










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.53 n.3 Pretoria Dec. 2023
http://dx.doi.org/10.17159/2310-3833/2023/vol53n3a7
RESEARCH ARTICLE
Cross-cultural adaptation of the administration instructions of the Developmental Test of Visual Perception (3rd Edition) for isiZulu-speaking children
Sumarié NaudeI, II, III; Catharina Jacoba Elizabeth UysI; Belia Margaretha BekkerIV
IDepartment of Occupational Therapy, University of Pretoria, South Africa; Sumarie Naude: http://orcid.org/0000-0001-7338-8323; Catharina Jacoba Elizabeth Uys: http://orcid.org/0000-0001-9722-9941
IIAt time of study: Post graduate student at Department of Occupational Therapy, University of Pretoria, South Africa
IIICurrent: Occupational Therapist for Department of Education (Prospectus Novus School) Pretoria, South Africa
IVPrivate practice, Pretoria, South Africa; http://orcid.org/0000-0002-3310-3810
ABSTRACT
INTRODUCTION: Visual perceptual skills are vital for developing academic skills and contribute to language development and socio-cultural participation. The Developmental Test of Visual Perception 3rd Edition evaluates visual perceptual skills but is only available in English. lsiZulu is the most spoken language in South Africa (24,4%), with English being the fourth. Therefore, the English version of the Developmental Test of Visual Perception 3rd Edition cannot be described as a universally authentic assessment instrument in this context.
METHODOLOGY: This study aimed to translate and cross-culturally adapt the Developmental Test of Visual Perception 3rd Edition administration instructions into isiZu lu using a five-stage qualitatively driven multimethod sequential design. Qualitative feedback on the functional, cultural and conceptual equivalence was obtained at various intervals.
RESULTS: This study demonstrated a methodology for translating and cross-culturally adapting the administration instructions of the Developmental Test of Visual Perception 3rd Edition into isiZulu to advance the authenticity of the assessment within the South African context. The isiZulu version was found to be functionally, culturally and conceptually equivalent.
CONCLUSIONS: This research has demonstrated a framework upon which the cross-cultural adaptations of other assessment instruments and other languages in South Africa can be based.
IMPLICATIONS FOR PRACTICE:
• The rigorous methodology demonstrated in this research can be used as a framework to guide other studies in the translation and cross-cultural adaptation of other assessment instruments and into other languages.
• This study demonstrated that multiple contributors from various backgrounds are necessary to ensure equivalence during the process of translation and cross-cultural adaptation. However, an emphasis is placed on the value of including occupational therapists with clinical experience when translating and cross-culturally adapting assessment instruments intended to be used within the field of occupational therapy.
• Through the rigorous method used to translate and cross-cultural adapt the DTVP-3, this study enhanced its authenticity as an assessment instrument within the South African context. Having isiZulu administration instructions available could provide equal opportunity to children who may not be as proficient in English as in isiZulu.
• Once a distribution agreement has been reached with ProEd Inc., the original publisher and licence holder, the isiZulu administration instructions of the DTVP-3 will be made available for use in South Africa with isiZulu-speaking children.
Keywords: authentic assessment practice, functional equivalence, cultural equivalence, conceptual equivalence, linguistic translation, cross-cultural adaptations, assessment instrument
INTRODUCTION AND LITERATURE REVIEW
This article presents the rigorous method used to translate and cross-culturally adapt the Developmental Test of Visual Perception Third Edition (DTVP-3) administration instructions into isiZulu while maintaining its functional, cultural and conceptual equivalence. This cross-cultural adaptation was done in advocacy for improved authentic assessment practices in evaluating visual perceptual skills among isiZulu-speaking children in South Africa.
Visual Perception
Schneck defines visual perception as the process incorporating the reception and cognition of stimuli perceived by the visual system1. The components of visual perception are essential for the processing and interpreting of information gained through the visual system. Therefore, it constitutes the ability to derive functional meaning from the visual world12. Visual-motor functions and visual perception support a child's ability to engage in meaningful educational occupations such as reading, writing and other school-related tasks3,4. Visual perceptual development has also been linked to developing functional skills such as attention, social interaction and motor development in childhood5.
The evaluation of visual perceptual skills and how they impact occupational engagement falls within the scope of occupational therapy intervention3. The American Occupational Therapy Association outlines the occupational therapy process as consisting of evaluation, intervention and targeting intervention outcomes within the client's functional context3. Therefore, it is imperative that occupational therapists have authentic assessment instruments to accurately evaluate skills and subskills to identify deficiencies and inform efficient intervention and effectively target outcomes13. Many of the characteristics of authentic assessment, such as evaluating occupational performance within appropriate contexts and taking into account the impact of the environment on occupational functioning, is well established within the profession of occupational therapy3,6.
Authentic Assessment
Authentic assessment is an alternative to traditional evaluation procedures and was born within the context of early childhood intervention (ECI)7. It advocates for using developmentally appropriate evaluation methods within an environment that emulates the functional setting within which the child would naturally perform the skills under investigation8. Conventional testing is argued to introduce limits in terms of content, procedures, process and evidence, which may lead to mismeasurement of a child's abilities in an unnatural context and deny their rights to beneficial expectations and opportunities8-11. Such mismeasurement misrepresents the child and instead of highlighting competence within uniqueness, may over-emphasize the child's limitations8,10,11 . Bagnato et al. have emphasized eight major standards for developmentally appropriate and authentic assessment instruments and procedures based on over 25 years of collaborative documents compiled by many major national professional organizations8. These standards are acceptability, authenticity, collaboration, evidence, multi factors, sensitivity, universality and utility.
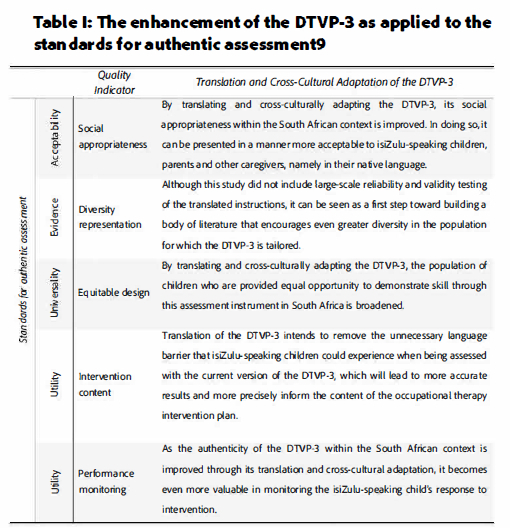
Each standard can be described using quality indicators which highlight aspects important for ensuring that the standards are upheld. These standards can be considered an ideal for which ECI assessment instruments and occupational therapy assessment practices should strive. This study has focused on specific quality indicators that fall under the standards of acceptability, evidence, universality and utility. These quality indicators are social appropriateness, diversity representation, equitable design, intervention content and performance monitoring. When applied to the DTVP-3, these quality indicators are enhanced through translation and cross-cultural adaptation as shown in Table I (below)
The Developmental Test of Visual Perception
The DTVP was one of the first visual perceptual tests to be developed based on statistically established norms8. It has gained popularity since the second edition was released8. The third and latest edition (the DTVP-3) is widely used by occupational therapists to evaluate visual perceptual skills.
