










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.53 n.2 Pretoria Aug. 2023
http://dx.doi.org/10.17159/2310-3833/2023/vol53n2a2
RESEARCH ARTICLE
Occupational therapists' acceptance of 3D printing
Shelley Louise BarterI, III; Alexandra Jean WilliamsII, III; Gina RenckenIII; Nonjabulo NdabaIII; Pragashnie GovenderIII
IHillcrest Private Hospital, KwaZulu-Natal, South Africa. Shelley Louise Barter: https://orcid.org/0000-0002-3692-8519
IIEntabeni Rehabilitation Unit, KwaZulu-Natal, South Africa. Alexandra Jean Williams: https://orcid.org/0000-0002-8557-5860
IIIDiscipline of Occupational Therapy, School of Health Sciences, University of KwaZulu-Natal, Durban, South Africa. Gina Rencken: https://orcid.org/0000-0002-3658-4453; Nonjabulo Ndaba: https://orcid.org/0000-0002-8273-028X; Pragashnie Govender: https://orcid.org/0000-0003-3155-3743
ABSTRACT
INTRODUCTION: In occupational therapy, three-dimensional printing is being explored as an alternative design and manufacturing technique to the conventional fabrication of orthotics and assistive devices. The global applications and literature are rapidly growing, but the South African - specific literature is deficient. The Technology Acceptance Model depicts that one's perception of any particular technology is a significant determinant of their acceptance of it, determining whether the technology system is successfully adopted or disregarded
AIM: To determine the perceived acceptance of three-dimensional printing technology amongst occupational therapists in KwaZulu-Natal and whether exposure to the technology system, in the form of a three-dimensional printing workshop, influences their perception of the technology
METHOD: The study followed a multi-method design consisting of two phases; phase one involved the creation of the intervention tool (workshop), which was developed through a process guided by Design-Based Research. Phase two involved the implementation of the intervention and data collection. Therapists documented their perceptions in a questionnaire before and after exposure; following a pre and post-test design, enabling comparison. The questionnaires were based on the Technology Acceptance Model, including 13 questions scored on a seven-point Likert scale and five open-ended questions. The quantitative data were analysed descriptively, and qualitative data were analysed thematically
RESULTS: All four categories of the Technology Acceptance Model-based questionnaire displayed a significant change (p < 0.05) between the pre and post-test responses, with a medium effect size
CONCLUSION: Exposure to three-dimensional printing influences therapists' perception of the technology
IMPLICATIONS FOR PRACTICE
• The application of Three-Dimensional Printing (3DP) in occupational therapy practice has the potential to enable increased accuracy and precision of items fabricated by therapists; enabling customisation and individualisation to the exact specifications of a patient.
• 3DP can open doors to a broad spectrum of items that are not easily accessible, affordable, or not even available, accessing ideas and blueprints from a global pool of resources through open-source sites.
• With the process of fabrication being digital, not only does this reduce manual labour, but fabricating without touching the patient can reduce pain and prevent disruption of a repair/ surgical site/ wound.
• The digital process also allows patients to see and visualise the product during the design process, enabling input prior to printing, contributing to reduced wastage.
Keywords: Assistive Technology, Three-dimensional Printing (3dp), Technology Acceptance Model (tam), Additive Manufacturing, Orthosis, Splinting, Assistive Devices
INTRODUCTION
Three-Dimensional Printing (3DP), also known as additive manufacturing, is a type of manufacturing whereby items are fabricated in consecutive layers with guidance from a computer-aided design (CAD) file1. Until recently, 3DP technology remained largely inaccessible to the general public, dominated primarily by prominent stakeholders2. Today, the applications of 3DP have expanded to the general market, from the commercial and academic environments to clinical settings as well3.
The application of 3DP across healthcare domains is rapidly expanding, completely revolutionising traditional practices with the ability to create whilst ensuring personalisation, time efficiency and accuracy4-55 In occupational therapy practice specifically, 3DP is being explored as an alternative design and manufacturing technique to conventional processes within two areas of practice: assistive devices and splinting/ orthotics6. Technology may present hurdles to current practices; however, it also provides new opportunities for enhancing and enabling patient engagement and meaning in life. For this reason, it is recommended that therapists engage beyond their typical practices to advocate for their patients7.
Despite the rapid advancements in technology globally, acceptance and resultant use of advancements such as 3DP by individuals, in this case, occupational therapists, cannot be assumed and therefore, must be examined8. This study aimed to determine the perceived acceptance of 3DP technology by occupational therapists working in South Africa. The findings of this study are intended to provide a gateway to further research and advancements in occupational therapy practice and service delivery within the South African context.
