










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versión On-line ISSN 2310-3833
versión impresa ISSN 0038-2337
S. Afr. j. occup. ther. vol.53 no.2 Pretoria ago. 2023
http://dx.doi.org/10.17159/2310-3833/2023/vol53n2a7
RESEARCH ARTICLE
Comparing the impact of two occupational therapy interventions on academic learning outcomes for children with Human Immunodeficiency Virus
Caraleigh OttoI, II; Pamela GretschelI; Elelwani RamugondoI
IDivision of Occupational Therapy, Department of Health and Rehabilitation Sciences, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa. Pamela Gretschel: http://orcid.org/0000-0002-7890-3635; Elelwani Ramugondo: http://orcid.org/0000-0002-1987-4651
IIPrivate Practice, Western Cape, South Africa. Caraleigh Otto: https://orcid.org/0000-0002-7162-9194
ABSTRACT
INTRODUCTION: The strong association between perinatal HIV infection and poor performance in academic learning is further challenged by various barriers to learning in the South African context of basic education. This study investigated the efficacy of a novel play-informed, caregiver-implemented, home-based intervention (PICIHBI) for improving academic learning in HIV-positive children
METHODOLOGY: A single-blinded, randomised comparison group design was selected to compare PICHIBI with conventional one-on-one occupational therapy interventions. Children with HIV aged 5 to 8 years old on ART and their primary caregiver (N=23) were randomly allocated to an intervention group. The primary outcome of academic learning was measured using the Griffiths Mental Developmental Scales-Extended Revised and the short form Beery-Buktenica Visual Motor Integration test, 5th edition at baseline, mid (5 months) and post-intervention (after 10 months
RESULTS: At baseline, the total sample (n=23) presented with below-average performance in all assessed academic learning outcomes. Between-group differences for all academic learning outcomes were not significant at mid or post-test assessment points. A statistically significant within-group change in visual motor integration was noted in the PICIHBI from baseline to mid-test (p=.019). In the conventional group, there were statistically significant changes in visual perception from baseline to mid (p=.001) and baseline to post-test (p=.009). The sub scale Performance in the conventional group improved significantly from baseline to mid-test (p=.027
CONCLUSION: While improvements were noted, children in both groups continued to present with academic learning concerns at post-test. These concerns motivate the need for continued monitoring and further investigation into the feasibility and effectiveness of occupational therapy interventions targeting the academic learning challenges of this population
Implications for practice
This paper adds to an emerging body of evidence aiming to demonstrate the effect of occupational therapy interventions on occupational outcomes for children with perinatal HIV infection. The paper presents a detailed overview of the conceptualisation of learning as an occupational outcome. The paper further presents consideration of the practical challenges linked to the implementation of, adherence to and sustainability of rehabilitation interventions in low to middle-income countries.
Keywords: HIV-positive children, Griffiths Mental Developmental Scales, Beery-Buktenica Visual Motor Integration, learning as an occupational outcome, play-informed, caregiver-implemented, home-based intervention
INTRODUCTION AND LITERATURE REVIEW
Prevention of mother-to-child transmission programmes (PMTCT)1 have led to the wider provision of antiretroviral therapy (ART) and, as a result, more children with Human Immunodeficiency Virus (HIV) are reaching school-going age2. In South Africa, an estimated 260,000 children (aged 0 to 14) live with HIV3. Their academic learning success is negatively impacted by delays in their motor and neuro-cognitive functioning4,5,6,7,8.
