










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versión On-line ISSN 2310-3833
versión impresa ISSN 0038-2337
S. Afr. j. occup. ther. vol.53 no.3 Pretoria dic. 2023
http://dx.doi.org/10.17159/2310-3833/2023/vol53n3a5
MAPPING REVIEW
Wrestling with evidence-based practice: An evidence mapping review of publication trends in the South African Journal of Occupational Therapy
Fatima HendricksI, II; Helen BuchananI, III; Asia R ClarkI, IV
IDuring the study: Department of Occupational Therapy, School of Health Sciences, Chicago State University. United States of America; https://orcid.org/0000-0002-0080-7598
IICurrent: PhD student, Department of Sociology, lbn Haldun University, Turkey
IIIDivision of Occupational Therapy, Department of Health and Rehabilitation Sciences, University of Cape Town. South Africa; https://orcid.org/0000-0001-5540-9928
IVCurrent: OTD Student, Department of Occupational Therapy, School of Health and Human Sciences, Indiana University-Purdue University Indianapolis. United States of America; https://orcid.org/0000-0003-4319-926X
ABSTRACT
INTRODUCTION: Occupational therapy research to support clinical decision-making must be responsive to local needs, illustrate our unique value to clients, communities and providers, and demonstrate efficacy for quality assurance and reimbursement. This article examines the publication trends in the South African Journal of Occupational Therapy (SAJOT) with the intention of contributing to dialogues about evidence-based practice.
METHODS: A mapping review was undertaken of articles published in the SAJOT from January 2009 to December 2021. All articles excepting commentaries, book reviews and editorials were included. Articles were categorised by year of publication, title, author, research approach, study design, practice area, research affiliation, and nature of authorship. Quantitative research articles were classified according to the Australian National Health and Medical Research Council (NHMRC) levels of evidence.
RESULTS: Of the 265 articles published in the 13-year period, slightly more took a quantitative approach (52.1%) compared with qualitative approaches (42.4%). Most quantitative studies were Level III-2 studies (31.3%). Children and Youth was the practice area with the highest number of articles (34.8%) and the strongest evidence base.
CONCLUSION: As occupational therapy continues to wrestle with EBP, further dialogue about a national occupational therapy research strategy to identify and harness enablers and explore and mitigate the barriers identified in this review, is recommended.
IMPLICATIONS FOR PRACTICE
• This research serves as a bridge between theoretical findings and practical applications, by providing data from research that can be put into action through the development of research agendas by institutions.
• By understanding what research has been done, professionals can make informed decisions that are backed by evidence-based findings. This not only enhances the quality of their work but also improves overall efficiency and effectiveness.
• The study helps practitioners identify areas where improvements or interventions are needed. They shed light on potential challenges and offer possible solutions that can be implemented to address specific issues or concerns within their respective fields.
• This data provides a platform for collaboration between researchers and practitioners across institutions in terms of common research agendas.
Keywords: evidence-informed practice, levels of evidence, research gaps, national research strategy, children and youth
INTRODUCTION
The advent of evidence-based practice (EBP) precipitated a period during which the occupational therapy profession sought to expand the dominant paradigm of therapy based on expert opinion and practice experience, with practices supported by research evidence1. Reasons for adopting an evidence-based approach in occupational therapy have included blending theory and practice2, demonstrating the benefits and effectiveness of occupational therapy2-6, efficient services7, the survival of the profession6,8 and 'filling in knowledge gaps'6. Literature outside the occupational therapy profession has critiqued EBP for its:
• rooting in a scientocentric model9
• epistemological challenges and what is considered as knowledge within the hierarchy of evidence10
• restrictive nature (considering that decision-making requires more inclusive forms of evidence)11
• embedding of research evidence in power and racial injustice12
• role in widening disparities between evidence-based strategies and community resources for knowledge translation (thus exacerbating inequities)13
• exclusion of indigenous healing practices and failure to acknowledge disparate research funding to indigenous communities14,15 and,
• lack of engagement with what constitutes evidence16.
Whilst sharing these common issues, occupational therapy literature raises its own concerns. Firstly, systematic reviews carry the potential of individualised bias and inclusion criteria errors17. Secondly, several barriers have stunted the adoption of EBP, including lack of time, lack of availability and accessibility of research, and limited research skills18. Thirdly, historical, professional and institutional constraints exacerbate the theory-practice gap19. Fourthly, limited involvement in research20, and lastly, ongoing conceptual and practical challenges despite substantial international educational efforts21. A recent systematic review examining the international position statements on the use of EBP in occupational therapy from five Westernised countries highlighted similar concerns22. Factors limiting the uptake of EBP included "limiting occupation focus, lack of studies, lack of time, low quality/relevant research, negative attitudes, and lack of training, skills, and motivation"22 e10. Notably, the Canadian statement raises concern that the strict adherence to EBP limits the focus on occupation for therapists committed to enabling occupation using a client-centred, occupation focused approach23.