The DTVP-3 consists of five subtests evaluating eye-hand coordination, copying, figure-ground, visual closure and form constancy12. It can be administered to inform intervention strategies and measure the effectiveness of an intervention12. This link between the assessment instrument and the therapeutic outcomes is a characteristic of authentic assessment practices13.
The majority of the children seen by occupational therapists have already been identified as a potentially compromised population before obstacles to their occupational engagement could be further compounded by language barriers. In previous studies, the administration ofthe DTVP within the South African context was consistently conducted in English, except for one study, which did not elaborate on the method used to translate it into Afrikaans14. However, according to the 2022 census, the most represented first-spoken languages in the South African population were isiZulu (24,4%), isiXhosa (16,3%), Afrikaans (10,6%) and English (8,7%)15. The most represented first-spoken language in the province of Gauteng in 2022 was also isiZulu (23.1%)15. Hence, a significant representation of children evaluated using the DTVP-3 do not have access to it in their home language. Therefore, it cannot be considered an authentic assessment instrument for these children8,16.
Translation
Direct or linguistic translation of assessment instruments has been utilized in various contexts. A method of linguistic translation is crowdsourcing the translation through online open translation tools. However, one study experienced difficulties in quality assurance of the translation and establishing its suitability for different contexts17. In another study, Guo investigated the viability of using a machine translator, such as Google Translate, but found various challenges and shortfalls rendering this method insufficient when used in isolation18. Another method is reflected in a published case study by Jones et al19. While translating elements of the ABA intervention programme from English to Welsh, Jones et al. found it necessary to establish new terminology for key concepts19. Methods they used to devise new terminology included adaptation (allowing old words to gain new meaning), derivation and neologisms19. As part of this case study, it was also experienced that direct translation by professional translators tended to be inadequate in maintaining grammatical fluency. The technically correct translations also failed to capture the intent of the original text19.
Many authors have stressed that mere linguistic translation is insufficient to modify an assessment instrument for use with a different population group20-27. Instead, an instrument must be cross-culturally adapted to ensure equivalence and avoid potential sources of bias20-22,28. Pena emphasizes that merely meeting the requirements of equivalence is insufficient for an instrument to be cross-culturally adapted. It must also meet the requirements of functional, cultural and metric equivalence22.
Linguistic equivalence can be facilitated through the backward translation method of translating from the source language to the target language, followed by back-translation from the target language back to the source language by a translator unfamiliar with the original text. Then the original text and back-translated text are compared for discrepancies and consolidated22 Another method to ensure linguistic equivalence is through review by a native speaker of the target language22. Functional equivalence ensures that the same response or behaviour will be elicited in the target language as was intended in the source language29. One of two methods is often employed to facilitate functional equivalence22.One method is decentring, whereby wording in the target language may shi ft away from the original wording to prioritize linguistic familiarity22,30. Another method is adopting a dual focus in which the instrument is developed in both languages simultaneously22. Cultural equivalence emphasizes the degree to which different cultural and linguistic groups interpret and respond to the perceived meaning conveyed by the instrument items22,28.Cultural equivalence is closely related to functional equivalence22 Conceptual (or metric) equivalence is an evaluation of whether the difficulty of an item is comparable in both the source and target languages by taking into account the frequency with which it occurs in that language. According to Pena, using parallel vocabulary measures, which focus on word frequency comparisons between the source and target languages, may encourage metric equivalence during translation22.
It is clear that instruments used cross-culturally need to b equivalent on many levels to provide an equal opportunity to demonstrate skill22,24,31. Many authors reiterate that a translation should meet the basic standards set for all measures in that it must be reliable, valid, legal, and cost-effective, as well as meet the requirements for equivalence beyond mere linguistic translation20,22-25,27,28,31,32.
Various methods of cross-cultural adaptation have been recommended throughout literature20,21,23-25,27,32,26. Sousa and Rojjanasrirat have suggested a method for translation based on their review of methodological studies, focusing on the cross-cultural adaptation of instruments and scales within the context of health care research20. This method is based on seminal work by Guillemin, Bombardier and Beaton20,33,36. They recommend the following steps as a guideline:
Step 1: Translation of the original assessment instrument into the target language (forward translation) by at least two independent translators20,24,25,27,28,35. These translators produce the target language translations one (TL1) and two (TL2) respectively. The translators should have the target language (TL) their mother language and have experience in the culture and colloquialisms of the TL20.
Step 2: Comparison of TL1 and TL2 by a third bilingual, bicultural independent translator and a committee approach to resolving any discrepancies20,36. The committee consists of the two initial translators, the third independent translator and the researcher20. This committee reaches an agreement to produce the preliminary, initial translated version (P1-TL)20,27.
Step 3: Blind, backward translation of the P1-TL back to the original language (SL) by two other independent translators20,35,36. The mother language of the translators involved in this step should be the SL. However, they should be fluent in both the SL and the TL20. It is essential that the translators involved in the back-translation not be familiar with the original assessment instrument to avoid previous exposure from influencing the back-translation, thereby ensuring a blind back-translation20,24. They will produce two backward translated versions (B-TL1 and B-TL2)20.
Step 4: A multidisciplinary committee compares B-TL1 and B-TL2 to the SL20,35. This committee should consist of the researcher, all four translators involved in steps 1 and 3, a healthcare worker familiar with the original assessment instrument and at least one monolingual person whose mother language is the TL20. This committee then resolves any ambiguities or discrepancies between the SL, B0TL1 and B-TL2 to produce the pre-final version in the target language (P-FTL)20.
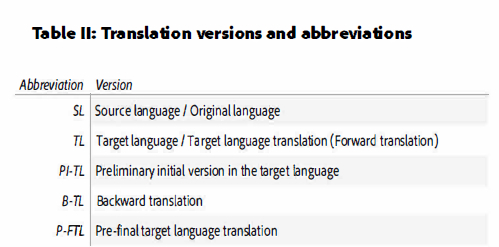
Step 5: Pre-test the P-FTL among participants whose language is the target language20,21,24,25. These participants whould be representative of the target population for which the translation is intended, and the use of a dichotomous scale (clear or unclear), is recommented20. Table II (page 57) summarizes the multiple translation versions and their respective abbreviations.