LITERATURE REVIEW
The South African healthcare system and access to assistive technology
South Africa has a two-tiered healthcare system. The public sector is underfunded and services three-quarters of the population, whilst the private sector is grossly inaccessible to the majority due to the exorbitant cost of private care9. In South Africa, approximately 7.5% of the population lives with a disability10. Individuals living with disabilities require assistive technology (AT) that enables them to actively engage and complete a task that they would not otherwise be able to do11. Without access to the appropriate AT, an individual with a disability may be unable to access opportunities available to the able-bodied12. Equitable access for this population was documented in the South African National Development Plan (NDP)13, this service however is fragmented and inaccessible. The government cannot meet between 35% and 85% of the total AT needs of the disabled population12, and with the proposed implementation of National Health Insurance, the National Department of Health will be solely responsible for providing this essential service. The greatest challenge to provision of AT in South Africa is the financial constraints impacting on service delivery and availability of products. To bridge this gap, local innovation, product development, and manufacturing needs to be cultivated and supported12.
3DP in the field of occupational therapy
Within the field of occupational therapy, 3DP is being explored as an alternative design and manufacturing technique to the conventional fabrication of orthotics and assistive devices (both of which fall within the domain of AT)6. An orthosis is a device applied externally to a body part to provide structural positioning or functional facilitation, referred to as 'splints' in the South African context. Fabricating orthoses requires clinical experience and can be labour-intensive14. 3DP may significantly reduce the equipment and materials required in the fabrication process of an orthotic. 3DP orthoses have also proven to be of lighter weight, better ventilated and more aesthetically pleasing compared to traditional thermoplastic orthoses15. Assistive devices are any item that enables an individual with a disability to complete a task that they would not otherwise be able to do16. 3DP has proven to be an effective method for designing, testing, and manufacturing unique assistive devices. The process has yielded greater patient satisfaction, functionality, and reduced cost17.
Another advantage of 3DP is the availability of online open-source platforms. The digital blueprint designs are distributed and shared globally, with the end-user having the opportu nity to customise the desig n for the specific needs of each patient15. Additionally, a potential benefit of using CAD is the opportunity for patient feedback during the design process prior to fabrication. This would cultivate a sense of ownership and improve patient satisfaction and subsequent compliance14. Input and feedback during the design process would also reduce unnecessary waste of materials, as adjustments can be made digitally before printing.
The gap in 3DP Research in occupational therapy
Limited research examines 3DP within healthcare and occupational therapy internationally, specifically in South Africa. This may be a barrier to potential advancements in therapy and technology integration for future practice. The Technology Acceptance Model (TAM) was developed in 1985, due to concern that employees were not using the Information Technology (IT) advancements made available to them. The original TAM consists of two major components: perceived usefulness and perceived ease of use, with the latter directly influencing the former. The model depicts that these two perceptions will influence the user's attitude towards the technology system, which will influence whether the user will accept or reject the technology. The two beliefs are directly influenced by the characteristics of the technology itself8. The TAM has become a leading model in explaining and predicting the acceptance and use of technology18. Previous empirical research studies have tested the TAM, and proven that tools based on this model have yielded results considered to be statistically reliable19. This study included questionnaires based on the TAM to determine therapists' perceived acceptance 3DP technology based on the following: usefulness, ease of use, attitude towards, and intention to use in future practice.
METHODOLOGY
Study design
The study used a multi- method design consisting of two distinct phases, outlined in Figure 1.
Phase one: Intervention tool development
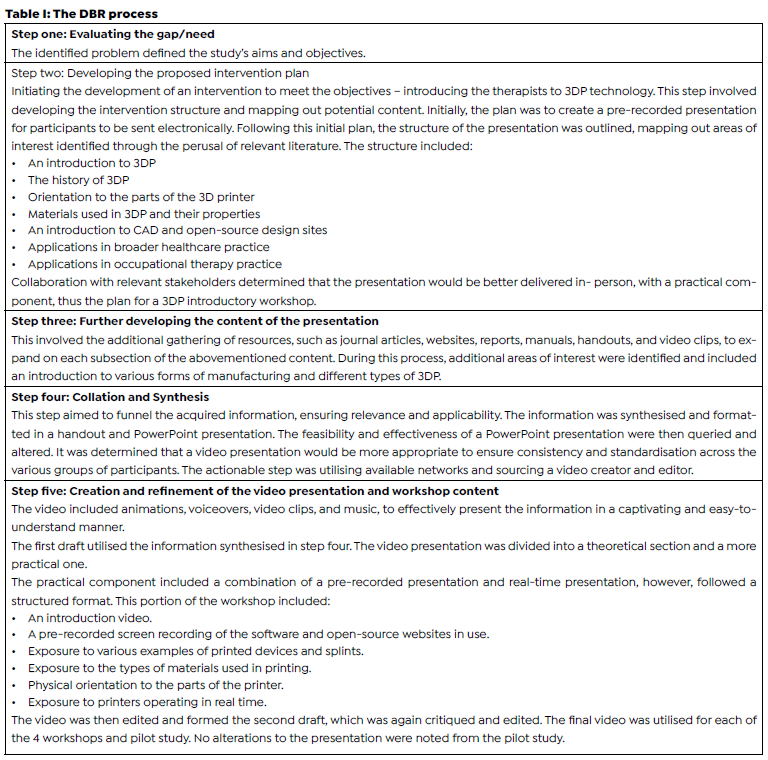
This phase was geared towards developing the intervention tool; the 3DP workshop and was guided by the Design-Based Research (DBR) process. The process begins with initially evaluating a problem within a specific context. Following this, a potential solution is designed - generally as an instructional tool. The researchers then test and develop the instructional tool through an iterative process, funnelling and refining the knowledge20.
