










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.54 no.1 Pretoria Abr. 2024
http://dx.doi.org/10.17159/2310-3833/2024/vol54no1a10
RAPID REVIEW
Occupational therapy practice with burn injuries: A Rapid Review
Hester M van BiljonI; Madri EngelbrechtII; Janke van der WaltIII; Shaheed M SoekerIV
IWork-Link Vocational Rehabilitation Practice, South Africa. http://orcid.org/0000-0003-4433-6457
IICentre for Disability and Rehabilitation Studies, Department of Global Health, Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa. https://orcid.org/0000-0002-4606-7572
IIIDivision Occupational Therapy, Department of Health and Rehabilitation Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, South Africa. https://orcid.org/0000-0001-5012-0121
IVOccupational Therapy Department, University of the Western Cape, South Africa. https://orcid.org/0000-0001-5382-1855
ABSTRACT
INTRODUCTION: The Occupational Therapy Association of South African commissioned a task team to gather evidence that would inform upcoming National Health policies on the role and practice of occupational therapists. This rapid review aimed to identify level 1 and 2 peer reviewed published evidence that describes occupational therapists' practice and intervention in all types of burn injuries, at all levels of care, and for all age groups.
METHOD: Using the South African Department of Health template and the Cochran Rapid Reviews method guide, a search for level 1 and 2 evidence sourced articles from CINAHL (EBSCO), MEDLINE (EBSCO), the Cochrane Library (Wiley) and OTSeeker data bases through the Stellenbosch University library with hand searching of references in the selected articles. Rayyan was used for the screening and selection of articles. The CASP appraisal tool was used for risk bias and quality assessment of the selected articles. Data was captured in Excel and Word, and analysed and synthesised in Microsoft Excel and Taguette. Results were presented in the form of an online workshop to stakeholders and discussions and questions incorporated into the discussion and conclusion of this review.
RESULTS: Eleven articles were selected and their quality assessed. Seven categories of evidence of occupational therapy interventions were extracted from selected articles: pain, oedema, scaring and abnormal skin sensations, joints and range of motion, psycho-social and functional impact of burn injuries, the education of burn injury victims and their families, and vocational rehabilitation. All interventions took place in healthcare facilities. Nine articles referred to occupational therapists working in multi-disciplinary teams. Occupational therapist worked with children and adult burn injury victims and with a variety of type of burn injury from acute to post discharge phases
CONCLUSION: There is level 1 and 2 evidence confirming occupational therapy intervention with burn injury victims with all ages and at all stages of injury within healthcare facilities. None of the evidence found is from the South African context. Such levels of evidence are needed to promote occupational therapy intervention in primary, preventative and community contexts.
IMPLICATIONS FOR PRACTICE:
Internationally there is level 1 and 2 evidence that confirms occupational therapists are members of multi-disciplinary teams addressing the functional ability and participation in activities of burn injury victims. None of this evidence is from South Africa. As a matter of priority, South African clinical occupational therapy practice and intervention within the field of burn injury, need to be researched and disseminated as level 1 and 2 evidence.
Keywords: intersectoral burn injury intervention, multidisciplinary rehabilitation, pressure garment, splinting, systematic review, randomised control trail, psychosocial functioning, occupational engagement
INTRODUCTION
A burn injury is an injury to the skin or other organic tissue, caused by heat, radioactivity, electricity, friction or chemical contact1. Burn injuries are a global public health problem and most burn injuries occur in the home or workplace. Living in low- and middle-income countries (LMICs) puts people at greater risk for burn injuries than those in high-income countries (HICs) and burn risk correlates with socioeconomic status. High risk population groups for burn injuries are females, children under the age of 5 and older adults. In South Africa, where inequality is among the highest in the world, more than half of the population live below the country's designated upper-middle-income poverty line2 and burns in this population group are seen as a major public health issue, responsible for a significant amount of long term disability3. A literature review on rehabilitation practices for burns survivors in low and middle income countries4 calls for research to investigate undocumented burn rehabilitation services.
The World Health Organisation (WHO) constitution states that "health is a state of complete physical, mental and social well-being" and that "the enjoyment of the highest attainable standard of health is one of the fundamental rights of every human being without distinction of race, religion, political belief, economic or social condition"5:1. This ethos is also enshrined in the South African Constitution6 and, with a specific focus on rehabilitation, in the National Rehabilitation Policy (NRP)7. This policy emphasises the creation of equitable, accessible and quality rehabilitation services for all in South Africa, describing the components of rehabilitation as: prevention and health education, identification and diagnosis, medical rehabilitation and therapeutic devices, education, assistive devices, vocational rehabilitation and psychosocial rehabilitation7. A position paper focusing on the role of occupational therapy within rehabilitation the Occupational Therapy Association of South Africa (OTASA)8, positions occupational therapy rehabilitation as the link between healthcare and the resumption of daily occupations. The latter brings purpose, meaning and satisfaction in life and allows the realisation of potential8. To achieve such ideals, legislation9 and strategies such as the National Health Insurance (NHI)10 were effected and associations representing rehabilitation professions, were approached to provide evidence for best practice. For occupational therapy practices to be recognised and remunerated, an evidence base that is contextually relevant and that has been informed by high quality research is important11.
