










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkClean Air Journal
versión On-line ISSN 2410-972X
versión impresa ISSN 1017-1703
Clean Air J. vol.28 no.1 Pretoria 2018
http://dx.doi.org/10.17159/2410-972x/2018/v28n1a11
RESEARCH ARTICLE
Household air pollution exposure and respiratory health outcomes: a narrative review update of the South African epidemiological evidence
Busisiwe SheziI; Caradee Y WrightII, III, *
IEnvironment and Health Research Unit, South African Medical Research Council, Durban, South Africa, busisiwe.shezi@mrc.ac.za
IIEnvironment and Health Research Unit, South African Medical Research Council, Pretoria, South Africa
IIIDepartment of Geography, Geo-informatics and Meteorology, University of Pretoria, Pretoria, South Africa, cwright@mrc.ac.za
ABSTRACT
One of the greatest threats to public health is personal exposure to air pollution from indoor sources. The impact of air pollution on mortality and morbidity globally and in South Africa is large and places a burden on healthcare systems for treatment and care of air pollution-related diseases. Household air pollution (HAP) exposure attributed to the burning of solid fuels for cooking and heating is associated with several adverse health impacts including impacts on the respiratory system. The researchers sought to update the South African evidence on HAP exposure and respiratory health outcomes from 2005. Our quasi-systematic review produced 27 eligible studies, however, only four of these studies considered measures of both HAP exposure and respiratory health outcomes. While all of the studies that were reviewed show evidence of the serious problem of HAP and possible association with negative health outcomes in South Africa, no studies provided critically important information for South Africa, namely, local estimates of relative risks that may be applied in burden of disease studies and concentration response functions for criteria pollutants. Almost all of the studies that were reviewed were cross-sectional, observational studies. To strengthen the evidence of HAP exposure-health outcome impacts on respiratory health, researchers need to pursue studies such as cohort, time-series and randomised intervention trials, among other study designs. South African and other researchers working in this field need to work together and take a leap towards a new era of epidemiological research that uses more sophisticated methods and analyses to provide the best possible evidence. This evidence may then be used with greater confidence to motivate for policy-making, contribute to international processes such as for guideline development, and ultimately strengthen the evidence for design of interventions that will reduce HAP and the burden of disease associated with exposure to HAP in South Africa.
Keywords: environmental health, air quality, household emissions
Introduction
While episodes of unusually high air pollution attract attention and public health concern, the greatest damage to public health is associated with long-term exposure to air pollution (HEI 2017). Outdoor and indoor personal exposure to air pollution, combined, comprise the largest environmental risk factor for mortality, responsible for 6.4 million deaths in 2015 (11% of global deaths) (Cohen et al. 2017).
The costs of air pollution in Africa are high - estimated at around USD450 billion in 2013 (Roy 2016). The economic impacts include life years lost, increased healthcare (and subsequent demand on government) and lost worker productivity due to air pollution impacts on health.
Globally, epidemiological studies and systemic reviews have shown associations between exposure to household air pollution (HAP) and a variety of diseases and symptoms (Jedrychowski et al. 2017; Tanaka et al. 2012; Koo et al. 2011; Pope et al. 2010). The indoor environment represents an important microenvironment in which people spend approximately 90% of their time each day (WHO 2014a).
According to the World Health Organization (WHO), HAP is responsible for more than 1.6 million annual deaths globally, and 2.7% of the global burden of disease (WHO 2014b). HAP is reported to increase irritation of the airways, coughing, irregular heartbeat, difficulty breathing and premature death in people with heart and lung disease (Gurley et al. 2013; Laumbach and Kipen, 2012; Ritz and Wilhelm, 2008). Exposure further worsens existing respiratory diseases such as bronchitis, cardiovascular disease and emphysema (Laumbach and Kipen, 2012; Fisk et al. 2010; Rinne et al. 2006). Exposure to solid fuel burning indoors has also been associated with tuberculosis (TB) (Jafta et al. 2015; Lin et al. 2014), cataract (Ravilla et al. 2016) and adverse birth outcomes (Wylie et al. 2017; Pope et al. 2010).
