










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.54 no.1 Pretoria Abr. 2024
http://dx.doi.org/10.17159/2310-3383/2024/vol54no1a3
RESEARCH ARTICLE
Activities of daily living with grasp types and force measurements during object manipulation
Monique M. KellerI; Roline Y. BarnesI; Corlia BrandtII
IDepartment of Physiotherapy, School of Health and Rehabilitation Sciences, Faculty of Health Sciences, University of the Free State, South Africa. Monique M. Keller: https://orcid.org/0000-0002-1513-295X. Roline Y. Barnes: https://orcid.org/0000-0002-3743-0077
IIDepartment of Physiotherapy, School of Therapeutic Sciences, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa. https://orcid.org/0000-0002-8445-1348
ABSTRACT
BACKGROUND: Limited scientific evidence guides hand rehabilitation towards improved hand function, and safe early return to work. Grasp types, the subunits of object manipulation and the forces which may improve functional outcomes, have been identified as missing links that may inform rehabilitation after second to fifth metacarpal fractures, through progression of basic and instrumental activities of daily living (ADL). The aim of the study was to collect ADL forces through grasp types to inform hand rehabilitation for second to fifth metacarpal fractures.
METHODS: This cross-sectional, quantitative study included 32 conveniently sampled healthy adults aged 20 and 59 years. Thirty-one (31) ADLs, both basic and instrumental, each associated with a predominant grasp type, were tested. The participants donned two testing gloves, with force sensing resistors (FSRs) glued to the fingertips, the ADLs were performed, and forces measured. The researcher imported the force data into an Excel spreadsheet for both descriptive and inferential analyses with STATA.
RESULTS: Fourteen males and 18 females, with a mean age of 37 years, participated. Statistically significant differences between genders were found for seven grasp types. Three thumb-adducted power palm grasps, three thumb-abduction precision pad grasps, and one thumb-abduction power palm grasp constituted the testing. Light and heavy ADLs and their associated grasp types were identified
CONCLUSION: To ensure optimal hand function, early safe return to ADLs should be the goal of second to fifth metacarpal fracture rehabilitation and may be achieved by incorporating active grasp types as exercises with graded resisted grasp types and ADLs.
IMPLICATIONS FOR PRACTICE:
• Occupational therapists can incorporate grasp types in their observation during assessments of individuals who sustained second to fifth metacarpal fractures to determine the subcomponents of functional deficits.
• Hand rehabilitation may be augmented by incorporating grasp types in isolation during unresisted active joint range of motion.
• Occupational therapists, guided by the analysis of hand functioning, can incorporate ADLs with the predominant grasp types which may improve hand function.
• Grasp force data may guide safe and early return to function.
Keywords: human grasp, manipulation, hand rehabilitation, ctivities of daily living, grasp force data
INTRODUCTION
Hand function plays a crucial role in an individual's ability to perform daily tasks, and a hand injury can have devastating consequences. The primary role of the human hand lies in the manipulation of objects to achieve specific goals1. Difficulties in using one's hands can significantly impact independence and participation. The hand's capacity to attain various positions and exert precise pressure for object manipulation is attributed to the combined contributions of the skeletal structure, muscular strength, and the extensive sensory input from nerves. This sensory feedback is crucial for evaluating the characteristics such as shape, size, texture, and weight of the objects. In both the grasping and lifting processes, the brain relies on accurately interpreting the information received from the hand and executing appropriate responses1.
Robinson et al.2 found that acute wrist and hand injuries impose a substantial burden on society and individuals. Therefore, hand rehabilitation should be based on scientific evidence and best practices to improve hand function. Internationally hand and wrist injuries account for 20% of all emergency visits2, with metacarpal fractures being the most common3.
Hand rehabilitation involves more than just face to face consultations; it also includes home exercise programs (HEP). Adherence to these programmes has a significant impact on the effectiveness and outcomes of hand therapy interventions4. When considering the effectiveness of HEP, Gülke et al. 20185, undertook research involving 60 individuals who had experienced a single diaphyseal or metaphyseal second to fifth metacarpal fracture. The goal was to compare the effectiveness of a standard physical therapy (PT) program with a newly developed HEP following surgical management through open reduction internal fixation. The participants were divided into two groups using controlled block randomisation after a 2-week splinting period. The PT group received 12 sessions of 30-minute PT over 6 weeks, with therapists recommending exercises for home use. In contrast, the HE group participants performed exercises three times a day, consisting of four to six exercises per session lasting 20 to 30 minutes. The study's results indicated that a well-structured HEP post-surgery for second to fifth metacarpal fractures (excluding the thumb) showed comparable effectiveness to traditional rehabilitations.
