










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Physiotherapy
On-line version ISSN 2410-8219
Print version ISSN 0379-6175
SAJPHYS vol.80 n.1 Cape Town 2024
http://dx.doi.org/10.4102/sajp.v80i1.1985
REVIEW ARTICLE
Bilateral versus unilateral upper limb training in (sub)acute stroke: A systematic and meta-analysis
Justine DembeleI, II; Lisa Tedesco TriccasI; Lisa Elogni Renaud AmanzonwéI, III; Oyéné KossiI, III, IV; Annemie SpoorenI
IREVAL, Faculty of Rehabilitation Sciences, Hasselt University, Diepenbeek, Belgium
IIDepartment of Rehabilitation, National Reference Centre of Physical Medicine and Rehabilitation, Ouagadougou, Burkina Faso
IIIUnit of Neurology and NeuroRehabilitation, University Hospital of Parakou, Parakou, Benin
IVENATSE, National School of Public Health and Epidemiology, University of Parakou, Parakou, Benin
ABSTRACT
BACKGROUND: Integrating high dosage bilateral movements to improve upper limb (UL) recovery after stroke is a rehabilitation strategy that could potentially improve bimanual activities
OBJECTIVES: This study aims to compare the effects of bilateral with unilateral UL training on upper limb impairments and functional independence in (sub)acute stroke
METHOD: Five electronic databases (PubMed, Scopus, PEDro, ScienceDirect, Web of Science) were systematically searched from inception to June 2023. Randomised controlled trials comparing the effect of bilateral training to unilateral training in stroke survivors (< 6 months poststroke) were included. The treatment effect was computed by the standard mean differences (SMDs
RESULTS: The review included 14 studies involving 706 participants. Bilateral training yielded a significant improvement on UL impairments measured by FMA-UE compared to unilateral training (SMD = 0.48; 95% CI: 0.08 to 0.88; P = 0.02). In addition, subgroup analysis based on the severity of UL impairments reported significant results in favour of bilateral UL training in improving UL impairments compared to unilateral training in "no motor capacity" patients (SMD = 0.66; 95% CI: 0.16 to 1.15; P = 0.009). Furthermore, a significant difference was observed in favour of bilateral UL training compared to unilateral UL training on daily activities measured by Functional Independence Measure (SMD = 0.45; 0.13 to 0.78; P = 0.006
CONCLUSION: Bilateral UL training was superior to unilateral training in improving impairments measured by FMA-UE and functional independence in daily activities measured by Functional Independence Measure in (sub)acute stroke
CLINICAL IMPLICATIONS: Bilateral upper limb training promotes recovery of impairments and daily activities in (sub)acute phase of stroke
Keywords: bilateral training; functions; rehabilitation; (sub)acute stroke; upper limb.
Introduction
Stroke remains the third-leading cause of death and disability combined in the world (Adoukonou et al. 2021; Feigin et al. 2022). Up to 80% of stroke survivors experience upper limb (UL) sensorimotor impairment at the (sub)acute stage, and few demonstrate complete functional recovery at 6 months post-stroke (Agbetou Houessou et al. 2021; Hayward et al., 2019; Kossi et al. 2016). The upper extremity is severely affected in 18% of cases (Persson et al. 2012), which leads to limitation in activities of daily living and reduction of quality of life (Sleimen-Malkoun et al. 2011).
Bilateral UL intervention after stroke involves practice of certain activities with both ULs to improve movement of the affected limb and includes both bilateral training (BT) with or without external assistance (Chen et al. 2019; Lee et al. 2017). Bilateral training includes repetitive practice of identical bilateral arm movements in symmetrical or alternating patterns and to bimanual training where both limbs perform different movements. A previous review and meta-analysis analysed the effect of BT compared to unilateral training on recovery of the UL after stroke (Chen et al. 2019). In a meta-analysis comparing the effects of bilateral and unilateral training, Lee et al. (2017) determined that constraint-induced movement therapy (CIMT) exercises were more effective than BT with regard to increased UL capacity (Lee et al. 2017).
At the neurophysiological and structural levels, the execution of bilateral movements post-stroke may facilitate cortical neural plasticity by these mechanisms: motor cortex disinhibition, increased recruitment of the ipsilateral pathways from the contralesional or contralateral hemisphere, upregulation of descending premotorneuron commands onto propriospinal neurons (Stinear et al. 2014) and interhemispheric interaction of affected and unaffected cerebral cortex (Latimer et al. 2010).
Due to neuroplasticity in the first 3 months after stroke (Stinear et al. 2020), this phase is therefore a critical window for experimental and restorative interventions to promote recovery after stroke (Overman & Carmichael 2014). Although previous meta-analyses compared the effect of BT and unilateral interventions, BT included various rehabilitation protocols, so BT alone has not been investigated separately. As a result, the previous analyses did not directly compare BT with unilateral training. To assess the effect of BT, it is important to compare different types of bilateral and unilateral training on the different levels of the International Classification of Functioning, Disability and Health (ICF), motor function levels, in both basic unilateral activities, and complex activities in which both hands are involved. Our study thus aimed to compare the effects of bilateral with unilateral UL training on UL impairments and functional independence in (sub)acute stroke, in a systematic review of the literature and meta-analysis.
Methods
This systematic review and meta-analysis was performed according to our protocol, registered in the international prospective register of systematic reviews, PROSPERO (https://www.crd.york.ac.uk/prospero/logout.php; registration N° CRD42021251028). Our study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Data sources and literature search
Five electronic databases (PubMed, Scopus, PEDro, ScienceDirect and Web of Science) were searched for relevant articles published in English or French from their inception until December 2022. An update was made to extend search to June 2023. To initiate the search, general keywords were first designed using core concepts: population (stroke), intervention, comparator and outcomes. A more detailed search strategy using combinations of key terms related to core concepts and their synonyms was also carried out. The search strategy was adapted to each database with combinations of keywords and Medical Subject Headings (MeSH) terms used as applicable. Published reviews and the reference lists of retrieved publications were searched manually in databases.
Study selection
After duplicates were removed, two reviewers independently examined the titles and abstracts of identified studies for relevance using EndNote X9 software. Full-text copies of potentially eligible studies were assessed and determined according to the following inclusion and exclusion criteria. Study selection was determined by consensus between reviewers, and rating was performed. Differences in scores were discussed until consensus was reached. When necessary, disagreements were resolved by consensus involving a third author.