This research process is appropriate when the knowledge related to the problem is particularly new and when instructional material is lacking21-23. The DBR process is not a precise research methodology but rather a team collaboration engaged in a process of systematically examining, constructing, and evaluating information and tools for learning22. The DBR team consists of any stakeholder or collaborator whose expertise and knowledge contribute to development within the iterative cycle21. This team consisted of five co-authors. Three collaborators were clinicians with experience and published work in the field of splinting and rehabilitation in occupational therapy, and the other two are clinicians practicing in the field of physical rehabilitation in occupational therapy, with prior 3DP experience.
Phase two: Data collection
Phase two was geared towards developing the data collection tool, conducting the pilot study, and running the 3DP workshops and data collection process. Four workshops were run to cater to therapists in different areas in KwaZulu-Natal.
Study design: The second phase followed a quasi-experimental design consisting of a one-group pre-test, post-test design. In this study, the dependent variable was the therapists' perceived acceptance of 3DP technology, which was assessed before and after participating in a 3DP introductory workshop (independent variable).
Setting: The study was located in KwaZulu-Natal, South Africa. South Africa has been described as both a developing and developed country, having high levels of inequality, juxtaposing wealthy neighbourhoods and poverty-stricken settlements24-26. South African healthcare expenditure aggregates to over R500 billion annually and is approximately evenly split between the public and private healthcare sectors, despite the former providing care for the large majority of the country27. Public facilities are, as a result, often overcrowded, have limited resources, long waiting times, and staff shortages26. A setting with two contrasting healthcare sectors required representation of both within the study.
The government is unable to meet a significant portion of the assistive technology needs within South Africa affecting the large majority accessing public healthcare, but in time also affecting the entire disabled population with the proposed implementation of National Health Insurance. One of the most significant challenges faced within this context, with the provision of products and services, is the financial constraints which directly impact resource availability, often resulting in extended waiting times. Waiting times of over two years have been reported, with devices no longer suitable to the patient's needs, size, environment, and life roles that have changed12.
Participant selection and sampling: Participants included practising occupational therapists in physical or paediatric rehabilitation in either the public or private healthcare sectors in KwaZulu-Natal. The database of the Occupational Therapy Association of South Africa (OTASA) was accessed to attain membership figures; however, membership with OTASA is not mandatory, and it is therefore expected that not all therapists are registered with the association.
Therefore, the total number of potential participants in the target population was consequently unknown. However, the number of public sector hospital departments invited to participate in the study was 28, and the number of private sector practices invited was approximately 50. In total, 40 therapists consented to participation and were involved in the study. Non-probability convenience sampling was utilised. Public sector therapists were accessed via the chairperson of the KZN provincial forum, who aided in the distribution of the invitation and detailed explanation of the research study via email to each department. Private practice therapists were invited via networking, occupational therapy messenger groups and practice searchers were conducted via the internet to extend the invitation.
Research tools: The study included a pre-test, post-test questionnaire based on the TAM. A portion of the questionnaire was obtained, with permission, from a previous study conducted in the United States of America that successfully developed a TAM-based questionnaire and utilised it to determine occupational therapy students' attitudes and perceptions of 3DP technology28. The questionnaire included 12 biographical questions; 13 questions based on the TAM (scored on a seven-point Likert scale ranging from one (totally disagree) to seven (totally agree), and ended with five open-ended questions. The biographical questions were to determine the therapists' experience in the field and with 3DP, their practice habits, and their age - creating an opportunity to generate further discussions of potential influences. The open-ended questions were developed by looking at the TAM categories, and were phrased to create space for further perspectives and opinions to provide depth to the first 13 questions scored on a Likert scale. The pre-test and post-test questionnaires were administered directly before and after the therapists participated in an introductory workshop.
Research procedure: Four workshops were conducted with four different groups of therapists. The workshops were held at various settings (a public hospital, a private hospital, a private practice, and at a tertiary institution's occupational therapy department). Locations were chosen based on ease of access for therapists living in the Pietermaritzburg area, the Upper Highway area, North Coast and Westville Central area, and therapists were given a choice as to which workshop to attend. The workshops were run by the researcher and a co-facilitator and attended by the research supervisors (all of whom comprise the collaborators involved in the DBR process that produced the workshop content). Each workshop was 2.5 hours in length (including arrival and refreshments). The workshops spanned several weeks. At the start of the workshop, therapists completed the pre-test questionnaire; they then engaged in the presentation and practical components of learning before completing the post-test questionnaire. Questionnaires were collected at the end of the workshop, each therapist's pre and post-test responses were stapled together, enabling direct comparison of changes in responses.