In order to provide evidence for best practice, OTASA commissioned the development of standard operating procedures (SOPs) and operationalised a task team of occupational therapists to compile level 1 and 2 evidence in the form of rapid reviews to support and inform the SOPs. Level 1 and 2 evidence, as described by Burns et al.12, is evidence produced in the form of systematic reviews and randomised control trials (RCT) . To produce a summary of such evidence for stakeholders. Garritty et al.13. suggests the use of a rapid review. This rapid review has a specific focus on occupational therapy intervention offered for burn injuries, and excluded review of effectiveness of different interventions. Three documents were used to inform the planning, analysis, synthesis, reporting format of the results, discussion and conclusion, namely the WHO's information document on burn injuries1, the South African rehabilitation policy7 and the OTASA's burns SOP14.
Summary of the focus for this rapid review
This rapid review was aimed at identifying level 1 and 2 peer reviewed published evidence that describes occupational therapy intervention for all types of burns injuries at all levels of healthcare and for all age groups.
METHOD
The OTASA rapid review task team consisted of the four authors, all of them occupational therapists. They met on a weekly basis to ensure consistency and uniformity in approach. The South African Department of Health method guide and template for rapid reviews15 and the Cochran Rapid Reviews method guide13 were used to inform the methodology for this rapid review. The first author and principal researcher for this review, was assisted by the other authors during all phases of the review. The time frame in which this rapid review was completed was January 2023 to May 2023.
Search strategy
Step 1: Topic and review refinement
The OTASA Rapid Review Task Team and authors of the OTASA SOP were stakeholders involved in setting and refining the review question, eligibility criteria and outcome. The review question formulated was: What burn injury related Level 1 and 2 evidence exists for occupational therapy intervention across the human lifespan?
The following population, intervention and outcome (PIO) elements were discussed and considered for the review: Population: A human being, from all age, gender and cultural groups, who had sustained a burn injury, for which intervention at any setting or level of healthcare is needed and/or sought with a referral to occupational therapy. Intervention: Any form of occupational therapy as per the WFOT and OTASA definition and the OTASA Burns SOP14,16,17. Outcomes: Occupational therapy intervention that enables persons whose functional ability is affected by burn injuries, enhancing their ability to engage in the occupations they value, want to, need to, or are expected to do, or modifying the occupation or environment to better support their occupational engagement.
Step 2: Strategy and search
Evidence considered for this review included systematic reviews and RCTs written in English, peer reviewed, published between January 2012 - May 2023 and that were accessible to the review team as full texts. Three of the reviewers had access to the Stellenbosch University library where the following data bases were searched by the first author, on13 March 2023: CINAHL (EBSCO), MEDLINE (EBSCO), the Cochrane Library (Wiley) and OTSeeker. A hand search of the references of articles that were selected after screening, was then undertaken.
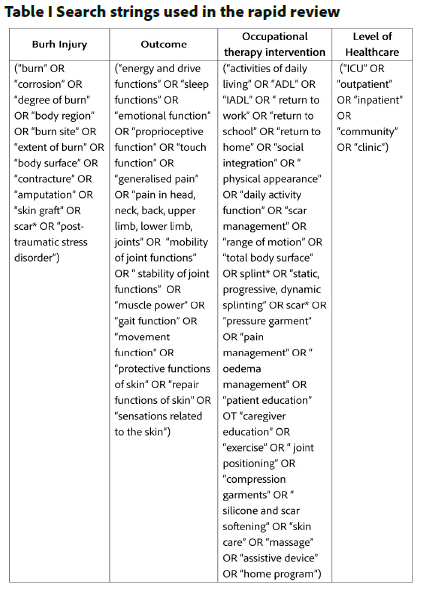
The OTASA Burns SOP document14, Medical Subject Headings (MeSH), key and index words with Boolean operators and the Participant, Intervention, Outcome (PIO) were used during an iterative group checking process, to develop the search string shown in Table I (page 89).
In addition, the following database-specific restrictors were used:
• CINAHL (EBSCO): Date, Language and Full Text availability: 9 articles were found. Adding "occupational therap*": 42 articles were found including the previous 9. Adding "randomised control trial" OR "RTC" and "systematic review": produced nothing.