The inclusion critera were randomised controlled trials (RCTs) published in English and French, involving acute and subacute (<6 months) stroke survivors (18) aged >18 years; investigating bilateral UL training like sensorimotor training, active and non-active movements; task-oriented training, strengthening and BT with or without a device, compared to unilateral training with or without a device; conventional therapy; neurodevelopmental therapy; conventional occupational or physiotherapy; electrical stimulation, to establish the effects of the interventions on UL function measured by the Fugl-Meyer Assessment for upper extremity (FMA-UE), the Wolf Motor Function Test (WMFT), Action Research Arm Test (ARAT), Box and Block Test (BBT) and the Functional Independence Measure (FIM).
Systematic reviews or meta-analyses, uncontrolled trials, clinical trials, quasi-randomised trials, case studies, stroke duration ≥ 6 months post-stroke, other neurological conditions apart from stroke and those with participants under 18 years of age were excluded. In addition, studies that did not provide data as mean scores and standard deviation (SD) of outcomes were excluded from the meta-analysis, and those not in line with the definition of the World Health Organization (WHO) pertaining to rehabilitation (WHO 2011) such as invasive and pharmacological interventions.
Risk of bias assessment
Two authors used the Cochrane risk of bias tool to assess the risk of bias in studies. This tool assesses the risk of bias in seven areas: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting and any other bias (Higgins et al. 2011).
Data extraction
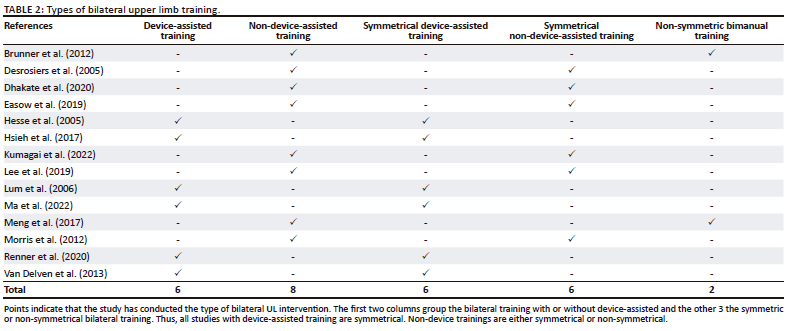
Two types of BT were considered in our review. The first category was bilateral UL training with device-assisted BT and non-device-assisted BT. The second category was symmetrical or non-symmetrical bilateral UL training. In symmetrical training, both ULs perform identical movements to manage a task. In non-symmetrical BT or tasks functional bilateral training, both ULs perform typically functional tasks, e.g. closing a box.
The most common definitions reported for dose dimensions of motor intervention include the duration of practice reflected by time spent in a therapy, schedule of therapy, for example, frequency of sessions and intensity level of task (Dalton et al. 2022; Hayward et al. 2021). The included studies were also classified into two subgroups according to the training dose: (group 1) total duration of training ≥ 20 h or a session length ≥ 5 h per week considered as a high dose; (group 2) total duration of training of < 19 h or a session length < 5 h per week considered as a low dose.
Upper limb impairment severity in the included studies was assigned based on the FMA-UE scores or ARAT at baseline. Fugl-Meyer Assessment for upper extremity scores of 0-22 or ARAT scores of 0-10 represent no capacity; FMA-UE scores of 23-31 represent poor capacity and match ARAT scores of 11-21; FMA-UE scores of 32-47 represent limited capacity and match ARAT scores of 22-42; FMA-UE scores of 48-52 represent notable capacity and match ARAT scores of 43-54; FMA-UE scores of 53 through 66 or ARAT scores 55-57 represent full capacity (Hoonhorst et al. 2015).
Data analysis
A meta-analysis was performed for the data synthesis using Review Manager Version 5.3 software, with a random effects model in which a p-value < 0.05 was considered significant. Effect size (ES) was estimated by calculating the standardised mean difference (SMD). The SMD reflects the intervention ES in each study relative to the variability observed in that study. An SMD of 0 means that the treatment and control have equivalent effects. Improvement is associated with higher scores on the outcome measure. Standardised mean differences >0 or <0 indicate the degree to which the treatment is more or less effective, respectively, compared to the control. Effect size was calculated based on means and standard deviations and on the sizes of the intervention and control groups. Heterogeneity was assessed using the results of the chi-squared test (significance level: p = 0.05) and the I2 statistic to quantify consistency. An I2 value of 50% or higher indicated the presence of substantial heterogeneity.
Ethical considerations
This systematic review and meta-analysis did not require formal ethical clearance because all data were obtained from publicly available sources and were analysed anonymously.
Results
Study selection
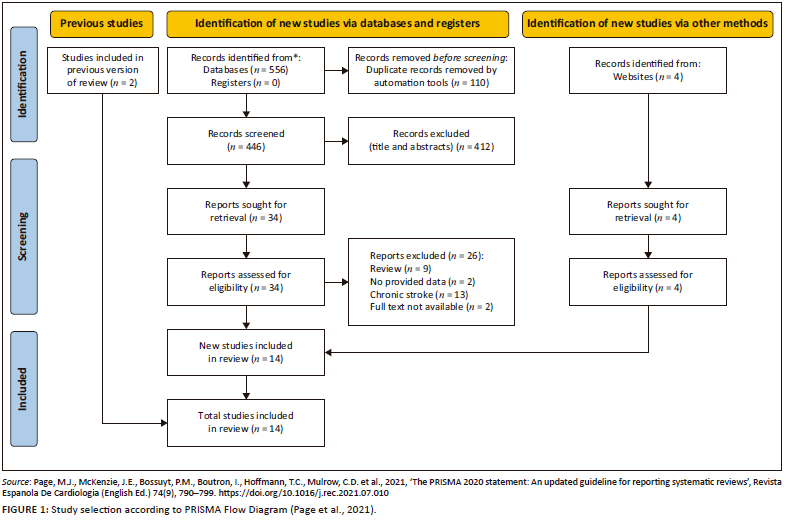
Figure 1 shows an overview of our selection strategy process. A total of 558 studies were selected through electronic databases, while four additional records were identified through other bibliographic sources. After removal of duplicates, screening of titles and abstracts and reviewing of full texts, 15 RCTs met the inclusion criteria for the qualitative analysis and 14 studies were included in the meta-analysis. One trial was excluded for meta-analysis because data were not available either publicly or from the authors (Burgar et al. 2011).