Valdes et al.6 advocated for hand therapy HEPs that are appealing and promote adherence. Valdes et al.6:569 stated that "Generally speaking, an HEP for an individual attending hand therapy tends to be multimodal so that information is taught in the clinic is carried over into the home environment." They suggest that home exercises should be integrated into clients' daily routines while protecting the injured body structure. Although there is a growing body of literature advocating for enhanced hand rehabilitation and improved adherence, the authors found a dearth of studies incorporating grasp types and force sensor data, especially incorporating 10 fingers during ADLs, to back the inclusion of daily routines, grasp types and ADLs into HEPs safely.
Kimmerle et al.7 also emphasised the need for more functional assessments and rehabilitation therapies for individuals with hand injuries. The functional hand repertoire model encourages therapists to incorporate reaching, object manipulation, and releasing as one of the components of hand actions into the key components of hand actions, considering factors such as object properties, movement patterns, and task demands7. In a recent study, Valdés et al.8 reported that most of the 311 participants believed that occupational-based interventions should be included in hand therapy management, 40% using occupation-based interventions should be included in hand therapy management, 40% using occupation-based interventions between 26% and 50% of time. The Disability of the Shoulder, Hand and Arm (DASH) outcome measure was the most frequently used outcome measure8
Incorporating grasp types, which are the subunits of manipulation during ADLs, into hand rehabilitation may improve hand function and can ideally be included in HEPs. However, there is currently a lack of force sensing scientific evidence on when to incorporate safe grasping based on the force production on injured hand structures.
Previous studies have investigated grasp types and their frequency of use in common manipulation tasks. For example, Bullock9 observed the unstructured hand-use behaviour of individuals during their working day. The unstructured hand-use behaviour of two housekeepers and two machinists was investigated by taking video footage over 7.45 hours of their working day. In previous studies, hand grasps were measured regarding pre-selected objects with the hand posture used in manipulation9. In another study, Sperling and Jacobson-Sollermani10, encoded the human grasp types and general surfaces of the hand in 30 participants while they were eating a meal, and documented 1 277 different grips. The most comprehensive collection of grasp types is collated in the GRASP taxonomy of the human hand grasp types11.
Riddle et al.12 measured individual finger forces among participants with or without osteoarthritis. The research was undertaken to provide a biomechanical hand model to determine the effect of osteoarthritis on hand function12. Although the study is useful, Riddle et al.12 suggested that force testing during the execution of a wider variety of everyday ADL tasks is required.
Studies measuring forces with limited fingers and grasps and using sensors on a glove or objects have been performed12-15. Castro and Cliquet, for instance, investigated the grasping of cylindrical objects and measured the associated static forces with FSRs14, while Romeo et al.15 determined the finger forces exerted with a tripod grasp during spherically shaped ball-grasping, with the FSRs mounted on the contact areas of the ball. The above studies measured forces including only limited grasps which is challenging to generalise the results to hand rehabilitation for example after metacarpal fractures.
In hand rehabilitation, after having sustained second to fifth metacarpal fractures, individuals may interpret returning to light function differently, leading to inappropriate bending, torsion, and shear loading between the two fracture ends, thus disrupting the bone healing process16. The healing of the bone could also be disrupted by physical damage to the new capillaries and repairing tissue, with possible non-union as a result16. A scientific approach is needed to inform hand rehabilitation, grade rehabilitation forces with grasp-type exercises, and ensure a timely but safe return to ADLs.
The study aimed to gather force sensing data through grasp types and forces during ADLs, intended for the advancement of hand rehabilitation specifically tailored for second to fifth metacarpal fractures. The objectives of this cross-sectional study were to determine the basic and instrumental task forces exerted by the human hand through its grasps on the objects that it manipulates, as well as the associations between mean maximum forces and gender among a purposively sampled group of healthy human adults between the ages of 20 and 59 years, and with the aid of FSRs.