HAP is derived from multiple indoor sources (Colbeck and Nasir 2010) varying from one building to another and depending on fuels used for heating and cooking, smoking habits and use of a wide variety of consumer products and building materials (Shezi et al. 2017; Jafta et al. 2017; Tanaka et al. 2012; Verma et al. 2010). This is also influenced by time activity patterns i.e. cooking period, number of meals cooked, single or multiple fuel use and number of cigarettes smoked and further compounded by confounding variables such as outdoor air pollution sources near the homes (Shezi et al. 2017; Colbeck and Nazir 2010). In developing countries, the most significant indoor air quality issue is exposure to pollutants released during combustion of solid fuels used for cooking and heating in the home (Wylie et al. 2017; Pope et al. 2010).
The measured mean concentrations of the HAP vary depending on the sources, for example, average particulate matter with an aerodynamic diameter of 2.5 (PM25) concentration in households using solid fuels has been reported to range from 133.5 ug/m3 to 670 ug/m3 (Balakrishnan et al., 2015; Balakrishnan et al., 2013; Clark et al., 2010), while the carbon monoxide (CO) average concentrations have been reported to range from 2.7 ppm to 14.3 ppm. The average PM25 concentrations in households using cleaner fuels have been reported to range from 10 ug/m3 to 38 Ug/m3 (Shezi et al. 2017; Tunno et al., 2015; Evans et al. 2000). Studies conducted in South Africa have also reported high mean concentrations in households using both clean and dirty fuels (Jafta et al. 2017; Shezi et al. 2017; Wernecke et al 2015; Rollin et al. 2004) which exceed the guidelines set out by the WHO for indoor air quality in households; South African indoor air quality guidelines pertaining to household air pollution are under review and have not yet been promulgated.
South Africa is a middle-income country burdened by poverty and inequality where many South Africans are exposed to biomass fuels used for cooking and heating indoors. Many families live in close proximity to industrial areas and major roads (Albers et al. 2015; StatsSA 2012; Norman 2007) where outdoor pollutants may also be transported indoors (Colbeck and Nasir 2010). Vulnerable groups such as people who are elderly, women, young children, people with pre-existing diseases and people living in poverty are more susceptible to air pollution health impacts (Barnes 2014).
The WHO comparative risk assessment determined the mortality burden and Disability Adjusted Life Year (DALYs) due to HAP. HAP associated with household solid fuel use for cooking and heating caused 0.5% of all deaths in South Africa in 2000 (uncertainty 0.3% -0.6%) (Norman et al., 2010). More than 10 years ago, Wichmann and Voyi (2005) published a review of the air pollution and health epidemiological studies in South Africa, focussing on methodological issues and the need for quantitative intervention studies. In 2014, Barnes (2014) described behavioural change studies for reduction of HAP in developing countries, calling for more rigorous study design and interventions grounded in behavioural change theory. In recent years, anecdotal evidence suggests that studies on the impact of HAP and associated respiratory health outcomes has been growing in South Africa (Barnes et al., 2009). In this narrative review, evidence from the recently published South African studies that considered HAP exposure and associated respiratory health outcomes to augment our current knowledge is collated. An attempt to identify research gaps and suggest directions for further studies is made.
Review methods
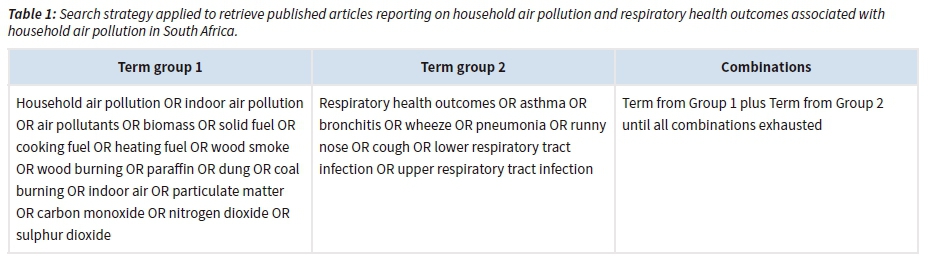
A quasi-systematic (i.e. following the guidelines for systematic review but with slight differences in methods to accommodate all available evidence) review of the South African evidence on HAP (term group 1) and associated respiratory health outcomes (term group 2) was conducted using the PRISMA guidelines (Moher et al. 2009). PubMed, Web of Science, Science Direct and Google Scholar were searched for studies with full text in English, published between 2005 and 2017. The term groups listed in Table 1 were used for the separate searches and in various combinations. The reference lists of included papers were searched to ensure that no studies were omitted.
