










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkAfrican Vision and Eye Health
On-line version ISSN 2410-1516
Print version ISSN 2413-3183
AVEH vol.82 n.1 Cape Town 2023
http://dx.doi.org/10.4102/aveh.v82i1.859
ORIGINAL RESEARCH
Bedside teaching in optometry: A millennial view on an ancient teaching and learning method
Elzana KempenI; Mathys J. LabuschagneII; Mpho P. JamaIII
IDivision Health Sciences Education, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIClinical Simulation and Skills Unit, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
IIIDivision Student Learning and Development, Faculty of Health Sciences, University of the Free State, Bloemfontein, South Africa
ABSTRACT
BACKGROUND: Bedside teaching is a key component of a positive learning environment where non-technical skills and professional attributes can be taught. It is also one of the few ways to transfer professionalism: a core competency in a health science curriculum. This study investigated the experiences and perceptions of optometry students on bedside teaching to improve its effectiveness, and tailor it to the needs of the millennial generation students.
AIM: This study aimed to determine the experiences and perceptions of optometry students on bedside teaching (apprenticeship) during an ocular pathology clinic.
SETTING: The study was done at the Department of Optometry at the University of the Free State, South Africa.
METHODS: A qualitative case study was undertaken. All 17 final-year optometry students (N = 17) were invited to participate. Data were collected using an open-ended questionnaire. Content analysis was used to analyse the experiences and perceptions of the participants
RESULTS: Bedside teaching is a generally well-perceived experience from the student's perspective. The role of the supervisor was mentioned as the critical factor that facilitated learning, specifically learning by observing the application of theory and handling and treatment of the patient.
CONCLUSION: This study showed that millennial students perceived bedside teaching positively and provided valuable insights into this teaching and learning method in an undergraduate optometry clinical education setting. Experiential learning benefited these millennial students who prefer learning by observation.
CONTRIBUTION: A blueprint for the learning triad in bedside teaching is provided for optometry educators to apply this teaching and learning method successfully according to the needs of the current generation of students.
Keywords: bedside teaching; optometry education; clinical learning environment; millennial generation; qualitative research.
Introduction
Students in higher education are perceived as consumers who are actively involved in their learning. For this reason, it is imperative to investigate the effectiveness of a specific teaching and learning method and incorporate the students' perceptions and ideas on enhancing the chosen teaching and learning method and, ultimately, the overall learning environment.1 In alignment with this assertion, Johanson2 has expressed the need to determine the suitability of specific educational approaches to optimise teaching and learning strategies according to the needs of the millennial generation. Some of the needs include being part of a group, having access to quick answers, and having a stimulating environment where students do not become impatient and bored. Therefore, this further supports the need to investigate the effectiveness of some forms of teaching and learning, in particular, bedside teaching in a health science curriculum.
Students perceive bedside teaching as valuable and essential for learning skills related to effective communication, physical examination, clinical reasoning, and professionalism.3 Byszewski et al.4 state that students have identified bedside teaching as a vital component of a positive learning environment and the only way to transfer professionalism, which is one of the core competencies in a health science curriculum. Numerous studies on medical students' perceptions of bedside teaching focus on ward-round teaching.3,5 However, bedside teaching may be defined in multiple ways,6 and different teaching models that can be utilised are described in the literature.5 For example, apprenticeship, together with role modelling and ward-round teaching, are regarded as instructional models for managing bedside teaching that may be applied in an undergraduate optometry programme such as that of the University of the Free State (UFS). When the apprenticeship instructional model is applied in health sciences education, students are provided with an opportunity to build confidence through observing good practice. At the same time, ward-rounds allow students to see the physical signs of various diseases and conditions in actual patients,5 including patients with ocular pathology. In the optometry curriculum, where this study was conducted, bedside teaching or role modelling is practised throughout the clinical rotation by qualified optometrists supervising students during clinics. However, no studies have been conducted in South Africa to determine the perceptions of the current optometry students regarding bedside teaching, which is also an apprenticeship method.
The aim of the study was to determine the experiences and perceptions of undergraduate millennial optometry students on this teaching and learning method and make recommendations that may enhance learning in the clinical setting.
