










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.54 n.1 Pretoria Apr. 2024
http://dx.doi.org/10.17159/2310-3833/vol54no1a8
RESEARCH ARTICLE
Perceptions on transitioning from impairment-based to occupation-based practice in public healthcare within KwaZulu-Natal
Phana Lucy GumedeI, II,; Chantal Juanita ChristopherII; Deshini NaidooII
IUntumjambili District Hospital, Kranskop, KwaZulu Natal, South Africa. https://orcid.org/0009-0009-1916-8915
IIDiscipline of Occupational Therapy, School of Health Sciences, University of KwaZulu Natal. Chantal Juanita Christopher: https://orcid.org/0000-0002-4959-7288. Deshini Naidoo: https://orcid.org/0000-0001-6276-221X
ABSTRACT
INTRODUCTION: Holistic healthcare service delivery requires rehabilitation personnel to consider all the components of health that influence the client's quality of life. However, there is limited literature on approaches to implementing rehabilitation services within South African public healthcare. This study explored rehabilitation personnel's (such as occupational therapists, speech therapists, physiotherapists) use of occupation-based practice impairment-based practice and the barriers and facilitators associated with their practice choice.
METHODS: A qualitative research design was conducted through semi-structured interviews (13 participants), a focus group (4 participants) and community mapping. Purposive sampling was utilised to select participants in the iLembe district, KwaZulu-Natal, South Africa. Data were analysed using deductive thematic analysis.
FINDINGS: Three themes emerged from the study; Attitudes towards impairment-based practice, Reflections on OBP, and The way forward. The need to focus on all the components of health rather than just the disease and the benefits of using the occupation-based practice approach were highlighted. Additionally, different factors required to implement holistic rehabilitation services and the barriers to OBP were identified.
CONCLUSION: Although the study identified OBP benefits, various barriers associated with its implementation were identified. Rehabilitation personnel, community stakeholders, and clients must work together to improve OBP implementation in public healthcare by combating the barriers identified in the study.
IMPLICATIONS FOR PRACTICE:
This study has implications for rehabilitation service implementation in the iLembe district public healthcare sector. OBP was perceived to have more quality of life and health outcomes, which leads to implications for practice. There is a need to transition from the medical model with approaches only focusing on body structures and functions into approaches that consider all the components of health, such as the OBP. Even though there are barriers towards OBP implementation, rehabilitation personnel can still promote its implementation through inter-professional practice, continuous professional development and health promotion. Furthermore, there are implications for undergraduate programmes to equip undergraduates with the skills to implement OBP within under-resourced facilities.
Keywords: holistic healthcare intervention, rehabilitation personnel, International Classification of Functioning, Disability and Health (ICF), social model of disability, personal and contextual barriers and facilitators, occupation-based practice, impairment-based practice.
BACKGROUND
Impairment-based practice (IBP) was reported as the dominant paradigm within medical-oriented healthcare facilities in South Africa, focusing on body structures and function1. The dominance of the medical model, which defines health as the absence of disease, results in a limited focus on external components influencing the client's participation, in contrast with the World Health Organisation's (WHO) definition of health2. This appears at odds with the WHO's definition of health as not just the absence of disease but a complete state of physical, mental and social well-being2.
Holistic healthcare interventions require more than focusing predominantly on the impairments. Healthcare providers must consider other factors, such as contextual factors and activity participation, especially when implementing rehabilitation services3.
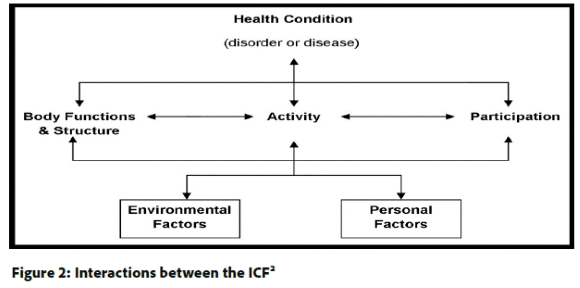
The WHO has been promoting this agenda, as seen in their shift from the International Classification of Functioning, Disability, and Health (ICF) in 1980 to 20012. The paradigmatic shift entailed changing terminology and service focus from a "consequences of disease" classification to a "components of health" classification in 20012. These components of health represented a move toward including components that consider an individual's holistic health. The ICF is a multifaceted classification providing a theoretical base for implementing healthcare services, specifically rehabilitation services. There are two parts of the ICF, namely Functioning and Disability, which includes body functions and structures, activities, participation, and contextual factors, including environmental and personal factors2. The framework highlights participation limitations within roles and activities, which are influenced by physical and social factors while emphasising the importance of activities and participation in health and quality of life. The initial shift towards the inclusion of activities and participation in the ICF resulted in a need for a subsequent shift towards focusing more on occupation-based practice (OBP) to facilitate improved quality of life and health. OBP includes activities (such as activities of daily living and work) and participation (how a client can participate in activities), which are often unaddressed during the implementation of rehabilitation services4.
Hall & Visagie5 noted that the ICF is not optimally utilised in clinical rehabilitation practice in South Africa. Additionally, efforts to view clients from a holistic perspective are primarily outside of the medical model6. These contentions are influenced contextually as South Africa has increased unemployment and poverty rates, negatively impacting access to healthcare services, especially in poor communities3. Personal resource restrictions create a need for more client-specific and context-specific healthcare.