Studies comparing the HIV-infected child's functional and intellectual abilities to their HIV-uninfected peers9,10, 11 support the call for children with HIV to receive intervention12,13. HIV is particularly prominent in low-income countries like South Africa, where its negative effect on neuro-cognition and visual perceptual skills is undoubtedly exacerbated by contextual barriers to learning14. Despite this, at the time of this study, only one intervention study focused on promoting developmental outcomes in an HIV-infected paediatric population in South Africa could be sourced. In this study, a home stimulation programme taught to the child's caregiver significantly improved the developmental progression of HIV positive children who were younger than 2 years and 6 months15. Occupational therapists promote a child's ability to engage in academic learning, often using play as a means to address barriers limiting their engagement and performance in academic learning 16. Descriptions of, and studies exploring the effectiveness of occupational therapy interventions for HIV-positive children are scant. This paper presents the results of a postgraduate study investigating and comparing the effect of two occupational therapy interventions on the academic learning of HIV-infected children. The hypothesis for the study was that HIV-positive children on ART aged 5-8 years, taking part in the novel play-informed caregiver-implemented home-based intervention (PICHIBI), would demonstrate more improvement in their academic learning outcomes than those children receiving conventional one-on-one occupational therapy intervention. The conceptualization of academic learning outcomes to guide the development of the PICIHBI is presented in Figure 1 (above).
MATERIALS AND METHODS
Design and ethical considerations
Drawing on the CONSORT statement, a single-blinded, randomised comparison group design17 was used to report the effectiveness of the novel PICIHBI. Ethical approval for the study was obtained from the University of Cape Town Human Research Ethics Committee (HREC/REF: 772/2014). The study was a sub-study nested in a larger study registered with the South African National Clinical Trial Registry through the National Health Research Ethics Council (Trial number: DOH-27-0115-4892). The larger study is registered with the South African National Clinical Trial Registry through the National Health Research Ethics Council (trial number: DOH-27-0115-4892).
Participants
All children aged between 5 years 0 months and 8 years 0 months and their caregivers attending the monthly outpatient paediatric anti-retroviral (ARV) clinic at Groote Schuur hospital, a tertiary hospital based in Cape Town, were considered eligible to participate in the study. Caregiver participants were those persons who spent no less than seven hours of direct contact time a week with the child, and who were able to attend at least five out of the ten intervention sessions. All child participants lived in low-income areas and were HIV positive following vertical transmission. The clinic database consisted of 60 participants who met these criteria. A translator fluent in isiXhosa assisted in contacting the potential participants.
Sample size and power
A convenient sample of 27 dyads (caregiver and child) was arrived at to align with 90% power at a non-inferiority difference of 6 points between groups with a standard deviation of 10. This power was retained even after a 15% loss to follow-up, reducing the chance of a Type II error.
Randomisation
Using a random sequence generator, participants were assigned to treatment groups. Randomisation was completed after the participants had consented to participate and conducted their baseline assessments. All researchers and assessors were blinded to the allocation process.
Measures (Instrumentation)
A background information questionnaire completed by caregivers collected data relating to caregiver and child socio-demographics, the developmental history of the child, an overview of medical and rehabilitation interventions provided to the child up to this point, the child's ART treatment regime, and their schooling, play, and television viewing habits. Caregivers were asked to comment on their child's learning and bring copies of their school reports to provide information about their academic learning progress in the school context.
The Griffiths Mental Development Scale-Extended Revised (GMDS-ER) version for children aged 2-8 years consists of six subscales. Four of the six subscales were used in this study: language (subscale C), eye-hand coordination (subscale D), performance (subscale E) and practical reasoning (subscale F). Functional age in each subscale can be obtained through computation and developmental quotients for each subscale can be calculated by dividing the functional age of the child by their chronological age at the time of testing18. The GMDS-ER is used in South Africa as well as internationally and is considered to be a valid and reliable tool to use with diverse populations2,19,20,21.
The Beery-Buktenica Developmental Test of Visual Motor Integration 5th edition (DTVMI)22 was used to assess the child's ability to coordinate their visual perception and motor abilities. The DTVMI is frequently used in South Africa 23,24,25. The DTVMI has high reliability and validity across a 3-18-year age range and adequate cross-cultural validity 22,26,27. Standard scores were calculated from raw scores using USA norms.
Academic learning outcomes were represented by standardized scores with a mean quotient of 100 (15) for the GMDS-ER and a mean standard score of 100 (15) for the DTVMI. Scores between 90-109 are considered average and <70 as intellectually impaired22,19.