Study and participants characteristics
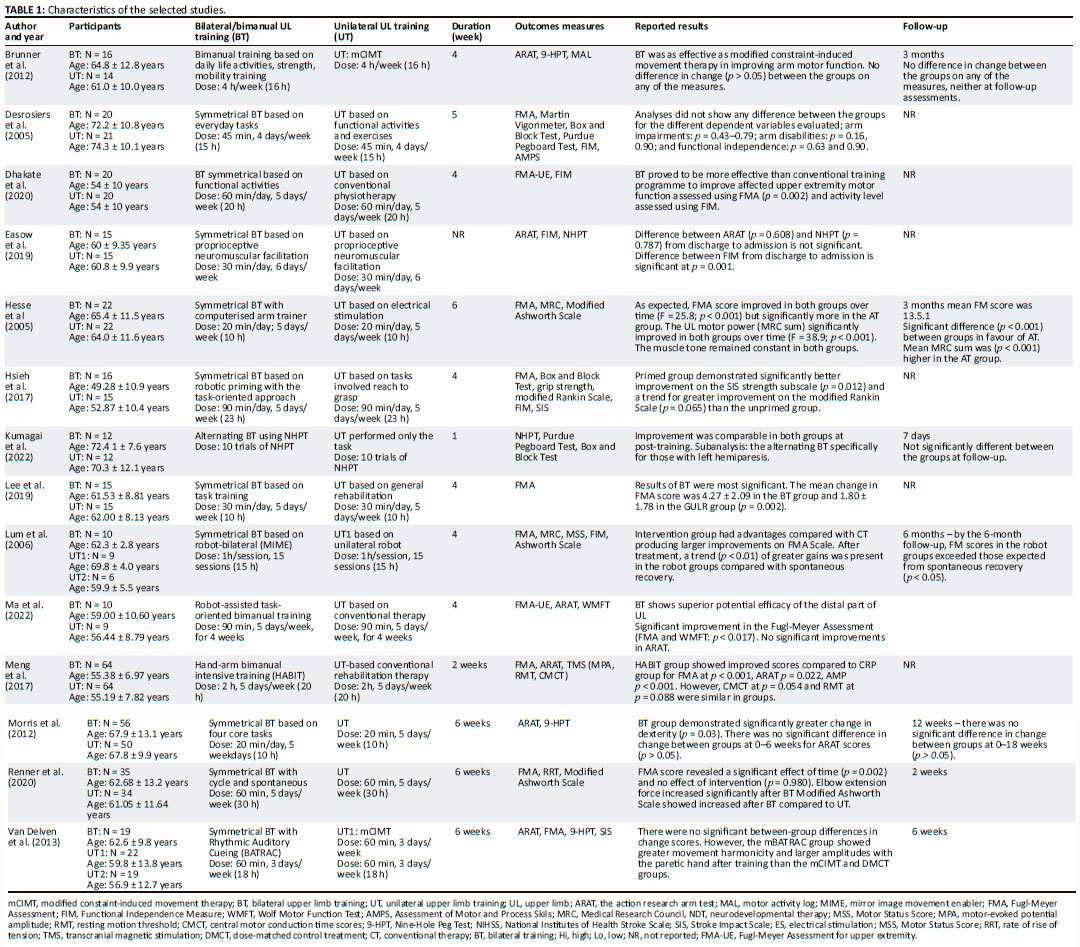
The main characteristics of the studies and participants in the 14 studies are shown in Table 1. A total of 706 participants were included with an age range from 49.3 to 74.3 years (SD from 2.0 to 13.22). Seven studies recruited patients with limited motor capacity with a FMA-UE score mean from 33 to 43 (Desrosiers et al. 2005; Dhakate & Bhattad 2020; Lum et al. 2006; Meng et al. 2017; Van Delden et al. 2015) or ARAT score mean 30 and 26 (Brunner, Skouen & Strand 2012; Easow & Chippala 2019); three other studies had participants with no motor capacity with a FMA-UE score mean from 6.6 to 17 (Hesse et al. 2005; Lee et al. 2017; Renner, Brendel & Hummelsheim 2020); in three studies, patients had poor motor capacity (Hsieh et al. 2017; Ma et al. 2022; Morris et al. 2008), and in one study, patients had notable capacity according to the aforementioned classification of severity above (Kumagai et al. 2022).
Table 2 gives the type of BT described in each included study. Most studies were symmetrical biliteral training without device assistance.
Content and dosage of intervention
The details of interventions and the control groups are provided in Table 2. Six studies explored the effects of bilateral device-assisted training on UL motor function after stroke. The control group was unilateral UL training, including conventional training, for example, neurodevelopmental therapy. Eight studies investigated BT without device-assisted and these were functional tasks training. Among these eight studies, six studies performed symmetrical BT and two studies performed non-symmetrical BT.
The total duration of the interventions was 10-30 h of BT for 2-6 weeks while the duration of a session varied from 20 min to 2 h, 3-6 times per week.
Risk of bias
Overall, 100% of studies presented low risk of bias with respect to random sequence generation, 64.29% with allocation and concealment, 14.29% with blinding of participants and personnel, 71.43% with blinding of outcome assessment, 28.57% with incomplete outcome data, 50% with selective reporting and 64.29% with other biases.