Hence, whilst health care professionals in general, and occupational therapists specifically, have wrestled with EBP, there have been suggestions to move towards the evolving concept of evidence informed practice (EIP)24-26. EIP is defined as the holistic integration of research evidence, practitioner expertise and the people experiencing the practice, with equal consideration of all three components (without preferencing evidence)26'27. Although EBP has been similarly defined, evidence has dominated the other two considerations of practitioner expertise and clients. Whilst recognising the emergence of EIP as an area of theoretical and conceptual growth in seeking to address the limitations of EBP, the term EBP is still largely used in occupational therapy literature. This article thus uses the term EBP rather than EIP,
A shift towards evidence that is more strongly grounded in research requires substantial re-orientation not only in the practice of occupational therapy but also in education and research28. Based on Kuhn's29 four stages in the development of a profession - pre-paradigm, dominant paradigm, period of crisis and a period of accepting a new paradigm - the profession has to navigate a period of crisis in moving from the previous dominant paradigm (expert-based practice) into the new paradigm of EBP. To explore how far we have come in transitioning to this new paradigm in South Africa, we undertook a mapping review to examine publication trends in the South African Journal of Occupational Therapy (SA JOT) over the past thirteen years (2009-2021) with the intention of evaluating our progress towards developing the evidence-base required to support occupational therapy practice in South Africa. We had three objectives: (1) to summarise the recent publication trends in SAJOT over the last thirteen years; (2) to analyse the research generated during this period by research approach and evidence level; and (3) to identify current research gaps,
LITERATURE REVIEW
Fleming-Castaldy and Gillen28 368 state that "the integration of science into a profession requires introspection, confrontation, and discourse."
Introspection leads us to think about the importance of research activity broadly. More specifically, introspection requires us to observe and examine our thoughts and feelings about EBP in relation to the values of the occupational therapy profession and its ethical foundations, and the profession's responsiveness and relevance in meeting mounting people and planet pressures.
EBP originated as evidence-based medicine (EBM) as early as 1991 but became popularised through Sackett who defined it as "the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients"2 71. EBP very quickly became adopted by other health professions including occupational therapy. The initial definition has evolved to encapsulate the process of weighing up the evidence (usually considered to be research evidence) together with professional knowledge and experience and client values, preferences and circumstances within a specific context in order to make the best possible decision about health care for a client30. This definition leads us to reconsider what is meant by 'evidence' through an epistemological lens on knowledge37 and truth32.
Central to this debate is the origin of EBP in medicine and its evolvement from EBM to EBP, with the former having a firm grounding in positivism which "assumes that phenomena are measurable using the deductive principles of the scientific method"33,129. In this context, evidence has traditionally been viewed as quantitative research, organised into a hierarchy according to the degree of bias inherent in their designs34. The roots of EBP are thus strongly embedded in logical empiricism which forms the foundation of experimental research34 and values factual and objective information32. Juxtaposed with this is the alternative position of diversity in ways of knowing31,32.
Although rooted in different philosophies these forms of naturalistic inquiry view knowledge as being founded on perceptions of experiences and understandings of the world which cannot be separated from the outside world35. Hence, the concept of providing care operates within a particular worldview that determines the type of evidence required and influences thinking about what is considered 'high-quality' evidence. Occupational therapy's unique focus on achieving health and participation through engagement in occupations36 encompasses a broad interpretation of health that departs from a biomedically-oriented approach to one concerned with participation and social justice37 Occupational therapy thus spans positivistic and naturalistic ways of knowing which requires diverse research designs38 which necessitates quantitative and quantitative approaches to knowledge generartion.
Confrontation, the second aspect of integrating science into the profession, necessitates active engagement with the established knowledge base underpinning practice. Hinojosa raised three concerns related to EBP in occupational therapy17, viz. (a) Should occupational therapy adopt a hierarchy of evidence from medicine? (b) What are the consequences of assuming that randomised controlled trials provide the best, if not the only, evidence that establishes credibility? (c) Is internal validity more important than external validity when judging the value of a research study? An important consideration is the confrontation on how much of what is taught and researched in South Africa, is produced in South Africa, as part of broader occupational consciousness39 dialogues about occupational therapy hegemony and context, the manifestations of which are described in the critiques of EBP at the outset of this paper. Furthermore, the EBP assumption that health care decisions are made at an individual level by the therapist with input from the client, may not be appropriate in an African society where the Ubuntu philosophy encompasses a culture of collectivism with decisions being made for the well-being of the family, community and individual40,41 .
Another confrontation calls for an examination of the tensions arising from a "disconnect between our commitment to currency and efficacy, and the press to include outdated and unsubstantiated information" in textbooks, and practices that are outdated yet still in use28 364 A practical example of such a confrontation relates to evidence presented in a systematic review which challenges the continued use of traditional approaches, such as Bobath in promoting sensori-motor control of limbs, activities of daily living and quality of life42. However, it is for precisely these reasons that EBP requires active dialogue.
The third aspect, discourse, requires interchange of ideas, knowledge and experience of the application of the new paradigm of EBP. An example is the relationship between evidence and ethics. Chabon43 advocates that our use of EBP in conjunction with our Code of Ethics elevates us as professionals and encourages public trust in the profession . The standing of EBP is evident in the World Federation of Occupational Therapists (WFOT) Code of Ethics441 which states that "Occupational therapists will .... apply their acquired knowledge and skills in their professional work, based on the best available evidence."
"Notably, the term evidence-based practice is absent from the Occupational Therapy Association of South Africa (OTASA) Code of Ethics45 (currently under revision) and the Ethical and Professional Rules of the Health Professions Council of South Africa (HPCSA)46 although inferences are present in both as reflected in these statements:
"Occupational therapy personnel shall achieve and continuously maintain high standards of competence and be aware of current trends and legal issues or developments affecting their practice"45 3."A practitioner shall at all times keep his or her professional knowledge and skills up to date"46.20.
Discourse thus requires assertive educators that model reflection and critical dialogue on how to move forward beyond comfort zones of practice based on tradition43. Beyond educators, it also demands that clinicians actively engage their clients in ensuring their values and preferences are considered, their safety is promoted, and that they participate actively in decision-making and exercise their healthcare choices7,8,28. Locally, Hinojosa's17 reflections recede against the broader social and historical impacts of apartheid on health in the context of South Africa.