Theoretical perspectives
Sir William Osler introduced bedside teaching to medical training in the early 1900s.7 As one of the most popular role models in modern medicine, he only taught students at the bedside and showed them how to use all their senses when examining and managing a patient.7 Bedside or ward-based teaching, therefore, can be defined as clinical teaching carried out in the presence of a patient.3 Qureshi8 adds to this definition that it is a clinical teaching where patient-centred care is directly observed and learned. This teaching and learning method provides an optimal opportunity for students to learn clinical skills, clinical reasoning, communication skills, and interpersonal skills, as well as for educators to role model a holistic approach to patient care.5,9,10,11,12 Furthermore, in the late 1990s, Nair et al.7 emphasised that the bedside is the only site where history taking, physical examination, empathy, and a caring attitude can be taught and learnt by example. Ramani et al.13 also confirm this opinion and explain that these crucial elements of education for good patient care cannot be effectively accomplished in a classroom.
Apprenticeship and role modelling are seen as one of the teaching models for managing bedside teaching.5 The reasons for using an apprenticeship approach are threefold. Firstly, to role model, a holistic approach to patient care; secondly, to provide an opportunity to demonstrate a physical examination of a patient; and thirdly for the students to observe the protocol followed in a specific clinic.5 It also provides the supervisor with a valuable opportunity to teach professionalism and empathy as part of the hidden curriculum.13
Dent5 explains that the learning triad during this teaching and learning method comprises a patient, the student and the supervisor or tutor, which is a formula for an effective student learning experience. Patients are considered the cornerstone of this teaching and learning method.12 For the patient to be actively involved in the learning process, information about the session must be provided to them. The supervisor must ensure that the discussions during bedside visits and patient information shared with students will be confidential.13 Williams et al.3 caution that orienting the patient and explaining the purpose of the bedside encounter are important signs of respect not to be negated, as such actions will foster trust and cooperation. However, Chretien et al.14 warn that the examination of patients in the presence of the students may be experienced as an invasion of the personal space of patients, and the patients may very well be concerned about possible embarrassment and the risk of objectification. Even so, LaCombe9 stated that some patients enjoy being involved in this teaching and learning method. This feeling is confirmed by Peters and Ten Cate,15 who found that patients appreciated bedside teaching as they felt that extra time and special attention were given to their medical condition.
Although this teaching practice is considered one of the best in knowledge transfer, the teaching and learning environment must be conducive to learning, as students may feel intimidated by an unfamiliar environment. The tutor or supervisor should ensure that all students participate and that the anxiety a student may feel is allayed.5 A supervisor using good communication skills can make students feel secure by providing adequate demonstrations, explanations, and formative feedback.12 A study by Williams et al.3 found that students believe that simple reassurance from the facilitator is enough to alleviate their anxiety. Peters and Ten Cate15 also confirmed that when supervisors provide suitable guidance, students are more motivated to engage in clinical reasoning and problem-solving.
Context of this study
During the last year of the 4-year programme at UFS, South Africa, students take responsibility for patient management in the advanced speciality areas such as Pathology, Contact Lenses, Low Vision, Binocular Vision, and Paediatrics. Although bedside teaching (apprenticeship, internship, or traineeship) or role modelling is practised throughout the clinical rotation, during the pathology clinic, three apprenticeship sessions were explicitly scheduled for students to observe a supervisor examining and managing a patient from the case history until the management plan was discussed with the patient. Three students were assigned to a supervisor for the session. The supervisors assigned to these sessions were involved in the pathology clinic and the teaching of ocular pathology and had experience in the field of pathology. Williams et al.3 compiled a list of knowledge and skills acquired during bedside teaching. These knowledge and skills outcomes formed the objectives for the session, namely:
•obtaining a case history
•performing a physical examination
•performing diagnostic and therapeutic procedures
•acquiring knowledge about medical instrumentation
•generating a differential diagnosis
•formulating a management plan
•applying clinical reasoning
•communicating effectively
•exhibiting professional bedside demeanour
•demonstrating empathy.
Patients booked for this session were introduced to the supervisor and students and informed that the session would be a teaching encounter where the students would observe the supervisor performing an eye examination of someone with ocular pathology. The patients were also reassured that they could ask questions anytime during the examination to feel comfortable with the procedure.10
After the session, when the patient had left, the students had the opportunity to ask questions and time was provided to clarify aspects of uncertainty. A short debriefing session was held to ensure that there were no unresolved issues among the students.