The iLembe community comprises 89.2% isiZulu-speaking Africans, 3.4% White, 6.9% Asian, and 0.8% Coloured populations7. A quarter of the population lives in traditional and informal settlements; 50% of the roads are in good condition, and 50% in fair and poor conditions7. The South African public healthcare sector caters to 80% of the country's population; however, numerous barriers exist to accessing rehabilitation services8. These barriers include a lack of human resources, budget constraints, transportation limitations, a focus on the medical model, high turnover rates in acute hospitals, poor compliance, communication challenges and a breakdown in referral pathways9,10. Anecdotally, therapists have highlighted the challenges above as the critical reasons for the decreased use of OBP in South Africa. There is limited research regarding therapists' experiences in implementing OBP11. Thus, there is a need to explore rehabilitation personnel's experiences with implementing IBP and OBP, and the different factors affecting their practice choice within public healthcare in South Africa. Understanding their views and beliefs will assist in understanding the rationale for their practice choice when implementing rehabilitation services within the district. The need for holistic healthcare requires exploring the factors influencing rehabilitation personnel's practice choice. Local conditions influence contextual factors linked to clients' access to rehabilitation services and personnel practice choices within the district. The study aimed to explore the factors influencing rehabilitation personnel's practice choices when implementing rehabilitation services in public healthcare. and personal and contextual barriers and facilitators promoting effective OBP implementation.
METHOD
Study design
An explorative qualitative research design was used to understand the rehabilitation personnel's perceptions regarding IBP and OBP, and the rationale behind their practice choice. This research approach supported exploring rehabilitation personnel's experiences, social context, and views12 through semi-structured interviews, a focus group, and community mapping. These data collection methods allowed the researcher to capture and understand the participant's in-depth perceptions and feelings through careful and focused analysis.
Study population, sampling and recruitment strategy
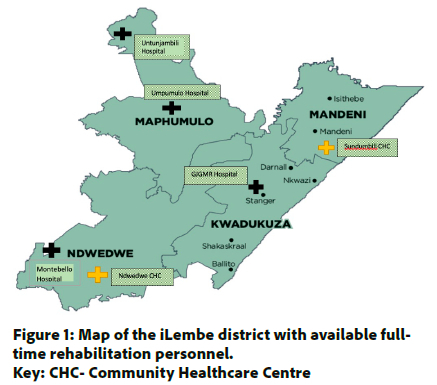
Participants were recruited by the first author over two months by contacting the facility managers and acquiring the names of the individuals employed in the district's hospitals and primary healthcare institutions, as seen in Figure 1 (below). Purposive sampling was utilised to recruit individuals working in the district for maximum variation. The sample comprised five occupational therapists , nine physiotherapists, three speech therapists, and three of which were key informants including one assistant director, chief physiotherapist and occupational therapy deputy head of department. For the purposes of this study, 'rehabilitation personnel' refers to personnel who are involved in rehabilitation of clients in an acute hospital. This included occupational therapists, physiotherapists, speech and language therapists. The study population comprised of rehabilitation personnel working in the iLembe district's public healthcare sector with more than six months work experience in the South African public healthcare sector and registered with the Health Professions Council of South Africa (HPCSA). The individuals who met the inclusion criteria described above were invited to participate in the study telephonically.
Data collection
The data collection tools were semi-structured interviews, a focus group and community mapping. The one focus group was aimed at critical key informants. The thirteen semi-structured interviews targeted community service officers and grade one practitioners to explore the factors influencing their practice choice. The ICF's biopsychosocial perspective guided the compilation of the questions used for the semi-structured interviews and the focus group to understand the participants' perceptions of the different practice choices and which contextual factors influence them.
Semi-structured interviews
Semi-structured interviews allow participants to give in-depth opinions on their experiences and report a detailed explanation of their perceptions13,14. The semi-structured interviews comprised of eight open-ended questions that explored the perspectives of the people responsible for implementing rehabilitation services. Further, exploring their perception on IBP and OBP, and OBP facilitators and barriers. The data from the face-to-face and zoom semi-structured interviews which ranged from 15 minutes to 1 hour, were recorded using an audio-recording device and manually transcribed. The interviews were conducted in English, a language both the participants and the researcher were comfortable with and could effectively communicate in. Different venues within KwaDukuza, Maphumulo, Ndwedwe, and Mandeni were utilised, depending on where the participant was employed.
Focus groups
Focus groups provide many different forms of interaction14, allowing the researcher to identify contradictions between participants. The focus group assisted in defining OBP in a neutral language and improved insight into positive and negative factors contributing to OBP and IBP implementation in the district. It was conducted for one and a half hours on the Zoom platform, with key informants: an Acting Head of Department, Assistant Director (AD), Chief and grade one practitioner. These key informants are involved in the development of policies, permanent staff employment, the training of community service officers (CSO) and make decisions concerning rehabilitation services at a district level.
The data were recorded using Zoom and manually transcribed. The focus group allowed participants to share their opinions, knowledge, and insights on the topic, and to receive feedback from other participants. The researcher conducted the focus group in English, which all the participants reported they were comfortable to converse in.
Community mapping
Community mapping was used to understand the contextual influences of OBP within the iLembe district, such as available healthcare facilities with and without rehabilitation personnel, and facilities, such as special schools and sheltered workshops. Data for community mapping was obtained through interacting with community members and healthcare practitioners in the district.
Pilot study
The pilot study was conducted to test the semi-structured interview's viability, and the necessary changes were made in the questions and questioning method before data collection. Two rehabilitation personnel from different settings within the public healthcare sector participated in the pilot. This assisted in amending the questions and prompts for the semi-structured interviews to improve clarity and elicit sufficient information depth. It also allowed the researcher to become familiar with implementing data collection method before the main study.
Data Analysis
Data were analysed using deductive thematic analysis guided by the ICF framework15, which allowed the researcher to analyse the participants' perceptions of IBP and OBP concerning the components of health, as seen in Figure 2 (below). Furthermore, Braun and Clark's six-step data analysis techniques16 guided the write up process of the study's key findings using sub-themes and themes. Initially, the researcher engaged in a process of familiarisation with the data, which was done through transcribing verbatim from the audio recordings and analysing the transcripts with guidance from the supervisors using thematic coding. After coding, similar concepts and findings were grouped to formulate sub-themes and themes. These sub-themes and themes were generated and reviewed, and then the final themes were defined and named ,and used to write up the data findings.