To be eligible, studies had to have been carried out in South Africa. All epidemiological study designs including cross-sectional studies, cohort studies, longitudinal studies, case-cross-over studies, intervention studies etc. were eligible. All studies that provided estimates of HAP exposure concentrations (by indicator, proxy or actual measurements) as well as respiratory health outcomes found to be associated with HAP exposure were included. We noted whether the correlate and health outcome was measured at the level of the individual, household or community. The review was not restricted by defining a minimal study sample size and studies of all sample sizes were included.
Results
After removing all ineligible articles, mostly since they were studies unrelated to South Africa, our searches using both formal methods (described above) and informal means (such as personal communication with researchers) produced a total of 27 articles. Of this total, only 4 studies measured HAP exposure (mainly by proxy/indicators of air pollution exposure) and respiratory health outcomes. Ten studies assessed HAP but no respiratory health outcome(s) and the remaining 13 studies did not measure HAP, instead used ambient AQ monitoring station data (or other) for exposure assessment.
Table 2 describes in brief the four studies that included HAP exposure monitoring and associated respiratory health outcomes by type of study, setting, sample size, methods, exposure information and outcome results. None of the studies measured HAP, instead, they used indicators or proxies for exposure, such as presence of environmental tobacco smoke (ETS) and fuel used for cooking and / heating in the home. Elf et al. (2017) used passive samplers to measure ETS. All of the studies were cross-sectional epidemiological study designs and the largest sample size was ~ 3 000 schoolchildren (Shirinde et al., 2014) with the other three studies having sample sizes of less than 1 000 individuals (no sample size calculations were provided). One study did not set out to measure HAP but rather focussed on ETS exposure.
Inter-comparison of the findings of the studies is difficult due to the heterogeneity in the study design, target population and health outcomes of interest. Both Albers et al. (2015) and Shirinde et al. (2014) found that among schoolchildren (albeit of different ages) there was an association between respiratory outcomes (most notably wheeze) and use of non-electrical heating sources. Elf et al. (2017) and du Preez et al. (2011) consider TB as a health endpoint and ETS and solid fuel use, and ETS, respectively, in relation to TB.
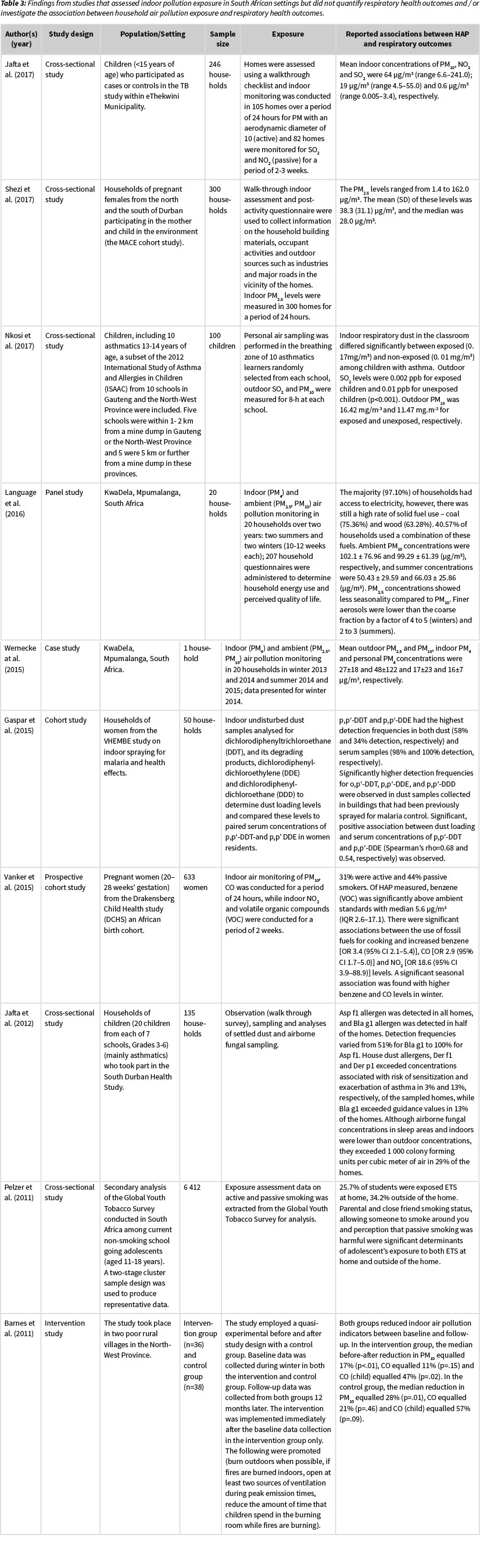
Tables 3 and 4 summarise the remaining studies that the researchers reviewed as part of this review exercise. These studies did not meet the study inclusion criteria; however, they do provide useful information on the levels of various air pollutants in the indoor and outdoor environments of different parts of South Africa. Since they did not mention respiratory health outcomes, the researchers do not discuss them in detail here, but included them as a reference for future research.