It is clear from the literature that cross-cultural translation of an assessment instrument requires a systematic and methodological approach for equivalence to be maintained20,22,24,28. Receiving administration instructions in a language other than the child's first language could have a detrimental effect on the child's opportunity for equal performance and does not align with the standards of authentic assessment22,24. Placing a child in such a situation could lead to mismeasurement and misrepresentation of the child's abilities8. Since isiZulu is the most represented spoken language in South Africa; there is a significant need for cross-cultural adaptation of the administration instructions of the DTVP-3 to isiZulu. This article reports on the rigorous process necessary to translate and cross-culturally adapt the administration instructions of the DTVP-3 into isiZulu.
METHODOLOGY
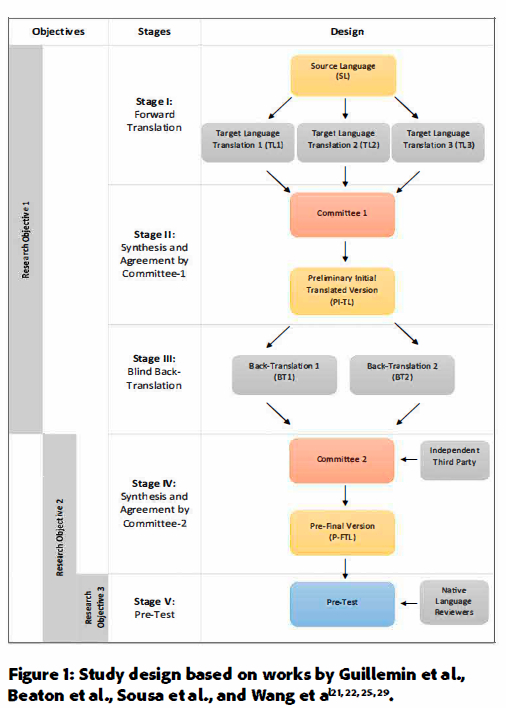
This study aimed to cross-culturally adapt the instructions of the DTVP-3 using a combination of the methods suggested in literature; as well as examining the functional, cultural and conceptual equivalence after translation into isiZulu to improve the authenticity of the DTVP-3 as an assessment instrument within the South African context8,20,22,28. The study's objectives were as follows: Objective 1: To translate the administration instructions of the DTVP-3 into isiZulu linguistically22. Objective 2: To examine whether the isiZulu translation represents a cross-cultural adaptation which satisfies the standard for ensuring functional22, cultural22, and conceptual20 equivalence. Objective 3: To conduct a pre-test study to provide preliminary feedback on whether the adaptation is comprehensible for the isiZulu-speaking child in the Tshwane (Gauteng Province, South Africa) area. This qualitatively driven multimethod sequential study followed the ethical principles of human research and received approval from the Faculty of Health Sciences Research Ethics Committee (Ethics Approval: 459/2020)37. Figure 1 (page 58) presents the five stages of the design and is based on work by Guillemin et al., Sousa et al., Wang et al., and Beaton et al20,21,24,28. Each stage implements one or more of the research objectives. Therefore, the study design has been described in reference to the objectives.
Objective 1: To translate the administration instructions of the DTVP-3 into isiZulu linguistically
Stage I: Forward Translation: The original version was linguistically translated from the source language (SL), English, into the target language (TL), isiZulu, using three independent translators. Translator 1 was a native isiZulu-speaking occupational therapist trained in the administration of the DTVP-3. Translator 2 was a bilingual isiZulu-speaking layperson unfamiliar with the DVTP-3 but familiar with colloquialisms, slang and contextual interpretations of the target language. Translator 3 was a bilingual and bicultural third party trained in teaching languages to children. Translators 1, 2 and 3 produced target language translation 1 (TL1), target language translation 2 (TL2) and target language translation 3 (TL3), respectively.
Stage II: Synthesis and Agreement by Committee-1: Next, TL1, TL2 and TL3 were compared by committee-1, who discussed and resolved any discrepancies between the three translations to synthesize the preliminary initial translated version in the target language (PI-TL). Committee-1 consisted of translator 1, translator 2, translator 3 and the researcher.
Stage III: Blind Back-Translation: During stage III, the PI-TL was translated back into the SL by two other independent translators. Translator 4 was a healthcare professional unfamiliar with the DTVP-3. Translator 5 was a bilingual and bicultural layperson. Translators 4 and 5 produced back-translation 1 (BT1) and back-translation 2 (BT2), respectively. Both back-translators were unfamiliar with the original assessment instrument to preclude previous exposure to the original SL administration instructions from influencing the backward translation.
Objective 2: To examine whether the isiZulu translation represents a cross-cultural adaptation which satisfies the standard for ensuring functional, cultural, and conceptual equivalence.
Stage IV: Synthesis and Agreement by Committee-2: At this stage, committee-2 compared the SL, PI-TL, BT1 and BT2 versions. The committee discussed and resolved discrepancies to synthesize the pre-final version in the target language (P-FTL). Committee-2 consisted of translator 1 (TL1 translator), translator 2 (TL2 translator), translator 3 (TL3 translator), translator 4 (BT1 translator), translator 5 (BT2 translator), the researcher, and an independent isiZulu-speaking third party. This independent third party was a native isiZulu-speaking professional trained in administering the original assessment instrument. By including a native isiZulu speaker who was also a trained professional, the quality of the P-FTL was enhanced. This third party contributed relevant clinical experience in administering the assessment instrument with isiZulu-speaking children.
Following the conclusion of stage IV, the committee-2 discourse was analysed for themes of functional, cultural and conceptual equivalence. This analysis was verified by an external rater through a random sampling of 42%.
Objectives 2&3:To conduct a pre-test study to provide preliminary feedback on whether the adaptation is comprehensible for the isiZulu-speaking child in the Tshwane (Gauteng Province, South Africa) area
Stage V: Pre-test: During the pre-test stage, the newly translated and adapted isiZulu version of the administration instructions was used by isiZulu-speaking occupational therapists to administer the DTVP-3 to isiZulu-speaking children. The administering therapists first attended a virtual refresher on the administration procedures and received the isiZulu administration instructions on identical cue cards. These measures were undertaken to minimise administrator variability.
After each administration, the child provided qualitative descriptive feedback regarding his/her experience using a feedback questionnaire. The administering therapist assisted each child in recording his/her response to the questionnaire. Each participating occupational therapist also provided feedback on the functional, cultural and conceptual equivalence of the isiZulu administration instructions by completing an equivalence feedback questionnaire (adapted from Hambleton and Zenisky's Translation and Adaptation Review Form)31,32. The questions of the equivalence feedback form were analysed for themes of functional, cultural and conceptual equivalence.