Through the framework of introspection, confrontation, and discourse there is a need to bring the considerations of power, race, gender, and class and other dimensions into the conscious dialogues about EBP, in terms of inequality in the production and reproduction of knowledge and social relations in occupational therapy. However, current dialogues in occupational therapy and EBP do not sufficiently foreground the fundamental question about the epistemological underpinnings about what knowledge is, how it is produced and by whom, which this mapping review can provide glimpses into. Hence, can a discussion on progress towards becoming an evidence-based profession in South Africa be authentic without addressing issues of decoloniality and epistemology as root constructs, perhaps described in Kuhn's29 words as an unresolved failure? Do we continue an evaluation into the growth of EBP in South Africa despite the 'unresolved failure' of sufficient robust epistemological engagements or do we proceed to evaluate our progress towards the implementation of EBP within practice, education, and research? Aware of these unresolved issues, we proceed to examine EBP specifically to establish what scholarly articles were published in the SAJOT, with a clear intent of contributing to discussions and debates about EBP. As the official journal of the OTASA, the SAJOT predominantly publishes research and academic articles produced by South African occupational therapists. It therefore provides an ideal forum for monitoring paradigm shifts within the profession.
METHODS
A mapping review was conducted to plot publication trends in the SAJOT. Mapping provides a systematic approach to understanding the 'map' of a profession, theory, research question, or practice and is useful for identifying trends on a particular topic47.
A mapping review focuses on "categorising, classifying, characterising patterns, trends or themes in evidence production or publication"48,14. The objectives of the review were to: (1) summarise the publication trends in the SAJOT over a 13-year period; (2) analyse the research during this period according to evidence level; and (3) identify research gaps. Ethical clearance was not obtained as this is not a requirement for a mapping review.
The search strategy was conducted manually from the SAJOT website and double checked on Scielo.org.za which holds an online repository of SAJOT issues. All articles published in the SAJOT from January 2009 (volume 39, issue 1) to December 2021 inclusive (volume 51, issue 3) were retrieved and screened for eligibility. All researched articles were included but commentaries, book reviews and editorials were excluded. As the journal only became digitised in late 2010 (volume 40, issue 3), the authors hand-searched articles published prior to this date. The journal website content search function was used to identify potentially relevant articles from volume 40 issue 3 (2010) to volume 51, issue 3 (2021).
The full-text articles were read to extract the following data from each included article: a) year of publication; b) research approach; c) research design; d) practice area; e) author affiliation; and, f) presence of interdisciplinary authorship. The research approach was classified as quantitative, qualitative or mixed methods, and the research design was captured as it was reported, for example 'cross-sectional', 'quasi-experimental', 'descriptive', 'analytical'. Articles that did not describe the study design were labelled as 'not reported' and those based on literature reviews were labelled 'not applicable'. To analyse publications on contribution to EBP (objective 2), articles reporting quantitative research designs were classified according to the hierarchy of evidence described by the Australian National Health and Medical Research Council (NHMRC)49.
The NHMRC hierarchy was developed in response to the bias towards intervention studies in existing evidence hierarchies49. This hierarchy appreciates that responses to the different types of clinical questions, such as those related to intervention, assessment, prognosis, and aetiology, require different research designs, and thus different evidence hierarchies. In doing so, the importance of the appropriate research design to answer the specific research question is elevated. Hence, our decision to select it as the tool to categorise evidence levels to examine the trajectory of locally produced research.
The NHMRC hierarchy indicates the best study design for the particular question. It is organised according to EBP question type (intervention, diagnosis, prognosis, aetiology and screening intervention), and categorises articles as: Level I (systematic review of level II studies), Level II (randomized controlled trials), Level III-1 (pseudorandomised controlled trials including other experimental or prospective observational studies), Level III-2 (comparative studies with concurrent controls), Level III-3 (retrospective studies) and Level IV (case reports, position statements, etc). Level IV was broadened to include opinion papers and non-systematic literature reviews. Qualitative studies and mixed methods studies were noted as such and were not assigned to a research hierarchy.
We used the OTASA fields of practice in use at the time of the study as a guide for categorising practice areas. Fields of practice were collapsed where necessary, for example adult neurology and adult physical were grouped together and renamed adult physical rehabilitation. Additional categories, such as occupational therapy education, and management and leadership, were created as the need arose. Naming of some field of practice categories were changed to align with terminology that was in use at the time of data collection.
All three co-authors coded the research approach, research design and level of evidence. Coding discrepancies were resolved through discussion to achieve consensus. Data were captured in a Microsoft Excel spreadsheet, codes assigned to all non-numerical data, and cleaned for analysis. Once the final data sets were assigned agreed-upon codes, the Microsoft Excel 'COUNTIFS' formula was used to calculate frequencies and percentages. Descriptive statistics were used to summarise the data and patterns across the years to identify trends (objective 1) and gaps (objective 3), and to describe the evidence by research approach and evidence level (objective 2).
RESULTS
In total, 265 articles met the inclusion criteria and were included in the analysis of publication trends in the SAJOT.
General publication trends
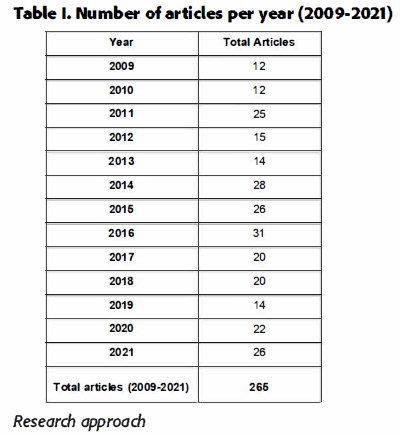
Number of articles per year
Table I (below) shows the number of research articles published in the SAJOT per year from 2009 to 2021 (n=265). The most active publication year (31 articles) was 2016 followed by 2014 (28 articles), 2015 and 2021 (26 articles each).