Methods
The protocol for the study was approved by the Research Ethics Committee from the university at which the study was conducted. Written informed consent was obtained from the participants by the primary author. Information gathered during the questionnaire survey was given anonymously and no names or personal information could be linked to the information provided.
A qualitative case study approach was used for the study. An open-ended questionnaire that allowed for the perceptions and ideas of the participants to emerge was employed. Qualitative research stems from an interpretative paradigm16 and aims to understand aspects of life and the meaning people attach to life experiences.17 This research design was applied to this study as it typically strives towards describing, exploring, and understanding how each case exists holistically in its real-life context.
The sample population included all students enrolled in their fourth and final year in the undergraduate optometry programme at the UFS during 2017 (N = 17). Students were invited to complete the questionnaire to explore their experiences and perceptions of the teaching and learning method. The ages of the students were 21 (n = 11) and 22 (n = 6) and being born between 1996 and 1997 classified them as millennials.2
With the use of the questionnaire, the students were encouraged to engage in reflective practice. Gibbs' cycle of reflection was adapted for the questionnaire.18 Gibbs's reflective cycle has been linked to reflective practices within healthcare disciplines and builds on Kolb's experiential cycle by adding the important dimension of emotion.18 This reflective cycle focuses on including personal feelings and thoughts and recommendations for future actions. According to this cycle, a series of eight questions were presented to each participant. The eight questions from the existing literature were adapted for this study.19
Content analysis was used to provide knowledge, new insights, and a representation of facts to attain a full and condensed description of the students' experiences during the teaching and learning method. An inductive approach was followed to develop recommendations for implementing the specific teaching and learning method in the optometry programme at the UFS.20 This was carried out through the researcher's interaction with the data while discovering patterns, themes and categories.21
Ethical considerations
Ethical clearance to conduct this study was obtained from the University of the Free State Health Sciences Research Ethics Committee (HSREC) (No. HSREC 128/2016).
Results
The response rate for the questionnaire was 100% (N = 17). Four themes emerged after interrogating the data relating to the experiences and perceptions of the teaching and learning method. These themes, namely observational experience, personal feelings influencing the experience, supervisor as a role model and strengths and weaknesses, reflect the positive and negative factors that influenced the students' experience. For each theme, some recommendations made by the participants also emerged and are included in the results.
Theme 1: Observational experience
This teaching and learning method provided the participants with an observational experience. The practical observation of a professional at work was the main factor that enhanced the participants' learning and understanding:
'… I learn through seeing and hearing, so it was very insightful for me to go through the process.' (Participant 1, male, fourth-year student)
Participants mentioned that observing the supervisor handling a patient demonstrated the thinking process of the supervisor in a clinical environment. They also mentioned that the teaching and learning method allowed the observation of specific procedures that should be performed specifically on a pathology patient:
'What tests to do and how to do the tests by observing the method of a lecturer.' (Participant 12, female, fourth-year student)
While most of the participants concentrated on tests, some mentioned that bedside teaching included the demonstration of the handling and treatment of the patient, as confirmed with the statement:
'To get a better … way of thinking in approaching a pathology patient.' (Participant 5, female, fourth-year student)
Lastly, it also provided the opportunity to observe the flow of the specific clinic:
'We could observe how an optometrist handles a pathology patient and how they handle the flow of the entire clinic.' (Participant 11, female, fourth-year student)
As a result of students experiencing this observational experience as positive, they recommended that bedside teaching be implemented in all the specialised clinics for the final years and the general clinic in the third year. They felt it was an excellent way to prepare for the clinic and demonstrate what is expected from them. A participant even recognised the advantages for students and the improvement of patient care:
'Expand it to all the specialised 4th year clinics and before the 3rd year to see patients in the general clinic. This should help things get smoother with more self-confidence, students in better emotional conditions and, consequently, better care for each patient.' (Participant 10, female, fourth-year student)
Theme 2: Personal feelings influencing the experience
This theme elucidated participants' feelings, influencing the teaching and learning experience. The expressed feelings before, during and after the experience were primarily positive. The participants were excited to learn from the supervisor and see a patient with possible pathology. The participants also reported that they felt curious. They also felt reassured that they would be guided before examining a patient independently:
'I was excited to see my first pathology and to take tips on how examiners prefer to do techniques.' (Participant 2, male, fourth-year student)
'It was a reassuring thought that a supervisor would help us before seeing our first path patient without guidance.' (Participant 15, female, fourth-year student)
During the experience, participants felt inspired and interested while observing the supervisor testing a patient. They felt part of the experience and found the experience stimulating, informative, and helpful; thus, making them feel more at ease. During the experience, they also thought they could identify and improve their weaknesses.