Of the twenty-three studies listed in Table 3 and 4, two studies were review articles, six studies used questionnaires and interviews which are methods of assessment that are based on self-report and recall. Either indoor and / or outdoor pollutants were measured in 15 studies and some of the studies measured multiple pollutants. Particulate matter with an aerodynamic diameter of 10 (PM10) was measured in twelve studies while PM25 and particulate matter with an aerodynamic diameter of 4 (PM4) were measured in four and two studies, respectively. Two studies measured respiratory particulate matter (RPM). NO2 was measured in five studies; NOx in one study and volatile organic compounds were also measured in one study. Three studies measured CO and seven studies measured sulphur dioxide (SO2). Ozone (O3) was measured in one study and total reduced sulphur was also measured in one study. Indoor undisturbed dust samples were undertaken in one study to analyse for dichlorodiphenyltrichloroethane (DDT), dichlorodiphenyl-dichloroethylene (DDE) and dichlorodiphenyl-dichloroethane (DDD), while settled dust and airborne fungal sampling was also conducted in one study.
Discussion
Few published studies conducted in South Africa in recent years have sought to show associations between HAP and respiratory health outcomes. All of the studies that did so used cross-sectional study design. This is unfortunate since most international systematic reviews for HAP exposure and health outcome association only use data from cohort, time series, long-term panel (longitudinal) and case-crossover studies. Our studies are therefore not contributing to international evidence on this important topic, nor are they providing reliable evidence that is generalizable to others parts of South Africa. While cross-sectional studies are typically less expensive and easier to implement compared to other epidemiological study designs, the data produced from cross-sectional studies is not as useful and the lack of randomisation, among other shortfalls, prohibits generalisation. Researchers need to work towards larger, more complex epidemiological studies and also use of existing, high quality (where possible) data in South Africa that will help to address the problem of HAP and respiratory health. While it will likely cost more, other study designs beside cross-sectional studies, will provide opportunities for HAP monitoring over substantial periods of time to provide exposure information that can then be associated with health outcomes, preferably diagnosed by a health professional (and not self-reported or parent-reported) for more precise results, in a more meaningful way.
It is also important to account for potential biases and critical confounders, including age, sex, and individual socio-economic status, among others, when planning a HAP and respiratory health study, and also when reporting study results as failure to control for confounding variables can lead to erroneous associations between HAP and respiratory outcomes.
While the reviewed studies predominantly report on combustion generated variables (type of fuel used for cooking or heating and active or passive smoking) with PM, CO and NO2, being products of incomplete combustions, other sources of indoor air pollutants not necessarily emitted by incomplete combustion such as building materials, ventilation characteristics and cleaning agents may not be ignored.