Trustworthiness
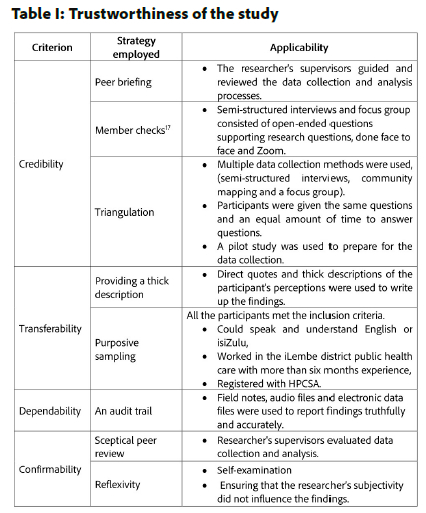
The researcher used various strategies to ensure the trustworthiness of the study, as seen in Table I (below).
Ethical considerations
The study followed the Protection of Personal Information Act 4 of 2013 guidelines restricting disclosure of personal and confidential information18. The purpose of the study, and voluntary participation and confidentiality were emphasised, meaning participants' information was confidential, and withdrawal from the study could occur at any point in the study. Informed consent was obtained from the participants before data collection. All the participants were assigned pseudonyms to ensure anonymity.
Ethical clearance was received from Humanities and Social Sciences Research Ethics committee and the KZN Department of Health (DOH). Gatekeeper permission was obtained from the iLembe District Office. After completing this research study, the findings were sent to the participants, the facility managers and DOH to influence rehabilitation service implementation and awareness.
FINDINGS
Demographics
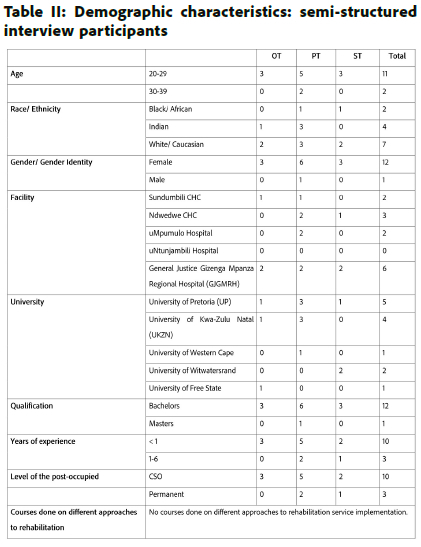
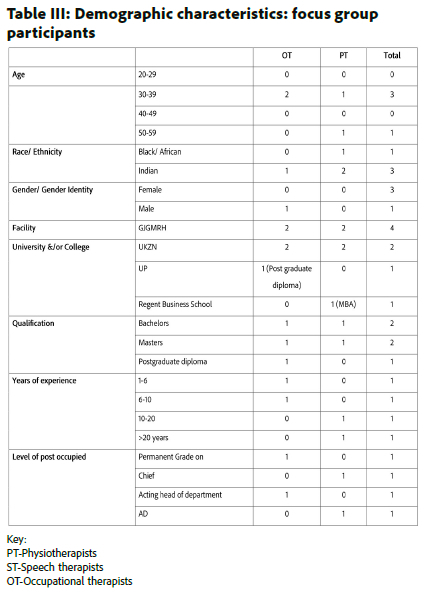
Seventeen participants took part in this study in total. There were thirteen participants in the semi-structured interviews; three speech therapists, three occupational therapists and seven physiotherapists as seen in Table II (adjacent). The focus group comprised four participants, represented in Table III (adjacent). Tables II and III illustrate the participants' experiences and different factors influencing their practice choice and view of rehabilitation services within the district.
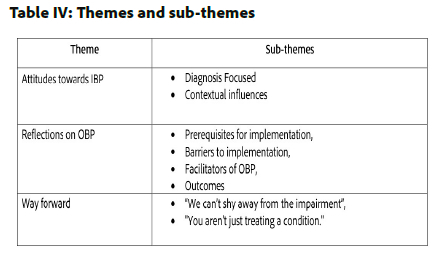
Themes and sub-Themes
Three themes were formulated from the data sub-themes gleaned from the analysis of the data, as illustrated in Table IV (below). Theme 1 related to attitudes towards IBP while highlighting how public healthcare is geared towards treating body structures and functions and the different factors promoting IBP. Theme 2 explored reflections on OBP and factors influencing its implementation and Theme 3 discusses participants' positionalities in moving towards more OBP-oriented rehabilitation approaches.
Theme 1: Attitudes towards IBP
Participants highlighted an increased need to understand how the client's diagnosis impacts their client's body functions and structures, as seen in IBP. IBP was described as focusing solely on the impairment experienced by the client and the main reason for referrals from other healthcare practitioners. Participants outlined different factors influencing their practice choice and the implications of using IBP. Two sub-themes were identified: Diagnosis Focused and Contextual influences.
Diagnosis Focused
IBP was seen to only focus on body functions and structures, neglecting other components of the ICF, namely, activities and participation and environmental and personal factors. They reported that these limits understanding of other factors influencing the client's health, including restrictions in participation, activity limitations and contextual factors. Participants from different facilities and professions noted that IBP does not allow for a holistic view of the client's needs to offer optimal rehabilitation intervention.
"Sometimes you can be solely focused on one aspect... if somebody... had a physical injury you focus so much on the physical injury that you tend to overlook their psych aspects"
(Participant 9, occupational-therapist CSO, semi-structured interview)
Contextual influences
Most participants highlighted an increased need to understand how the client's impairment impacts their client's body functions and structures, as seen in IBP. Furthermore, IBP was described as focusing solely on the client's impairment and the reason for referrals from other healthcare practitioners.
"What we find difficult when we go into the ward, we can't get straight in there and always start functional rehab because sometimes patients are very sick ... when we doing our undergrad, we always focusing on function ... and that's ... fine function and activity-based treatment.
But sometimes it doesn't always work in the first... maybe two sessions in a... patient that's really... unwell, and it's not there yet."