• MEDLINE (EBSCO): "occupational therap*" AND "burn*", the date range, language, Linked Full Text, Abstract available, Human, All sex, All clinical, Scholarly (Peer Reviewed) Journals, All ages, All subject subsets: 35 articles were found.
• Cochrane Library (Wiley): Applying the date, All Text and the above search string showed no results. Adding "occupational therap*" AND "burn*" still had no results.
• OTSeeker advanced search option was used with the date range and the Burns, resulted in 10 articles.
The 42 articles from CINAHL, 35 articles from MEDLINE, and 10 articles from OTSeeker were downloaded into the reference manager Mendeley18 which removed 14 duplicates. From hand-searching references of the 73 articles, four articles were found relevant and added to the final evidence pool of 77 articles.
Step 3: Study Screening and Selection
Rayyan19 software was used to screen articles and generate a PRISMA flow diagram (Figure 1 adjacent). Two of the authors, used the blinded setting to screen the articles and conflicts were resolved by discussion and consensus. Title and abstract screening excluded 63 articles and full text screening a further three, resulting in 11 articles being included for the review.
Step 4: Risk of bias assessment, quality appraisal and data extraction
The first author created data extraction templates in Excel and Word to extract quantitative and qualitative data from the included articles. The Critical Appraisal Skills Programme (CASP)20,21 appraisal tool, which offers healthcare professional various checklists to check the quality of articles, was used. The CASP Systematic Review20 and the CASP RC20 checklists were applied in this rapid review. The quality rating indicated in Table III (page...) was devised by allocating scores to the three answer options: Yes = 2, Can't tell = 1, and No = 0. A higher rating percentage indicated higher quality research. Comments were noted during the appraisal and considered in the discussion section of this review.
Step 5: Evidence Synthesis
Quantitative data were analysed in Excel predominantly with frequencies/percentages. The qualitative data were analysed using Taguette22. During weekly group discussions the results of the analysis were reported and discussed. Final synthesis of the results was done by the first author.
Step 6: Reporting and dissemination of results
The results of the rapid review were presented in the form of an online workshop with 274 attendees. The workshop was organised by OTASA for stakeholders who included the OTASA membership, OTASA management and members of the Health Professions Council of South Africa (HPCSA) board. Discussion, questions and feedback from attendees were encouraged. These were considered and used to enrich and refine the review's discussion and conclusion.
RESULTS
The PRISMA 2020 diagram23, Figure 1 (below), shows the results of the search, screen and selection of burn related evidence for occupational therapy.
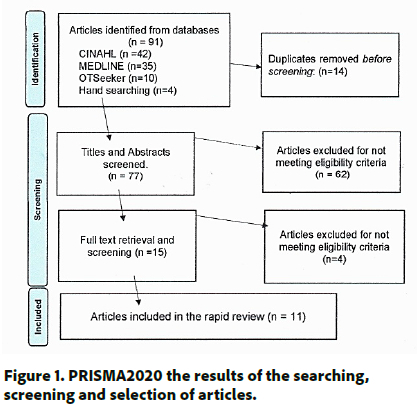
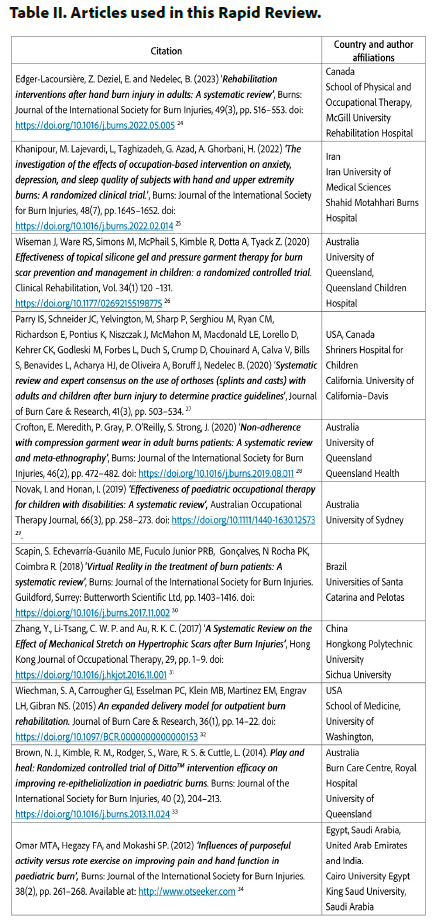
Table II (below) lists the 11 included articles, in order of year of publication. There were deve randomised control trials (RCT's) and six systematic reviews. All articles had a university affiliation and were published in high impact journals hosted by publishing companies and that had 'pay-to-publish' policies. None of them were from South Africa. Only one author had an African affiliation. Four of the articles were from Australia, three from North America and one from South America. There was one article from Iran, one from China and one article reported a multi-national collaboration.