METHODS
In a previous published study17, the methodology of this study was described. A brief overview follows. Participants who met the inclusion criteria and provided informed written consent wore gloves with FSRs attached to the fingertips. A total of 105 ADLs, consisting of 38 basic and 67 instrumental, were observed over a 24-hour period to capture hand use. The researchers supplemented the task data with the use of the English DASH questionnaire18 by adding tasks that were not in the task list but appeared in the DASH to ensure comprehensive coverage. The 105 ADLs were categorised into five sections namely: personal care and hygiene, transport and mobility, home environment (inside the home), gardening and outdoor activities, and a miscellaneous category "other" for ADLs not falling into the aforementioned categories. The ADL tasks were further classified as light, medium, or heavy demand based on a study by Han et al.19. To investigate the biomechanical features of callus, Han et al.19 conducted a compression test, and the resulting load-displacement forces of bone callus were measured19. The early stages of callus displacement ranged from 0.6 to 1.3 millimetres with forces of 5N.
To ensure reliability, the demographic questionnaire, FSR measurements, and grip strength measurements were conducted using a standardised and piloted method led by one researcher and a trained research assistant. The finger force sensor measurement data collected during the piloted feasibility study17, were recorded on a laptop using Realterm software. During this feasibility study, the researcher then determined the predominant grasp types employed for each of the 105 ADLs. Subsequently, the data for each activity were imported into an Excel spreadsheet and converted into Newton (N) forces. The maximum force per finger per activity was calculated, and the activities were categorised into light, moderate, or heavy force groups. Specifically, activities with finger forces measuring between 0 and 3 N were classified as light, those between 3 and 7 N as moderate, and those exceeding 7 N as heavy. Upon completing the feasibility study the researcher identified and grouped the ADLs with similar grasp types and similar maximum forces within each category of light, medium, and heavy demand ADL, following the classification proposed by Feix et al.11 to place them in the same force category. A total of 31 ADLs were thus selected for measurement in this study. Information pertaining to the participants, instrumentation and testing procedures are now presented.
Participants
The research study included adult human participants residing and working in east Gauteng, specifically in the city of Kempton Park and its neighbouring areas within the Ekurhuleni municipality. The researcher purposively selected individuals from the local community, considering their age range (20-59 years), language spoken (English or isiZulu), and
their residence's proximity to the testing facility. Individuals under 20 years of age were excluded due to skeletal immaturity20, while those over 59 years of age were excluded based on literature suggesting a low incidence of metacarpal fractures in this age group21. Participants with previous hand injuries were also excluded. No incentives were provided for participation.
Instrumentation
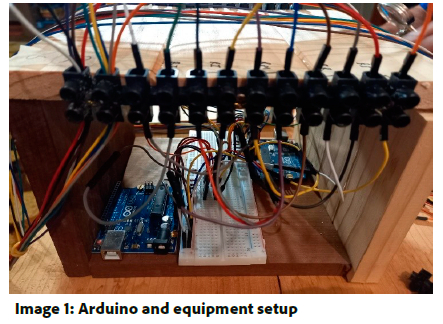
The instrumentation used to measure ADL forces was previously described in Keller et al.17. In brief, Flexiforce 13mm FSRs, ARDUINO Pro mini, 10 K 0.25 W resistors, ESP-01 kit, and Arduino UNO R3 compatible boards were utilised to capture the ADL grasp forces. The pressure applied to the tested object produced a resultant voltage (V) output, which was displayed on a software program visible to the researcher on a laptop or desktop computer. These V-values were then converted to forces, measured in Newton (N). The maximum force exerted during each ADL was recorded and saved in an Excel spreadsheet and FSRs detected forces exerted on the objects. The FSRs were connected in series with 10-Kohm resistors, which were inserted into the ARDUINO Pro mini. The FSRs were connected to the Arduino Pro Mini 5V via a USB port.
Arduino Uno hardware consists of circuit boards and a microcontroller placed on the Arduino Uno. The Arduino Uno is a programmable microprocessor specifically designed to record changes in V. An image of an Arduino Uno board is included in Image 1 (below). Each Arduino Uno board has the capability to monitor up to five FSRs. Therefore, in this study, two Arduino Uno boards were employed to monitor ten FSRs, one for each finger. The microcontroller chip, located on the circuit board's crystal resonator, controls the speed of the microcontroller's operations. This chip enables the upload of custom software from a computer to the main microcontroller via a USB cable, facilitating communication between the computer and Arduino.