(Participant 1, occupational-therapist, focus group)
"They just refer a patient for the impairment; they never refer a patient because the patient can't dress ... I think doctors are more trained for more impairment based"
(Participant 2, occupational-therapist CSO, semi-structured interview)
Participants reported a dominance of the medical model within healthcare facilities and amongst other healthcare practitioners who expect them to implement IBP rather than OBP. Further, noting a limited understanding of OBP among other healthcare professionals, high turnover rates, and limited staff are some of the reasons for focusing on body functions and structures as it is perceived as the faster practice choice.
"This facility is quite acute, so patients come and go... quickly, so you tend to prioritise your rehab towards the patient, especially if they're inpatient or outpatient, and then you tend to focus a lot more on. what the impairment is what the condition is? How can you treat it"
(Participant 9, occupational-therapist CSO, semi-structured interview)
"You sort out... the major issues... the cause of a problem and... it gets the patient through the system faster so it's less taxing on resources ... resources are usually... limited, understaffed there's loads of patients"
(Participant 3, physiotherapist CSO, semi-structured interview)
Some participants in the semi-structured interviews reported they felt their roles as physiotherapists were more IBP-oriented to improve body functions and structures, while OBP was the domain of occupational therapists to improve participation using activities. This perception was held by half of the permanent physiotherapy staff who engaged in the study, the CSOs were observed to have a deeper understanding of the ICF framework and holistic interventions.
"I think with physio we want to get you to your highest-level functioning as early as possible. we deal with the impairment itself"
(Participant 7, physiotherapist, semi-structured interview)
"The ICF method it targets everything the patient's impairment. What they can do? What they cannot do? Activities they used to do? And how it impacts their activities?... their environment and personal factors" (Participant 4, speech-therapist CSO, semi-structured interview)
Theme 2: Reflections on OBP
Many participants displayed uncertainty when defining OBP and required verbal prompting to report their perceptions of the practice. When they could articulate their understanding of the practice, they regarded OBP as a more holistic approach considering all the "components of health". Some participants who utilised OBP needed to be made aware of the practice name. They highlighted that OBP was client-specific and yielded more activity participation and performance outcomes when utilised correctly. Participants also highlighted factors influencing OBP implementation in the district, resulting in the following sub-themes; Prerequisites for implementation, Barriers to implementation, Facilitators of OBP, and Outcomes.
Prerequisites for implementation
OBP required an initial assessment that allowed participants to gain insight into the client's personal and environmental activity limitations and facilitators. The insight into the client's life allowed participants to work towards improving health and quality of life. Participants noted that OBP must be implemented correctly to yield results and improve participation, which requires intense planning, intentionality, time, and knowledge.
"If you do a good subjective and you ask them what job you do ... what are your hobbies . you will always think of ways to incorporate your exercises"
(Participant 11, physiotherapist CSO, semi-structured interview)
"We have the whole knowledge of occupational science and everything that contributes. to how I do occupation-based treatment. My skills are not always the best"
(Participant 2, occupational-therapist CSO, semi-structured interview).
Barriers to implementation
Participants identified barriers to OBP implementation in the district's public healthcare, namely; contextual barriers, such as, community-specific and facility-specific; and personal factors, such as, client-specific factors.
The district was observed to be predominantly made up of hills, valleys and gravel roads outside the central towns. Participants noted that most clients are unemployed and poverty-stricken, leading to an inability to afford transportation fees, resulting in non-compliance with rehabilitation services.
The district has six public healthcare facilities (five hospitals and two CHCs) with rehabilitation services, with the rehabilitation personnel being primarily CSOs. There are 34 clinics in the district, but not all have outreach programmes, limiting access to rehabilitation services.
Participants noted a communication barrier as the community members in the district were predominantly isiZulu speaking. Therefore, being unable to speak and understand isiZulu was a limitation towards implementing OBP. Thus, it is difficult to understand the clients leading to difficulties in obtaining subjective information on their activity, participation and contextual needs.
"Language barrier... your different languages trying to explain how to do a certain thing in a certain way but at the same time, cultures, people have different ways of doing different occupations"
(Participant 10, occupational-therapist CSO, semi-structured interview)
Some participants in the focus group reported a lack of facilities outside DOH to carry over OBP, including sheltered workshops and schools catering to individuals with different disabilities. No schools catered to children with only physical disabilities, hearing, visual, and multiple impairments. Moreover, there were no remedial and prevocational schools in the district. The lack of these facilities was believed to be a societal constraint negatively impacting quality of life and carryover of OBP into the community.
"Children with disabilities that... have physical disabilities, but have good cognitive function, are not being included in mainstream schools, because those schools do not cater for children with disabilities"
(Participant 1, occupational-therapist, focus group)
There are three schools for severely mentally disabled children and one school for the neutrally impaired in the iLembe district.
Participants identified human resources as a contextual limitation towards implementing OBP as it requires intense planning and intentionality. It was difficult due to the human resource constraints, specifically permanent staff, as noted in Tables V and VI (below). Most participants working in the district were CSOs. They reported having limited experience and skills, which restricted client-specific OBP, which requires intentionality and planning.
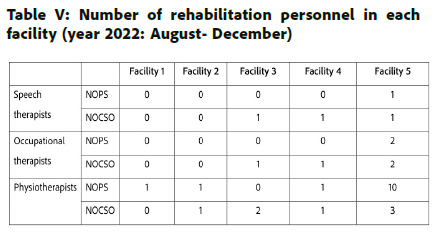
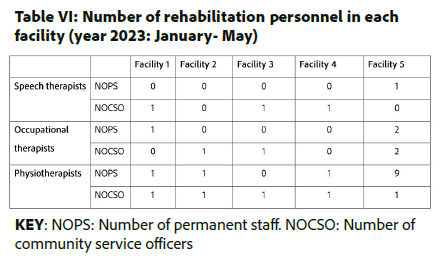
Participants noted that limited human resources as seen in Table V and VI, and high facility turnover rates in acute settings led to shorter rehabilitation sessions.