The experience excited most participants as it prepared them to see a patient on their own. The experience also gave them self-confidence, and they felt better prepared emotionally; therefore, they felt they could care better for their patients. Other feelings mentioned were that they felt calmer, reassured, relieved, and informed:
'Satisfied as it showed me how certain conditions and characteristics present and also gives an idea of how to approach certain situations.' (Participant 2, male, fourth-year student)
'I now know more about how to approach and treat a pathology patient, and I feel more confident to see a real patient for the first time rather than just having only theoretical knowledge.' (Participant 5, female, fourth-year student)
A few participants before the experience observed feelings of uncertainty, discomfort, nervousness, and fear. These feelings were mainly because of the students not knowing what to expect:
'I felt a bit uncomfortable. My expectation was that it was going to be a session in which we are told everything that we are doing wrong instead of making us part of the process.' (Participant 1, male, fourth-year student)
Although no negative feelings were expressed during the experience, a couple of participants voiced negative feelings after the experience. They were disappointed because their patient did not present with any pathology:
'Afterwards, when the patient was diagnosed without pathology, I was disappointed. I did learn from the experience, but not as much as I had hoped.' (Participant 3, male, fourth-year student)
Recommendations made to improve on these negative feelings were to see more than one patient with different types of ocular pathology during the teaching and learning experience:
'Each group should have an opportunity to see two or more patients so that more pathology can be seen.' (Participant 14, female, fourth-year student)
It should also be ensured that a patient with ocular pathology is seen, as a participant stated that:
'A patient with more pathology (should be seen) to help us better deal better with challenges.' (Participant 16, female, fourth-year student)
Theme 3: Supervisor as a role model
The fact that the supervisors were friendly and helpful also contributed to the teaching and learning method's success. The participants expressed that they were allowed to ask questions when uncertain, and the supervisor explained everything without trying to catch them out and working together in a small group:
'I became more familiar with the evaluation process and glad that we could openly ask questions and also learn from other students' questions that I did not think of.' (Participant 5, female, fourth-year student)
Participants felt inspired and interested while observing the supervisor testing a patient:
'Inspired. It was very inspiring to see how the lecturer works with the patient and how much knowledge the lecturer has about the patient's condition.' (Participant 9, female, fourth-year student)
The supervisor's application of critical thinking, illustration of professionalism, and provision of good explanations of tests and how to apply time management were identified by participants:
'It helped a lot to see practically what someone does, how one thinks about things what you see or do not see, how to get to the final diagnosis and how to think critically.' (Participant 6, female, fourth-year student)
A participant provided recommendations for the lecturer and/or supervisor. These included the supervisor involving the students in the procedure and providing explanations or reasons for doing specific procedures. Also, to have an in-depth discussion about the management plan. The participant also stated that the supervisor should be prepared.
The participants also recommended repeating this experience with different eye-care professionals in the department. This will enable them to observe other methods of investigation and different ways to manage a patient.
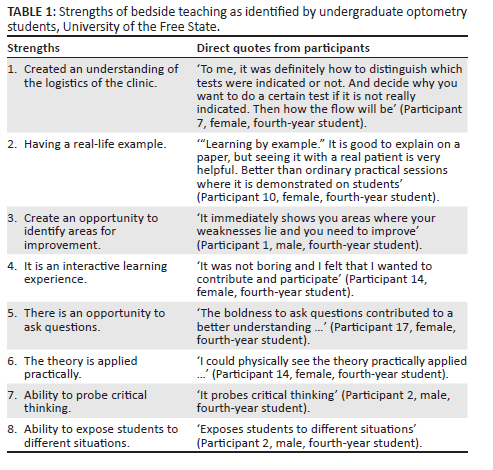
Theme 4: Strengths and weaknesses
The participants identified eight strengths of this teaching and learning method. These eight strengths, with direct quotes from the participants, on bedside teaching, are depicted in Table 1.