To prepare the hardware for testing, the researcher downloaded Arduino software from the Arduino.cc website and installed it on their laptop. This software provided the necessary tools to create a sketch that could receive and process V measurements from the FSRs.
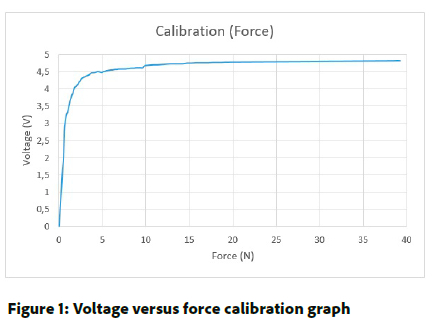
Prior to the experiments, the FSRs underwent calibration using a range of calibrated weights spanning from 1 gram to 10 kilogrammes (kg). For each weight, the corresponding V was recorded. This process enabled the researcher and technical expert to construct a graph illustrating the relationship between V and weight. By utilising the equation F = m × g, where F represents force in N, g is the gravitational acceleration (m/s2), and m is the mass (kg), the researchers converted the V measurements to forces. Figure 1 (below) presents the V versus force graph obtained from this calibration process. This graph allows the conversion of any recorded V from the Arduino's FSRs to a corresponding force value. To determine the general equation for the V force graph, a curve-fitting program was employed. The resulting equation was found to be 0.5917 * tan(0.3223 * max value). The Arduino's were programmed to capture ten measurements per second.
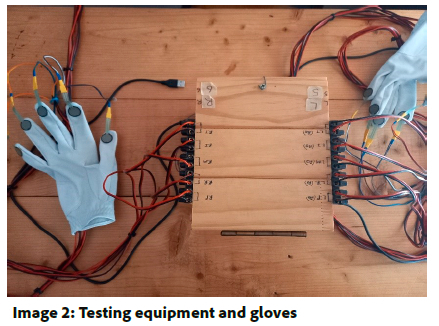
In order to measure the force exerted by each finger, two gloves were equipped with FSRs, with one FSR attached to each finger. Image 2 (below) depicts the gloves featuring the attached FSRs.
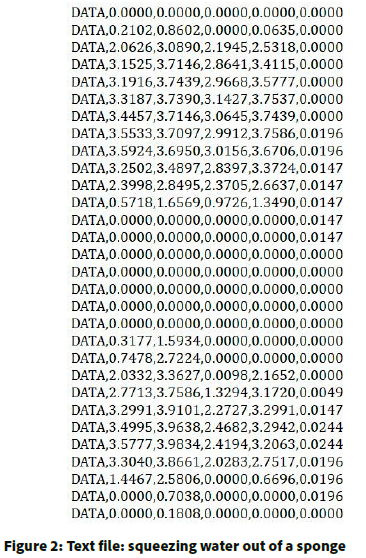
All measurements taken during the tasks were meticulously recorded and stored in comma-delimited text files. To facilitate this process, the software package Realterm was utilised. Subsequently, the comma-delimited text files were imported into Excel, where the V measurements were converted to forces using the aforementioned equation. An example of the text file capturing measurements from the five fingers of the left hand is presented in Figure 2 (below). For each grasp type, both the left and right hands, encompassing all ten fingers, were included in the text file. The researcher imported the data from the Excel spreadsheet into STRATA statistics software, using StataCorp, after which a statistician conducted data analysis.
Testing procedure
Pilot testing preceded the main data collecting during a feasibility study17. The researcher refined the design of the testing procedure and equipment after the feasibility study17. Changes made from the feasibility study are that golf gloves replaced household gloves, and the wires were positioned dorsally rather than volarly/palmarly on the hand. Stronger glue was used to secure the sensors to the gloves, applying the glue to all ten sensors and allowing five minutes for a more secure connection, as recommended by the glue manufacturer. To further prevent the sensors from detaching during testing, washing line pegs were used to secure the sensors to the gloves for five to ten minutes after gluing the FSRs to the gloves.