"We don't have permanent staff... if you just have comserves as well that's working, it'shard to do an MDT... most of the comserve's as well they... learning still"
(Participant 6, physiotherapist, semi-structured interview)
"I definitely think that the knowledge needs to be improved so that they have a good understanding of what's occupation-based, a good understanding about impairment based and when it's best to use which on... In acute hospital, you have such a short time, so you end up having to treat... the impairment. might not have the time frame to do all the occupations . it's easier to just treat the impairment"
(Participant 10, occupational-therapist CSO, Semi-structured interview)
Participants perceived OBP to require more time for planning and implementation, which was difficult to conduct in a fast-paced environment that required more straightforward approaches to counteract the time constraints.
"It's difficult to give... intense occupation-based therapy which takes planning which takes a lot of intentionality to put the patient's needs first if you're seeing a lot of patients by yourself"
(Participant 5, speech therapist CSO, semi-structured interview)
"...For doctors to... understand... rehab and the role of rehab and not just. being so focused on discharge"
(Participant 1, speech-therapist, semi-structured interview)
Numerous environmental barriers within the facilities were reported, includinglimited space, equipment, and infra-structure, as activity participation could not be simulated within the facilities to improve performance.
"Physical resources... we don't have space to store the equipment . it's a barrier as well and general understanding of what therapy is what therapy does for you"
(Participant 6, physiotherapist, semi-structured interview)
Participants identified client-specific barriers to OBP implementation, including poor support systems, unemployment, and poverty, limiting compliance and carryover of OBP at home.
"People don't have a family structure... the family abandons them or they just around people who don't really know them, so it's hard to. bring their occupation into therapy"
(Participant 1, speech therapist, semi-structured interview)
"Financially, a lot of patients cannot get to the hospital ... transport fees are... expensive"
(Participant 3, physiotherapist CSO, semi-structured interview).
Facilitators of OBP
Numerous environmental facilitators for OBP were identified. Participants reported needing a complete rehabilitation team, an excellent subjective assessment, MDT combined sessions, and working with the client and family to set therapy goals. One participant mentioned that standard operating procedures (SOPs) are required to improve access to rehabilitation services through the correct referral pathways and set a standard level for the rehabilitation services to be implemented.
"If somebody transfers out, gets another post or resigns and tires... the post gets frozen ... your patient load is increasing, and your staffing load is decreasing"
(Participant 2, physiotherapist, focus group)."
"When you see a patient, you have to assess... set some goals where you want to go with this patient. So your goals should come from what... the client wants to achieve... So I'll be working out every. session. with the patient will be directed in terms of. making this patient being able to integrate into the work environment."
(Participant 3, occupational-therapist, focus group)
"Having joint sessions where the OT, physio and... speech therapist worked together on one patient with the family member to get the optimal goals or outcomes"
(Participant 5, speech-therapist CSO, semi-structured interview)
"The SOP's and... DOH policies...it's not specifically for a certain condition, but it is how the patient can access the service...the pathway the patient needs to follow up to access the service, and in terms of referral pathways"
(Participant 2, physiotherapist, focus group)
Special schools and sheltered employment opportunities were noted as key factors required to facilitate OBP carryover in the community. Persons with disabilities were noted to have decreased opportunities to engage in activity performance and participation within the community, which are vital to improving quality of life and health outcomes.
"A program whereby these the skills that I acquire from the centre they can get some kind of... employment, or it can be... where they can start doing their own things maybe that will also give those disabled patients. some kind of purpose and have a meaningful life"
(Participant 3, occupational-therapist, focus group).
Outcomes
OBP was viewed as a holistic approach, facilitating activity participation and improved independence. OBP allowed participants to understand the different components of the client's health, such as functioning and disability, contextualfactors, the limitations towards activity performance and participation to work with the client towards returning to the highest level of independence possible. Additionally, allowing for carryover at home as clients could incorporate techniques learnt in therapy.
"Occupation-based is a more holistic approach, according to me, on how we can look at how getting the people back into society ... looking at what they can do... what must they do every day in their life to be able to be as independent as possible"
(Participant 2, occupational-therapist CSO, semi-structured interview)
"Patients... do recover mostly to a high level of functioning, returning to a high level of functioning... to a life that they used to live before so patients are more satisfied and then also... the quality of life... Today I had a patient that has low back pain; so she also said she doesn't have time to do all these extensive exercises because she is a mom of four kids, so she's... busy doing house chores all the time, so I taught her how to do her core exercises while doing dishes for instance"
(Participant 3, physiotherapist CSO, semi-structured interview)
"It's more functional based than just looking at just one joint or one impairment. it's looking at the person as a whole"
(Participant 11, physiotherapist CSO, semi-structured interview)
Theme 3: Way forward
Most participants had decreased insight into the Social Model of Disability (SMoD). Once the definition of SMoD was given to them, they identified the model to have similar principles with OBP, namely, the focus on participation in activities and not just the limiting impairment. Participants reported that OBP allowed for compensation for lost function and contextual adjustments if body functions and structures could not be improved. One participant highlighted that therapy should not be viewed as linear or binary. However, we should consider the different factors influencing the client, such as changes in body structures and functions, capacity to participate in activities, environmental facilitators and barriers, and personal factors. Participants reported that IBP and OBP could be used together depending on the client's needs. Most participants highlighted the need to transition towards OBP to address all the components of health as it is neglected in biomedical healthcare settings. These perceptions resulted in two sub-themes, "We can't shy away from the impairment" and "You are not just treating a condition".
"We can't shy away from the impairment."
Participants acknowledged that the client's body structure and function form part of the components of health. They reported a need to remediate the body structure and functions in acute stages of rehabilitation, if possible, through using different approaches and activities to improve participation in meaningful activities in different environments.
"...You can use both interchangeably because. we can't shy away from the impairment.
We still need to try to find ways to improve the impairment as well as trying to find ways to help the patient to do whatever they used to do".
(Participant 4, speech-therapist CSO, semi-structured interview).
"You aren't just treating a condition."