Three weaknesses emerged from the analysis of the data on this teaching and learning method. These weaknesses were:
1. Experience is limited to one patient or one condition only. Because of time constraints, this experience could only be illustrated on one patient with a possible condition. The participants identified this as a weakness and would have liked to be able to go through this experience with a variety of patients:
'The only weakness I can think of is that I would like an experience like this for each of the major conditions.' (Participant 2, male, fourth-year student)
2. The type of pathology differs for each group. Different groups saw different patients; therefore, the patient's conditions were not the same. The participants felt that this inconsistency affected their learning regarding the pathology. However, the nature of bedside teaching is the unpredictability of the case mix available for training:
'The type of patient you get determines how much you learn in terms of the degree of difficulty of the pathology.' (Participant 14, female, fourth-year student)
3. Patient is exposed. Some students felt that during this experience, the patient was exposed and mentioned that the patient should also be part of the evaluation instead of everyone just discussing the patient's condition:
'… it is not nice for the patient that everyone watches what is wrong with him or her and that everyone is talking about him or her.' (Participant 6, female, fourth-year student)
Discussion
Bedside teaching is a generally well-perceived experience from the students' perspective. The data indicated that clinical skills and reasoning were demonstrated during bedside teaching. Participants in this study noticed that they could observe an eye-care professional demonstrating conventional skills such as history taking, communication and physical examination, as well as the demonstration of the holistic approach to and treatment of a patient that includes compassion towards the patient. As a result, with this experience, the students were exposed to non-technical skills and professional attributes that, as Ramani et al.13 mentioned, cannot be taught in a classroom. In this study, the supervisors also took the opportunity to inform the students of the overall logistical functioning of the clinic, as it was the students' first exposure to a pathology clinic. That included the arrangement of the clinical notes and the administration that needs to be completed. This exposure ensured the students knew what was expected of them during the year, perhaps making them more comfortable in this clinic.
The success of bedside teaching was mentioned by all the participants, consistent with prior work in this field.4 Participants noticed that the experience was insightful and interesting and promoted critical thinking. The experience further contributed to their excitement and self-confidence to see patients independently. Millennial students benefit from experiential learning opportunities as it provides opportunities to reflect and reason.2 Three modes of Kolb's experiential learning cycle were applied in this teaching and learning method. Active experimentation would be implemented when the students started consulting patients independently. A significant result of the experiential learning cycle was that students who prefer to learn by observation might benefit significantly from this teaching and learning method. Further analysis showed that the strengths identified in this teaching and learning method also corresponded with the objectives of this method. The students felt that the clinic's functioning was practically and interactively illustrated as they were provided with a real-life example. They valued observing the supervisor applying the theory practically while evaluating and interacting with an actual patient.
The overwhelming feelings experienced by the students of this teaching and learning method were positive. The negative feelings brought up before the experience were on account of the uncertainty because it was something they had not experienced before. The students' recommendations indicate that the students did appreciate this teaching and learning method. A lot of the participants recommended implementing bedside teaching in all the specialised clinics in the fourth year and general clinics in the third year. They felt it was an excellent way to prepare for the clinic and demonstrate what is expected of them. The experience also gave them self-confidence, and they felt emotionally prepared to care better for their patients. The feelings expressed before, during and after the learning experience correspond with the millennial generation's characteristics, such as confidence, optimism, creativity, and collaboration.2
The findings of the questionnaire survey provide a valuable blueprint for the successful application of the components of the learning triad in bedside teaching, namely the patient, student, and supervisor.5 Figure 1 represents the learning triad with the essential key factors that emerged from the data of this study.
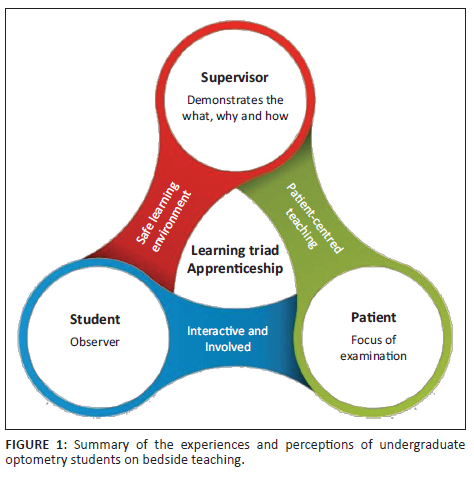
The role of the supervisor was mentioned several times right through the responses, and students identified the observation of the supervisor as the most critical factor that influenced their learning. Corresponding with the literature, the results also indicated that the supervisor seemingly played an essential role on the students' feelings that influenced the learning experience.3 It may be that the supervisors' friendliness and willingness to assist provided a sense of reassurance for the students, thus highlighting how essential it is for supervisors to create a safe learning environment at all times. It is also possible that this teaching and learning method was experienced as safe because the supervisor took responsibility for the treatment and management of the patient, and the students only had to observe and air their opinions. It appears that the students valued this 'learning without risks'. The millennial students embraced this teaching and learning method as they required frequent positive support from the supervisor throughout the experience.