Quality appraisal
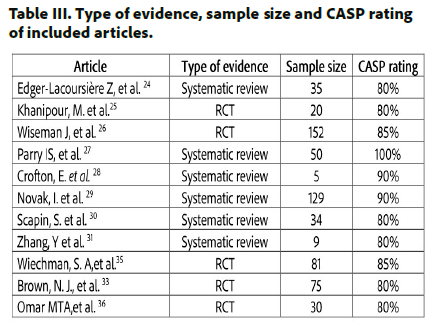
The results of the Critical Appraisal Skills Programme (CASP) Randomised Controlled Trial Standard checklist21 and Systematic Review checklist20 for the articles ratings expressed in percentage are presented in Table III (below). The sample size of each article reported the number of participants, if it was a RCT and the number of articles included if it was a systematic review.
Occupational therapy interventions reported
The articles provided evidence for occupational therapy involvement with the management of pain, oedema, scarring, abnormal skin sensation, joints and range of motion, psycho social issues, the functional impact of burn injury, the education of burn injury victims and their families and vocational rehabilitation. In some article's, tools, tests, equipment, and specific approaches that occupational therapists used during their intervention were also mentioned.
Occupational therapists were involved in pain management of burn injury victims specifically through play therapy and virtual reality. The use of play therapy with children with burn injuries showed better outcomes in terms of pain reduction, improvement of total active movement and hand function than those achieved using rote exercises34. Using virtual reality games and devices within this context was reported in several studies. The DittoTM (hand held education & distraction device for burns patients) device proved to be a worthwhile tool for paediatric pain management and as an adjunct to pharmacological analgesia therapeutic wound care procedures33. Virtual reality goggles were also used effectively for adjunctive pain control during occupational therapy in paediatric burn injury patients30. Occupational therapists used the following tools to rate the pain of service users with burn injuries: Adolescent Paediatric Pain Tool30, Numeric Pain Rating Scale (NPRS)30, Faces Pain Scale30, 34, Face, legs, activity, cry, consolability (FLACC)30, Wong-Baker faces30, Pain Behaviour Scale30, Visual analogue scale34 and the Children Trauma Screening Questionnaire26.
Oedema, scar and skin sensation management were reported occupational therapy interventions. The use of compression (adhesive compressive wrap, compression bandage or intermittent compression pump) to decrease hand oedema and increase hand function24 was reported. Elevation exercises, reversible massage, compression bandages and passive mobilization were used to reduce oedema that caused pain, maintain proper positioning and prevent deformity that affected function34,24. Intervention related to scarring was comprehensively reported with passive and active stretching being one of the most commonly used therapeutic techniques for scar management by both physiotherapists and occupational therapists31. Massage and splinting after burn injuries were defined as conservative scar management techniques used by occupational therapists31. Topical silicone gel and pressure garment therapy were interventions used for the prevention and management of abnormal post-burn scarring in children26, adults28 and to reduce hand scar thickness24. With burn injures, the experience of itch and pain is grouped into the category of sensory factors. Individuals overwhelmed by sensory information may experience stress and anxiety, and may engage in avoidance behaviours28. Occupational therapists' concern about the impact of such sensory factors on function was also reported. Therapists therefore also provided patients with strategies to deal with discomfort caused by pressure garment wear which included: adjusting and replacing the garments, massage and relaxation techniques38.
Occupational therapy outcomes for increased joint range of motion and the prevention of contracture management were achieved predominantly though splinting, casts and positioning24,27,34. The use of virtual reality, paraffin wax and massage to increase passive range of motion in the hand before engagement in activities of daily living was reported as an effective occupational therapy intervention24,30. Occupational therapy also incorporated the use of virtual reality-based rehabilitation to increase hand function and hand strength24. Play and games which reduce pain, improve hand movement and function as well as being reusable and versatile, are suggested options in the rehabilitation of children with a hand burn injury36. Hand function was measured using: Jebsen-Taylor hand function test (JTHFT) Michigan Hand Outcomes Questionnaire (MHQ), Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire, ergometer for range of motion of thumb IP joint, hydraulic dynamometer and pinch gauge36,24.