At the outset, participants underwent Covid-19 screening conducted by a proficient research assistant who had received thorough training in the screening process and was fluent in English and isiZulu. Subsequently, the participants completed a demographic questionnaire. Grip-strength measurements were then conducted using a calibrated Jamar hand-held dynamometer, following the standardised measurement guidelines outlined by the American Society of Hand Therapy. These grip-strength measurements preceded the force testing using FSRs. To ensure that the participants would not be fatigued and, that the validity of the force measurements, were not compromised, the grip-strength measurements with the hand-held dynamometer were taken by the primary author, after sixteen tasks and at the completion of the 31 tasks. Average grip strength of either the dominant or non-dominant hands differed by two kgs, based on an average of three maximal attempts, participants were granted an additional five minutes of rest before testing resumed. Through pilot testing, it was determined that five minutes provided sufficient resting time for participants to feel ready to continue with the testing.
Participants wore gloves with FSRs attached to both their right and left hands. After putting on the testing gloves, they were instructed to perform the tasks in a manner consistent with their normal activities at home. Participants performed ADLs such as putting washing on a washing line with pegs or dusting and squeezing water out of a sponge. Standardised instructions regarding data collection and testing procedures were provided to the participants. The researcher read out the tasks from the grasp types tested per type and per category sheet, ensuring that the necessary equipment for each task was within the participants' reach and that no additional objects needed to be manipulated, thereby allowing the FSRs to solely measure the forces exerted during the tasks.
Reliability and validity
Reliability was ensured through the utilisation of a single laboratory equipped with standardised, calibrated, and piloted FSRs and instrumentation. Grip strength testing employed a calibrated dynamometer. Both FSRs22 and the Jamar dynamometer23 have been established as valid tools for assessing forces and grip strength.
Data analysis
Descriptive statistics were employed to summarise the demographic characteristics of the participants as well as the finger force measurements. Two-sample t-tests were utilised to analyse differences in grip strength and force measurements based on gender.
Ethical considerations
This research was approved by the HSREC of the University of the Free State under the number (UFS-HSD2019/0046/2602-0002) obtained in 2021. Any associated research materials pertaining to the obtained results will be made accessible through the primary author's ORCID account.
RESULTS
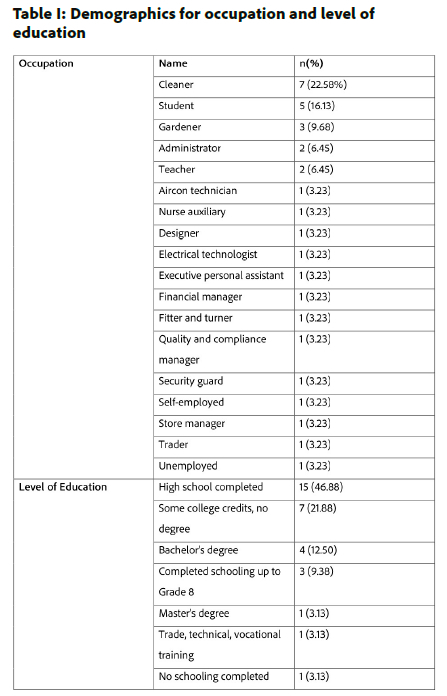
A total of thirty-two (32) participants, comprising 18 females and 14 males, with a mean age of 37 years, willingly agreed to take part in the study. Among the participants, two (6.25%) were left-handed, while the majority, thirty participants (93.75%), were right-handed. To gain insight into the participants' demographics, refer to Table I (adjacent), which provides information on their occupations and education levels.
Supplementary File 1 (attached as metadata) presents the means, standard deviations, as well as the minimum and maximum N force measurements for grasp force. For a detailed examination of maximum forces, please refer to Supplementary File 2 (attached as metadata). The grasp types per ADL were categorised into light, medium, and heavy demand categories, allowing us to identify which grasp types and ADLs could be employed in progressive hand rehabilitation. It is important to note that clinical reasoning should always guide hand rehabilitation, taking into consideration each individual patient's unique injury and comorbidities to ensure a safe rehabilitation process. The data provided in Supplementary File 2 is invaluable when prescribing a HEP with specific ADLs and grasp types. Each finger interacts with the manipulated object differently, and depending on the finger fracture and the individual's functional limitations, other ADL grasp types may be employed following an assessment. The precise results per category, as indicated in Supplementary File 2, will now be highlighted.