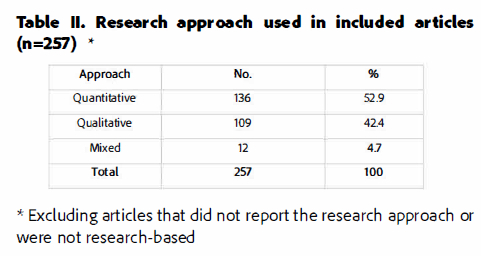
Research approach
Mixed method approaches were least used (n=12, 4.7%), whilst 52.9% of articles were quantitative (n=136) and 42.4% were qualitative (n=109) (Table II, page 40). Articles that did not report the research approach or were not research-based were excluded from this analysis (n=8; 3.0% of the total).
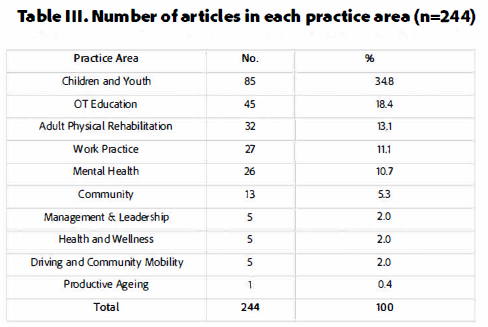
Practice Area
Table III (below) shows the number of articles published in each practice area in descending order. Articles that did not relate to practice, for example methodological, epistemological, and ethics articles (n=21; 7.9% of the total), were not included in the analysis. Children and Youth were highest (34.8%) whilst Productive Ageing was lowest (0.4%).
Research affiliation
Table IV (below) shows research affiliations for articles authored exclusively from one university (n=136). The University of the Witwatersrand was highest at 31.6%. Just over half (51.3%) of all articles were authored at single universities without co-author collaborations from other disciplines or other universities. Two articles (0.8% of the total sample) were authored by individuals in private practice and are not included in Table IV (below).
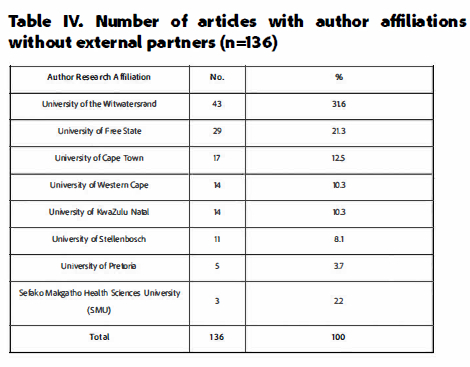
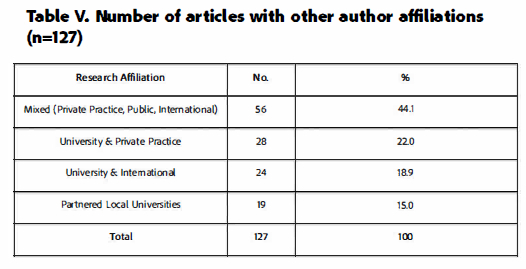
Table V (below) shows that 127 articles (47.9% of the total sample) had co-authors from multiple locations like local tertiary institutions with local universities, private practices, public institutions, international universities, and international organisations. Mixed co-authorship between private practice, public institutions and international settings was highest at 44.1% (n=56).
Interdisciplinary co-authorship
Compared to 168 (63.4%) articles with occupational therapy-only authorships, 85 articles (33.0%) had interdisciplinary co-authorship, such as occupational therapy with disciplines such as physiotherapy, biostatistics, and public health. Twelve articles (4.5%) were not authored by occupational therapists.
Evidence-based practice publication trends
This section addresses the second research objective on publication trends in the SAJOT over the last thirteen years (2009 to 2021) by summarising the research approach and study design (as reported in the articles). Figure 1 (below) shows the types of research designs found in the data set in the form of a word cloud. The higher the frequency of appearance, the larger the font size. Descriptive studies were most common followed by pretest-posttest studies.
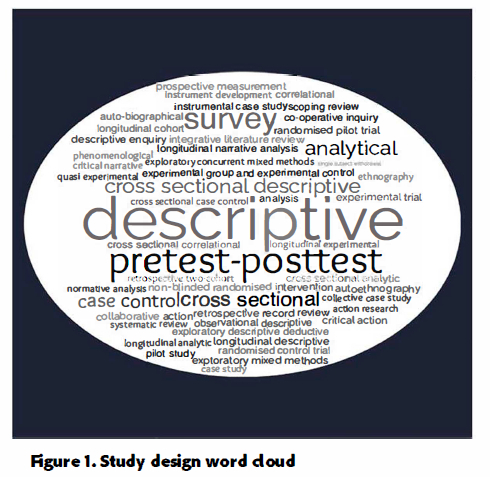
Table VI (below) presents the number of articles for each practice area according to research approach (quantitative, qualitative or mixed methods). Articles that were conceptual in nature and did not report research were categorised 'not applicable. The majority of studies were quantitative (n=136, 52.9%) but qualitative approaches were almost as high (n=109, 42.4%). Quantitative articles were further categorised by NHMRC evidence level49. Most quantitative articles were classified as level III-2 studies (n=83, 31.3%). Children and Youth was the practice area with the highest number of articles produced as well as the widest spread of evidence. The strongest level of evidence in this practice area was level I, but the level of evidence most prominently represented was level III-2 (n=36 articles).