Data analysis: The quantitative data collected from the pre-and post-test questionnaires were captured on a Microsoft Excel spreadsheet and were prepared for analysis using the IBM Statistical Package for Social Sciences (SPSS, Version 24.0). The data were analysed descriptively and collated using frequencies and means. The pre and post-test results from the 13 TAM-related questions were scored according to the four categories of the TAM including perceived usefulness, perceived ease of use, attitude towards use and intention to use. Paired t-tests were used to analyse the responses and compare the mean measurement taken from the pre- and post-test response29. Cohen's d was then used to calculate the effect sizes between the pre- and post-test responses30. The results were interpreted according to small, medium, and large effect. Results were then collated for representation in tabular format. Non-parametric tests could have been used and suitable, given the small sample size; however, a parametric test is often more likely to detect a significant difference when it exists and therefore paired t-tests were used31. The demographic questions were grouped, translated into quantifiable data, and represented in tabular format. The five open-ended questions in the survey were grouped by question and captured onto Microsoft Word.
The data were manually coded and thematically analysed using a deductive approach. The themes were predetermined and utilised in analysing both the pre- and post-test responses: 1) Perceived usefulness of the technology in practice, 2) Perceived ease of use of the technology system, 3) Attitude towards 3DP and the incorporation of the technology in practice, 4) Perceived accessibility of the technology system. The TAM informed the first three themes, whilst the last theme was informed by the review of literature throughout the research process, in combination with the experiential insight of living in a developing context. The specific subthemes were not determined deductively and were determined through the review, grouping and analysis of responses from the five open-ended questions.
Scientific rigour
Trustworthiness was ensured through replicability, transferability, confirmability, and triangulation. The detailed documentation of the following ensured replicability: the participants, the data collection tools and methods, the data collection process, and data analysis. The detailed record keeping of each step of the process will enable each step to be accurately repeated32. Transferability was ensured by providing sufficient detailed description of the study, so that readers can determine for themselves whether the findings are applicable to themselves in their own context33. Confirmability was established as three authors were privy to the raw data, were involved in the data analysis, and reviewed the discussions and conclusions drawn from this. Triangulation was achieved by converging multiple data sources, and the findings from this study are available for review by other professionals and experts in the field, enabling analyst triangulation34.
Ethical considerations
Ethical clearance was obtained from the Biomedical Research Ethics Committee (BREC) prior to the commencement of the study (Reference number: BREC/00003938/2022). Gatekeeper permission was obtained from the Department of Health, for therapists working within the public sector (NHRD reference: KZ_202201_024). In order to ensure informed consent and confidentiality within the study, the following was ensured: Interested participants were provided with a written detailed description of the research purpose and process, prior to involvement in the study. Participants were informed of the research procedure, its purpose, possible risks and benefits, the selection process, the knowledge that they can withdraw from the study at any time, and additionally were given an opportunity to ask questions before accepting the invite to join the study. Throughout the research process, all information obtained from the data collection tools did not contain identifying data. 3D printers were used throughout this research study; the printers are the property of the University of KwaZulu-Natal, and permission to utilise the equipment as students was granted.
RESULTS
Quantitative results
Demographics
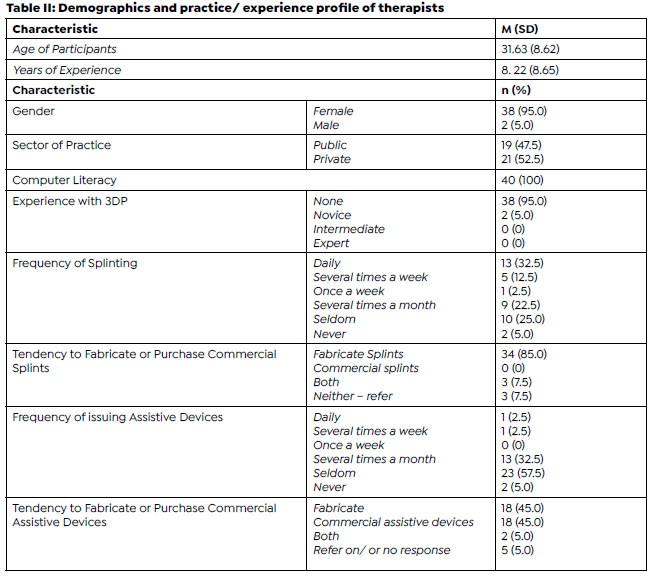
The demographic profile of the study participants is highlighted in Table II (above). The study included 40 occupational therapists, the majority of whom are females, with the age of the participants ranging from 22 to 54 years, (M = 31.63; SD = 8.62). The experience amongst the therapists ranged from 0 years (currently completing community service) to 33 years (M =8.22, SD = 8.65). The study comprised a nearly equal distribution of therapists working within the public (47.5%,) and private (52.5%,) healthcare sectors. All participants were computer literate, and 95% had no prior experience with 3DP. The therapist's practice profiles indicated the majority (32.5%) splinted daily, 22.5% splinted several times a month, and 25.0% seldomly splinted. 85.0% of therapists manually fabricate splints/ orthotics, rather than purchasing a commercial product. Assistive devices are seldom issued by 57.5% of therapists while 32.5% issue them several times a month. The tendency to fabricate (45%) or purchase commercial (45%) assistive devices was equally distributed amongst the therapists.