Occupational therapy in addressing psychosocial interventions were also reported in seven of the articles. These included chronic pain due to burns, scarring and the wearing of pressure garments which affected mental health, led to sleep deprivation, feelings of unattractiveness and lowered self-esteem and social acceptance34,35,28. Occupation-based interventions were reported to be effective in improving the anxiety, depression, and sleep quality in patients with hand burn injuries and were used to facilitate a sense of power and well-being in burn injury victim25. One of the occupation-based interventions used was the Cognitive Orientation to daily Occupational Performance (CO-OP) which proved effective in enabling the ability to perform meaningful activities and to reintegrate into society for patients with hand and upper extremity burns25. This protocol, along with traditional occupational therapy rehabilitation, proved an effective intervention on improving anxiety, depression, and sleep quality25. Virtual reality technology used during rehabilitation was associated with increased enjoyment, the reduction of pain, anxiety and stress30. Ditto™ provides procedural distraction and self-management education with a reduction of pain and anxiety being achieved in acute paediatric and adult burn injury victims33,29. Tests and tools used to assess psychosocial components were the Beck Anxiety Inventory (BAI), Self-Rating Depression Scale (SDS) and the Pittsburgh Sleep Quality Index25.
Patients with burn injuries reported reduced participation in activities of daily living, or an inability to fulfil premorbid roles24. Functional limitations caused by burn related injuries or resulting therapy were attended to by occupational therapists28,34. They did so through facilitation and adaptation of activities of daily living, including the provision of adaptive equipment, such as ADL universal cuffs and auxiliary tableware, and providing instructions for their use24. Interventions such as pressure garments however, were reported to cause restriction in homemaking, personal hygiene, shopping, leisure activities, and use of transportation28. The Canadian Occupational Performance Measure (COPM) was used to determine occupational performance level and satisfaction25. Quality of life and activities of daily living (ADL) was measured using: Barthel Index (BI)35, Functional Independence Measure (FIM)27, Burns Specific Health Scale-Brief (BSHS-B)24.
Occupational therapists applied an education component in their rehabilitation to increase the level of burn knowledge in their patients and their care givers24. Collaboration with parents of children with burn injuries was found to be an effective occupational therapy intervention29. It was also found that education, feedback, practical and emotional support from occupational therapists could aid adherence to the wearing of pressure garments28.
Vocational rehabilitation intervention by occupational therapists in the form of an outpatient work-hardening programme was reported as effective. The work hardening programme was a 4-6-week programme, including physical reconditioning, job simulation, education, and evaluation and monitoring of work-related behaviours and attitudes. Hours of participation were graded weekly, with the 1st week requiring 4 hours a day to 8 hours a day in the final week24. The Valpar 9 whole body range of motion work sample test was used to evaluate the outcome35.
All interventions of the randomised control trials and those systematic reviews that did mention the setting were reported to take place in healthcare facilities. These included burn units or centres in general hospitals34,33, outpatient departments35-26, children hospitals35, and specialised burns centres and hospitals25-35. No mention was made of occupational therapists working in communities, places of employment, schools or patients' homes. Nine of the 11 articles mentioned occupational therapist working in multidisciplinary teams.
Occupational therapists were reported to work with children26 and the following age categories were specified: 4-12 years33, 8-14 years34. They also worked with adults who had burn injuries and only one article reported biographic information; 18-65 years25. The types of burns which were reported, were hand and upper extremity burns34,24,2S, acute burn stage26 33, superficial and deep partial and full thickness thermal burns34 second to third degree burns25, hypertrophic scars causedby burns31 and burn injuries which had been skin grafted22,23.
DISCUSSION
Rehabilitation is included in the WHO definition of comprehensive healthcare5, and is positioned within preventive, promotive, curative and palliative care37 but remains poorly understood by healthcare managers and workers in South Africa38. A reasonable deduction, based on the small amount of published evidence found in this rapid review, is that rehabilitation specifically focused on burn injury rehabilitation and narrowed down even more to occupational therapy intervention, is in dire need of evidence to inform healthcare managers for planning of future healthcare systems.
Guided by the South African rehabilitating policy7 and the OTASA standard operating procedure for burn injuries14 the following three sectors of intervention were used in the discussion of the results of this review: prevention intervention, in- and outpatient intervention, and community intervention.
Primary Prevention intervention is to prevent impairment or disability from arising, to reduce the degree of disability and to reduce or address social disadvantage arising from a burn injury. None of the articles provided evidence of occupational therapy primary prevention intervention. This is of concern in the light of the World Health Organisation's plan for burn injury prevention and care notes and the United Nations Sustainable Development Goals39.
In- and outpatient intervention are offered when the service user goes to the occupational therapist at a healthcare facility. Intervention in such facilities requires the identification of disability or impairment with the aim of providing rehabilitation intervention. Interventions are aimed at limiting or arresting the effects of impairment or disability allowing service users with burn injuries to regain functional abilities, continue development, and enjoy quality life.