Effectiveness of bilateral versus unilateral training on upper limb impairments
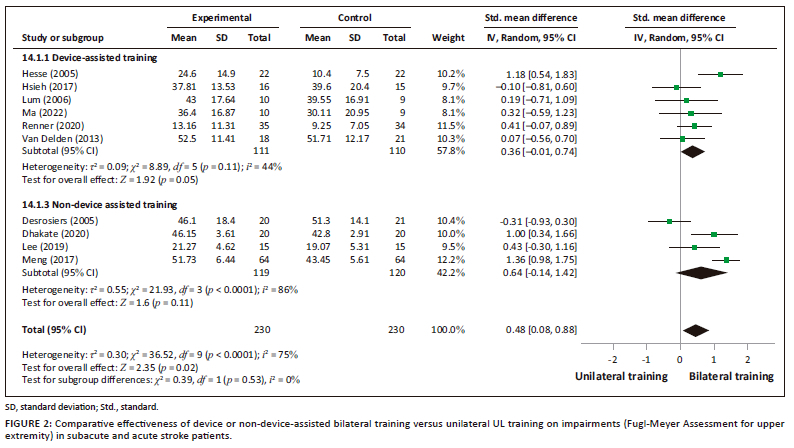
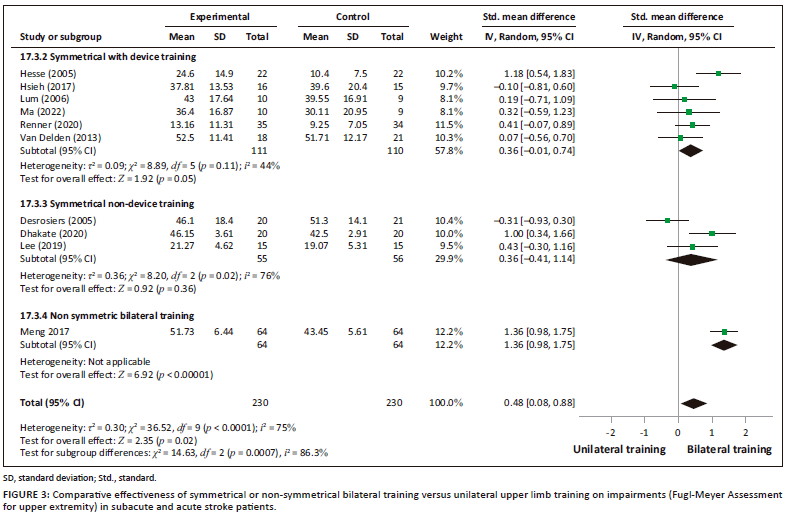
The results of the FMA-UE scores from 10 studies revealed a significantly improvement in favour of BT compared to the unilateral training group (SMD = 0.48; 95% CI: 0.08-0.88; p = 0.02) (Figure 2). However, high heterogeneity was present (I2 = 78%, p < 0.0001).
An analysis was performed according to the types of bilateral intervention on FMA-UE scores: device-assisted training and non-device-assisted training (Figure 2) and symmetrical with or without device training and non-symmetrical bimanual training (Figure 3). No significant improvements between bilateral UL training and unilateral UL training were observed in the analysis in terms of subgroups of interventions: bilateral device-assisted training (SMD = 0.36; 95% CI: −0.01 to 0.74) and bilateral non-device-assisted training (SMD = 0.64; 95% CI: −0.14 to 1.42). However, the results demonstrated significant improvement in favour of non-symmetrical BT (SMD = 1.36; 95% CI: −0.98, 1.75), but only one study was considered (Meng et al. 2017).
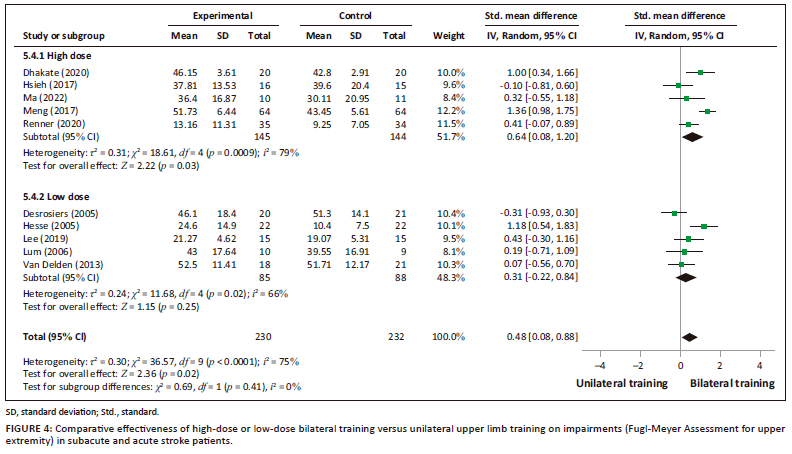
A subgroup analysis of high dose of FMA-UE scores showed significant effect (SMD = 0.64; 95% CI: 0.08-1.20; p = 0.03) but the low dose demonstrated no significant effect (SMD = 0.31; 95% CI: −0.22 to 0.85; p = 0.25) (Figure 4).
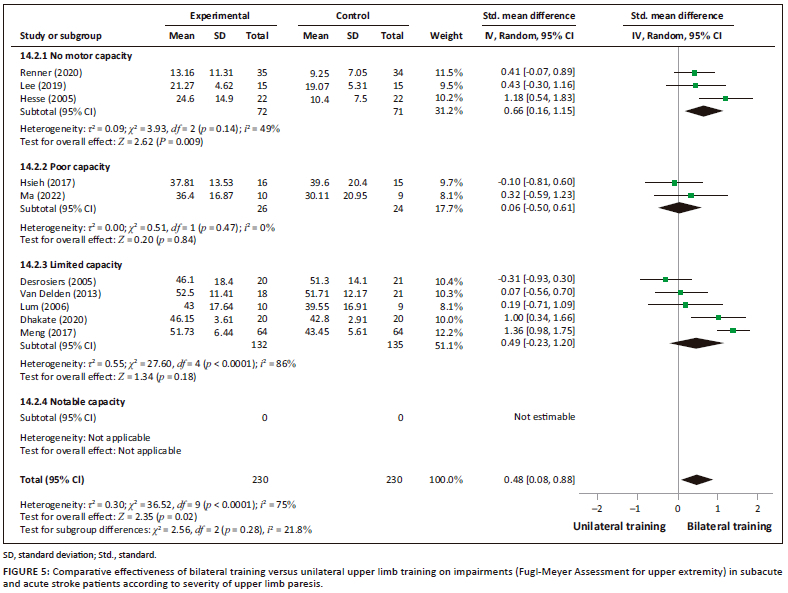
Three trials included in the subgroup of 'no motor capacity' reported significant results in favour of bilateral UL training in improving the UL impairments compared to unilateral training (SMD = 0.66; 95% CI: 0.16-1.15; p = 0.009). Two studies (Hsieh et al. 2017; Ma et al. 2022) with 'poor motor capacity' participants showed non-significant results (SMD = 0.06; 95% CI: −0.50 to 0.61). Five trials included in the subgroup of 'limited motor capacity' have also demontrated no significant improvement (SMD = 0.49, 95% CI: −0.23 to 1.20). The comparative effectiveness on impairment (FMA- UE) according to the severity of UL paresis is represented in Figure 5.