Procedures
A pilot study was conducted prior to the baseline to ensure inter-rater reliability. Five assessors, all occupational therapists trained in using the GMDS-ER, assessed sixteen children from a local tertiary children's hospital. The raw scores of these assessments were correlated with the aim being to achieve a minimum level of 90% agreement. Cronbach alpha coefficients were calculated to ensure internal consistency and the coefficients all exceeded the value of 0.70, an acceptable minimum value of reliability19. Raw scores differed by a maximum of two to eight points between any two assessors. There was 100% agreement on the age calculations. The reliability measure between the other GMDS-ER scores (quotient, age-equivalent, z-score, percentile) varied between 0.99 and 1.
Data were collected at three intervals, baseline test (before the intervention had started), mid-test (at five months) and post-test (at ten months). The caregivers completed the background information questionnaire at baseline assessment. Data were also collected on intervention session attendance rates and participant dropout rates for both intervention groups.
The therapists and researchers met monthly throughout the intervention period for group meetings to ensure the intervention was being carried out as documented. In these spaces, the challenges and successes related to designing and implementing this intervention were discussed within the methodology of a cooperative inquiry28.
PICIHBI group: Play informed, caregiver implemented, home-based intervention (PICIHBI)
The intervention design team drew on the National Curriculum Statements29 to guide the determination of the specific academic learning-related skills (literacy, numeracy, gross motor, fine motor, and language) to be focused on in each of the intervention sessions. Additionally, research focused on child development and play theory guided how to make optimal use of play as a means to guide the development of the afore-mentioned academic learning skills in the intervention30. Both the child and the caregiver attended the monthly 90-minute PICIHBI intervention sessions. During the first 45 minutes, while the children were cared for by the clinic-appointed childminder, the caregivers engaged with the occupational therapist, and other caregivers in the group, learning how to promote their child's engagement in play, learning and development. The remaining 45 minutes were experiential. Children joined in the sessions and caregivers were guided to apply the knowledge they had learned practically using play items provided to them in each session. At the end of each session, the dyad was given the play item (for example, crayons, scissors, puzzles etc.) that was used in that session to add to their 'Go Box', a take-home tool kit consisting of age-appropriate stimulation items. Caregivers could also use play items they had at home. Each group consisted of approximately five caregiver-child dyads, an occupational therapist, and a translator/facilitator. Caregivers were encouraged to implement the weekly group activities at home with their children. At the following group session, feedback from the caregivers was given and then documented, along with attendance, in the therapist's notes. This feedback was used to inform and build on the design of the intervention manual, which included the intervention sessions and protocols for implementing the intervention.
Comparison Group: Conventional one-on-one occupational therapy
Conventional one-on-one occupational therapy intervention was the comparison intervention. In this intervention, the child was the direct focus and although not compulsory, caregivers were welcome to sit in on and observe the sessions. Each child was offered ten 45-minute sessions. At the end of the ten sessions, once post-test had been completed, the child was issued with a 'Go Box' to take home with them.
Data collectors were blinded to the allocation of participants throughout the intervention period. Codes for each dyad were used to ensure blinding. Un-blinding occurred once all post-tests had been completed and all assessments had been scored. The participants and their caregivers were not blinded to the intervention, but to the hypothesis of the study. All assessments were administered outside intervention periods one and two.
Statistical Analysis
All data were analysed using the Statistical Package for the Social Sciences (SPSS)31 at 95% confidence interval and a significant p-value of <0.05. Performance below normal functional limits was rated as a score <-2 SD or <70, for both assessment tools. Univariate (descriptive), bivariate (correlations) and multivariate (regression) analyses took place. As the total sample size was less than 50, (N=23) the Shapiro-Wilk Test of Normality was used to determine the distribution of the sample. The Levene's Test for equality showed equal variances for all subscales during the test periods. Since there were no statistically significant differences between the groups using the 2-sample t-test (independent t-test), paired t-tests (dependent t-test) were conducted to determine whether any significant within-group changes had occurred. Analysis of Covariance (ANCOVA) was used where indicated, to establish which factors had the greatest relationships on variables of interest. Intention to treat (ITT) analysis was carried out in this study. The participants who did not attend all intervention sessions were still tested at post-test and their results were captured and analysed.