Even though the client cannot be isolated from their impairment, participants highlighted that the impairment cannot be treated without addressing the client as an active member of society. Due to the medical model dominance in the public healthcare settings in the district, participants reported a need to move towards more OBP. OBP allows participants to understand the client and the different factors influencing their health, such as their body structures and functions, environment, activities and participation.
"Occupational based would... be the better one because... if people are really wanting to do a specific task then if that if you start early. they are able to achieve that quicker"
(Participant 11, physiotherapist CSO, semi-structured interview)
"Occupation based. it's more functional. and allowing the patient to use those strategies in real life. it's more holistic"
(Participant 1, speech-therapist, semi-structured interview)
"I... think that focusing on occupation rather than impairment, focusing on getting these people out there, getting them to see that my disability doesn't stop me from doing these things"
(Participant 2, occupational-therapist CSO, semi-structured interview)
DISCUSSION
The study identified IBP as a non-holistic approach focusing on addressing body functions and structures, which concurs with the finding by Tomori et al9. This focus on impairment was found to sometimes neglect the other components of health, such as activity participation, and environmental and personal factors, which are critical when providing rehabilitation services. Even though IBP was viewed to focus on one component of health, it was still widely utilised in the district's public healthcare sector due to different factors such as stage of illness and rehabilitation, limited human resources, limited insight on OBP and physical resources geared towards body functions and structures in the healthcare facilities.
Despite the increased use of IBP approach, participants perceived OBP as a more holistic approach. It is perceived to consider all the components of health, including activity performance, participation, contextual factors, and how their presenting impairment, disability, and body functions interrelate to impact client health needs. The participants in this study suggested that OBP is multifaceted and aimed at improving health and well-being through activity participation, and easily generalised to client's lives19. OBP implementation was perceived to have improved quality of life by compensating for lost function by addressing contextual factors. Furthermore, it was viewed as allowing participants to view clients as occupational beings, not just their impairment10.
Although OBP was viewed as a holistic approach, there are numerous barriers impeding its implementation within the district. Contextual factors, namely, socio-demographic variables such as language, high unemployment, transport limitations, and crime rates which contradict findings by Aas & Bonsaksen's20, who found that these factors did not impact OBP access and implementation. Additionally, language barriers were found to cause difficulty in rehabilitation personnel's understanding of their clients' activities, participation, and contextual needs. Language barriers resulted in a decreased understanding of their client's contextual and personal factors, and rehabilitation goals. The previously mentioned barrier further limits the client's insight into rehabilitation services and OBP, along with other contextual factors such as poverty and transportation limitations leading to non-compliance, which reinforces findings by Narain & Mathye21.
Narain & Mathye21 further assert limited awareness of rehabilitation services in rural South African communities. The iLembe community is predominantly a Black community, and this was linked to the decreased awareness of rehabilitation services within the district, which was perceived to be a barrier to OBP implementation, as these services are perceived to be for wealthy White communities21. Limited awareness of OBP negatively impacts clients' personal factors, such as motivation to engage in activity-based approaches such as OBP, further impacting their function and participation within their context.
Contextual factors within the district, such as the decreased number of special schools and sheltered workshops, were perceived to decrease compliance and carryover of OBP into the community. Furthermore, emphasising a need for more of these facilities to carry over OBP within the community outside of DOH, which was not seen in other literature relating to OBP.
Contextual factors within the healthcare facilities, such as limited facilities offering rehabilitation services, limited rehabilitation personnel employed in the district's public healthcare sector and limited physical resources also served as barriers. The previously mentioned barriers led to limited time to explore activity performance and identify barriers to activity participation within the client's context. Additionally, this study highlighted the need for rehabilitation personnel to advocate and bring awareness to community stakeholders to conduct environmental changes in the district's healthcare facilities to promote activity performance and participation, which reinforces the findings by Scaffa & Reitz22.
Kwa-Zulu Natal DOH financial constraints influenced the lack of availability of physical resources for OBP implementation23. These facility-specific barriers concur with a study by Hall & Visagie5, which identified the dominance of the medical model, decreased human resources, high turnover rates, and limited time as factors that led to IBP being the primary practice choice. The previously mentioned barriers concur with multiple studies24-27, highlighting the limited availability of resources, participants' lack of experience and skills, and medical model dominance hinder OBP implementation. OBP was considered difficult to implement in a medical-model-based facility as pragmatic and contextual factors exerted opposing influences22,27. Due to a lack of experience and skills in implementing OBP, some recent graduates choose IBP over OBP27. CSOs found OBP inherently complex, requiring skills, time and complicated techniques to implement. They felt they needed more time to plan and experience implementing OBP24,25,27, leading to them implementing more IBP. Even though they viewed OBP to be holistic and client-specific, some permanent physiotherapists considered OBP to be an approach for occupational therapists and IBP as more aligned with physiotherapy, which is in keeping with findings from Narain & Mathye21 and Inglis et al.28. The perception that OBP is the core of the occupational therapy profession is one reason why OBP is not used by other rehabilitation personnel21. CSOs considered OBP as a practice all rehabilitation personnel should utilise as it encompasses all the components of health, including physiotherapists CSOs. Similarly, Narain & Mathye21 stated that physiotherapy must focus more on participation to meet the client's needs.
Contrary to findings by Wolf et al.29 and O'Donoghue et al.25, this study found that decreased family involvement was a barrier towards implementing OBP in terms of facilitating carryover and home-based OBP. Wolf et al.29 found that family involvement was perceived not to impact OBP implementation. In contrast, O'Donoghue et al.25 found that family members increased involvement resulted in the family feeling obligated to help the clients in their activity participation, becoming over-involved and taking over the client's responsibilities and decision-making. Unemployment and poverty were found to limit access to healthcare services and continuous OBP, as seen by Chichaya et al30 as accessing healthcare services is expensive for people with disabilities. Further, limiting continuous and practical OBP which is critical to producing activity and participation outcomes.