Community intervention entails the occupational therapist providing services outside of the health care facility to the service user. Such intervention is usually to follow-up, to assist and guide users and relevant role players in social and or economic wellbeing, and developing educational levels and/ or vocational skills and aptitudes for them to access places and participate in activities they value within communities of their choice. The OTASA position statement on rehabilitations states that in addition to facility-based rehabilitation programmes, occupational therapists are committed to community-based rehabilitation (CBR). Another concern is that there was no evidence to support occupational therapy burn injury interventions in the community while, in South Africa, taking rehabilitation to those who need it, is a key strategy to ensure equitable access to quality health care. Such a strategy should address social integration of people with disfiguring injuries or disabilities which is often the case with burn survivors. The development of rehabilitation programmes or services at community level should be given high priority to ensure the implementation of strategies that aim to educate and increase awareness about preventing common diseases and injuries which frequently cause disability, for example, hypertension, diabetes, burn injuries, road accidents7,39.
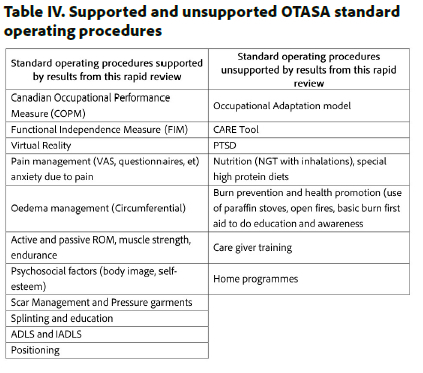
The OTASA SOP document which outlines14 South African occupational therapists' intervention with burn injuries was in a draft format at the time of this review, however it clearly lays out interventions, tools, tests and stages of rehabilitation. Many of these were supported by the evidence from this review but not all. Table IV (below) shows the detail of what procedures were and were not supported by evidence reported in this rapid review.
Investigating the current occupational therapy research focus areas in South Africa, Soeker et al.11 found that there was a scarcity of level 1 research evidence, across all fields of practice. They recommended that university research committees develop Think Tanks of academics, clinicians and communities to plan research focus areas. The education of under- and post-graduate occupational therapy students should also emphasise the development and of level 1 research methods and skills. They also addressed the need for research funding and awards to prioritise South African level 1 evidence research projects in occupational therapy.
Limitations of the study
The eligibility criteria of articles for this rapid review, namely level 1 and 2 evidence and peer reviewed articles published after 2012, ruled out published research done in South Africa and therefore articles that reported contextually relevant evidence related to the review question.
Gatekeeping of access to scientific evidence, mostly by large for-profit publishing companies, is a global concern. The pay-to-read or pay-to-publish concept favours large institutions, the rich and/or those fortunate enough to be affiliated with tertiary academic institutions. This excludes smaller non-profit groups, from scientific evidence. Due to the authors' affiliations with Stellenbosch University and the University of the Western Cape, access could be gained to repositories paid for by these two institutions. but this evidence may not be readily available to occupational therapy clinicians to guide their practice.
Future research and other recommendations
Evidence from levels 3 and 4 research should be considered. Systematic reviews and randomised control trials are types of research that presupposes a high level of academic experience and are expensive and time-consuming. Unfortunately, this is the evidence requested by authorities to set prescribed minimum benefits and finance health intervention. Graham et al40 supports this recommendation. They concur that conventional research methods, including randomized controlled trials, are powerful techniques for determining the efficacy of interventions. However, these designs, have practical limitations in many rehabilitation settings and they also suggest the consideration of available alternative methods.
Clinical researchers need to be enabled, supported and incorporated into research teams that generate evidence of occupational therapy intervention in burn injuries.
Research task teams should be established with specific directives to find, consolidate and publish evidence to fill the gaps identified in this review, namely occupational therapy intervention for prevention of burns-related disability, and community-based occupational therapy interventions for burn injuries in South Africa.
Ethical considerations
Ethical clearance was not required for this review as no primary data collection was done. The quality and bias of selected articles were tested to ensure quality results to inform thequestion of this review.
CONCLUSION
There is international level 1 and 2 evidence that confirms occupational therapy burn injury intervention with pain, oedema, scarring and abnormal skin sensation, joints and range of motion, psycho social, functional impact of burn injuries, the education of burn injury victims and their families and vocational rehabilitation. In addition, evidence shows that occupational therapists work with children and adults who had suffered burn injuries.
The South African National Rehabilitation Policy acknowledges that policymakers and funders, both nationally and provincially, have historically regarded rehabilitation as a low priority or an unaffordable luxury7. The reasons for this are complex and multi-faceted. In the case of burn rehabilitation, one of these facets is the absence of South African occupational therapy evidence that supports what clinicians do in the field of burn injury. Publishing evidence for practice should be a priority. Such evidence should start at preventing disability and impairment and include intervention in community rehabilitation. It should importantly include the clinical intervention of community service and basic level occupational therapists, those working with limited experience, resources and support at the coalface of rehabilitation.