Effectiveness of bilateral versus unilateral training on upper limb activity limitations
The effects of bilateral UL training compared to unilateral UL training on activities analysed by the WMFT, ARAT and BBT scores of seven studies did not demonstrate significant improvement in overall effect of activities following a group of training (SMD = −0.09 points; 95% CI: −0.15 to 0.32). We observed homogeneity of studies (I2 = 34%, p = 0.17). The comparison revealed no significant difference in the analysis in terms of types of bilateral UL intervention compared to unilateral training. Based on dose of intervention and severity of UL paresis, the comparison between bilateral UL training and unilateral UL training showed no significant difference in the WMFT, ARAT and BBT scores.
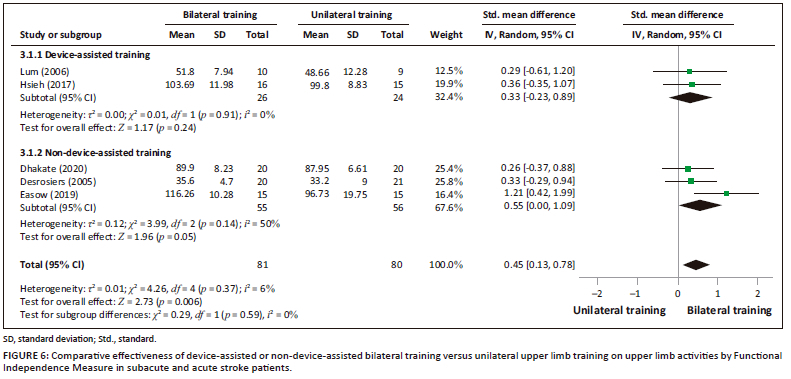
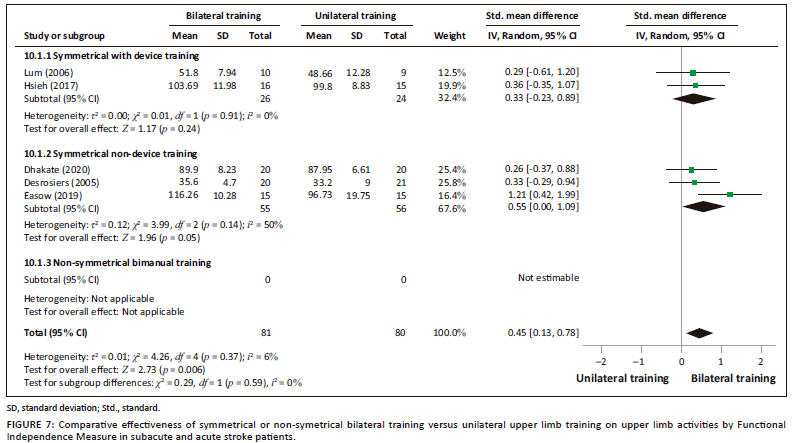
However, a significant difference was observed in favour of bilateral UL training compared to unilateral UL training in terms of improvement of daily activities measured by FIM (SMD = 0.45; 0.13-0.78; p = 0.006) (Figures 6, 7). There was homogeneity in the studies (I2 = 6%, p = 0.37).
Discussion
Our systematic review and meta-analysis aimed to compare the effectiveness of bilateral UL training with unilateral training on UL impairements and activities in acute and subacute stroke and to evaluate the influence of the types and dosage of BT and severity of UL paresis on UL recovery.
Our meta-analysis demonstrated that bilateral UL training is more effective than unilateral UL training in recovering of motor impairments measured by FMA-UE in (sub)acute stroke explored by 10 RCTs. Our results are similar to the results of Chen et al. (2019), who also reported significant improvement in overall FMA-UE scores in favour of BT in stroke patients (Chen et al. 2019). However, according to another meta-analysis, no significant differences were detected between BT and unilateral training for motor impairment (Chen et al. 2022). Currently, there are several types of UL BT in terms of content of intervention. Actually, all device training in our review was symmetrical, and we added an analysis of non-device training as symmetrical and non-symmetrical BT-based functional task training.
We have shown a significant improvement in UL impairment in favour of non-symmetrical BT compared to unilateral training. However, these findings should be interpreted with caution because the analysis was based on one study (Meng et al. 2017). Furthermore, the analysis shows that non-symmetrical training and training without technical assistance tend to have better improvement in UL activities measured by the WMFT, ARAT and BBT than unilateral training. As reported in other studies, repetitive bimanual movements can improve motor function promoting activity-dependent neuronal plasticity (Arya & Pandian 2014; Stinear et al. 2020). Regarding the positive effects of BT on motor function, several hypotheses have been proposed in the literature. Firstly, BT may promote positive neural interactions between sensorimotor areas in the ipsilesional and contralesional hemispheres to enhance coupling effects after stroke (Fan et al. 2015, 2016). Secondly, increased activity in sensorimotor areas after BT may contribute to functional reorganisation and neuroplasticity (McCombe Waller et al. 2014; Whitall et al. 2011). Thirdly, BT may restore normalised interhemispheric transcallosal inhibition (IHI) and reduce short-interval intracortical inhibition (SICI) in the ipsilesional hemisphere, both of which are associated with recovery of motor function after stroke (Swayne et al. 2008). Therefore, a higher dose of non-symmetrical BT could be further investigated so as to accurately highlight the effects on activities of daily living. In this field, more RCTs are needed to identify the optimal effect of BT based on functional tasks in UL activities post-stroke.
The significant improvement of motor impairments from BT was not accompanied by a greater improvement in UL activities as measured by the ARAT, WMFT and BBT compared to unilateral training. This is similar to two other systematic reviews (Chen et al. 2019; Coupar et al. 2010). Activity recovery is a very important goal for post-stroke patients in order to integrate the UL in daily activities (Nindorera et al. 2022). Daily activities sometimes require fine manipulation and some bimanual coordination. However, the majority of the included studies used analytical and symmetrical movements; in contrast, non-symmtrical bimanual movements with functional tasks were used less often. In addition, the lack of significant difference may be due to the outcome measures which were unimanual, yet the interventions were bilateral UL training.
Overall, as other studies did not report bimanual measures such as Adult Assisting Hand Assessment Stroke, it would be more appropriate that future interventions develop bilateral UL therapies focusing on functional tasks. In addition, they should include measuring tools that involve the use of both ULs, in a more natural situation in the activities of daily living. High scores on this tool can be obtained using only the nonparetic arm (Annabel 2018). However, the domains of self-care and transfers may require the use of both ULs. These two domains are composed of items based on activities of daily living performed by both ULs. Indeed, the items of this scale are based on bimanual activities of daily living in comparison with unilateral measures like WMFT and ARAT; thus, the practice of bimanual activities could have more impact in comparison with unilateral training. It is more likely that the greater improvement is due to the training of bimanual activities or bilateral activities. The need for more specific measures of bimanual activities is therefore necessary to support the conclusions of our review.