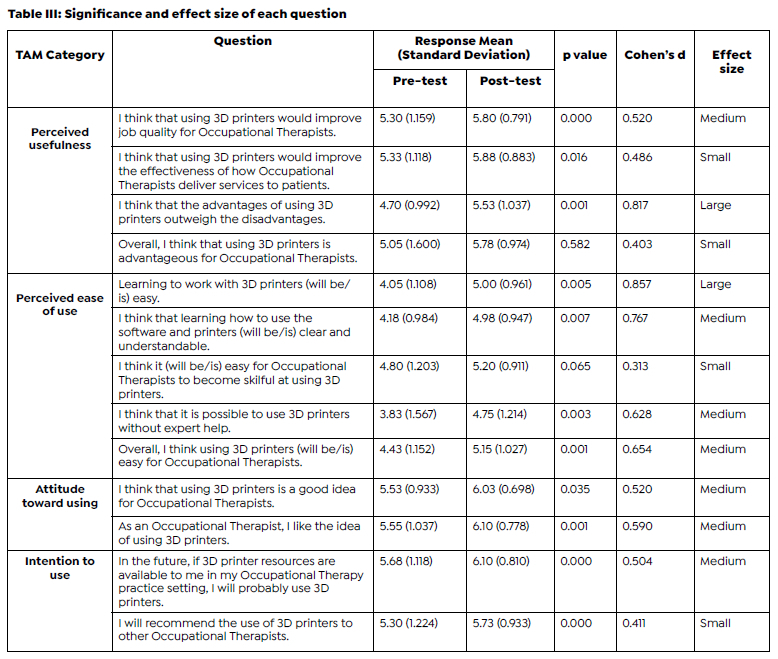
Table III (page 9) highlights the changes between the pre- and post-intervention responses. The questionnaires consisted of 13 questions across the four categories of the TAM. Of the 13 questions, 11 depicted a significant change (p < 0.05) between the pre- and post-test responses. In terms of the magnitude of change, four questions depicted a small effect size (0.2 > d< 0.5), 7 depicted a medium effect size (0.5 > d< 0.8), and 2 depicted a large effect size (d > 0.8). The effect size is the most significant outcome of empirical studies, as it depicts whether an intervention has caused an effect, and the magnitude of the effect35.
According to the TAM, the first three categories need to be favourable before the intention to use the technology is influenced.8 The categories, perceived usefulness, perceived ease of use, and attitude toward using all presented with a significant difference of p<0.05 from pre-test to post-test, and medium effect sizes between 0.5 to 0.7. Therefore, the fourth category, intention to use, would also depict a significant change when comparing the pre and post-test responses. The score difference for intention to use was highly significant (p= 0.0), but the medium effect size (d= 0.518) was the lowest for all categories, indicating a lower clinical change.
Qualitative Findings: Pre-test
Participants answered five open-ended questions relating to 3DP technology and integrating the technology system into practice, in the pre and post-test questionnaires. Table V (page 10) shows a summary of the themes.
Pre-test Theme 1: Perceived usefulness of the technology in practice
Advantages
Some participants perceived the technology as being useful for its applications in splinting and assistive device production. Their perceptions were geared towards the customisation and individualisation of splints and assistive devices. Precision, accuracy and reduced human error were noted. Participants acknowledged that 3DP may produce neater, more aesthetically pleasing end products and promote time-efficiency in the fabrication process of assistive devices when compared to manual fabrication or procurement. Despite previous concerns regarding the expense and financial outlay for 3DP, several participants noted that it may be cost-effective in the long run.
"Allows OTs to make splints without hurting a patient or disrupting a repair, it is neater/cleaner, reduces stress on OTs to be perfect. (P19 - 28yrs, public practitioner)
"Better cosmetic outcome; possibly lower profile designs." (P27 - 36yrs, private practitioner)
Disadvantages
Participants perceived the technology as being disadvantageous for two primary reasons; the extended time required to print items and the perceived inability to remould items. It was explicitly noted that a rapid turnaround time is essential in public settings with high patient loads. Participants also noted the concern regarding the ability to adjust and alter the items once printed, as in manual fabrication. The concern was centred around the need for alterations, specifically in the splinting process, to ensure comfort and to meet the patient's individualised needs with their specific condition/ diagnosis.


"I feel that the time it takes to print objects may be a challenge as you may not be able to issue a device on the spot." (P14 - 36yrs, public practitioner).