While, exposure data misclassification and validity of exposure are often overlooked or underestimated and not critically discussed (Wichmann and Voyi, 2005), the lack of direct exposure measurement such as the use of home monitors and personal monitors present results that are in some part questionable.
None of the studies reviewed provided concentration response functions for the criteria air pollutants in South Africa (DEA, 2009). This point was made by Wichmann and Voyi (2005) and it still holds true in 2017. This is still a major gap in our knowledge in both South Africa and on the continent. South African researcher continue to use the international literature and WHO evidence, without making contribution to this important body of knowledge.
Another shortfall is that only one study reviewed in this exercise was an intervention study (under real life conditions). The WHO calls for the support of research that is driven by interventions and searching actively for solutions, in particular for urban settings, in relation to air pollution and health (WHO 2014). In South Africa, research partnerships and consortia may assist to create large research teams to lead intervention studies to address HAP and adverse health impacts in areas of greatest concern.
Our study had some limitations. There were very few studies to critically review hence the researchers opted to describe them descriptively instead. Wichmann and Voyi (2005) provided a critical synthesis of the evidence in this field up to 2005. The authors did not find a substantial number of studies to add to that body of literature beyond 2005. The authors set out to find studies that had measured HAP and simultaneously measured respiratory health outcomes. The authors may have not identified all studies relevant to the review inclusion criteria, although they tried to avoid this by searching the literature regularly and speaking with South African researchers in the air pollution and health fields. The authors did not consider mortality as an end-point. Wichmann and Voyi (2006) found that exposure to cooking and heating smoke from polluting fuels was significantly associated with 1-59-month mortality, after controlling for mother's age at birth, water source, asset index and household crowdedness (RR=1.95; 95% CI=1.04, 3.68).
Conclusions
The South African studies on HAP and respiratory health outcomes do provide some evidence of the serious impacts of HAP and especially the use of solid fuels in the home on respiratory health in the country, but the studies are few and limited. South African and other researchers working in this field need to work together and take a leap towards a new era of epidemiological research that uses sophisticated methods and analyses to provide the best possible evidence. This evidence may then be used with greater confidence to, for example, motivate for policy-making, contribute to international systematic reviews for guideline development and other purposes, and ultimately strengthen interventions that will reduce HAP and the burden of disease associated with exposure to HAP in South Africa.
Acknowledgements
We thank MA Oosthuizen for assisting with data collection. B Shezi and CY Wright receive research funding support from the South African Medical Research Council. CY Wright receives funding support from the National Research Foundation.
References
Albers P. N., Wright C. Y., Mathee A., & Voyi K. 2015, 'Household fuel use and child respiratory ill health in two towns in Mpumalanga South Africa', South African Medical Journal 105: 573-7. [ Links ]
Amegah A. K. & Agyei-Mensah S. 2017, 'Urban air pollution in Sub-Saharan Africa: Time for action', Environmental Pollution 220: 738-43. [ Links ]
Ayo-Yusuf O. A., Olufajo O., & Agaku I. T. 2014, 'Exposure to secondhand smoke and voluntary adoption of smoke-free home and car rules among non-smoking South African adults', BMC Public Health 14: 580. [ Links ]
Barnes B., Mathee A., Thomas E., & Bruce N. 2009, 'Household energy, indoor air pollution and child respiratory health in South Africa', Journal of Energy in Southern Africa 20: 4-13. [ Links ]