The dose of the training is important to reach functional recovery after stroke (Amanzonwé et al. 2023; Kossi et al. 2023; Nindorera et al. 2023). Interventions favouring intensive high repetitive task-specific training in all phases post-stroke have strong evidence for better results on motor function and activities (Veerbeek et al. 2014). With regard to subgroup analyses, our results showed that recovery of motor impairments can be favoured by intensive bilateral UL training in the acute and subacute stroke with at least 1 h of training, 5 times per week. Additional studies with bilateral task-oriented intervention, dimensions of dose articulation as proposed by Hayward et al. (2021) and long-term follow-up could provide more evidence on the effectiveness of motor function of the UL but are not reported. Chen et al. (2022) observed significant improvements in motor impairment in BT, when the dose of intervention was high.
Our analysis showed significant improvements for the subgroup of patients with 'no motor capacity' on pooled results of FMA-UE score for three studies. The effectiveness of bilateral UL training in patients with low motor capacity may be explained by the fact that patients use the two ULs and decrease intralateral inhibition in bilateral tasks when both hemispheres are activated (Stinear et al. 2020). The contribution of the healthy hand is therefore important in the management of patients after stroke (Van Gils et al. 2018). The healthy UL contributes to the movement of the injured side even with poor strength which allows a better recovery; however, in the unilateral UL training, it is difficult to do the training when the patient does not have a certain degree of motor strength. This training method could be further investigated in patients after acute and subacute stroke to support our results.
Strengths and limitations
A strength of our systematic review and meta-analysis is that it includes only studies with high-quality scientific evidence, namely RCTs. In addition, to the best of our knowledge, our review may be the first meta-analysis looking at the effect of types of bilateral UL training in acute and subacute stroke. A limitation of our systematic review and meta-analysis is the heterogeneity encountered among the studies and limited studies in some analysed subgroups. In addition, the search strategy was limited to full publications in English or French; therefore, relevant publications in other languages may have been missed.
Conclusion
Our systematic review and meta-analysis aimed to compare the effectiveness of bilateral with unilateral UL training in acute and subacute stroke. Our results noted that bilateral UL training was more effective in impairments, especially in the interventions with greater dose, severe impairment and on complex activities as measured by FIM. However, no significant effects were found on activities measured by ARAT, WMFT and BBT scores. The analysis of types of BT shows no significant difference between bilateral and unilateral training.
Acknowledgements
Competing interests
The authors have declared that no competing interest exists.
Authors' contributions
J.D. and O.K. contributed to the study design and conception.
All authors contributed substantially to the manuscript writing and revision.
J.D. and O.K. extracted data and analysed studies quality.
J.D. wrote the initial draft of the manuscript.
Funding information
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Data availability
The data that support the findings of this study are not openly available due to confidentiality and are available from the corresponding author, O.K., upon reasonable request.
Disclaimer
The views and opinions expressed in this article are those of the authors and are the product of professional research. It does not necessarily reflect the official policy or position of any affiliated institution, funder, agency, or that of the publisher. The authors are responsible for this article's results, findings, and content.
References
Adoukonou, T., Kossi, O., Fotso Mefo, P., Agbétou, M., Magne, J., Gbaguidi, G. et al., 2021, 'Stroke case fatality in sub-Saharan Africa: Systematic review and meta-analysis', International Journal of Stroke: Official Journal of the International Stroke Society 16(8), 902-916. https://doi.org/10.1177/1747493021990945 [ Links ]
Agbetou Houessou, M., Hountada, H., Yahouédéou, B., Choki, B., Kossi, O. & Adoukonou, T., 2021, 'Knowledge of stroke risk factors and signs in Parakou, a Northern City of Benin in West Africa', Cerebrovascular Diseases (Basel, Switzerland) 50(1), 88-93. https://doi.org/10.1159/000512715 [ Links ]
Amanzonwé, E.R., Tedesco Triccas, L., Codjo, L., Hansen, D., Feys, P. & Kossi, O., 2023, 'Exercise dosage to facilitate the recovery of balance, walking, and quality of life after stroke', The South African Journal of Physiotherapy 79(1), 1846. https://doi.org/10.4102/sajp.v79i1.1846 [ Links ]
Arya, K.N. & Pandian, S., 2014, 'Interlimb neural coupling: Implications for poststroke hemiparesis', Annals of Physical and Rehabilitation Medicine 57(9-10), 696-713. https://doi.org/10.1016/j.rehab.2014.06.003 [ Links ]
Brunner, I.C., Skouen, J.S. & Strand, L.I., 2012, 'Is modified constraint-induced movement therapy more effective than bimanual training in improving arm motor function in the subacute phase post stroke? A randomized controlled trial', Clinical Rehabilitation 26(12), 1078-1086. https://doi.org/10.1177/0269215512443138 [ Links ]
Burgar, C.G., Lum, P.S., Scremin, A.M.E., Garber, S.L., Van der Loos, H.F.M., Kenney, D. et al., 2011, 'Robot-assisted upper-limb therapy in acute rehabilitation setting following stroke: Department of veterans affairs multisite clinical trial', Journal of Rehabilitation Research and Development 48(4), 445-458. https://doi.org/10.1682/JRRD.2010.04.0062 [ Links ]