The literature describes the patient as the foundation of the learning triad.12 Notably, students stated that more could be learned when the patient is presented with a pathology. To avoid disappointment, as was experienced by the students in this study, it should be emphasised that the goal should be patient-centred teaching, regardless of the diagnosis. As in a previous study by Chretien et al.,14 the students also mentioned that the patient was exposed. Therefore, care should be taken to inform the patient about the teaching experience, and the patient should provide consent for the supervisor to use them for the purpose of teaching. In this study, the patients were not asked to comment on the experience; therefore, their feelings were not included in the data.
It seems that students could take responsibility for their learning during this experience. In this learning triad of supervisor, patient, and student, the students felt it was their responsibility to participate in the experience, not the supervisor's duty to involve them. This highlights the view that students must realise their learning will be limited if they do not ask questions. Again, an environment should be created where students have the courage to ask questions or make comments without feeling exposed or foolish, and it appears as if the students in this study felt safe in the small group and learned from each other. Students also expressed the opinion that the experience might have been even better if they had reviewed the theory before coming to the clinic or brought textbooks or class notes with them. This might indicate that students have started to realise their responsibility in their learning.
Conclusion
In conclusion, the objective of this teaching and learning method analysed from the study's data agrees with the literature in that this teaching and learning method is clinical teaching where students can observe and learn patient-centred care directly from an example.
The participants recommended that this method be implemented more frequently in other clinics and that it should not be limited to one patient only. It is important to note that the apprenticeship model is applied throughout the year with supervisors rotating in clinical rooms. If the same format of the apprenticeship can be applied more than once, the students will be exposed to different patients and pathology. During this experience, the supervisors could only consult two patients each in the allocated time for the clinic, and two clinics were used for this experience. Unfortunately, because of the demands of service delivery in the public health sector, it might only be practical to repeat this experience once a year. This particular year group also comprised a small group of students; larger classes would put enormous strain on the supervisor and the functionality of the clinic, should this experience be implemented as recommended. Another possibility for utilising bedside teaching or role modelling more often would be to let the fourth year do the role modelling and allow the third year to sit in as an observer. The effectiveness of this recommendation should be, however, explored further.
To effectively apply the apprenticeship teaching and learning method for this generation of students the educator needs to emphasise the goal of patient-centred teaching, regardless of the diagnosis. Students also need the reassurance and suitable guidance with clear communication throughout the examination. To complete this observational teaching and learning method it is important to make time to incorporate an in-depth discussion on the management plan and reflection on the experience to answer any questions the students might have. From the results of this study, it can be concluded that bedside teaching in Optometry is still a valid and useful training method - even for the millennial generation.
Acknowledgements
This article is partially based on Elzana Kempen thesis entitled 'Experiential learning in the expanded scope of the undergraduate optometry programme at the University of the Free State' towards the degree of Philosophiae Doctor in Health Professions Education in the Division Health Sciences Education Faculty of Health Sciences at the University of the Free State on October 2020, with promoters M.J. Labuschagne and M.P. Jama.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
This study was done as a part of a thesis to obtain a PhD. E.K., M.J.L., and M.P.J in collaboration with the Health Professions Education (HPE), University of Free State were responsible for the conceptualisation and planning of the study. E.K. wrote the research protocol, collected the data, and also wrote the first draft of the article. M.J.L. was the study supervisor. M.P.J. was the co-supervisor of the study and contributed to editing the article. All the authors approved the final version of the article.
Funding information
This study was funded through a bursary by the Health and Welfare Sector Education and Training Authority (HWSETA).
Data availability
The data that support the findings of the study are available from the corresponding author, E.K., upon reasonable request.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors.