As part of stage V, two native language reviewers also provided feedback on the equivalence of the isiZulu translation through the equivalence feedback questionnaire22. The two native isiZulu speakers were occupational therapists with experience in administering the DTVP-3 who had not been involved in stages I to IV.
Population
During stages I to IV, the target population consisted of professionals and laypersons fluent in isiZulu based in KwaZulu-Natal Province, Free State Province, North West Province and Gauteng Province, South Africa. The stage V pre-test represented three population groups. The first target population for stage V was isiZulu-speaking children between the ages of seven years two months and ten years seven months attending primary schools in Tshwane, Gauteng Province, South Africa. The second population of stage V was isiZulu-speaking administering therapists. These were occupational therapists practising in Tshwane, Gauteng, South Africa. The therapists were not known to the children prior to the study. The third population of stage V was native language reviewers based in KwaZulu-Natal Province, South Africa.
Sampling method and sample size
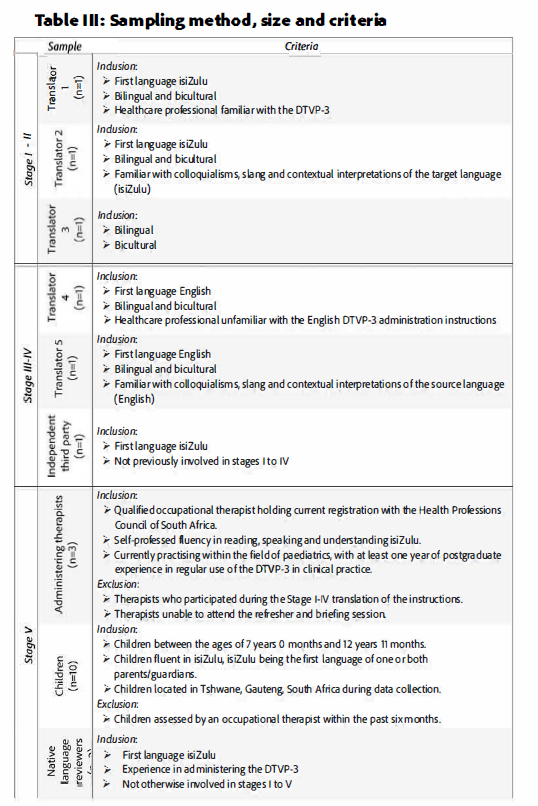
The stages I to IV participants were recruited using purposive snowball sampling from the researcher's and supervisors' network of professional acquaintances and colleagues. Translators 1 to 5 and the independent third party were recruited to meet specific criteria as shown in Table II (page 59)
The stage V administering therapists and native language reviewers were recruited using purposive snowball sampling through acquaintances, colleagues, fellow postgraduate students, and school-based occupational therapists' professional networks. It should be noted that stage V represents a pre-test (not a pilot study); therefore, a small sample size was used to gain initial feedback from the target population before a pilot study is conducted20.The second target population of stage V was children from primary schools in the vicinity of the administering occupational therapists. The sample of children was recruited by contacting local schools. After permission from the Gauteng Department of Education (GDE) and the principals of each primary school was obtained, information was made available to the parents. This information explained the details of the study and invited their children to participate voluntarily. The third population of stage V was the native language reviewers, who were recruited using purposive snowball sampling of acquaintances, colleagues, fellow postgraduate students, and school-based occupational therapists' professional network.
Data Collection and Analysis
The data collected in stage I (TL1, TL2 and TL3) was tabulated and underwent a content comparison. Discrepancies between the versions were noted for discussion in stage II by committee-1.
The discrepancies and agreements reached by the committee-1 members were detailed and tabulated, as demonstrated by Pasin et al38. The data collected during stage III (BT1 and BT2) were combined in table form and underwent a content comparison with the SL. Discrepancies between the versions were noted for discussion by committee-2, who compared the original SL, PI-TL, BL1 and BL2. The discussion points of committee-2 were recorded, and the researcher noted whether they related to functional, cultural and conceptual equivalence. A random sample (42%) of the recording and observations regarding equivalence made was verified by an external rater.
The data collected from stage V also underwent content analysis. The responses to the child feedback questionnaire (completed by the isiZulu-speaking children) and equivalence feedback questionnaire (completed by the administering therapists and native language reviewers) were summarized as recommended by the ITC Guidelines for Test Translation and Adaptation32.
RESULTS
Stages I - IV
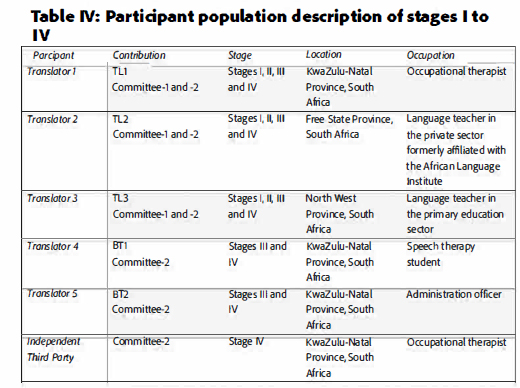
This study proceeded through five rigorous stages of translation and cross-cultural adaptation. Table IV (below) describes the demographics of the participants in stages I to IV As shown in this table, the participants represented various locations in the provinces of KwaZulu-Natal, Free State, North West and Gauteng, contributing a variety of vernaculars which broadened the translation beyond the dialect of a single province.
As part of stage I, the translators completed the forward translation of the DTVP-3 administration instructions to produce the three isiZulu versions (TL1, TL2 and TL3). Google Translate, and the researcher's basic familiarity with elementary isiZulu, were used to prepare the comparison of SL, TL1, TL2 and TL3 by numbering the corresponding sentences. This numbering was done to ease the comparison of translated versions and facilitate verbal referencing of specific sentences during stage II.
The stage II committee-1 meeting took place on a virtual platform. The members of committee-1 were translator 1, translator 2, translator 3 and the researcher. During this committee, the members compared TL1, TL2 and TL3. They collaborated to adapt or correct discrepancies between the translations, reaching an agreement on the version that would become PI-TL. The administration instructions consisted of 46 numbered sentences, each discussed individually by committee-1.
Committee-1 collaborated to alter or combine TL1, TL2 and TL3 in 61% of the sentences. In 4% of the sentences, either TL2 or TL3 were agreed upon as the PI-TL without alteration. In 35% of the sentences, TL1 was agreed upon by all members as the PI-TL without alteration. These unaltered sentences from TL1 were judged as the most appropriate and easily understandable wording. TL1 appeared to consist of shorter, more concise sentences.
This numbering was done to ease the comparison of translated versions and facilitate verbal referencing of specific sentences during stage II.