RESULTS
The baseline test sample size consisted of 27 dyads (n=27). One participant was transferred to a home of safety, leaving 26 participants who underwent randomisation following baseline assessment. The small sample resulted from dyads not meeting the inclusion criteria, not wanting to participate or not being contactable for assessment dates. Two participants were lost to follow-up after the baseline test, and one was transferred to a home of care. The total sample at the end of the study was n=23. Please refer to Figure 2 (page 67).
Baseline demographics
Baseline demographics are presented in Table I (above).
Mothers were the main caregivers, with the majority attaining a high school level of education. Participants in both groups generally had low viral load LDL* The independent t-test showed statistical significance for a time in which participants had been on ART (p=.021) with the comparison group being on ART longer. The Levene's Test for equality of variances was used on baseline test demographics to test if both groups had equal variances.
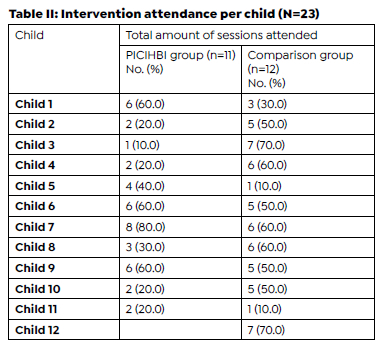
Intervention attendance
The session attendance rates varied across the intervention period with participants reporting that transport and employment factors affected their attendance at the intervention sessions. Various measures were put into place to reduce the effects of varied attendance; including reimbursing the participants for their transport costs to and from the hospital and providing the caregivers with letters to give to their employers for the days of work missed. Table II (above) shows the intervention attendance.
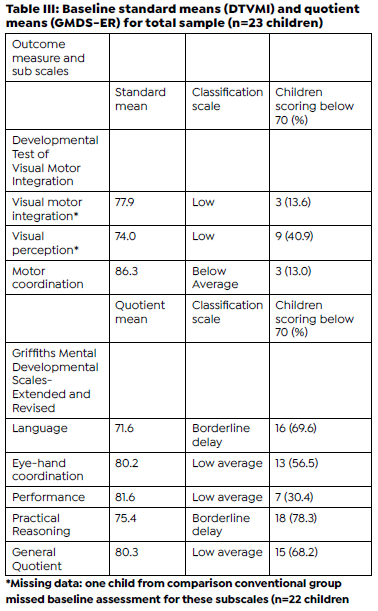
Aim 1: Academic learning profile of children with HIV
The academic learning profile of the total sample measured at baseline is presented below in Table III (above). The standard means of the DTVMI, and the quotient means of the GMDS-ER showed that the total sample presented with below-average scores for all academic learning outcomes measured at baseline. Standard mean and quotient mean scores below 70 indicate the presence of significant challenges. The academic learning outcomes most affected were visual perception, language, and practical reasoning.
Aim 2: Preliminary effectiveness of the PICIHBI for improving academic learning
The preliminary effectiveness of the PICIHBI for improving academic learning is represented by the presentation of Table IV and V (page 70) describing the between-group and within-group changes in both the PICIHBI and comparison conventional group for both the DTVMI and GMDS-ER.
Overall change in DTVMI scores over time
There were not statistically significant between-group differences at any time point in the intervention (p>0.05). Statistically significant within-group changes were noted. In the PICIHBI group, VMI improved from baseline to mid-test (p= .019). In the comparison conventional group, there was a statistically significant improvement in VP from baseline to mid-test (p= .001). While the mean VP standard score decreased from mid-test to post-test (88.7), the overall change in VP from baseline to post-test remained significant (p= .009). The only decrease in mean standard scores from baseline to post-test was seen in the PICIHBI group for motor co-ordination. In the other subtests, both groups improved throughout the intervention period. These changes were not statistically significant. None of the children in the PICIHBI scored <70 (severe delay) at post-test.