Light ADLs, accompanied by their associated grasp types11, which are suitable for individuals with injuries in any finger, include tasks such as dusting (light tool), operating a cellular phone (lateral), using a television remote (ventral), and handling money (lateral tripod). The medium force ADLs and their corresponding grasp types vary depending on the finger involved, and therapists should refer to the supplementary files to guide their prescription and utilisation in hand rehabilitation. Heavy demand ADLs and grasp types, which should be delayed to ensure proper bone healing, include activities such as squeezing water out of a sponge (power sphere), drying clothes (medium wrap), opening and closing large round taps (quadpod), opening tight or new jars (four-finger sphere and precision disk), and lifting a 25 kg box (adducted thumb).
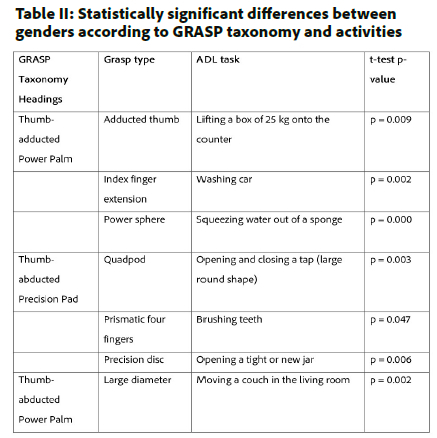
An analysis of the force measurements for grasp types per ADL task, conducted using the GRASP Taxonomy11 and presented with the results of the t-test of equal variance in Table II (below), revealed statistically significant gender differences. However, no statistically significant difference in grasp forces was observed for the remaining 25 tested tasks.
Furthermore, a two-sample t-test with equal variance was performed to assess gender differences in grip strength measurements taken prior to the force testing. The results indicated no statistically significant difference, with p = 0.0958.
DISCUSSION
When comparing the data for healthy participants in this research to the results of Riddle et al.12, some similarities can be observed. The age ranges of the healthy participants in Riddle et al.'s study (20 to 65 years) and the participants in this study are relatively close, with ages ranging from 20 to 59 years for the collection of force data. However, it should be noted that the individual finger forces collected by Riddle et al. for the osteoarthritic group12 cannot be directly compared to the findings of this research.
In another study by Castro and Cliquet14, the range of forces measured for different weights and finger positions was documented. For example, for the index and middle fingers, a 0.2 kg weight resulted in forces ranging from zero to one-and-a-half N, while a 1.02 kg weight led to forces ranging from zero to seven N. Comparing these grasp forces to the findings of the present study, similar forces ranging from zero to seven N were observed during tasks involving cylindrical object manipulation. Additionally, Romeo et al.15 measured forces exerted by the thumb, index finger, and middle finger, allowing for a comparison of these three fingers. The forces in their study ranged from 0.3N to a maximum of 2.7N. Comparatively, in this research, the average maximum forces per finger during the power-sphere grasp were as follows: thumb 2.44N, index finger 1.48N, middle finger 1.38N, ring finger 1.66N, and little finger 0.21N. These findings align with the previous study, even though the FSRs in this research were mounted on the fingers of a glove rather than the manipulated object.
Several studies investigating finger and grasp forces have explored potential associations with gender. Rice, Leonard, and Carter13 and Castro and Cliquet14 found significant differences in grip and pinch strength measurements between genders but did not observe significant differences in the forces exerted. Similarly, in this study, the majority of grasp types (78%) showed no statistically significant difference between male and female participants. The identification of grasp types in ADL and the maximum grasp forces measured in this research offer valuable exercise options for physiotherapists and occupational therapists to incorporate into hand rehabilitation and home exercise prescriptions after hand fractures such as second to fifth metacarpal fractures.
CONCLUSION AND LIMITATIONS
The collection of force-sensing data during the 31 ADL tasks provided a substantial contribution to the existing knowledge base, shedding light on different hand manipulations. However, due to the inherent complexities and individual differences among participants, drawing absolute conclusions from the data remains challenging, even with larger sample sizes. It is important to acknowledge that the use of FSRs on gloves to measure grasp forces may introduce variations compared to grasping without gloves, as the hand relies on sensory feedback from the skin.
While the error rate on the FSR sensors during testing was minimal and no data was lost, future research should consider increasing the sample size and directly attaching FSRs to the skin. Additionally, efforts should be made to ensure a balanced representation of genders, handedness, and various occupations, as the current sample primarily consisted of students and cleaners, limiting the generalisability of the study's findings.