The stage II committee-1 meeting took place on a virtual platform. The members of committee-1 were translator 1, translator 2, translator 3 and the researcher. During this committee, the members compared TL1, TL2 and TL3. They collaborated to adapt or correct discrepancies between the translations, reaching an agreement on the version that would become PI-TL. The administration instructions consisted of 46 numbered sentences, each discussed individually by committee-1. Committee-1 collaborated to alter or combine TL1, TL2 and TL3 in 61% of the sentences. In 4% of the sentences, either TL2 or TL3 were agreed upon as the PI-TL without alteration. In 35% of the sentences, TL1 was agreed upon by all members as the PI-TL without alteration. These unaltered sentences from TL1 were judged as the most appropriate and easily understandable wording. TL1 appeared to consist of shorter, more concise sentences. Since the occupational therapist produced TL1, it could be argued that experience in working with the target audience (namely young children) and relevant experience in administering the DTVP-3 was a significant asset during the translation process.
During stage Ill, translators 4 (BT1) and 5 (BT2) blind back-translated the PI-TL from isiZulu into English. Translator 4 and translator 5 were specially selected to have no prior familiarity with the SL. The majority (74%) of the 46 sentences revealed no discrepancy between the SL, BT1 and BT2. Therefore, most sentences were accurately translated during stages I and II. Of the 46 sentences, 26% (n=12) revealed some discrepancies.
The stage IV committee-2 meeting was conducted virtually where the members compared the SL, PI-TL, BT1 and BT2, deliberated on the discrepancies and reached an agreement to produce the P-FTL. The members of committee-2 were translator 1, translator 2, translator 3, translator 4, translator 5, an independent third party and the researcher. T
Table V (page 60) shows an analysis of the discourse during committee-2. Committee-2 judged PI-TL as the most accurate version in 33% of the sentences with discrepancies. In these instances, PI-TL was accepted as the P-FTL without alteration. Of the sentences which contained discrepancies, 67% were discussed by the committee-2 members who collaborated and produced P-FTL while considering various factors of equivalence (i.e. functional, cultural and conceptual equivalence). The equivalences described in Table V were not mutually exclusive, and some sentences enjoyed consideration of multiple sub-characteristics.
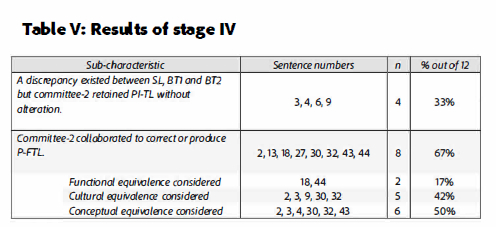
When considering the 12 sentences which revealed discrepancies, cultural equivalence was the main discussion point for 42% of the 12 sentences. An example of a sentence considering cultural equivalence is sentence number 9: "See the dog? You are going to draw a line from the dog to this bone over here." During the committee-2 discussion, the members agreed that "from... to...", as it occurs in sentence number 9, is not a culturally appropriate manner of giving instructions in isiZulu. Instead, the members agreed that P-FTL should read: "Buka inja. Dweba ulayini uyaku [sic] kwithambo (Look at the dog. Draw a line to the bone)."
Another example of cultural equivalence occurred in sentences number 2, 7 and 9, where committee-2 chose "dweba" (draw) instead of "uzodweba" (you will draw) to remain faithful to the culturally familiar way of giving instructions. In four sentences (3, 18, 30 and 32), committee-2 concluded that appropriate pointing to the target picture is vital for ensuring cultural equivalence. The necessity for pointing is also due to the way instructions are given in isiZulu, which differs from English.
Functional equivalence was the focus of 17% of the discussion surrounding the 12 sentences with discrepancies. An example of this occurred in sentence 44: "...there may be more than one shape like the one at the top." Decentring was necessary to ensure that the instructions elicit the same response from the child. The PI-TL was not clear that the child had to look for more than one answer. However, committee-2's P-FTL version ensured the child would understand to look for multiple responses. Similar confusion was revealed in sentence 18: "The car can go around the racetrack in either direction." Initially, this sentence was mistranslated as "imoto ingahamba noma yikuphi. (The car can go anywhere)", which the child could misinterpret as drawing anywhere on the page instead of within the targeted stimulus. After much deliberation, committee-2 improved on the functional equivalence to ensure that the desired response (drawing a line within the targeted stimulus) would be elicited.
Conceptual equivalence was the focus of discussion in 50% of these sentences. In the P-FTL, conceptual equivalence was obtained through words such as "ulayini" (used in sentences 2, 3, 7, 9, 10, 13, 14, 17 and 19) instead of "umugqa". Umugqa is the proper isiZulu word for "line"; however, it was decided that it may not be equally familiar to young children. Similarly, the word "ipeni" (sentences 4, 6, 8, 15 and 19) was chosen for pencil since it was considered by committee-2 to be more familiar to a young child than the proper isiZulu word for ''pencil". Conceptual equivalence proved challenging in sentences number 30 and 32, which read "...which of these shapes down here are part of the drawing at the top of the page.' The isiZulu word for "part of "or "ingxenye" ("part") was considered by the committee-2 members as unlikely to be in a young child's vocabulary. In sentences number 30 and 32, the committee agreed that with appropriate pointing by the administering therapist, ingxenye should be omitted. Similarly, sentence 43 also includes "...they may be part of a drawing ", which presented the same challenge. However, in this case, decentring was required to maintain equivalence. Committee-2 agreed that "inhlangane neminye imidwebo" ("combined with other drawings") would be the most suitable alternative in this case.
To ensure rigour, an external rater corroborated the equivalence analysis. Out of the 12 sentences with discrepancies, a random selection of 42% was designated for verification. The randomised sentence numbers and the committee-2 meeting recording were provided to the external rater for blind verification. The results of the external rater report confirmed that the equivalences observed during the analysis were present points of discussion during the committee-2 discourse.
Stage V
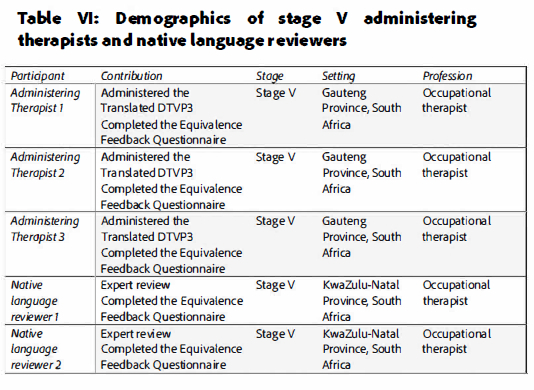
The sample of participants in stage V consisted of administering therapists (n=3), native language reviewers (n=2) and isiZulu-speaking children (n=10). All the administering therapists involved in the stage V pre-test were trained occupational therapists and fluent speakers of isiZulu. Similarly, both native language reviewers who contributed to stage V were native isiZulu speakers and trained occupational therapists. Refer to Table VI (below) for the contributions, settings and professions of the administering therapists (n=3) and native language reviewers (n=2).