Acknowledgements
The team would like to acknowledge Stellenbosch University (SU), the SU library and SU occupational therapy departments who assisted, encouraged and enabled the access to evidence used in this rapid review. We also acknowledge the Chief Operating Officer of OTASA, Anisha Ramlaul, for her vision, organising of the workshop and patience in this project. Without their support this review would not have been possible.
Conflicts of Interest
The authors have no conflict of interest to declare
Author contributions
Shaheed M. Soeker initiated and supervised the rapid review. All authors planned and participated in the review. Hester van Biljon wrote the article, which was approved by all listed authors.
REFERENCES
1. World Health Organisation. Burns. Fact Sheet, https://www.who.int/news-room/fact-sheets/detail/burns (2018). [ Links ]
2. The World Bank IBRD + IDA. The World Bank in South Africa. #AFRICA CAN. Epub ahead of print 2023. https://www.worldbank.org [ Links ]
3. Cloake T, Haigh T, Cheshire J, et al. The impact of patient demographics and comorbidities upon burns admitted to Tygerberg Hospital Burns Unit, Western Cape, South Africa. Burns 2017;43:411-416. https://doi.org/10.1016/j.burns.2016.08.031 [ Links ]
4. Jagnoor J, Lukaszyk C, Fraser S, et al. Rehabilitation practices for burn survivors in low and middle income countries: A literature review. Burns 2018; 44: 1052-1064. https://doi.org/10.1016/j.burns.2017.10.007 [ Links ]
5. World Health Organization. Constitution of the World Health Organization.49,Geneva,2020. [ Links ]
6. The Republic of South Africa. The Constitution of the Republic of South Africa, 1996. Republic of South Africa 1996; 1-182. [ Links ]
7. Republic of South Africa, Tshabalala-Msimang M. REHABILITATION FOR ALL. National Rehabilitation Policy. November 2000. GovernmentPublishers,Pretoria,2000. [ Links ]
8. OTASA. Occupational Therapy Association of South Africa Position Statement on Rehabilitation. South African J Occup Ther 2017;47:63-64. [ Links ]
9. South African Government. National Health Act 61 of 2003. SouthAfrica,2003. [ Links ]
10. National Department of Health. White Paper: National Health Insurance Policy - Towards Universal Health Coverage. Dep Heal 2017;1-67. [ Links ]
11. Soeker M, Olaoya O. Determining the research priorities for the profession of occupational therapy in South Africa. South African J Occup Ther 2023;53:6-7. [ Links ]
12. Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plast Reconstr Surg 2011; 128:305-310.doi:10.1097/PRS.0b013e318219c171 [ Links ]
13. Garritty C, Gartlehner G, Kamel C, King VJ, Nussbaumer-Streit B, Stevens A, Hamel C AL. Cochrane Rapid Reviews. Interim Guidance from the Cochrane Rapid Reviews Methods Group. 2020. [ Links ]
14. Pillay R, Flieringa H, Powell N. OTASA Burns Rehabilitation Standard Operating Protocol for Occupational Therapy. OTASA,Pretoria,2023. [ Links ]
15. South Africa Department of Health. METHODS GUIDE FOR RAPID REVIEWS FOR COVID-19 MEDICINE REVIEWS. 2021. [ Links ]
16. WFOT. WFOT Definition of Occupational Therapy, https://wfot.org/resources/definitions-of-occupational-therapy-from-member-organisations (2012). [ Links ]
17. OTASA. Occupational Therapy Association of South Africa: Where do occupational therapists work, https://www.otasa.org.za/about-otasa/#:~:text=WhatisOccupationalTherapy (OT, thea ctivities of everyday life. (2023). [ Links ]
18. Mendeley Ltd. Mendeley Reference Manager. Elserivier 2020; https://www.mendeley.com/reference-management/mend. [ Links ]
19. Rayyan Sytems I. Rayyan Intelligent Systematic Review. Rayyan https://rayyan.qcri.org [ Links ]
20. Critical Appraisal Skills Programme. CASP Systematic Review, http://creativecommons.org/licenses/by-nc-sa/3.0/www.casp-uk.net (2018). [ Links ]
21. Critical Appraisal Skills Programme. CASP Randomised Control Trial, http://creativecommons.org/licenses/by-nc-sa/3.0/www.casp-uk.net (2021). [ Links ]