Barnes B. R. 2014, 'Behavioural change, indoor air pollution and child respiratory health in developing countries: A review', International Journal of Environmental Research and Public Health 11: 4607-18. [ Links ]
Cohen A. J., Brauer M., Burnett R., Anderson H. R., Frostad J., Estep K., Balakrishnan K., Brunekreef B., Dandona L. & Dandona R. 2017, 'Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015', The Lancet 389: 1907-18. [ Links ]
Colbeck I. & Nasir Z.A. 2010, 'Indoor Air Pollution. In: Lazaridis M & Colbeck I (eds) Human Exposure to Pollutants via Dermal Absorption and Inhalation', Dordrecht: Springer Netherlands. [ Links ]
Department of Environmental Affairs. 2009, 'National Environmental Managerment: Air Quality Act, 2004 (Act No. 39 of 2004)', South Africa. [ Links ]
Du Preez K., Mandalakas A., Kirchner H., Grewal H., Schaaf H., Van Wyk S., & Hesseling A. 2011, 'Environmental tobacco smoke exposure increases Mycobacterium tuberculosis infection risk in children', The International Journal of Tuberculosis and Lung Disease 15: 1490-97. [ Links ]
Elf J. L., Eke O., Rakgokong M., Variava E., Baliram Y., Motlhaoleng K., Lebina L., Shapiro AE.,Breysse PN. & Golub J. E. 2017, 'Indoor air pollution from secondhand tobacco smoke, solid fuels, and kerosene in homes with active tuberculosis disease in South Africa', BMC Research Notes 10: 591. [ Links ]
Fisk W.J., Eliseeva EA & Mendell M.J. 2010, 'Association of residential dampness and mold with respiratory tract infections and bronchitis: a meta-analysis', Environmental Health 9: 72. [ Links ]
Gaspar F. W., Chevrier J., Bornman R., Crause M., Obida M., Barr D. B., Bradman A., Bouwman H. & Eskenazi B. 2015. 'Undisturbed dust as a metric of long-term indoor insecticide exposure: Residential DDT contamination from indoor residual spraying and its association with serum levels in the VHEMBE cohort', Environment international 85: 163-7. [ Links ]
Gurley E.S., Salje H., Homaira N., Ram P.K, Haque R., Petri Jr. W.A., Bresee J., Moss W.J., Luby S.P., Breysse P. & Azziz-Baumgartner E. 2013. 'Seasonal concentrations and determinants of indoor particulate matter in a low-income community in Dhaka, Bangladesh', Environmental Research 121: 11-16. [ Links ]
HEI (2017) State ofGlobalAir2017, 'Special Report, Health Effects Institute', Boston. https://www.stateofglobalair.org [ Links ]
Jafta N., Batterman S. A., Gqaleni N., Naidoo R. N., & Robins T. G. 2012, 'Characterization of allergens and airborne fungi in low and middle-income homes of primary school children in Durban, South Africa', Americanjournal of industrial medicine 55: 1110-21. [ Links ]
Jafta N., Jeena P., Barregard L., & Naidoo R. 2015, 'Childhood tuberculosis and exposure to indoor air pollution: a systematic review and meta-analysis', The International Journal of Tuberculosis and Lung Disease 19:596-602. [ Links ]
Jafta N., Barregard L., Jeena P. M., & Naidoo R. N. 2017, 'Indoor air quality of low and middle income urban households in Durban, South Africa', Environmental research 156: 47-56. [ Links ]
Jedrychowski W., Majewska R., Spengler J., Camann D., Roen E., & Perera F. 2017, 'Prenatal exposure to fine particles and polycyclic aromatic hydrocarbons and birth outcomes: a two-pollutant approach', International archives of occupational and environmental health 90, 255-64. [ Links ]
Kistnasamy E. J., Robins T. G., Naidoo R., Batterman S., Mentz G., Jack C., & Irusen E. 2008. 'The relationship between asthma and ambient air pollutants among primary school students in Durban, South Africa', International Journal of Environment and Health 2: 365-85. [ Links ]
Koo C., Gupta N., Baliff J., Hudock K., & Haas A. 2011, 'A tale of two sisters: Biomass fuel exposure-related lung disease', Clinical radiology 66: 190-3. [ Links ]
Laumbach R.J. & Kipen H.M. 2012, 'Respiratory health effects of air pollution: update on biomass smoke and traffic pollution,' Journal of Allergy and Clinical Immunology 129: 3-11. [ Links ].