Overall change in GMDS-ER scores over time
No statistically significant between-group differences were found for any of the GMDS-ER outcomes at any time point (p>0.05). One within-group change was noted. A statistically significant improvement in performance was observed for the conventional group from baseline to mid-test (p=.027). While not statistically significant, changes were noted within the two groups. Except for language and practical reasoning in the conventional group, all post-test assessment scores were higher than the baseline assessment scores in both groups. Scores generally improved from baseline to mid-test except for eye-hand coordination in the PICIHBI group and language, practical reasoning, and general quotient in the comparison conventional group. Eye-hand coordination and general quotient improved at post-test and were higher than the baseline assessment, while language and practical reasoning continued to decline, and post-test scores were lower than baseline.
Aim 3: Grade progression
The third objective was to track the grade progression of the children in each group. Only one child in the comparison conventional group repeated a grade, grade one, the second year of formal schooling in South Africa.
Adverse Effects
No adverse effects were noted or documented.
DISCUSSION
At the time, this study was novel in its exploration of the impact of an occupational therapy intervention on the academic learning outcomes of the HIV-infected child on ART. Baseline results showed that the total sample all performed below average on all academic learning outcomes as measured by the DTVMI and the GMDS-ER. The academic learning outcomes most affected were visual perception, language, and practical reasoning. For visual perception, 40.9% of the total sample scored <70 at baseline. The high percentage of children experiencing difficulties with visual perception correlates with the results of a study by Laughton et al 32. showing the negative impact of HIV on visual perception, regardless of the ART regime provided. Visual perceptual difficulties are a concern as a visual learning approach is dominant in many school environments33. For practical reasoning and language, 78.3% and 69.6% respectively of the children scored <-2 z-scores, which was also consistent with prior studies describing neurodevelopment in HIV children 2 7,11,21.
Between-group analysis showed that there were no statistically significant differences in the performance of the groups at all measurement points for all academic learning outcomes. This showed that PICIHBI had equivalent effects on the academic learning outcomes for HIV-positive children aged 5 - 8 years, on ART and living in low SES families, when compared to the comparison conventional group.
Within-group analysis showed some statistically significant results. PICHIBI was significantly more effective (p=.019) in improving visual motor integration over a five-month intervention period, from baseline to mid-test. The positive change in a group format intervention over a five-month period is encouraging as well-developed visual motor integration skills have been linked to the development of effective handwriting in children34 and high levels of academic performance25. The conventional intervention was significantly beneficial in improving visual perception over a five- and ten-month intervention period, which could possibly be linked to the more intensive focus placed on specific visual perceptual skills within the format of the individual conventional intervention approach. A statistically significant improvement in performance was observed for the comparison conventional group (p=.027) from baseline to mid test. While there were decreases and increases in other academic learning outcomes, between assessment points for each group, none of these changes was statistically significant which supports specific time points were not more viable to effect changes in these outcomes. While there was a decrease in the number of children scoring <70 seen from baseline to post-test in both groups, children continued to present with difficulties in academic learning outcomes at post-test.
Limitations
A small sample size (n=23) resulted in wider confidence intervals affecting the generalizability of the results. No follow-up assessments were conducted, and this limited the researcher's discernment if the improvements or digression in scores in the various academic learning outcomes, were purely due to intervention or in addition to the natural maturation of a child over time. Not all variances measured in the two groups were equal and this may have affected a Type I error rate. Attaining participants' recent school reports would have allowed for further comparisons to be made between academic learning outcomes assessed in the intervention, and the child's engagement and performance in academic learning in the context of the school classroom.
CONCLUSION
This article highlighted the delays in various academic learning outcomes of HIV-positive children which will assist in informing occupational therapy practice protocols, policies, and legislations, relating to academic learning for children with HIV on ART in South Africa. Delays in the areas of language and practical reasoning should urge occupational therapists to partner with communication science therapists and educational specialists to design interventions which support the academic progress of children with HIV living in the multi-lingual context of South Africa. Rehabilitation in South Africa continues to be undermined by staffing constraints limiting access to services. The group format of the PICIHBI holds the potential to have a greater reach when compared to conventional one-on-one intervention35. Attendance was however problematic with a slightly higher level of attendance in the comparison control group. Further investigation into the feasibility and effect of PICHBI within a larger multi-site study, drawing on mechanisms to build on attendance, is thus recommended.