"Fabricating according to individual diagnosis/needs of patient /fit assists with comfort. Not sure if the 3D splint will be comfortable as it isn't individually moulded? Or is it?" (P24 - 31yrs, public practitioner).
Pre-test Theme 2: Perceived ease of use of the technology system
Simple/ easy
A minority of participants felt that operating the printer and its accompanying software would not be difficult despite the initial training requirement.
"Ease of use might prove to be less of a problem specifically regarding younger occupational therapists familiar with newer technology." (P39 - 23yrs, public practitioner).
Difficult/ requires expertise
The majority of participants perceived the technology as requiring expert training to operate. Many indicated that they felt the technology would be complex, require expertise, and be time-consuming to learn how to use proficiently.
"Probably needs a dedicated OT who can be consulted to assist." (P18 - 23yrs, private practitioner).
"Training and understanding of staff, e.g., maybe one staff is trained but when he/ she leaves there is no handover to the next therapist." (P28 - 35yrs, public practitioner).
Willingness to learn and adopt a new skill
The willingness of therapists to learn a new skill was also queried by several participants, noting that therapists may be resistant to change.
"New technology makes me slightly uneasy in terms of learning to use, therefore, I am sure others would be apprehensive but willing to learn to use it." (P21 - 31yrs, private practitioner).
Pre-test Theme 3: Attitude towards 3DP and the incorporation of the technology in practice
Novice
Many participants reported having limited to no prior knowledge or experience in 3DP technology, nor an understanding of how it works or could potentially be applied in practice settings. As a result of limited insight, several participants did not report strong opinions (or any opinion) of the technology system and waited until after the presentation to formulate an opinion.
"I have very limited understanding. I had not heard of this concept prior. I only knew of commercial splints and assistive devices." (P40 - 27yrs, public practitioner).
Advancements
Certain participants acknowledged the technological direction in which the world is advancing and felt that 3DP would be a useful resource with an application in occupational therapy practice. They expressed excitement and optimism towards incorporating the technology in practice, perceiving it as a tool to enhance therapists' skills and remain relevant.
"Think it should be part of therapeutic media in undergrad training. It's a no brainer." (P26 - 51yrs, private practitioner).
"Occupational therapists are usually old school and not trend setters. It is important to stay up to date with technology relevant to our field. To incorporate technology in order not to become outdated". (P27).
Traditional practice, fear of automation and loss of scope of practice
Several participants raised concerns about job security; fear of automation and other disciplines encroaching on occupational therapy practice. They also raised concern of extracting from core occupational therapy skill sets and specialities; affecting the therapeutic relationship with a patient, and removing the ability to be hands-on with a patient.
"I am concerned it may "rule out" the role of an OT in splinting as doctors may be able to 3D print splints themselves therefore reduce the no. of specialists required for an injury." (P31 - 27yrs, private practitioner).
Pre-test Theme 4 : Perceived accessibility of the technology system
Expense
A resounding perception of inaccessibility was evident, specifically due to the perception of the technology being highly costly to purchase. Participants noted that the technology would be especially inaccessible in the public healthcare sector, due to limited budgets and the structuring of the healthcare system.
"I feel it does have a place and can be very beneficial, however it is probably something that you might only see in a tertiary hospital or private setting and not in other settings." (P38 - 23yrs, public practitioner).
Context
Participants were concerned about the practicality and effectiveness of operating a 3D printer instead of manual labour. The technology requires electricity, which raises concerns within South Africa, as all are accustomed to regular power outages and load-shedding.
"In government settings we can barely access AFOs, wheelchairs, slings etcetera which are small things - the country does not eve n have electricity, so accessibility on technology within this setting is extremely limited". (P19).
Maintenance: updates, repairs, technical support, replacements
Repeatedly participants raised concerns regarding the practicality and feasibility of utilising a technology that will require maintenance, repairs, servicing and replacement of broken parts. Regular updating of the software programme to operate the system was also reported, with the above concerns further highlighted as significantly problematic in the public healthcare sector due to limited funding and resources.
"If it broke in the public sector, it wouldn't be serviced or repaired/replaced easily due to poor funding." (P24 -31yrs, public practitioner).
Qualitative Findings: Post-test
Following exposure to 3DP participants reported having a clearer understanding of what 3DP is, what the technology system entails, the printing process and the actual and potential applications for practice.
Post-test Theme 1: Perceived usefulness of the technology in practice
Advantages
Participants' perceptions were geared towards the technology being beneficial in ensuring accuracy and exact specifications, individualisation, and producing aesthetically pleasing, durable and lightweight items. Participants noted that the benefits listed would cultivate patient compliance and satisfaction. Notably, the participants perceived the technology as being far more beneficial in the production of assistive devices than splints, specifically due to the extended time requirements for printing and patients generally requiring splints to be fitted and issued immediately. Participants appreciated the allowance for creativity, creating a wide variety of items, and especially manufacturing items that are not usually easily accessible.