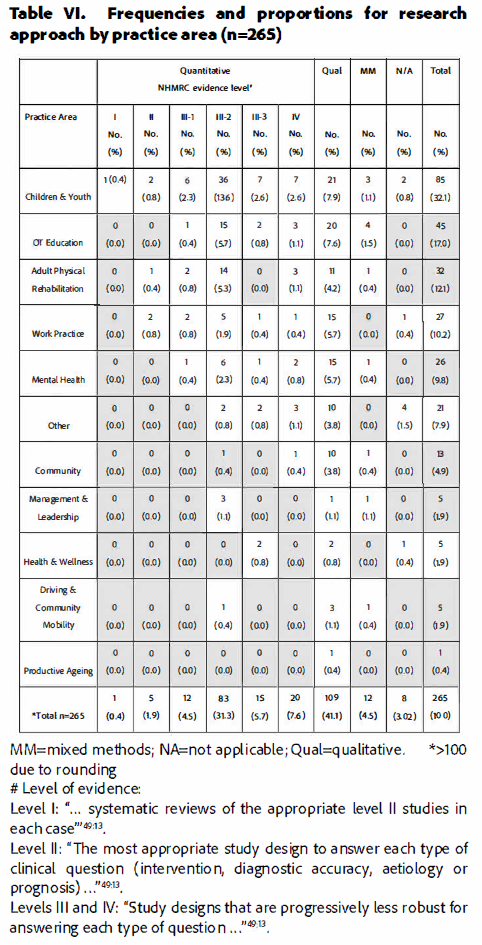
Gaps in the research
The distribution of research articles across practice areas is dominated by five main areas: Children and Youth, Occupational Therapy Education, Adult Physical Rehabilitation, Work Practice and Mental Health, and could be supportive of EBP. Table VI (adjacent) provides valuable insights into practice areas where research is noticeably lacking: management and leadership, health and wellness, driving and community mobility and productive ageing. Few studies reported level I (0.4%), II (1.9%) and (4.5%) designs.
DISCUSSION
This mapping review of research articles published in the SAJOT over a 13-year period examined the patterns in research output with the intention of contributing to dialogues about EBP. The inconsistency in the number of articles published in each issue may be due to several factors. Peaks in the data over the 13-year period could be due to professional conferences which may have encouraged more submissions. The OTASA hosted national conferences in 2012, 2014 and 2016 and co-hosted the World Federation of Occupational Therapists international congress in 2018 may have encouraged authors to work towards submitting articles in preparation for their presentations, resulting in the observed peaks in 2011,2014, and 2016. During the review period, university research programmes were under pressure due to interrupted schedules resulting from student movement protests such as the Rhodes Must Fall50 and Fees Must Fall51 movements, which may have impacted research output capacity due to shortened academic calendars. The COVID-19 public health crisis may have been a further reason for the decline in publications, as educators were under pressure to move to online modes of teaching which was extremely time-consuming and likely affected research productivity. However, the publication figures for 2020 and 2021 do not reflect this.
With regard to the research approach used, qualitative and quantitative approaches were reasonably on par with each other, but mixed methods approaches were less often utilised, possibly due to the resource demands of conducting such studies and the complexity of synthesising the findings. The relatively large number of articles with authors from multiple locations and co-authorship across disciplines and institutions could be used to leverage resources. Given the modest research output seen in the SAJOT, leveraging research partnerships through interdisciplinary and multi-partner collaborations could potentially increase the number of articles published in the SAJOT per year. An opportunity to increase research output could be to develop communities of practice between clinicians and academics similar to the collaborations between the University of the Western Cape and clinicians.
This mapping review shows the variety of study designs that were used over the 13-year period. The type of study design relates to the research question which raises questions about how decisions are made on which questions to investigate, in terms of push or pull demands, i.e. leading the field by asking new questions, or leading the field through responsive research. Guided by Fleming-Castaldy and Gillens28 suggestions of introspection, confrontation, and discourse, EBP requires that our understanding of occupation arises from, and is deeply connected to, what is observed in daily practice, integrating both push and pull demands in the research questions being asked. Of note were the relatively similar number of quantitative and qualitative studies that were published and the noticeable lack of level I and level II studies. This could indicate a predominance of student research, that academics are publishing higher level studies in other journals, or that this type of research is not being conducted. Soeker and Olumide52 similarly reported a paucity of level I studies in their content analysis of the OTASA research database. The gaps in level I and II research are a threat to the profession in terms of the evidence required by the National Department of Health (NDOH) for National Health lnsurance53. Collective action is thus needed to explore ways of producing the levels of evidence which the NDOH is calling for.
The current study identified a strong research focus on Children and Youth which had the highest number of articles and widest spread of evidence. Other relatively productive research areas were occupational therapy education, adult physical rehabilitation, work practice and mental health. An analysis of the OTASA research database of published and unpublished South African research produced from 2017 to 2019 similarly identified education and training and mental health as the most common research areas52. While this research production is encouraging, we need to explore how and where this research is being implemented. We also need to consider why research is low in some practice areas. Possible explanations for the limited spread of articles across some practice areas could be the low number of occupational therapists specialising in those fields, difficulty securing research funding and limited time and capacity to conduct research.