Lessons learnt
During the process of planning and implementing the RCT, the following lessons were learnt:
• Diligent reporting of all aspects of the process of the study must take place in line with the CONSORT statement17 to ensure all decisions made and actions taken, are documented.
• Although the RCT took place in a central site which participants were already accessing for other health services, regular attendance was still a challenge. Researchers planning RCTs need to consider the existing health, employment and personal schedules of participants when planning sessions and factor in reimbursement for travel to and from appointments, to encourage more regular attendance.
• Researchers planning RCTs should plan to conduct post trial follow up assessments to monitor the sustained impact of the interventions.
Conflicts of interest
The Authors declare that there is no conflict of interest.
Author contributions
Caraleigh Otto: Conceptualization, Methodology, Investigation, Original draft preparation, Writing-Reviewing and Editing. Pam Gretschel: Conceptualization, Methodology, Writing-Reviewing and Editing, Visualization, Supervision, Project administration. Elelwani Ramugondo: Conceptualization, Methodology, Writing-Reviewing and Editing, Supervision, Project administration
REFERENCES
1. Department of Health: National Consolidated Guidelines for the Prevention of Mother-to-Child Transmission of HIV (PMTCT) and the Management of HIV in Children, Adolescents and Adults. 2015. [accessed 2022 June 22]. doi:https://www.knowledgehub.org.za/system/files/elibdownloads/2019-07/National%2520consolidated%2520guidelines%25202015.pdf [ Links ]
2. Potterton J, Hilburn N, Strehlau R. Developmental status of preschool children receiving cART: a descriptive cohort study. Child: Care, Health and Development. 2016; 42(3):410-414. doi: http://dx.doi.org/10.1111/cch.12321 [ Links ]
3. Aids info: People living with HIV receiving ART. [accessed 2020 June 15]. Available from: https://aidsinfo.unaids.org/ [ Links ]
4. Chinembiri, B.; Wei, C.; Ming, Z.; Kai, S. A Comparison of the Visual Perceptual Processing Skills of Children (6-10 Years Old) with and without Human Immuno-Deficiency Virus (HIV) Using the Test of Visual Perceptual Skills-3rd Edition (TVPS-3) in Harare, Zimbabwe. Preprints. 2018. doi:https://www.preprints.org/manuscript/201808.0462/v1 [ Links ]
5. Knox J, Arpadi SM, Kauchali S, Craib M, Kvalsvig JD, Taylor M, et al. Screening for developmental disabilities in HIV positive and HIV negative children in South Africa: Results from the Asenze Study. PLOS ONE. 2018; 13(7):e0199860. doi:https://doi.org/10.1371/journal.pone.0199860 [ Links ]
6. Laughton B, Cornell M, Boivin M, Van Rie A. Neurodevelopment in perinatally HIV-infected children: a concern for adolescence. Journal of the International AIDS Society. 2013;16(1). doi:http://dx.doi.org/10.7448/ias.16.1.18603 [ Links ]
7. Puthanakit T, Ananworanich J, Vonthanak S, Kosalaraksa P, Hansudewechakul R, van der Lugt J, et al. Cognitive Function and Neurodevelopmental Outcomes in HIV-infected Children Older Than 1 Year of Age Randomized to Early Versus Deferred Antiretroviral Therapy. Pediatric Infectious Disease Journal. 2013; 32(5):501-508. doi:http://dx.doi.org/10.1097/inf.0b013e31827fb19d [ Links ]
8. Odejayi R, Franzsen D, De Witt P. Visual motor integration delay in preschool children infected with HIV. South African Journal of Occupational Therapy. 2019;49(3):24-30. doi:http://dx.doi.org/10.17159/2310-3833/2019/vol49n3a5 [ Links ]
9. Boyede G, Lesi, Ezeaka C, Umeh. Impact of sociodemographic factors on cognitive function in school-aged HIV-infected Nigerian children. HIV/AIDS - Research and Palliative Care. 2013; 145. doi:http://dx.doi.org/10.2147/hiv.s43260 [ Links ]