Chen, P.-M., Kwong, P.W.H., Lai, C.K.Y. & Ng, S.S.M., 2019, 'Comparison of bilateral and unilateral upper limb training in people with stroke: A systematic review and meta-analysis', PLoS One 14(5), e0216357. https://doi.org/10.1371/journal.pone.0216357 [ Links ]
Chen, S., Qiu, Y., Bassile, C.C., Lee, A., Chen, R. & Xu, D., 2022, 'Effectiveness and success factors of bilateral arm training after stroke: A systematic review and meta-analysis', Frontiers in Aging Neuroscience 14, 875794. https://doi.org/10.3389/fnagi.2022.875794 [ Links ]
Coupar, F., Pollock, A., Van Wijck, F., Morris, J. & Langhorne, P., 2010, 'Simultaneous bilateral training for improving arm function after stroke', The Cochrane Database of Systematic Reviews 2010(4), CD006432. https://doi.org/10.1002/14651858.CD006432.pub2
Dalton, E.J., Churilov, L., Lannin, N.A., Corbett, D., Campbell, B.C.V. & Hayward, K.S., 2022, 'Early-phase dose articulation trials are underutilized for post-stroke motor recovery: A systematic scoping review', Annals of Physical and Rehabilitation Medicine 65(1), 101487. https://doi.org/10.1016/j.rehab.2021.101487 [ Links ]
Desrosiers, J., Bourbonnais, D., Corriveau, H., Gosselin, S. & Bravo, G., 2005, 'Effectiveness of unilateral and symmetrical bilateral task training for arm during the subacute phase after stroke: A randomized controlled trial', Clinical Rehabilitation 19(6), 581-593. https://doi.org/10.1191/0269215505cr896oa [ Links ]
Dhakate, D. & Bhattad, R., 2020, 'Effectiveness of bilateral arm training on upper extremity motor function and activity level in patients with sub- acute stroke', International Journal of Current Research 12(20), 31-37. https://doi.org/10.31782/IJCRR.2020.122012 [ Links ]
Easow, A. & Chippala, P., 2019, 'Effects of bilateral upper limb task training on upper limb function in acute stroke: A randomized controlled trial', Indian Journal of Physiotherapy and Occupational Therapy - An International Journal 13, 218. https://doi.org/10.5958/0973-5674.2019.00164.3 [ Links ]
Fan, Y., Lin, K., Liu, H., Wu, C., Wai, Y. & Lee, T., 2016, 'Neural correlates of motor recovery after robot-assisted stroke rehabilitation: A case series study', Neurocase 22(5), 416-425. https://doi.org/10.1080/13554794.2016.1215469 [ Links ]
Fan, Y., Wu, C., Liu, H., Lin, K., Wai, Y. & Chen, Y., 2015, 'Neuroplastic changes in resting-state functional connectivity after stroke rehabilitation', Frontiers in Human Neuroscience 9, 546. https://doi.org/10.3389/fnhum.2015.00546 [ Links ]
Feigin, V.L., Brainin, M., Norrving, B., Martins, S., Sacco, R.L., Hacke, W. et al., 2022, 'World Stroke Organization (WSO): Global stroke fact sheet 2022', International Journal of Stroke: Official Journal of the International Stroke Society 17(1), 18-29. https://doi.org/10.1177/17474930211065917 [ Links ]
Hsieh, Y.-W., Wu, C.-Y., Wang, W.-E., Lin, K.-C., Chang, K.-C., Chen, C.-C. et al., 2017, 'Bilateral robotic priming before task-oriented approach in subacute stroke rehabilitation: a pilot randomized controlled trial', Clinical Rehabilitation 31(2), 225-233. https://doi.org/10.1177/0269215516633275 [ Links ]
Hayward, K.S., Churilov, L., Dalton, E.J., Brodtmann, A., Campbell, B.C.V., Copland, D. et al., 2021, 'Advancing stroke recovery through improved articulation of nonpharmacological intervention dose', Stroke 52(2), 761-769. https://doi.org/10.1161/STROKEAHA.120.032496 [ Links ]
Hayward, K.S., Kramer, S.F., Thijs, V., Ratcliffe, J., Ward, N.S., Churilov, L. et al., 2019, 'A systematic review protocol of timing, efficacy and cost effectiveness of upper limb therapy for motor recovery post-stroke', Systematic Reviews 8(1), 187. https://doi.org/10.1186/s13643-019-1093-6 [ Links ]
Hesse, S., Werner, C., Pohl, M., Rueckriem, S., Mehrholz, J. & Lingnau, M.L., 2005, 'Computerized arm training improves the motor control of the severely affected arm after stroke: A single-blinded randomized trial in two centers', Stroke 36(9), 1960-1966. https://doi.org/10.1161/01.STR.0000177865.37334.ce [ Links ]
Higgins, J.P.T., Altman, D.G., Gøtzsche, P.C., Jüni, P., Moher, D., Oxman, A.D. et al., 2011, 'The Cochrane collaboration's tool for assessing risk of bias in randomised trials', British Medical Journal (Clinical research ed.) 343, d5928. https://doi.org/10.1136/bmj.d5928 [ Links ]
Kim, S.H. & Park, J.H., 2019, 'The effect of occupation-based bilateral upper extremity training in a medical setting for stroke patients: A single-blinded, pilot randomized controlled trial', Journal of Stroke and Cerebrovascular Diseases: The Official Journal of National Stroke Association 28(12), 104335. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.104335 [ Links ]
Kossi, O., Batcho, C.S., Adoukonou, T. & Thonnard, J.-L., 2016, 'Functional recovery after stroke in Benin: A six-month follow-up study', Journal of rehabilitation medicine 48(8), 671-675. https://doi.org/10.2340/16501977-2128 [ Links ]
Kossi, O., Bonnechère, B., Agbetou, M., Somasse, R., Hokpo, A., Houehanou, Y.C.N. et al., 2023, 'Relationships between cardiorespiratory fitness, physical activity practices, and functional outcomes one-year post-stroke in northern Benin: A case-control study', Topics in Stroke Rehabilitation, 1-12. https://doi.org/10.1080/10749357.2023.2207286
Kumagai, M., Uehara, S., Kurayama, T., Kitamura, S., Sakata, S., Kondo, K. et al., 2022, 'Effects of Alternating Bilateral Training Between Non-Paretic and Paretic Upper Limbs in Patients with Hemiparetic Stroke: A Pilot Randomized Controlled Trial', Journal of Rehabilitation Medicine 54, jrm00336. https://doi.org/10.2340/jrm.v54.1970. [ Links ]
Latimer, C.P., Keeling, J., Lin, B., Henderson, M. & Hale, L.A., 2010, 'The impact of bilateral therapy on upper limb function after chronic stroke: A systematic review', Disability and Rehabilitation 32(15), 1221-1231. https://doi.org/10.3109/09638280903483877 [ Links ]