A viable recommendation towards building a more coherent and comprehensive body of evidence is the development of a national occupational therapy research strategy and agenda that focuses the research output of universities with national strategic priorities. To this end, the relatively recent launch of an OTASA database of South African occupational therapy research will enable mapping of the research that has been done, identifying gaps, and determining research priorities. This OTASA Research Committee initiative seeks to address the fragmentation and poor dissemination of South African occupational therapy research54. Du Toit55 advocated that to strengthen research dissemination and support the growth and recognition of the profession the OTASA should develop a research plan, in collaboration with universities, for producing and disseminating research that is relevant and appropriate for the South African practice context. Progress has been made in this regard through a recent survey of OTASA members which identified three research priority areas: "effectiveness of occupational therapy intervention, evidence-based occupational therapy practice and the development of valid and reliable occupational therapy measurement tools"52,6. Researchers should seriously consider how they can contribute to broadening and strengthening the evidence-base for our profession by focusing on these identified research priorities53.
At a systemic level, factors that continue to hamper the implementation of EBP include lack of access to appropriate research information56, limited resources and poor infrastructure in public health services, gaps in published research for the health conditions, context and type of practice in South Africa52'53 and a weak EBP culture56. Proposals arising from a national occupational therapy survey included the need for training to equip occupational therapists to implement EBP and increased availability and access to resources for research56.
Training has to occur at multiple levels - in formalised undergraduate and postgraduate programmes and as part of continuing professional development (CPD). To ensure that the country produces graduates that are adequately equipped to become evidence-based practitioners, university programmes need to instil thinking that both challenges and changes existing practices as advocated by Fleming-Castaldy and Gillen28. In line with the WFOT Minimum Standards for the Education of Occupational Therapists, educational curricula should incorporate content to equip students with the knowledge, skills and attitudes for EBP56. CPD activities could form part of a nation-wide programme aimed at equipping practitioners with the tools required for EBP and to provide updates on the latest evidence in particular fields of practice. Online tutorials could be a practical way of offering further training opportunities for participants to work through practical case examples designed to help them navigate through the thought processes related to EBP56.
Limitations
The authors acknowledge that the number of publications included in this review is not necessarily a full indication of research activity in South Africa. As the mapping review was limited to publications in the SAJOT it cannot be assumed to represent a complete view as research published in other journals has not been accounted for.
CONCLUSION AND RECOMMENDATIONS
As South African occupational therapists wrestle with dialogues about EBP, establishing a longitudinal view of the state of our evidence base is important for perspective making. In lieu of both the benefits and limitations of a paradigm shift in practice towards EBP, as alluded to by Kuhn's30 stages in the development of a profession, this mapping review provides significant clues, and perhaps challenges, about where we are, and where we may need to go.
On a micro-level, this mapping review offers insights that there may be missed opportunities in client-centeredness and subsequent client-provider conversations about evidence options due to the limited range of evidence produced. On a macro-level, in addition to contributing to larger dialogues about EBP, the review may be used to identify evidence gaps to set agendas for future research, evaluate grant applications according to the need for further research in a particular practice area, and to inform policy. It may also be useful for motivating for research funding to produce higher levels of evidence. Lastly, the review could be used as a discussion document to inform operational and strategic research priorities at local and national levels.
Author/s contributions
Fatima Hendricks conceptualised the original article and contributed to all subsequent data collection, analyses and revisions, and approved the final version of the article. Helen Buchanan guided the re-conceptualisation of the original draft and contributed to all subsequent data collection, analyses and revisions, and approved the final version of the article. Asia Clark assisted with the data extraction and analyses and approved the final version of the article.
REFERENCES
1. Ottenbacher K, Tickle-Degnen L, Hasselkus B. Therapists awake! The challenge of evidence-based occupational therapy. American Journal of Occupational Therapy. 2002; 56: 247-249. doi: https://doi.org/10.5014/ajot.56.3.247 [ Links ]
2.Sackett DL, Rosenberg WMC, Gray JAM, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn't. British MedicalJournal. 1996; 312: 71. doi: https://doi.org/10.1136/bmj.312.7023.71 [ Links ]
3.Bannigan K. Occupational therapy is not a leisure pursuit. British Journal of Occupational Therapy. 2004; 67: 147. doi: https://doi.org/10.1177/030802260406700401 [ Links ]