10. Cohen S, ter Stege JA, Geurtsen GJ, Scherpbier HJ, Kuijpers TW, Reiss P, et al. Poorer cognitive performance in perinatally HIV-infected children versus healthy socioeconomically matched controls. Clinical Infectious Diseases. 2014; 60(7):1111-1119. doi: http://dx.doi.org/10.1093/cid/ciu1144 [ Links ]
11. Frolek Clark GJ, Schlabach TL. Systematic Review of Occupational Therapy Interventions to Improve Cognitive Development in Children Ages Birth-5 Years. The American Journal of Occupational Therapy.2013; 67(4):425-3. doi: http://dx.doi.org/10.5014/ajot.2013.006163 [ Links ]
12. Linn K, Fay A, Meddles K, Isbell S, Lin PN, Thair C, et al. HIV-Related Cognitive Impairment of Orphans in Myanmar With Vertically Transmitted HIV Taking Antiretroviral Therapy. Pediatric Neurology. 2015; 53(6):485-490. doi: http://dx.doi.org/10.1016/j.pediatrneurol.2015.08.004 [ Links ]
13. Guo Y, Li X, & Sherr L. The impact of HIV / AIDS on children's educational outcome: A critical review of global literature. AIDS Care. 2012; 24(8): 993-1012. doi: https://doi.org/10.1080/09540121.2012.668170 [ Links ]
14. Donald KA, Walker KG, Kilborn T, Carrara H, Langerak NG, Eley B, et al. HIV Encephalopathy: pediatric case series description and insights from the clinic coalface. AIDS Research and Therapy. 2015;12(1): 2. doi:http://dx.doi.org/10.1186/s12981-014-0042-7 [ Links ]
15. Potterton, J., Steward, A., Cooper, P., Becker, P. The effect of a basic home stimulation programme on the development of young children infected with HIV. Developmental Medicine & Child Neurology. 2009; 52(6):547-551. doi: http://dx.doi.org/10.1111/j.1469-8749.2009.03534.x [ Links ]
16. Dankert HL, Davies PL, Gavin WJ. Occupational Therapy Effects on Visual-Motor Skills in Preschool Children. The American Journal of Occupational Therapy. 2003; 7(5):542-549. doi: http://dx.doi.org/10.5014/ajot.57.5.542 [ Links ]
17. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. Trials. 2010;11(1). doi: http://dx.doi.org/10.1186/1745-6215-11-32 [ Links ]
18. Reyes A, Pacifico R, Benitez B, Villanueva-Uy E, Lam H, Ostrea Jr EM. Use of the Griffiths Mental Development Scales in an agro-industrial province in the Philippines. Child: Care, Health and Development. 2010; 36(3):354-360. doi: http://dx.doi.org/10.1111/j.1365-2214.2010.01080.x [ Links ]
19. Luiz DM, Foxcroft CD, Stewart R. The construct validity of the Griffiths Scales of Mental Development. Child: Care, Health and Development. 2001; 27(1):73-83. doi: http://dx.doi.org/10.1046/j.1365-2214.2001.00158.x [ Links ]
20. Laughton B, Springer PE, Grove D, Seedat S, Cornell M, Kidd M et al. Longitudinal developmental profile of children from low socio-economic circumstances in Cape Town, using the 1996 Griffiths Mental Development Scales. South African Journal of Child Health. 2010; 4(1), 106-111. PMID:22984637; PMCID:PMC3439644. [ Links ]
21. Lowick S, Sawry S, Meyers T. Neurodevelopmental delay among HIV-infectedpreschool children receiving antiretroviral therapy and healthy preschool children in Soweto, South Africa. Psychology, Health & Medicine. 2012; (5):599-610.doi: http://dx.doi.org/10.1080/13548506.2011.648201 [ Links ]
22. Beery KE & Beery NA. The Beery-Buktenica Developmental Test of Visual-Motor Integration with supplementary developmental tests of Visual perception and Motor coordination Administration, scoring and teaching manual (5th ed.). 2004. Minneapolis, MN: NCS Pearson, Inc. [ Links ]
23. Dunn M, Loxton H, Naidoo A. Correlations of Scores on the Developmental Test of Visual-Motor Integration and Copying Test in a South African Multi-Ethnic Preschool Sample. Perceptual and Motor Skills. 2006; 103(3):951-958. doi: http://dx.doi.org/10.2466/pms.103.3.951-958 [ Links ]