"It is a technology that our profession needs as we always make customised devices. Also beneficial to our patients who are more active and will require devices that will not limit them e.g. Weight." (P13 - 27yrs, public practitioner).
Disadvantages
Participants raised apprehension regarding the feasibility of using the 3D printer in practice due to the long print times, thus preventing fitting and issuing of splints and assistive devices during the session, delaying service delivery. Participants also noted, that even though open source design sites are available for use, they are not occupational therapy specific, and therefore may not be appropriate.
"I think it has its role. However, when you are making 12 splints in a day that need to be individualised with tight time constraints, I don't think the printer would be easy to use under pressure." (P24).
Post-test Theme 2: Perceived ease of use of the technology system
Simple/ easy
The majority of participants reported a changed perception in admitting that operating the printer and its software seemed far less complex and daunting than they initially thought. The participants agreed that training would be required but would be user-friendly and easy to grasp.
"More accessible and a lot easier to use than I thought it would be. Would now definitely consider buying one in the future." (P34 - 32yrs, private practitioner).
Difficult/ requires expertise
Several participants felt that the technology system would be difficult to grasp even with training. They concluded that the ease of use would depend on the individual therapist's skills and technological proficiency. Some participants specifically felt that the designing process would prove to be difficult in learning how to operate the software, and specifically due to the perceptual demands of the design process.
"I might struggle with CAD design as dimensions and shapes might get confusing." (P11 - 27yrs, private practitioner).
Driving force; passionate therapists to drive 3DP forwards in the profession
In their post-test responses, a few participants expressed the need for several therapists to take ownership and take charge of this potential 'field' to drive the process and avail themselves as consultants.
"Need to actually have OTs working at designing and testing. Need OTs to actually put in the effort with development in order for it to be used successfully in the general OT practice/ setting in RSA." (P18).
Post-test Theme 3: Attitude towards 3DP and the incorporation of the technology in practice
Advancements
The majority of participants expressed excitement at the possibility of incorporating 3DP into practice, growing and evolving as a profession with technology. They viewed the technology system as something innovative with broad applications that will enhance intervention and complement the skills occupational therapists are equipped with.
"Wow - the possibilities are endless!' Really, really interested! Can't believe all the options available." (P28). "The need for more education and research is apparent and I think it should be encouraged to help keep OTs on the forefront." (P36 - 36yrs, private practitioner).
Traditional practice and concern regarding gatekeeping
Several participants still raised concerns about job security. However, this time more also raised concerns about the technology, and specifically open-source platforms being available to other professions and the public - enabling anyone to print aids and splints, posing a serious safety concern as clinical reasoning will not be applied.
"The disadvantage is that there is no clear sort of gatekeeping to protect our role and clearly define OTs as key fabricators for assistive devices and splints, if the software can be used by anyone, which impacts our role in device/ splint fabrication." (P40).
Post-test Theme 4: Perceived accessibility of the technology system
Expense
Many participants admitted that the cost and accessibility were far less of a barrier than they assumed. Although an initial outlay is required to purchase the printer, they felt that it would result in cost-effectiveness in the long run as the materials are inexpensive.
"More positive about the prospect now, the financial implications are not as daunting and the fact that open source provides so many options is encouraging." (P36).
Several participants expressed that the cost of the technology system would still be a barrier and result in reduced accessibility. Specifically, in the public sector, the outlay of finances for a printer would not take priority considering the lack of resources.
"The accessibility problems within our context would still limit what types of facilities could use this technology." (P38).
Context
Participants perceived load-shedding and limited internet access in some areas as problematic, as electricity is required to operate the printer and the internet is necessary in utilising open-source sites or computer-aided design software.
"Loadshedding is a nightmare! But we have generators in our hospital so that wouldn't be a problem for me personally." (P28).
Maintenance
Maintenance concerns did not surface as frequently compared to the pre-test responses. However, participants still raised concerns regarding repair, troubleshooting, technological support, and upgrading the technology system.
"Technology becomes quickly outdated- constant need to upgrade printer." (P5 - 37yrs, public practitioner).
DISCUSSION
Within the field of occupational therapy, the global literature and applications of 3DP in practice are rapidly growing, revealing a paucity of South African-specific literature. This study, which is the first to the author's knowledge, aimed to determine the perceived acceptance of 3DP technology by occupational therapists, and to further determine whether the therapists' perception of the technology would be altered from exposure to the technology in the form of an introductory workshop.
A total of 40 therapists participated in the study, including male and female participants, with the age range spanning from 22 to 54 years, and their years of experience ranging from 0 years (currently completing community service) to 33 years. There was a balanced representation of therapists working in public and private practice. Therapists that were a part of the research study attended a 3DP workshop and completed a questionnaire based on the Technology Acceptance Model (TAM), before and after exposure to the technology during the workshop. The TAM portrays that a user's attitude towards a technology system is a pivotal determinant of whether the user will accept or reject the technology. The attitude is influenced by two crucial factors, 'perceived usefulness' and 'perceived ease of use'8. In addition to the categories of the original TAM, an additional dominant influential factor emerged; 'perceived accessibility'.