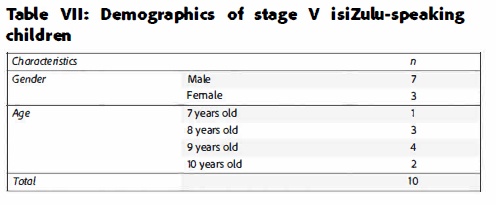
The sample of isiZulu-speaking children (n=10) who participated in stage V ranged from seven years two months old to ten years seven months old. All the children were located in Gauteng Province, South Africa. Nine of the ten children were attending mainstream schools and one was from a school for learners with special educational needs. Table VII (adjacent) shows the demographic representation of the isiZulu-speaking children. Assent was obtained from each child before the assessment was administered. The administering therapists then administered the DTVP-3 to the isiZulu-speaking children (n=10) using the isiZulu instructions. Following the assessment, the children verbally responded to the Child Feedback Questionnaire. The Child Feedback Questionnaire was developed for this study and consisted of three dichotomous questions relating to the children's experience of the isiZulu administration instructions. The average responses for the three questions were 9.3 out of 10 positive responses. Therefore, the majority of the responses from the isiZulu-speaking children indicated that they could understand the isiZulu administration instructions.
After administering the DTVP-3, the therapists (n=3) completed the equivalence feedback questionnaire. This questionnaire was also completed by native language reviewers (n=2), who had read through the isiZulu administration instructions. Responses to 80% of the questionnaire items indicated unanimous agreement that the translation was successfully translated and cross-culturally adapted while maintaining functional, cultural and conceptual equivalence. Responses to questionnaire items consisted of either minor rewording suggestions or variations that had already been discussed during the committee stages. Overall, all five occupational therapists (administering therapists and native language reviewers) indicated that the DTVP-3 was successfully translated and cross-culturally adapted. One of the questionnaire item responses recommended an addition that does not occur in the SL but would improve upon the practicality of administering the instrument. The suggestion was to add the phrase "Ngikombise [sic] futhi (Show me again)." Also, in response to a question regarding metaphors, idioms and colloquialisms, one participant suggested alternate wording for the visual closure subtest instructions. The suggestion is a simplified paraphrasing of the SL instructions and therefore employs a great degree of decentring. The P-FTL more accurately mirrors the SL version, but the suggested simpler version represents a more culturally appropriate manner of speaking. This suggestion should be considered when the translation is prepared for a pilot study (not included in the scope of this research).
One native language reviewer suggested a significant alteration to how subtest five is presented to the child. This recommendation was noted but not incorporated into the P-FTL since it significantly deviated in structure and length from the SL version. In the researcher's clinical opinion, this could compromise the psychometric properties of the subtest. In the comments section of the questionnaire, four of the five occupational therapists commented that the SL and P-FTL are equivalent. Native language reviewer 1 described the translated version as concise and easy to administer. She also version as concise and easy to administer. She also emphasized that even in cases where no direct translation was possible, the meaning remained the same. Administering therapist 1 described the P-FTL version as being "perfect".
DISCUSSION/IMPLICATIONS OF RESEARCH
This study demonstrated a rigorous method for translating and cross-culturally adapting an assessment instrument such as the DTVP-3 to advance the authenticity of the assessment within the South African context. To the researcher's knowledge, this is the first time this method has been applied to test administration instructions in a South African setting. The main finding of this study is that the methodology produced the pre-final isiZulu administration instructions that were revealed to be functionally, culturally and conceptually equivalent to the original version of the OTVP-3. Ther strength of the methodology is that it consisted of five stages, and included two communities with various contributors from diverse backgrounds and professions. Various successes and challenges were experienced throughout the study, providing a road map for future researchers. This study discusses these successes and challenges.
As integrated into the methodology, the committee approach proved vital to the cross-cultural adaptation of the DTVP-3 into isiZulu. From the beginning of the study, emphasis was placed on translation with the target audience in mind. Simple, developmentally appropriate language was prioritized over pure vocabulary and formal grammar. As a result, conceptual equivalence was the predominant consideration in the discourse of both committee-1 and committee-2. This emphasis on age-appropriate language was also confirmed by the responses of the two administering therapists and two native isiZulu-speaking occupational therapists. All four therapists judged the P-FTL as similar in meaning, difficulty, commonality, structure, length, familiarity and complexity (according to their responses on the Equivalence Feedback Questionnaire) and therefore equivalent. Another advantage of the translation methodology used for this study is the addition of the third translator (TL3 translator) in the stage I forward translation. This translator had experience teaching children languages, which contributed much value to the translation and the committee-1 discourse.
Various practical considerations worked well during the stage I to IV committees. Google Translate, and the researcher's basic familiarity with elementary isiZulu, were used to prepare the comparison of SL, TL1, TL2 and TL3 by numbering the corresponding sentences. This numbering was done to ease the comparison of translated versions and facilitate verbal referencing of specific sentences during the committee discussions. Stages I to IV committee meetings were conducted virtually on a well-known virtual meeting platform. Conducting the meeting on-line broadened the geographical reach of the study so that participants from other provinces could be included and also allowed for more scheduling flexibility.
It proved to be very important that all the committee members be familiar with the administration procedure of the DTVP-3 in order to apply the translation to the context. The translators were initially provided with examples of the subtests, but some confusion remained regarding whether the children would have to read the instructions themselves. It was explained that the instructions would be given verbally by a therapist trained in the DTVP-3. This understanding of the context and administration procedure influenced both committees' discourse, especially committee-1.
South Africa's eleven official languages often blend where cultures harmonize together. As a result, many isiZulu dialects have developed. Although the translation proved to be equivalent, the differences in the dialects were apparent during both committees and the feedback received from the therapists involved during stage V. Some dialect differences, such as the use of "ingxenye" (part), ended up being discussed repeatedly.
One aspect that also contributed much value to the translation was the inclusion of multiple occupational therapists in stages I to IV. During the stage I forward translation, the occupational therapist who produced TL1 was able to draw on his training and experience with the DTVP-3 to benefit the translation. As a result, TL1 was concise and accepted as the equivalent version for almost half (n=22) of the sentences chosen by committee-1. For the stage IV committee-2 discussion, the independent third party was also a trained occupational therapist. During the committee-2 collaboration, both occupational therapists contributed their experience and assisted in making the translation more applicable to real-life administration, thereby enhancing its equivalence. In the context of this translation, the inclusion of an additional occupational therapist may have added more value to committee-2 than the monolingual third party suggested by some previous studies20.