24. Lotz L, Loxton H, Naidoo AV. Visual-motor integration functioning in a South African middle childhood sample. Journal of Child & Adolescent Mental Health. 2005; 17(2):63-67. doi: http://dx.doi.org/10.2989/17280580509486602 [ Links ]
25. Pienaar AE, Barhorst R, Twisk JWR. Relationships between academic performance, SES school type and perceptual-motor skills in first grade South African learners:NW-CHILD study. Child: Care, Health and Development. 2013;40(3):370-378. doi: http://dx.doi.org/10.1111/cch.12059 [ Links ]
26. Beery KE (1997). The Beery-Buktenica Developmental Test of Visual-motor integration with Supplemental Developmental tests of visual perception and motor co-ordination Administration, Scoring and teaching manual (4th ed.). New Jersey: Modern Curriculum Press, Parsippany. [ Links ]
27. van Jaarsveld A, Vermaak M, van Rooyen C. The developmental status of street children in Potchefstroom, South Africa. South African Journal of Occupational Therapy. 2011; 41(1): 5-8. Available from: http://www.scielo.org.za/scielo.php?script=sci_arttext&pid=S2310-38332011000100003&lng=en. [ Links ]
28. Gretschel P, Ramugondo EL, Galvaan R. An introduction to Cultural Historical Activity Theory as a theoretical lens for understanding how occupational therapists design interventions for persons living in low-income conditions in South Africa. South African Journal of Occupational Therapy. 2015; 45(1): 51-55. doi: http://dx.doi.org/10.17159/2310-3833/2015/v45no1a9. [ Links ]
29. Department of Education. Curriculum and Assessment Policy Statements (CAPS). Pretoria, South Africa. 2011. [accessed 2022 October 06]. https://www.education.gov.za/Curriculum/CurriculumAssessmentPolicyStatements(CAPS).aspx [ Links ]
30. Case-Smith J, Richardson P & Schultz-Krohn W. An overview of occupational therapy for children. In J. Case-Smith (Eds.) 5th edition, Occupational therapy for children (pp. 2-29). Philadelphia: Elsevier Mosby. [ Links ]
31. IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corporation. [ Links ]
32. Laughton B, Cornell M, Kidd M, Springer PE, Dobbels EFM, Rensburg AJV, et al. Five year neurodevelopment outcomes of perinatally HIV-infected children on early limited or deferred continuous antiretroviral therapy. Journal of the International AIDS Society. 2018; 21(5). doi: http://dx.doi.org/10.1002/jia2.25106 [ Links ]
33. Schneck, C. Visual Perception. In: Case-Smith. J. Occupational Therapy for children (5th ed.). Missouri, USA: Elsevier, Mosby. 2005; 412-448. [ Links ]
34. Volman MJM, van Schendel BM, Jongmans MJ. Handwriting Difficulties in Primary School Children: A Search for Underlying Mechanisms. The American Journal of Occupational Therapy.2006; 60(4):451-60. doi: http://dx.doi.org/10.5014/ajot.60.4.451 [ Links ]
35. Morris LD, Grimmer KA, Twizeyemariya A, Coetzee M, Leibbrandt DC, Louw QA. Health system challenges affecting rehabilitation services in South Africa. Disability and Rehabilitation. 2019; 43(6):877-83. doi: http://dx.doi.org/10.1080/09638288.2019.1641851 [ Links ]
 Correspondence:
Correspondence:
Caraleigh Otto
caraleigh@nthandohome.co.za
Received: July 2022
Peer review: September 2022
Revised: December 2022
Accepted: March 2023
Published: August 2023
Editor: Blanche Pretorius: https://orcid.org/0000-0002-3543-0743
Funding: The first author received funding from the National Research Fund, South Africa, and the University of Cape Town Postgraduate Research Funding Centre to support her completion of her postgraduate studies.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}