The insights gained from this study's findings have implications for the development of clinical hand rehabilitation guidelines, particularly regarding the forces involved in predominant grasp types. These findings can inform physiotherapists and occupational therapists in designing effective exercise programmes and prescribing home exercises for individuals who sustained second to fifth metacarpal fractures.
Clinical Implications
Incorporating grasp types as free active exercises while the injured finger is immobilised may be started early to maintain joint range of motion and improve hand function. The researcher suggests that starting ADLs falling into the light category with immobilisation may be beneficial as long as no pain is experienced, and the treating doctor has been consulted about early functional rehabilitation and HEP. Clinical reasoning should be used, as well as the extent of the fracture and associated injuries.
Author contributions
Monique Keller proposed the topic for the research, wrote the protocol for ethical approval and the first version of the article. The protocol and article were read, elaborated upon, and refined by Monique Keller, Roline Barnes and Corlia Brandt.
Acknowledgements:
The authors acknowledge Thomas Feix for permitting the use of the GRASP Taxonomy, Paul Keller and JeanPaul Heynek for their technical support, the participants, and Zvifadzo Matsena Zingoni at the University of the Witwatersrand for her statistical assistance.
Conflicts of interest
None to declare.
REFERENCES
1. UKEssays. The Major Function Of Human Hand Psychology Essay [Internet]. November 2018. [Accessed 12 December 2023]; Available from: https://www.ukessays.com/essays/psychology/the-major-function-of-human-hand-psychology-essay.php?vref=1. [ Links ]
2. Robinson LS, Sarkies M, Brown T, O'Brien L. Direct, indirect and intangible costs of acute hand and wrist injuries: A systematic review. Injury, 2016; Dec; 47(12): 2614-2626. http://dx.doi.org/10.1016/j.injury.2016.09.041. [ Links ]
3. Gudmundsen TE, Borgen L. Fractures of the fifth metacarpal. Acta Radiologica, 2009; Apr; 50(3): 296-300. http://dx.doi.org/10.1080/02841850802709201. [ Links ]
4. Groth GN, Wilder DM, Young VL. The impact of compliance on the rehabilitation of patients with mallet finger injuries. Journal of Hand Therapy, 1994; 7(1): 21-24. http://dx.doi.org/10.1016/s0894-1130(12)80037-8. [ Links ]
5. Gülke J, Leopold B, Grözinger D, Drews B, Paschke S, Wachter NJ. Postoperative treatment of metacarpal fractures-Classical physical therapy compared with a home exercise program. Journal of Hand Therapy, 2018; Jan 1: 31(1): 20-28. https://doi.org/10.1016/j.jht.2017.02.005. [ Links ]
6. Valdés K, Naughton N, Algar L. Usefulness of a hand therapy application. Journal of Hand Therapy, 2022; 35(4): 569-574. http://dx.doi.org/10.1016/j.jht.2021.03.007. [ Links ]
7. Kimmerle M, Mainwaring L, Borenstein M. The functional repertoire of the hand and its application to assessment. American Journal of Occupational Therapy, 2003;57:489-98. http://dx.doi.org/10.5014.ajot.575.489 [ Links ]
8. Valdés K, Naughton N, Cantero-Téllez R, Szekeres M. The use of occupation-based interventions and assessments in hand therapy: A cross-sectional survey. Journal of Hand Therapy, 2023;Jan1;36(1):214-220. https://doi.org/10.1016/j.jht.2021.10.008. [ Links ]
9. Bullock IM, Zheng JZ, De La Rosa S, Guertler C, Dollar AM. Grasp frequency and usage in daily household and machine shop tasks. IEEE Trans Haptics, 2013; 6(3): 296-308. http://dx.doi.org/10.1109/TOH.2013.6. [ Links ]
10. Sperling L, Jacobson-Sollerman C. The grip pattern of the healthy hand during eating. Scandinavian Journal of Rehabilitative Medicine, 1977;9(3):115-21. [ Links ]
11. Feix T, Romero J, Schmiedmayer HB, Dollar AM, Kragic D. The GRASP Taxonomy of Human Grasp Types. IEEE Trans Human-Machine Systems, 2016;46(1):66-77. http://dx.doi.org/THMS.2015.2470657. [ Links ]