Through the rigorous method used to translate and cross-cultural adapt the DTVP-3, this study also enhanced its authenticity as an assessment instrument within the context of South Africa. It can be said that the newly translated isiZulu instructions have improved the DTVP-3's social appropriateness within this context. Social appropriateness is a quality indicator of authentic assessment. It can be expected that both professionals and parents would find the DTVP-3 a more socially appropriate assessment instrument for isiZulu-speaking school-going children when presented in their native language. Another indicator of authentic assessment procedures is an equitable design enabling equal opportunity to demonstrate skills. Having the administration instructions of the DTVP-3 available to isiZulu-speaking children in their native language provides equal opportunity to children who may not be as proficient in English as in isiZulu. The DTVP-3's utility is founded on its capacity to inform intervention goals and facilitate performance monitoring when treating isiZulu-speaking children with visual perceptual and visual-motor integration difficulties seeking therapeutic intervention. Therefore, its utility as an indicator of authentic assessment can now be considered more appropriate.
The methodology followed during this study was not dependent on the researcher's fluency in the target language. The implication is that an assessment instrument's translation and cross-cultural adaptation can be carried out without being limited by a researcher's language skills. This methodology has already incorporated various mechanisms to ensure that it transcends the language skills of any one participant.
Limitations of the study
Although this qualitatively driven multimethod sequential study presented a thorough and rigorous methodology, it is merely preliminary. Some limitations must be considered. The researcher acknowledges that this study included a limited, non-representative sample of administering therapists (n=3) and children (n=10). This study intended to progress only to the pre-test stage. Therefore, a pilot study was not included in the scope of this research. Should this study have included a larger sample of administering therapists and children or have progressed to a pilot study, other threats to equivalence might have been revealed. Another limitation of this study is the limited inclusion of participants from the provinces of Gauteng, Free State, Mpumalanga and KwaZulu-Natal. The populations of the Northern Cape, Western Cape, Limpopo, North-West and Eastern Cape provinces were not represented.
The isiZulu administration instructions are currently limited to use by therapists fluent in isiZulu. This is another motivation for further research applying the methodology to more assessment instruments in more languages.
Future studies should consider including the original developer/publisher of the assessment instrument in the committee discussions. If the developer could be a contributor to the committee-2 review, the feedback could inform an adaptation of the English version for the South African context.
CONCLUSION
This study describes a rigorous methodology for translating and cross-culturally adapting the administration instructions of an assessment instrument, such as the DTVP-3, into isiZulu to advance the authenticity of the assessment within the South African context. The methodology progressed through five stages: 1) forward translation, 2) synthesis and agreement by committee one, 3) blind back-translation, 4) synthesis and agreement by committee two and 5) pre-testing. The methodology was shown to successfully ensure the functional, cultural and conceptual equivalence of the isiZulu version. The difficulties and successes experienced throughout the process are also reported. This research is intended to be a framework upon which the cross-cultural adaptations of other assessment instruments and other languages in South Africa can be based.
Author contributions
All listed authors contributed to the study design, data analysis, references and final review. Sumarie Naude was responsible for the data procurement and writing of the first draft. All authors contributed to and agreed with the of the final, revised manuscript.
Acknowledgements
The authors wish to acknowledge the participants who contributed their time and knowledge to this research. Particularly, the occupational therapists and other professionals who applied their clinical experience and cultural knowledge and without whom this research would not have been possible.
Conflicts of interest
The authors have no conflicts of interest to declare.
REFERENCES
1. Schneck CM. Visual perception. In: Case-Smith J, O'Brien JC, editors. Occupational therapy for children. 6th ed. Missouri: Mosby/Elsevier; 2010. p. 373-403. [ Links ]
2. Schneck CM. Best practices in visual perception and visual-motor skills to enhance participation. In: Clark GF, Fioux JE, Chandler BE, Cashman J, editors. Best practices for occupational therapy in schools. 2nd ed. Bethesda: AOTA Press; 2019. p. 489-96. [ Links ]
3. American Occupational Therapy Association. Occupational therapy practice framework: Domain and process 3rd ed. Am J Occup Ther. 2014;68(Suppl 1):S1-S48. https://doi.org/10.5014/ajot.2014.682006 [ Links ]
4. National Early Literacy Panel, National Institute for Literacy, National Center for Family Literacy. Developing early literacy: Report of the national early literacy panel: A scientific synthesis of early literacy development and implications for intervention. Washington, DC: National Institute for Literacy; 2008. https://doi.org/10.1037/e563852009-001 [ Links ]
5. Glass P. Development of the visual system and implications for early intervention. Infants Young Child. 2002;15(1):1-10. https://doi.org/10.1097/00001163-200207000-00003 [ Links ]
6. Bazyk S, Case-Smith J. School-based occupational therapy. In: Case-Smith J, O'Brien JC, editors. Occupational therapy for children. 6th ed. Maryland Heights: Mosby/Elsevier; 2010. p. 713-43. [ Links ]
7. de Sam Lazaro SL. The importance of authentic assessments in eligibility determination for infants and toddlers. J Early Interv. 2017;39(2):88-105. https://doi.org/10.1177/1053815116689061 [ Links ]
8. Bagnato SJ, Neisworth JT, Pretti-Frontczak K. Linking authentic assessment and early childhood intervention: Best measures for best practices. 2nd ed. Baltimore: Paul H. Brookes Publishing; 2010. [ Links ]
9. Bagnato SJ. Authentic assessment for early childhood intervention: Best practices. New York: The Guilford Press; 2007. [ Links ]
10. Bagnato SJ. The authentic alternative for assessment in early intervention: An emerging evidence-based practice. J Early Interv. 2005;28(1):17-22. [ Links ]