Lee, Y., Kim, M.Y., Park, J.-H. & Park, H.Y., 2017, 'Comparison of the effects of bilateral and unilateral training after stroke: A meta-analysis', NeuroRehabilitation 40(3), 301-313. https://doi.org/10.3233/NRE-161418 [ Links ]
Lum, P.S., Burgar, C.G., Van der Loos, M., Shor, P.C., Majmundar, M. & Yap, R., 2006, 'MIME robotic device for upper-limb neurorehabilitation in subacute stroke subjects: A follow-up study', Journal of Rehabilitation Research and Development 43(5), 631-642. https://doi.org/10.1682/JRRD.2005.02.0044 [ Links ]
Ma, D., Li, X., Xu, Q., Yang, F., Feng, Y., Wang, W. et al., 2022, 'Robot-Assisted Bimanual Training Improves Hand Function in Patients With Subacute Stroke: A Randomized Controlled Pilot Study', Frontiers in Neurology 13, 884261. https://doi.org/10.3389/fneur.2022.884261 [ Links ]
McCombe Waller, S., Whitall, J., Jenkins, T., Magder, L.S., Hanley, D.F., Goldberg, A. et al., 2014, 'Sequencing bilateral and unilateral task-oriented training versus task oriented training alone to improve arm function in individuals with chronic stroke', BMC Neurology 14(1), 236. https://doi.org/10.1186/s12883-014-0236-6 [ Links ]
Meng, G., Meng, X., Tan, Y., Yu, J., Jin, A., Zhao, Y. et al., 2017, 'Short-term efficacy of hand-arm bimanual intensive training on upper arm function in acute stroke patients: A randomized controlled trial', Frontiers in Neurology 8, 726. https://doi.org/10.3389/fneur.2017.00726 [ Links ]
Morris, J.H. & Van Wijck, F., 2012, 'Responses of the less affected arm to bilateral upper limb task training in early rehabilitation after stroke: a randomized controlled trial', Archives of Physical Medicine and Rehabilitation 93(7), 1129-1137. https://doi.org/10.1016/j.apmr.2012.02.025 [ Links ]
Nindorera, F., Nduwimana, I., Sinzakaraye, A., Bleyenheuft, Y., Thonnard, J.-L. & Kossi, O., 2022, 'Relationships between walking speed, activities and participation in people with chronic stroke in Burundi', The South African Journal of Physiotherapy 78(1), 1800. https://doi.org/10.4102/sajp.v78i1.1800 [ Links ]
Nindorera, F., Nduwimana, I., Sinzakaraye, A., Havyarimana, E., Bleyenheuft, Y., Thonnard, J.-L. et al., 2023, 'Effect of mixed and collective physical activity in chronic stroke rehabilitation: A randomized cross-over trial in low-income settings', Annals of Physical and Rehabilitation Medicine 66(4), 101704. https://doi.org/10.1016/j.rehab.2022.101704 [ Links ]
Overman, J.J. & Carmichael, S.T., 2014, 'Plasticity in the injured brain: More than molecules matter', The Neuroscientist: A Review Journal Bringing Neurobiology, Neurology and Psychiatry 20(1), 15-28. https://doi.org/10.1177/1073858413491146 [ Links ]
Page, M.J., McKenzie, J.E., Bossuyt, P.M., Boutron, I., Hoffmann, T.C., Mulrow, C.D. et al., 2021, 'The PRISMA 2020 statement: An updated guideline for reporting systematic reviews', Revista Espanola De Cardiologia (English Ed.) 74(9), 790-799. https://doi.org/10.1016/j.rec.2021.07.010 [ Links ]
Persson, H.C., Parziali, M., Danielsson, A. & Sunnerhagen, K.S., 2012, 'Outcome and upper extremity function within 72 hours after first occasion of stroke in an unselected population at a stroke unit. A part of the SALGOT study', BMC Neurology 12, 162. https://doi.org/10.1186/1471-2377-12-162 [ Links ]
Renner, C.I.E., Brendel, C. & Hummelsheim, H., 2020, 'Bilateral arm training vs unilateral arm training for severely affected patients with stroke: Exploratory single-blinded randomized controlled trial', Archives of Physical Medicine and Rehabilitation 101(7), 1120-1130. https://doi.org/10.1016/j.apmr.2020.02.007 [ Links ]
Sleimen-Malkoun, R., Temprado, J.-J., Thefenne, L. & Berton, E., 2011, 'Bimanual training in stroke: How do coupling and symmetry-breaking matter?', BMC Neurology 11, 11. https://doi.org/10.1186/1471-2377-11-11 [ Links ]
Stinear, C.M., Lang, C.E., Zeiler, S. & Byblow, W.D., 2020, 'Advances and challenges in stroke rehabilitation', The Lancet. Neurology 19(4), 348-360. https://doi.org/10.1016/S1474-4422(19)30415-6 [ Links ]
Stinear, C.M., Petoe, M.A., Anwar, S., Barber, P.A. & Byblow, W.D., 2014, 'Bilateral priming accelerates recovery of upper limb function after stroke: A randomized controlled trial', Stroke 45(1), 205-210. https://doi.org/10.1161/STROKEAHA.113.003537 [ Links ]
Swayne, O.B.C., Rothwell, J.C., Ward, N.S. & Greenwood, R.J., 2008, 'Stages of motor output reorganization after hemispheric stroke suggested by longitudinal studies of cortical physiology', Cerebral Cortex 18(8), 1909-1922. https://doi.org/10.1093/cercor/bhm218 [ Links ]
Van Delden, A.L.E.Q., Beek, P.J., Roerdink, M., Kwakkel, G. & Peper, C.L.E., 2015, 'Unilateral and bilateral upper-limb training interventions after stroke have similar effects on bimanual coupling strength', Neurorehabilitation and Neural Repair 29(3), 255-267. https://doi.org/10.1177/1545968314543498 [ Links ]
Van Gils, A., Meyer, S., Van Dijk, M., Thijs, L., Michielsen, M., Lafosse, C. et al., 2018, 'The adult assisting hand assessment stroke: Psychometric properties of an observation-based bimanual upper limb performance measurement', Archives of Physical Medicine and Rehabilitation 99(12), 2513-2522. https://doi.org/10.1016/j.apmr.2018.04.025 [ Links ]
Whitall, J., Waller, S.M., Sorkin, J.D., Forrester, L.W., Macko, R.F., Hanley, D.F. et al., 2011, 'Bilateral and unilateral arm training improve motor function through differing neuroplastic mechanisms: A single-blinded randomized controlled trial', Neurorehabilitation and Neural Repair 25(2), 118-129. https://doi.org/10.1177/1545968310380685 [ Links ]
 Correspondence:
Correspondence:
Oyéné Kossi
oyene.kossi@gmail.com
Received: 11 Sept. 2023
Accepted: 18 Oct. 2023
Published: 23 Jan. 2024


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}