12. Riddle M, MacDermid J, Robinson S, Szekeres M, Ferreira L, Lalone E. Evaluation of individual finger forces during activities of daily living in healthy individuals and those with hand arthritis. Journal of Hand Therapy, 2020; 33(2): 188-197. http://dx.doi.org/10.1016/j.jht.2020.04.002. [ Links ]
13. Rice MS, Leonard C, Carter M. Grip Strengths and Required Forces in Accessing Everyday Containers in a Normal Population. American Journal of Occupational Therapy, 1998; 52(8):621-626. http://dx.doi.org/10.5014/ajot.52.8.6.621. [ Links ]
14. Castro MCF, Cliquet A. J. A low-cost instrumented glove for monitoring forces during object manipulation. IEEE Trans Rehabilitative Engineering, 1997; 5(2): 140-147. http://dx.doi.org/10.1109/86.593280. [ Links ]
15. Romeo RA, Cordella F, Zollo L, Formica D, Saccomandi P, Schena E, et al. Development and preliminary testing of an instrumented object for force analysis during grasping. Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2015; 2015: 6720-6723. http://dx.doi.org/10.1109/EMBC.2015.7319935 [ Links ]
16. LaStayo PC, Winters KM, Hardy M. Fracture healing: Bone healing, fracture management, and current concepts related to the hand. Journal of Hand Therapy, 2003; 16(2): 81-93. http://dx.doi.org/10.1016/s0894-1130(03)80003-0. [ Links ]
17. Keller MM, Barnes R, Brandt C. Evaluation of grip strength and finger forces while performing activities of daily living. Occupational Health Southern Africa, 2022; 28(5): 187-190. https://journals.co.za/doi/abs/10.10520/ejc-ohsa_v28_n5_a6 [ Links ]
18. Hudak PL, Amadio PC, Bombardier C. Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand) [corrected]. The Upper Extremity Collaborative Group (UECG). American Journal of Industrial Medicine. 1996; 29(6): 602-608. Erratum in: American Journal of Industrial Medicine, 1996; 30(3): 372. PMID: 8773720. http://dx.doi.org/10.1002/(SICI)1097-0274(199606)29:6<602:AID-AJIM4>3.0.CO;2-L. [ Links ]
19. Han W, He W, Yang W, Li J, Yang Z, Lu X, et al. The osteogenic potential of human bone callus. Scientific reports. Nature Publishing Group, 2016; 6: 36330. http://dx.doi.org/10.1038/srep36330. [ Links ]
20. De Sanctis V, Di Maio S, Soliman A, Raiola G, Elalaily R, Millimaggi G. Hand X-ray in pediatric endocrinology: Skeletal age assessment and beyond. Indian Journal of Endocrinology and Metabolism, 2014; 18: S63-71. http://dx.doi.org/10.4103/2230-8210.145076. [ Links ]
21. Nakashian MN, Pointer L, Owens BD, Wolf JM. Incidence of metacarpal fractures in the US population. Hand, 2012; 7(4): 426-430. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3508027/pdf/11552_2012_Article_9442.pdf. http://dx.doi.org/10.1007/s11552-012-9442-0. [ Links ]
22. Sadun AS, Jalani J, Sukor JA. Force Sensing Resistor (FSR): a brief overview and the low-cost sensor for active compliance control. Proceedings of SPIE, 2016, Jul 11. https://doi.org10.1117/12.2242950. [ Links ]
23. Mathiowetz V. Comparison of Rolyan and Jamar dynamometers for measuring grip strength. Occupational Therapy International, 2002: Aug 1; 9(3): 201-209. https://doi.org/10.1002/oti.165 [ Links ]
 Correspondence:
Correspondence:
Monique Keller
Email: Monique.keller@wits.ac.za
Submitted: 15 August 2023
Reviewed: 21 October 2023
Revised: 19 December 2023
Accepted: 21 December 2023
Editor: Blanche Pretorius https://orcid.org/0000-0002-3543-0743
Data availability: Available on request from corresponding author.
Funding: The study was funded by the FRC Seed funding grant (001 254 8491105 5121105 000000 0000000000 5254) obtained from the University of the Witwatersrand and the South African Society of Physiotherapy Research Foundation grant (RF2020/08/01).
Supplementary Data
The supplementary data is available in pdf: [Supplementary data] [Supplementary data 2]