11. Neisworth JT, Bagnato SJ. The mismeasure of young children: The authentic assessment alternative. Infants Young Child. 2004;17(3):198-212. https://doi.org/10.1097/00001163-200407000-00002 [ Links ]
12. Hammill DD, Pearson NA, Voress JK. Developmental test of visual perception examiner's manual. 3rd ed. Austin: Pro-Ed; 2014. [ Links ]
13. Grisham-Brown J, Hallam R, Brookshire R. Using authentic assessment to evidence children's progress toward early learning standards. Early Child EducJ. 2006;34(1):45-51. https://doi.org/10.1007/s10643-006-0106-y [ Links ]
14. Visser M, Nel M. Visual perception of five-year-old Afrikaans-speaking children in Bloemfontein using the Beery VMI-6, DTVP-3 and TVPS-3: A follow up study of their English-speaking counterparts in Bloemfontein. S Afr J Occup Ther. 2018;48(2):31-43. http://dx.doi.org/10.17159/2310-3833/2017/vol48n3a6 [ Links ]
15. Census 2022 statistical release. Pretoria, South Africa: Statistics South Africa. 10 October 2023. Available from: https://census.stat.ssa.gov.za/assets/documents/2022/P03014_Census_2022_Statistical_Release.pdf (accessed 15 October 2023) [ Links ]
16. Smith M, Visser MM, van Heerden R, Raubenheimer J. Considerations when assessing urban south African children with the developmental test of visual perception 2nd edition (DTVP-2). South AfricanJournal of Occupational Therapy. 2018;48(1):51-9. https://doi.org/10.17159/2310-3833/2017/vol48n1a9 [ Links ]
17. Beaven T, Comas-Quinn A, Hauck M, de los Arcos B, Lewis T. The open translation MOOC: Creating online communities to transcend linguistic barriers. J Interact Media Educ. 2013;18. https://doi.org/10.5334/2013-18 [ Links ]
18. Guo J-W. Is google translate adequate for facilitating instrument translation from English to mandarin? Comput Inform Nurs. 2016;34(9):377-83. https://doi.org/10.1097/cin.0000000000000287 [ Links ]
19. Jones EW, Hoerger M, Hughes JC, Williams BM, Jones B, Moseley Y, et al. ABA and diverse cultural and linguistic environments: A welsh perspective.J Behav Educ. 2011;20:297-305. https://doi.org/10.1007/s10864-011-9138-5 [ Links ]
20.Sousa VD, Rojjanasrirat W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline.J Eval Clin Pract. 2011;17(2):268-74. https://doi.org/10.1111/j.1365-2753.2010.01434.x [ Links ]
21.Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine (Phila Pa 1976). 2000;25(24):3186-91. https://doi.org/10.1097/00007632-200012150-00014 [ Links ]
22.Peña ED. Lost in translation: Methodological considerations in cross-cultural research. Child Dev. 2007;78(4):1255-64. https://doi.org/10.1111/j.1467-8624.2007.01064.x [ Links ]
23. Smit J, van den Berg CE, Bekker L-G, Seedat S, Stein DJ. Translation and cross-cultural adaptation of a mental health battery in an African setting. Afr Health Sci. 2006;6(4):215-22. [ Links ]
24. Guillemin F, Bombardier C, Beaton D. Cross-cultural adaptation of health-related quality of life measures: Literature review and proposed guidelines. J Clin Epidemiol. 1993;46(12):1417-32. https://doi.org/10.1016/0895-4356(93)90142-N [ Links ]
25. Gjersing L, Caplehorn JR, Clausen T. Cross-cultural adaptation of research instruments: Language, setting, time and statistical considerations. BMC Med Res Methodol. 2010;10(13):1471-2288. https://doi.org/10.1186/1471-2288-10-13 [ Links ]
26. Behling O, Law KS. Characteristics of useful measures. Thousand Oaks: Sage Publications Inc.; 2011. https://dx.doi.org/10.4135/9781412986373 [ Links ]
27. GuoJ-W, Chiang H-Y, Beck SL. Cross-cultural translation of the Chinese version of pain care quality surveys (C-PainCQ). Asian Pac Isl NursJ. 2020;4(4):165-72. https://doi.org/10.31372/20190404.1072 [ Links ]
28. Wang VC, Mayer F, Ottawa F, Wippert P-M. Translation reliability and test-retest reliability for elite athlete's injury risk factor questionnaire. Sports Exerc Res. 2015;17(2)231-41. https://doi.org/10.5297/ser.1702.009 [ Links ]
29. Greenfield PM, Trumbull E, Keller H, Rothstein-Fisch C, Suzuki LK, Quiroz B. Cultural conceptions of learning and development. Handbook of educational psychology: Routledge; 2014. https://doi.org/10.4324/9780203874790.ch29 [ Links ]
30. Beck CT, Bernal H, Froman RD. Methods to document semantic equivalence of a translated scale. Res Nurs Health. 2003;26(1):64-73. https://doi.org/10.1002/nur.10066 [ Links ]
31. Hambleton RK, Zenisky AL. Translating and adapting tests for cross-cultural assessments. In: Matsumoto D, van de Vijver F, editors. Cross-cultural research methods. New York: Cambridge University Press; 2011. p. 47-74. https://doi.org/10.1017/cbo9780511779381.004 [ Links ]
32. International Test Commission [Internet]. The ITC guidelines for translating and adapting tests (second edition). International Test Commission; [updated 2020; cited 2022 May 3]. Available from: https://www.intestcom.org/page/14. [ Links ]
33. Denti L, Marcomini B, Riva S, Schults PJ, Caminiti C. Cross-cultural adaptation of the stroke action test for Italian-speaking people. BMC Neurol. 2015;15(76):1-7. https://doi.org/10.1186/s12883-015-0335-z [ Links ]
34. Franco AR, Vieira RM, Riegel F, Crossetti MdGO. Steering clear from 'lost in translation': Cross-cultural translation, adaptation, and validation of critical thinking mindset self-rating form to university students. Studies in Higher Education. 2021;46(3):638-48. https://doi.org/10.1080/03075079.2019.1647414 [ Links ]
35. Oliva-Fanlo B, March S, Stolper E, Esteva M. Cross-cultural translation and validation of the 'gut feelings' questionnaire into Spanish and catalan. The European journal of general practice. 2019;25(1):39-43. https://doi.org/10.1080/13814788.2018.1514385 [ Links ]
36. Marinho Cezar da Cruz D, Parkinson S, da Silva Rodrigues D, Couto de Melo Carrijo D, Denubila CostaJ, Fachin-Martins E, et al. Cross-cultural adaptation, face validity and reliabilityof the model of human occupation screening tool to Brazilian Portuguese. 2019;27(4):691-702. https://doi.org/10.4322/2526-8910.ctoAO2007 [ Links ]
37. Hesse-Biber SN, Johnson RB. The Oxford handbook of multimethod and mixed methods research inquiry. Oxford, United States: Oxford University Press; 2015. https://doi.org/10.1093/oxfordhb/9780199933624.001.0001 [ Links ]
38. Pasin S, Avila F, de Cavatá T, Hunt A, Heldt E. Cross-cultural translation and adaptation to Brazilian Portuguese of the Paediatric Pain Profile in children with severe cerebral palsy. J Pain Symptom Manage. 2013;45(1):120-8. https://doi.org/10.1016/j.jpainsymman.2012.01.013 [ Links ]
 Correspondence:
Correspondence:
Sumarié Naude
otsumarie@gmail.com
Submitted: 21 June 2022
Reviewed: 17 December 2022
Revised: 21 July 2023
Accepted: 25 July 2023
Editor: Blanche Pretorius: https://orcid.org/0000-0002-3543-0743
Data availability: From The Corresponding Author
Funding: The Authors Have Received No Funding For This Research.