22. Rampin R, Rampin V, DeMott S. Taguette Version 0.10.1. hi@taguette.org 2020; BSD-3-Clause license, [ Links ] ©.
23. Page M, McKenzie J, Bossuyt P, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ Open; 372. Epub ahead of print 2021. https://doi.org/10.1136/bmj.n71 [ Links ]
24. Edger-Lacoursière Z, Deziel E, Nedelec B. Rehabilitation interventions after hand burn injury in adults: A systematic review. Burns 2023; 49: 516-553. https://doi.org/10.1016/j.burns.2022.05.005 [ Links ]
25. Khanipour M, Lajevardi L, Taghizadeh G, et al. The investigation of the effects of occupation-based intervention on anxiety, depression, and sleep quality of subjects with hand and upper extremity burns: A randomized clinical trial. Burns 2022; 48: 1645-1652. https://doi.org/10.1016/j.burns.2022.02.014 [ Links ]
26. Wiseman J, Ware RS, Simons M, et al. Effectiveness of topical silicone gel and pressure garment therapy for burn scar prevention and management in children: a randomized controlled trial. Clin Rehabil 2020; 34: 120-131. https://doi.org/10.1177/0269215519877516 [ Links ]
27. Parry IS, Schneider JC, Yelvington M, et al. Systematic review and expert consensus on the use of orthoses (splints and casts) with adults and children after burn injury to determine practice guidelines. J Burn Care Res 2020; 41: 503-534. https://doi.org/10.1093/jbcr/irz150 [ Links ]
28. Crofton E, Meredith P, Gray P, et al. Non-adherence with compression garment wear in adult burns patients: A systematic review and meta-ethnography. Burns 2020; 46: 472-482. https://doi.org/10.1016/j.burns.2019.08.011 [ Links ]
29. Novak I, Honan I. Effectiveness of paediatric occupational therapy for children with disabilities: A systematic review. Aust Occup Ther J 2019;66:258-273. https://doi.org/10.1111/1440-1630.12573 [ Links ]
30. Scapin S, Echevarría-Guanilo ME, Boeira Fuculo Junior PR, et al. Virtual Reality in the treatment of burn patients: A systematic review. Burns 2018; 44: 1403-1416. https://doi.org/10.1016/j.burns.2017.11.002 [ Links ]
31. Zhang Y, Li-Tsang CWP, Au RKC. A Systematic Review on the Effect of Mechanical Stretch on Hypertrophic Scars after Burn Injuries. Hong Kong J Occup Ther 2017; 29: 1-9. https://doi.org/10.1016/j.hkjot.2016.11.001 [ Links ]
32. Wiechman SA, Carrougher GJ, Esselman PC, et al. An expanded delivery model for outpatient burn rehabilitation. J Burn Care Res2015;36:14-22.https://doi.org/10.1097BCR.0000000000000153 [ Links ]
33. Brown NJ, Kimble RM, Rodger S, et al. Play and heal: Randomized controlled trial of DittoTM intervention efficacy on improving re-epithelialization in pediatric burns. Burns 2014; 40: 204-213.https://doi.org/10.1016/j.burns.2013.11.024 [ Links ]
34. M. T. A. Omar FAH and SPM. Influences of purposeful activity versus rote exercise on improving pain and hand function in pediatric burn. Burns 2012;38:261-268. [ Links ]
35. Wiechman SA, Carrougher GJ, Esselman PC, Klein MB, Martinez EM, Engrav LH GN. An expanded delivery model for outpatient burn rehabilitation. J Burn Care Res 2015; 36: 14-22. https://doi.org/10.1097/BCR.0000000000000153 [ Links ]
36.Omar MTA, Hegazy FA, Mokashi SP. Influences of purposeful activity versus rote exercise on improving pain and hand function in pediatric burn. Burns 2012; 38: 261-268. https://doi.org/10.1016/j.burns.2011.08.004 [ Links ]
37. World Health Organization. Rehabilitation. Newsroom, 2020, p. https://www.who.int/news-room/fact-sheets/detail [ Links ]
38. Sherry K. Disability and rehabilitation : essential considerations for equitable, accessible and poverty-reducing health care in South Africa. South African Heal Rev 2014; 2014/2015: 89-99. https://hdl.handle.net/10520/EJC189294 [ Links ]
39. United Nations. Global Sustainable Development Report (GSDR) 2023. Geneva, Switzerland, https://www.worldbank.org (2023). [ Links ]
40. Graham J., Karmarkar A., Ottenbacher K. Small sample research designs for evidence-based rehabilitation: issues and methods. Arch Phys Med Rehabil 2012; 93: 2384. https://doi.org/10.1016/j.apmr.2011.12.017 [ Links ]
 Correspondence:
Correspondence:
Hester M. van Biljon
Email: HesterMvanBiljon@gmail.com
Submitted: 9 July 2023
Reviewed: 1 October 2023
Revised: 13 October 2023
Accepted: 13 October 2023
Editor: Blanche Pretorius:https://orcid.org/0000-0002-3543-0743
Funding: The Occupational Therapy Association of South Africa (OTASA) who requested the authors to do this rapid review, remunerated them.