4.Walker MF. Past conditional, present indicative, future indefinite. British Journal of Occupational Therapy. 2004; 67: 207-214. doi: https://doi.org/10.1177/030802260406711S127 [ Links ]
5.Ballinger C and Wiles R. A critical look at evidence-based practice. British Journal of Occupational Therapy. 2001; 64: 253-255. doi: https://doi.org/10.1177/030802260106400507 [ Links ]
6.Reagon C, Bellin W and Boniface G. Reconfiguring evidence-based practice for occupational therapists. international Journal of Therapy and Rehabilitation. 2008; 15: 428-436. doi: https://doi.org/10.12968/ijtr.2008.15.10.31211 [ Links ]
7. Coster W. International conference on evidence-based practice: a collaborative effort of the American Occupational Therapy Association, the American Occupational Therapy Foundation, and the Agency for Healthcare Research and Quality. American Journal of Occupational Therapy. 2005; 59: 356-358. doi: https://doi.org/10.5014/ajot.59.3.356 [ Links ]
8.Holm M. Our mandate for the new millennium: evidence-based practice. AmericanJournal of Occupational Therapy. 2000; 54: 575-85. doi: https://doi.org/10.5014/ajot.54.6.575 [ Links ]
9.Berg, H. Evidence-based practice in Psychology fails to be tripartite: a conceptual critique of the Scientocentrism in evidence-based practice in Psychology. Frontiers in Psychology. 2019; 10: 2253. doi: https://doi.org/10.3389/fpsyg.2019.02253 [ Links ]
10. Lagerlof H, Zuiderent-Jerak T, Sager M. Epistemological deliberation: the challenges of producing evidence-based guidelines on lifestyle habits. Evidence & Policy. 2021; 17(4): 709-727. doi: https://doi.org/10.1332/174426421X16149619907286 [ Links ]
11. Woodbury MG, Kuhnke JL. Evidence-based practice vs evidence-informed practice: What's the difference? Wound Care Canada. 2014; 12(1): 26-29. [ Links ]
12. Kirkland DE. No small matters: Reimagining the use of research evidence from a racial justice perspective. New York: William T. Grant Foundation; 2019. [ Links ]
13. Loper A, Fleming WO. Dismantling racism in public health: reconsidering the role of evidence. Pulse Newsletter, Association of Maternal and Child Health Programs. 2020 [accessed 2022 April 01]. https://amchp.org/dismantling-racism-in-public-health-reconsidering-the-role-of-evidence/#_ftnref2 [ Links ]
14.Bennett M. Decolonizing evidence to better support native communities. Community Health. 2020 [accessed 2022 April 01]. https://www.publichealth.columbia.edu/public-health-now/news/decolonizing-evidence-better-support-native-communities [ Links ]
15. Lucero E. From tradition to evidence: decolonization of the evidence-based practice system.Journal of Psychoactive Drugs. 2011; 43(4): 319-324. doi: https://doi.org/10.1080/02791072.2011.628925 [ Links ]
16. Lomas J, Culyer T, McCutcheon C, McAuley L, Law S. Conceptualizing and combining evidence for health system guidance. Canadian Health Services Research Foundation. 2005 [accessed 2022 April 01]. http://www.chsrf.ca/other_documents/pdf/evidence_e.pdf [ Links ]
17. Hinojosa J. The issue is... The evidence-based paradox. American Journal of Occupational Therapy. 2013; 67(2): e18-e23. doi: https://doi.org/10.5014/ajot.2013.005587 [ Links ]
18. Upton D, Stephens D, Williams B, Scurlock-Evans L. Occu pational therapists' attitudes, knowledge, and implementation of evidence-based practice: a systematic review of published research. British Journal of Occupational Therapy. 2014; 77(1): 24-38. doi:10.4276/030802214X13887685335544 [ Links ]
19. Steward B. The theory/practice divide: bridging the gap in Occupational Therapy. British Journal of Occupational Therapy. 1996; 59(6), 264-268. doi: https://doi.org/10.1177/030802269605900604 [ Links ]
20. Pitout H. Barriers and strategies to increase research involvement of South African occupational therapists. South African Journal of Occupational Therapy. 2014; 44(2): 17-21. [ Links ]
21. Bennett S, Townsend L. Evidence-based practice in Occupational Therapy: International Initiatives. World Federation of Occupational Therapists Bulletin. 2006; 53(1): 6-12. doi: https://doi.org/10.117/otb.2006.53.1.002 [ Links ]
22. Serwe KM, Cores K, Mettler M, Smith J, Steger K, Dougherty D. International position statements on evidence-based practice in occupational therapy: a qualitative content analysis. Annals of International Occupational Therapy. 2021; 4(3): e101-e108. doi: https://doi.org/10.3928/24761222-20200619-02 [ Links ]
23. Association of Canadian Occupational Therapy Regulatory Organizations. Joint position statement on evidence-based occupational therapy. 2009; https://www.caot.ca/document/3697/J%20-%20Joint%20Position%20Statement%20on%20Evidence%20based%20OT.pdf [ Links ]
24. Rycroft-MaloneJ. Evidence-informed practice: from individual to context. Journal of Nursing Management. 2008; 16(4):404-4088. doi: https://doi.org/10.1111/j.1365-2834.2008.00859.x [ Links ]
25. Kumah EA, McSherry R, Bettany-SaltikovJ, Van Schaik R Evidence-informed practice: simplifying and applying the concept for nursing students and academics. British Journal of Nursing. 2022; 31(6): 322-330. doi: https://doi.org/10.12968/bjon.2022.31.6.322 [ Links ]
26. Boaz A, Davies H, Fraser A, Nutley S (Eds.). What works now? Evidence-informed policy and practice. Bristol, UK: Policy Press; 2019. [ Links ]
27. Ontario Centre of Excellence for Child & Youth Mental Health (OCECYMH). Glossary. Ontario, Canada: Ontario Centre of Excellence for Child & Youth Mental Health. 2019 [accessed 2022 April 1]. http://www.kmbtoolkit.ca/glossary-glossaire#undefined [ Links ]
28. Fleming-Castaldy R, Gillen G. Ensuring that education, certification, and practice are evidence based. American Journal of Occupational Therapy. 2013; 67: 364-369. doi: https://doi.org/10.5014/ajot.2013.006973 [ Links ]