This study identified key factors to promote OBP implementation within the district. The need to improve the client-therapist ratio by employing permanent staff from each discipline to form a complete rehabilitation team in each healthcare facility was identified. More permanent staff would improve human resources to deliver rehabilitation services and access to supervision and mentorship for community service office31, thus improving OBP implementation. More staffing will promote inter-professional practice and collaboration with clients and their families to set therapy goals. Standard operating procedures (SOPs) focusing on improving access to rehabilitation services and awareness of the available rehabilitation services are required to implement OBP and access rehabilitation services.
CSOs spoke highly of OBP, indicating they valued the approach, which concurs with the literature20,22. However, their decreased skills, experience and knowledge resulted in decreased confidence to implement OBP, which is essential in OBP implementation. Furthermore, it highlights the need for undergraduate health science programmes in South Africa to better prepare newly graduated rehabilitation personnel's theoretical knowledge and skills in considering all the components of health and implementing the OBP approaches11. Facilities such as special schools and sheltered employment or employment opportunities are needed in the district to carry over OBP to improve activity participation and quality of life.
When transitioning towards more OBP approaches, it is vital to acknowledge that the clients' impairment is a part of their health. Following the findings by Oliver32, the study highlighted the importance of recognising the relationship between the client's impairment and other components of health. Neglecting body functions and structures, as seen in SMoD, creates a gap in understanding the holistic client and health32, thus, the importance of choosing a practice choice according to the client's needs. Different approaches can be utilised depending on the client's needs. Additionally, rehabilitation service implementation needs to be tackled collaboratively, with the understanding that the components of health are influenced by a dynamic system22,32,33. Activity participation is often unaddressed4; therefore, the study found that rehabilitation personnel must adopt more OBP approaches when implementing rehabilitation services.
Recommendations
It is suggested that DOH involves people with disabilities when formulating policies and addressing public healthcare concerns regarding disability. Rehabilitation personnel, other healthcare practitioners and policymakers are advised to be more aware of the components of health when formulating policies and implementing OBP. Additionally, to counteract human and physical resource barriers, DOH is advised to improve the budget towards rehabilitation services to promote the implementation of holistic, client-specific interventions. Non-holistic approaches may lead to further complications and unnecessary use of state resources (Revolving-door syndrome). Moreover, it is suggested that DOH funds training for rehabilitation personnel, and encourage rehabilitation personnel's continuous professional development to improve their knowledge of OBP implementation to conduct holistic, subjective, environmental assessments of client-specific healthcare needs.
Future studies exploring OBP in physiotherapy and speech therapy and other healthcare practitioners are required to improve insight into the effect of OBP within these disciplines. Rehabilitation personnel are advised to improve awareness of rehabilitation services, their role in holistic healthcare and the importance of OBP through health promotion programmes. Furthermore, rehabilitation personnel and community stakeholders must problem-solve ways to counteract barriers to access to rehabilitation services, e.g. outreach services.
Community stakeholders are advised to establish sheltered workshops and more schools catering to the needs of persons with disabilities to improve clients' community engagement, activity participation and quality of life.
The undergraduate curriculum should focus more on inter-professional practice and education, and encourage learning the skills required to implement OBP in public healthcare.
Limitations
The study explores the perspectives of rehabilitation personnel within public healthcare in semi-rural and rural communities in one district; therefore, contextual factors cannot be generalised to other populations. Furthermore, most participants were community service officers who still needed to establish their professional identity. The dominant medical model influenced their practice choices in their workplace. The study is focused on the perspective of rehabilitation personnel; this includes physiotherapists and speech and occupational therapists. The study did not consider the perceptions of other healthcare practitioners vital in providing holistic healthcare services.
CONCLUSION
OBP was found to improve the components of health, level of independence and carryover into the community. Even though OBP was perceived to have more health outcomes, IBP dominates the district's public healthcare facilities. IBP's dominance is accredited to factors such as the dominance of the medical model, acute phases of illness, high hospital turnovers, limited staff, skills, experience and insight into OBP and the belief that OBP is restricted for occupational therapists. The limited resources within the district's public healthcare system require rehabilitation personnel to problem-solve sustainable and innovative ways to improve OBP implementation. This requires the district stakeholders to work together and use the available resources to improve OBP and holistic healthcare implementation, considering all the components of health. The study emphasised the need for continuous learning and skills development to equip CSOs with the necessary skills to make them confident to implement OBP. Insight building amongst healthcare practitioners about OBP is required to decrease the misinformed perceptions associated with OBP.
Acknowledgements
The University of KwaZulu-Natal, the Department of Health, and the participants are acknowledged for participating in this study.
Author contributions
Phana Gumede conceptualised the study, collected the data and did the preliminary data analysis and the writing of the manuscript. Chantal Christopher and Deshini Naidoo assisted with the conceptualisation of the study and refined the data analysis and were critical reviewers of the manuscript and contributed toward the final version thereof.
Conflicts of Interest
None to declare.
