [ Links ]
Pollard, R.Q. & Barnett, S. 2009. Health-related vocabulary knowledge among deaf adults. Rehabilitation Psychology 54: 182-185. https://doi.org/10.1037/a0015771 [ Links ]
Ralarala, M.K. & Rodrigues, T. 2019. Incarcerated, incriminated or vindicated? An investigation into socio-pragmatic elements of police interviewing. In: Ralarala, M.K., Kaschula, R.H. & Heydon, G. (eds). New frontiers in forensic linguistics: Themes and perspectives in language and law in Africa and beyond. Cape Town: African Sun Media. https://doi.org/10.18820/9781928480174 [ Links ]
Smeijers, A.S. & Pfau, R. 2009. Towards a treatment for treatment: On communication between general practitioners and their deaf patients. The Sign Language Translator and Interpreter 3: 1-14. [ Links ]
UN-SCRPD. 2006. Convention on the rights of persons with disabilities. [Online]. Available at: http://www.un.org/disabilities/default.asp?navid15&pid150 [Accessed on 27 June 2020]. [ Links ]
Velasquez, D., Uppal, N. & Perez, N. 2020. Equitable access to health information for non-English speakers amidst the novel coronavirus pandemic. [Online]. Available at: 10.1377/hblog20200331.77927 [Accessed on 21 July 2020]. [ Links ]
Watkins, G. 2010. D/deaf people's access to sexual health support and information. University of Liverpool: Sahir House. [ Links ]
Wilson, M. & Sin, C.H. 2014. Research into the Deaf audience in the UK. [Online]. Available at: http://www.bslzone.co.uk/flles/4914/5320/1727/OPM_Report_Research_into_the_Deaf_Audience_Jan_2016.pdf. [Accessed on 17 July 2020]. [ Links ]
Zimbabwe Human Rights Bulletin. 2015. Rights of persons with disabilities. Number 109. English. August 2015. [ Links ]
Zimeye. 2020. [Online]. Available at: https://www.zimeye.net/people_with_disabilities-drag-mnangagwa-government-to-court-over-selective-dissemination-of-information/ [Accessed on 18 April 2020]. [ Links ]