29. Kuhn T. The structure of scientific revolutions, 2nd ed. Chicago: University of Chicago Press; 1970. [ Links ]
31. Cresswell J. Research design. Qualitative, quantitative and mixed methods approaches. 2nd ed. Thousand Oaks: SAGE Publications; 2003. [ Links ]
32. Higgs P, Smith J. Rethinking truth. 2nd ed. Cape Town: Juta and Company Ltd; 2006. [ Links ]
33. Bowling A. Research methods in health. Investigating health and health services. 3rd ed. Berkshire: Open University Press; 2009. [ Links ]
34. Evans D. Hierarchy of evidence: a framework for ranking evidence evaluating healthcare interventions.Journal of Clinical Nursing; 2003; 12: 77-84. doi: https://doi.org/10.1046/j.1365-2702.2003.00662.x [ Links ]
35. DePoy E, Gitlin L. Introduction to research. Understanding and applying multiple strategies. 3rd ed. St Louis: Elsevier Mosby; 2005. [ Links ]
36. American Occupational Therapy Association. Occupational therapy practice framework: domain and process (4th ed.). American Journal of Occupational Therapy. 2020; 74(Suppl. 2): 7412410010. doi: https://doi.org/10.5014/ajot.2020.74S2001 [ Links ]
37. Whiteford G, Wright-St Clair V. Occupation and practice in context. Sydney: Elsevier, 2005. [ Links ]
38. Tickle-Degnen L, Bedell G. Heterarchy and hierarchy: a critical appraisal of the "levels of evidence" as a tool for clinical decision-making. American Journal of Occupational Therapy. 2003; 57(2): 234-237. doi: https://doi.org/10.5014/ajot.57.2.234 [ Links ]
39. Ramugondo EL. Occupational Consciousness. Journal of Occupational Science. 2015; 22(4): 488-501. doi: https://doi.org/10.1080/14427591.2015.1042516 [ Links ]
40. Broodryk J. Ubuntu. Life lessons from Africa. Pretoria: Ubuntu School of Philosophy; 2002. [ Links ]
41. Pityana N. The renewal of African moral values. In: Makgoba M, (ed.). African renaissance. Cape Town: Mafube Publishing; 1999; 137-148. [ Links ]
42. Kollen BJ, Lennon S, Lyons B, Wheatley-Smith L, Scheper M, Buurke JH, Halfens J, Geurts AC, Kwakkel G. The effectiveness of the Bobath concept in stroke rehabilitation: What is the evidence? Stroke. 2009; 40(4): e89-e97. doi: https://doi.org/10.1161/STROKEAHA.108.533828 [ Links ]
43. Chabon S, MorrisJ, Lemoncello R. Ethical deliberation: a foundation for evidence-based practice. Seminars in Speech and Language. 2011; 32(4): 298-308. doi: http://dx.doi.org/10.1055/s-0031-1292755 [ Links ]
44. World Federation of Occupational Therapists. World Federation of Occupational Therapists (WFOT) Code of Ethics: 2016. [accessed 2023 June 14]. https://www.wfot.org/resources/code-of-ethics [ Links ]
45. Occupational Therapy Association of South Africa. Code of ethics and professional conduct (revised July 2005). 2005; 2010 October 01. doi: http://www.otasa.org.za/documents/code_of_ethics_2005.pdf [ Links ]
46. Health Professions Council of South Africa. Guidelines for good practice in the healthcare professions. Ethical and professional rules of the Health Professions Council of South Africa. Booklet 2. Pretoria: Health Professions Council of South Africa. 2016 [accessed 2022 April 1]. https://www.hpcsa.co.za/Uploads/editor/UserFiles/downloads/conduct_ethics/Booklet%202.pdf [ Links ]
47. Perryman CL. Mapping studies. Medical Library Association. 2016; 104(1): 79-82. doi: http://dx.doi.org/10.3163/1536-5050.104.L014 [ Links ]
48. Booth A. EVIDENT Guidance for Reviewing the Evidence: a compendium of methodological literature and websites. 2015 [accessed 2023 June 07]. https://www.researchgate.net/publication/292991575_EVIDENT_Guidance_for_Reviewing_ the_Evidence_a_compendium_of_methodoIogical_Literatureand_websites#fullTextFileContent [ Links ]
49. National Health and Medical Research Council. NHMRC additional levels of evidence and grades for recommendations for developers of guidelines. Stage 2 Consultation. Australian Government: NHMRC. 2009 [accessed 2023 September 14]. https://www.mja.com.au/sites/default/files/NHMRC.levels.of.evidence.2008-09.pdf [ Links ]
50. Ahmed AK. #RhodesMustFall: How a decolonial student movement in the Global South inspired epistemic disobedience at the University of Oxford. African Studies Review. 2020; 63(2), 281-303. [ Links ]
51. Booysen S (Ed.). Fees Must Fall: student revolt, decolonisation and governance in South Africa. Wits University Press, 2016. doi: https://doi.org/10.18772/22016109858 [ Links ]
52. Soeker, MS, Olaoya, O. Determining the research priorities for the profession of Occupational Therapy in South Africa. South AfricanJournal of Occupational Therapy. 2023; 53(1):6-7. doi: https://doi.org/10.17159/2310-3833/2023/vol53n1a2 [ Links ]
53. Franzsen D, Pretorius B. The need for high quality clinical research in occupational therapy. South African Journal of Occupational Therapy. 2023; 53(1): 4-5. doi: https://doi.org/10.17159/2310-3883/2023/vol53n1a1 [ Links ]
54. Pitout H. Research orientation of South African occupational therapists. South AfricanJournal of Occupational Therapy. 2013; 43(2), 5-11. [ Links ]
55. Du Toit S, Wilkinson A. Publish or perish: a practical solution for research and publication challenges of occupational therapists in South Africa. South African Journal of Occupational Therapy. 2009; 39: 2-7. [ Links ]
56. Buchanan H. Evidence-based practice in occupational therapy in South Africa and the Western Cape [PhD thesis]. Cape Town (South Africa): University of Cape Town; 2011. [accessed 2023 June 14]. https://open.uct.ac.za/handle/11427/10185 [ Links ]
 Correspondence:
Correspondence:
Helen Buchanan
helen.buchanan@uct.ac.za
Submitted: 24 October 2022
Reviewed: 15 February 2023
Revised: 15 June 2023
Accepted: 21 June 2023
Editor: Blanche Pretorius; https://orcid.org/0000-0002-3543-0743
Data availability: From the corresponding author
Funding: No funding was received for this study