REFERENCES
1. Alotaibi NM, Reed K, Nadar MS. Assessments used in occupational therapy practice: an exploratory study. 2009;23(4):302-18. [ Links ]
2. World Health Organization. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY. World Health Organization 2007. [ Links ]
3. Heymani S, Pillay D, de Andrade V, et al. A transformative approach to disability awareness, driven by persons with disability. South African Health Review 2020;2020(1):1-9. [ Links ]
4. Abdel Malek S, Rosenbaum P, Gorter JW. Perspectives on Cerebral Palsy in Africa: Exploring the Literature through the Lens of the International Classification of Functioning, Disability and Health. Child Care Health Dev 2020;46(2):175-186; https://doi.org/10.1111/cch.12733. [ Links ]
5. Hall R, Visagie S. A qualitative exploration of the uses of the International Classification of Functioning, Disability and Health at an inpatient neurorehabilitation facility in the Western Cape, South Africa. Disability and Rehabilitation 2022;44(4):582-9. [ Links ]
6. Kielhofner G. Conceptual Foundations of Occupational Therapy Practice. FA Davis; 2009. [ Links ]
7. ILembe District Municipality KZN. Profile and Analysis: District Development Model. .2023. [ Links ]
8. Magaqa Q, Ariana P, Polack S. Examining the availability and accessibility of rehabilitation services in a rural district of south africa: A mixed-methods study. Int J Environ Res Public Health 2021;18(9); https://doi.org/10.3390/ijerph18094692. [ Links ]
9. Tomori K, Nagayama H, Ohno K, et al. Comparison of occupation-based and impairment-based occupational therapy for subacute stroke: A randomized controlled feasibility study. Clinical Rehabilitation, 2015;29(8):752-762; https://doi.org/10.1177/0269215514555876. [ Links ]
10. Brown HV, Hollis V. The Meaning of Occupation, Occupational Need, and Occupational Therapy in a Military Context. 2013. [ Links ]
11. Hess-April L, Ganas N, Phiri L, Phoshoko P, Dennis L. Occupation-based practice in a tertiary hospital setting: occupational therapists' perceptions and experiences. South African Journal of Occupational Therapy 2017;47(3); https://doi.org/10.17159/2310-3833/2017/v47n3a5. [ Links ]
12. Hunter DJ, Mccallum J, Howes D. Defining Exploratory-Descriptive Qualitative (EDQ) Research and Considering Its Application to Healthcare. 2019. [ Links ]
13. Creswell John W, Creswell JD. Research design: Qualitative, quantitative, and mixed methods approaches. . Sage publications 2017. [ Links ]
14. Smithson J. Using & Analysing Focus Groups. Int J Soc Res Methodol 2000;3(2):103-19. [ Links ]
15. Dawadi S. Thematic Analysis Approach: A Step by Step Guide for ELT Research Practitioners. 2020. [ Links ]
16. Peel KL. beginner's guide to applied educational research using thematic analysis. Practical Assessment, Research and Evaluation 2020;25(1):1-16; https://doi.org/10.7275/ryr5-k983. [ Links ]
17. Birth L, Scott S, Cavers D, et al. Member Checking. Qualitative Health Research. Qual Health Res 2016;26(13):1802-1811. [ Links ]
18. de Stadler E, Esselaar P. A Guide to the Protection of Personal Information Act. Juta: Cape Town; 2015. [ Links ]
19. Estes J, Pierce DE. Pediatric therapists' perspectives on occupation-based practice. Scandinavian journal of occupational therapy. Scand J Occup Ther 2012;19(1):17-25. [ Links ]
20. Aas MH, Bonsaksen T. Exploring occupation-based practice among occupational therapists in hospitals and rehabilitation institutions. Scand J Occup Ther 2022; https://doi.org/10.1080/11038128.2022.2059564. [ Links ]
21. Narain S, Mathye D. Strategies to integrate physiotherapists into primary health care in South Africa. The South African Journal of Physiotherapy 2023;79(1). [ Links ]
22. Scaffa ME, Reitz SM. Occupational Therapy in Community-Based Practice Settings (8th Ed.). F.A. Davis Company; 2014. [ Links ]
23. The Department of Health. The Department of Health. Budget Vote 7.2023. [ Links ]
24. Copley JA, Rodger SA, Graham FP, et al. Facilitating student occupational therapists' mastery of occupation-centred approaches for working with children. . Canadian Journal of Occupational Therapy 2011;78(1):37-44. [ Links ]
25. O'Donoghue C, O'Leary J, Lynch H. Occupational Therapy Services in School-Based Practice: A Pediatric Occupational Therapy Perspective from Ireland. Occup Ther Int 2021;2021; https://doi.org/10.1155/2021/6636478. [ Links ]
26. Daud AZC, Judd J, Yau M, et al. Barriers of Occupation-based Intervention. Asian Journal of Quality of Life 2016;1(4):1-10; https://doi.org/10.21834/ajqol.v1i4.12. [ Links ]
27. Di Tommaso A, Wicks A, Scarvell J, et al. Experiences of occupation-based practice: An Australian phenomenological study of recently graduated occupational therapists. British Journal of Occupational Therapy. British Journal of Occupational Therapy 2019;82(7):412-21. [ Links ]
28. Inglis G, Faure M, Frieg A. The Awareness and Use of Outcome Measures by South African Physiotherapists. 2008. [ Links ]
29. Wolf TJ, Chuh A, Floyd T, et al. Effectiveness of occupation-based interventions to improve areas of occupation and social participation after stroke: An evidence-based review. The American Journal of Occupational Therapy 2015;69(1):6901180060p1-6901180060p11. [ Links ]
30. Chichaya TF, Joubert R, McColl MA. Applying the occupational justice framework in disability policy analysis in Namibia. South African Journal of Occupational Therapy 2019;49(1); https://doi.org/10.17159/2310-3833/2019/vol49n1a4. [ Links ]
31. Struwig N, van Stormbroek K. Support, supervision, and job satisfaction: Promising directions for preventing burnout in South African community service occupational therapists. . South African Journal of Occupational Therapy 2023;53(1):67-80. [ Links ]
32. Oliver M. The social model of disability: Thirty years on. Disability & society, 2013;28(7):1024-1026; https://doi.org/10.1080/09687599.2013.818773. [ Links ]
33. Pillay M, Kathard H. Decolonizing Health Professionals' Education: Audiology & Speech Therapy in South Africa. 2016. [ Links ]
34. Queirós A, Faria D, Almeida F. STRENGTHS AND LIMITATIONS OF QUALITATIVE AND QUANTITATIVE RESEARCH METHODS. European journal of education studies 2017; https://doi.org/10.5281/zenodo.887089. [ Links ]
 Correspondence:
Correspondence:
Phana Gumede
Email: phanagumede03@gmail.com
Submitted: 23 October 2023
Reviewed: 5 December 2023
Revised: 11 January 2024
Accepted: 11 January 2024
Editor: Hester M. van Biljon: https://orcid.org/0000-0003-4433-6457
Data availability: Upon reasonable request, from corresponding author
Funding: No funding was received for this research
* Masters degree student at the time of research