References
1.Orîndaru A. Changing perspectives on students in higher education. Proc Econ Financ. 2015;27:682-691. https://doi.org/10.1016/S2212-5671(15)01049-7 [ Links ]
2.Johanson L. Teaching the millennial generation: Considerations for nurse educators. Nurse Educ. 2012;37(4):173-176. https://doi.org/10.1097/NNE.0b013e31825a875a [ Links ]
3.Williams KN, Ramani S, Fraser B, Orlander JD. Improving bedside teaching: Findings from a focus group study of learners. Acad Med. 2008;83(3):257-264. https://doi.org/10.1097/ACM.0b013e3181637f3e [ Links ]
4.Byszewski A, Hendelman W, McGuinty C, Moineau G. Wanted: Role models - Medical students' perceptions of professionalism. BMC Med Educ. 2012;12(115):1-9. https://doi.org/10.1186/1472-6920-12-115 [ Links ]
5.Dent JA. Bedside teaching. In: Dent JA, Harden RM, Hunt D, editors. A practical guide for medical teachers. 3rd ed. Edinburg, New York: Elsevier Churchill Livinstone; 2009, p. 98-108. [ Links ]
6.Beckman T. A practical guide for medical teachers. Acad Med. 2004;79(4):343-346. https://doi.org/10.1097/00001888-200404000-00011 [ Links ]
7.Nair BR, Coughlan JF, Hensley MJ. Student and patient perspectives on bedside teaching. Med Educ. 1997;31(5):341-346. https://doi.org/10.1046/j.1365-2923.1997.00673.x [ Links ]
8.Qureshi Z. Back to the bedside: The role of bedside teaching in the modern era. Perspect Med Educ. 2014;3(2):69-72. https://doi.org/10.1007/S40037-014-0111-6 [ Links ]
9.LaCombe MA. On bedside teaching. Ann Intern Med. 1997;126(3):217-220. https://doi.org/10.7326/0003-4819-126-3-199702010-00007 [ Links ]
10.Salam A, Siraj HH, Mohamad N, Das S, Yousuf R. Bedside teaching in undergraduate medical education: Issues, strategies, and new models for better preparation of new generation doctors. Iran J Med Sci. 2011;36(1):1-6. [ Links ]
11.Peterson JA, Brommelsiek M. Interprofessional education to foster communication and resilience among health professional students. J Interprof Educ Pract. 2017;7:1-3. https://doi.org/10.1016/j.xjep.2017.01.001 [ Links ]
12.Garout M, Nugali A, Alhazmi A, Almoallim H. Bedside teaching: An underutilized tool in medical education. Intern J Med Educ. 2016;7:261-262. https://doi.org/10.5116/ijme.5780.bdba [ Links ]
13.Ramani S, Orlander JD, Struning L, Barber TW. Whither bedside teaching? A focus-group study of clinical teachers. Acad Med. 2003;78(4):384-390. https://doi.org/10.1097/00001888-200304000-00014 [ Links ]
14.Chretien KC, Goldman EF, Craven KE, Fasekus CJ. A qualitative study of the meaning of physical examination teaching for patients. J Gen Intern Med. 2010;25(8):786-791. https://doi.org/10.1007/s11606-010-1325-x [ Links ]
15.Peters M, Ten Cato O. Bedside teaching in medical education: A literature review. Perspect Med Educ. 2014;3(2):76-88. https://doi.org/10.1007/S40037-013-0083-Y [ Links ]
16.Cooper R, Fleischer A, Cotton FA. Building connections: An interpretative phenomenological analysis of qualitative research students' learning experiences. Qualitat Rep. 2012;17(17): 1-16. [ Links ]
17.Tavakol M, Sandars J. Quantitative and qualitative methods in medical education research. AMEE Guide No 90: Part II. Med Teach. 2014;36(10):838-848. https://doi.org/10.3109/0142159X.2014.915297 [ Links ]
18.Husebø SE, O'Regan S. Reflective practice and its role in simulation. Clin Simul Nurs. 2015;11(8):368-375. https://doi.org/10.1016/j.ecns.2015.04.005 [ Links ]
19.Burns N, Grove S. The practice of nursing research. Philadelphia: Elsevier Sounders; 2005. [ Links ]
20.Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2007;62(1):107-115. https://doi.org/10.1111/j.1365-2648.2007.04569.x [ Links ]
21.Patton MQ. Qualitative research and evaluation methods. Thousand Oaks, CA: Sage Publications; 2002. [ Links ]
 Correspondence:
Correspondence:
Elzana Kempen
kempene@ufs.ac.za
Received: 05 Apr. 2023
Accepted: 14 Aug. 2023
Published: 03 Nov. 2023