Language B, Piketh S.J, Wernecke B. & Burger R. 2016, Household air pollution in South African low-income settlements: a case study, WIT Transaction Ecology and Environment 207: 227-36. [ Links ]
Lin H.H., Suk C.W., Lo H.L., Huang R.Y., Enarson D.A. & Chiang C.Y., 2014, 'Indoor air pollution from solid fuel and tuberculosis: a systematic review and meta-analysis', The International Journal of Tuberculosis and Lung Disease 18:613-21. [ Links ]
Moher D., Liberati A., Tetzlaff J., & Altman D. G. 2010, 'Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement', International Journal of Surgery 8:336-41. [ Links ]
Morakinyo O. M., Adebowale A. S., Mokgobu M. I., & Mukhola M. S. 2017, 'Health risk of inhalation exposure to sub-10 um particulate matter and gaseous pollutants in an urban-industrial area in South Africa: an ecological study', BMJ Open 7:e013941. [ Links ]
Naidoo R. N., Jack C., Robins T., Batterman S., & Mentz G. 2013, 'Ambient pollution and respiratory outcomes among schoolchildren in Durban, South Africa', South African Journal of Child Health 7, 127-34. [ Links ]
Nkosi V., Wichmann J., & Voyi K. 2017, 'Indoor and outdoor PM 10 levels at schools located near mine dumps in Gauteng and North West Provinces, South Africa', BMC Public Health 17:42. [ Links ]
Nkosi V., Wichmann J., & Voyi K. 2015a, 'Chronic respiratory disease among the elderly in South Africa: any association with proximity to mine dumps?' Environmental Health 14:33. [ Links ]
Nkosi V., Wichmann J., & Voyi K. 2015b, 'Mine dumps, wheeze, asthma, and rhinoconjunctivitis among adolescents in South Africa: any association?', International Journal of Environmental Health Research 25:583-600. [ Links ]
Norman R, Cairncross E., & Witi J. 2007, 'Estimating the burden of disease attributable to outdoor air pollution in South Africa', South African Medical Journal 97: 782-90. [ Links ]
Norman R., Bradshaw D., Lewin S., Cairncross E., Nannan N., Vos T., & Group S. A. C. R. A. C. 2010, 'Estimating the burden of disease attributable to four selected environmental risk factors in South Africa', Reviews on environmental health 25: 87-120. [ Links ]
Nriagu J., Robins T., Gary L., Liggans G., Davila R., Supuwood K., Harvey C., Jinabhai CC. & Naidoo R. 1999, 'Prevalence of asthma and respiratory symptoms in south-central Durban, South Africa', European Journal of Epidemiology 15:747-55. [ Links ]
Peltzer K. 2011, 'Determinants of exposure to second-hand tobacco smoke (SHS) among current non-smoking in-school adolescents (aged 11-18 years) in South Africa: results from the 2008 GYTS study', International Journal of Environmental Research and Public Health 8:3553-61. [ Links ]
Pope D. P., Mishra V., Thompson L., Siddiqui A. R., Rehfuess E. A., Weber M., & Bruce N. G. 2010, 'Risk of low birth weight and stillbirth associated with indoor air pollution from solid fuel use in developing countries', Epidemiologic reviews 32:70-81. [ Links ]
Ravilla T.D., Gupta S., Ravindran R.D., Vashist P., Krishnan T., Maraini G., Chakravarthy U. & Fletcher A.E, 2016, 'Use of cooking fuels and cataract in a population-based study: The India Eye Disease Study', Environmental Health Perspective 124:1857-62. [ Links ]
Reddy P., Zuma K., Shisana O., Jonas K., & Sewpaul R. 2015, 'Prevalence of tobacco use among adults in South Africa: Results from the first South African National Health and Nutrition examination survey', South African Medical Journal 105:648-55. [ Links ]
Reddy P., Naidoo R. N., Robins T. G., Mentz G., Li, H., London S. J., & Batterman S. 2012, 'GSTM1 and GSTP1 gene variants and the effect of air pollutants on lung function measures in South African children', American journal of industrial medicine, 55:1078-86. [ Links ]
Rinne S. T., Rodas E. J., Bender B. S., Rinne, M. L., Simpson, J. M., Galer-Unti, R., & Glickman, L. T. 2006, 'Relationship of pulmonary function among women and children to indoor air pollution from biomass use in rural Ecuador', Respiratory Medicine 100: 1208-15. [ Links ]
Ritz B. & Wilhelm M. 2008, 'Ambient air pollution and adverse birth outcomes: methodologic issues in an emerging field', Basic & Clinical Pharmacology & Toxicology 102: 182-90. [ Links ]
Roy R. 2016, 'The cost of air pollution in Africa', OECD Publishing, Paris, France. [ Links ]
Shezi B., Jafta N., Sartorius B., & Naidoo R. N. 2018, 'Developing a predictive model for fine particulate matter concentrations in low socio-economic households in Durban, South Africa', Indoor Air, 28: 228-37. [ Links ]
Shirinde J., Wichmann J., & Voyi K. 2015, 'Allergic rhinitis, rhinoconjunctivitis and hayfever symptoms among children are associated with frequency of truck traffic near residences: a cross sectional study', Environmental Health, 14:84. [ Links ]
Shirinde J., Wichmann J., & Voyi K. 2014, 'Association between wheeze and selected air pollution sources in an air pollution priority area in South Africa: a cross-sectional study', Environmental Health, 13:32. [ Links ]
Siddiqui A. R., Gold E. B., Yang X., Lee K., Brown K. H., & Bhutta Z. A. 2008, 'Prenatal exposure to wood fuel smoke and low birth weight', Environmental Health Perspectives, 116:43 [ Links ]
Tanaka K., Miyake, Y., & Arakawa M. 2012, 'Smoking and prevalence of allergic disorders in Japanese pregnant women: baseline data from the Kyushu Okinawa Maternal and Child Health Study', Environmental Health, 11:15. [ Links ]
Thabethe N. D. L., Engelbrecht J. C., Wright C. Y., & Oosthuizen, M. A. 2014, 'Human health risks posed by exposure to PM10 for four life stages in a low socio-economic community in South Africa', The Pan African Medical Journal 18. [ Links ]
Tunno B.J, Shields K.N, Cambal L., Tripathy S., Holguin F., Lioy P., & Clougherty J.E. 2015, 'Indoor air sampling for fine particulate matter and black carbon in industrial communities in Pittsburgh,' Science of the Total Environment 536: 108-115. [ Links ]
Vanker A., Barnett W., Nduru P. M., Gie R. P., Sly P. D., & Zar H. J. 2015, 'Home environment and indoor air pollution exposure in an African birth cohort study', Science of the Total Environment 536: 362-367. [ Links ]
Verma T., Chimidza S., & Molefhi T. 2010, 'Study of indoor air pollution from household fuels in Gaborone, Botswana', Journal of African Earth Sciences 58:648-51. [ Links ]
Wernecke B., Piketh S. J., & Burger R. P. 2015, 'Indoor and outdoor particulate matter concentrations on the Mpumalanga highveld-a case study', Clean Air Journal 25:12-16. [ Links ]
WHO. 2014a, 'Global Burden of Diseases Due To Indoor Air Pollution', Available at: http://www.who.int/indoorair/health_impacts/burden_global/en/. [ Links ]
WHO. 2014b, 'WHO indoor air quality guidelines: household fuel combustion,' Geneva, Switzerland. [ Links ]
Wichmann J., & Voyi K. 2012, 'Ambient air pollution exposure and respiratory, cardiovascular and cerebrovascular mortality in Cape Town, South Africa: 2001-2006', International Journal of Environmental Research and Public Health, 9:3978-4016. [ Links ]
Wichmann J., & Voyi K. V. 2005, 'Air pollution epidemiological studies in South Africa: Need for freshening up', Reviews on Environmental Health, 20:265-302. [ Links ]
Wichmann J., & Voyi K. 2006, 'Influence of cooking and heating fuel use on 1-59 month old mortality in South Africa', Maternal and Child Health Journal, 10: 553-61. [ Links ]
Wylie B.J., Kishashu Y., Matechi E., Zhou Z., Coull B., Abioye A.I., Dionisio K.L., Mugusi F., Premji Z. & Fawzi W. 2017, 'Maternal exposure to carbon monoxide and fine particulate matter during pregnancy in an urban Tanzanian cohort', Indoor Air 27: 136-46. [ Links ]
Received: 18 March 2018
Reviewed: 10 June 2018
Accepted: 14 June 2018


{kind=link}
{kind=link}
{kind=link}
{kind=link}