Perceived usefulness
Perceived usefulness is the extent to which an individual believes that their performance or role would be enhanced by using a specific technology19. The therapists held the perception that the technology cultivates therapist creativity, enables the broad creation of items, customisation, precision, reduced human error, and creation of an end product that is aesthetically pleasing; both prior to and post-exposure to the technology. However, although the therapists had positive perceptions of the technology prior to exposure, it was noted that the positive perceptions increased following exposure. Exposure to the technology caused a medium effect size, further solidifying their original perception of the usefulness of the technology system. A significant difference, however, between the pre- and postexposure perception of usefulness was that most therapists felt that the technology would be better suited to producing assistive devices, rather than splints. Many of the therapists' splint on a daily/ weekly basis (47.5%). Unlike assistive devices with the primary goal of aiding function, splints can also be prescribed as an adjunct to medical intervention; they can be used to stabilise, immobilise and prevent injury or deformity36. As a result, a splint is generally issued within the session. For this reason, many therapists perceived the technology as inappropriate as a means of splint fabrication because 3DP can require extended printing times. An article by Willet37 states that the printer's type or specification will also determine its use. For example, there are entry level, hobbyist, enthusiast, professional, and industrial-level printers, which will vary in printing speed, quality of printing and complexity. Printing times depend on the print settings, for example; print density, layer height, and the requirement for structural support. Therefore, suitability is more so task and item-specific.
Perceived ease of use
Perceived ease of use can be described as the degree to which an individual is of the opinion that using/ operating a specific technology system would not require significant mental effort or physical exertion19. Perceived ease of use was explored by looking at whether therapists perceived the technology system (hardware and software) as easy to learn, whether they felt they could become proficient and skilful in using the technology, and whether they believed it would require expert training. This category displayed a medium effect size between pre and post-test responses. However, of significance was the large effect size in the change of perception as to whether the therapists perceived that learning to operate the technology proficiently would be easy. Initially, most therapists perceived the technology as requiring expert training, knowledge, and skill to operate. After exposure to the technology, there was a significant shift towards perceiving proficiency as attainable and within reach. Existing literature examining individuals' perceptions of ease of use of technology, shows that an individual's perceptions significantly depend on their perceived general technology self-efficacy38. Self-efficacy is a person's belief in his/ her capability to perform a particular task successfully and is one of the most powerful volitional predictors of how well a person performs39. Computer self-efficacy refers to one's confidence in learning, understanding and proficiently operating a new technology40. Research has shown that an individual's technological self-efficacy is a significant determinant of perceived ease of use38. All of the participants had minimal to no prior experience or knowledge of 3DP, after exposure, however, their perception of their ability to navigate and operate the technology was altered. These findings are validated by Research that has found that increased insight into a technology system correlates with reduced technology-related anxiety and increased interest in the technology41.
Attitude
In the study, 38 of the 40 participants reported no prior experience with 3DP and two reported that they were novices. As a result, having limited to no prior knowledge or experience in 3DP technology, nor an understanding of how it works or could potentially be applied in practice settings, many therapists did not initially report strong opinions/ feelings (or any opinion/ feeling) towards the technology system. However, despite their lack of experience, others formulated an opinion and acknowledged the technological direction in which the world is advancing and felt that 3DP might be a useful resource in occupational therapy practice. Following exposure to the technology system, therapists reported having a clearer understanding of what 3DP is, what the technology system entails, the printing process and the actual and potential applications in practice. Afterwards, most therapists expressed positivity towards the technology system (not discounting their concerns), viewing it as something innovative with broad applications that will enhance intervention and complement the skills occupational therapists' are already equipped with. These findings corroborate with a study by Holzinger, Searle, and Wernbacher42, where they depicted acceptance based on previous exposure to a technology system.
Several therapists raised concerns centred around job security, specifically due to the concern of automation. However, in an Oxford University study43, 702 common occupations were examined, and their risk of automation was analysed and compared. Occupational therapy only scored 0.35% risk of automatic. Despite continual technological advancements, occupational therapy is not at risk of automation as it requires continual creativity, complex relational interactions and is highly unpredictable and vast. Technology can however change how therapists provide services7. A frequent concern was centred around losing or extracting from core occupational therapy skill sets and specialities; worrying that using a technology system instead of hands-on labour might affect the therapeutic relationship with the patient. An additional concern was centred around the open-source platforms. It was admitted that open-source platforms would prove to be highly advantageous in providing a global sharing of designs and knowledge; however, these resources would also be accessible to other professions and the general public. This raised the concern of other healthcare disciplines encroaching on occupational therapy practice, but even more so the concern of the general public accessing open-source sites, posing a serious safety risk because clinical reasoning would not be applied. These concerns corroborate with an article by Vogels, Rainie, and Anderson44, which unpacks the uses of technology. The article states that the determinant of technology's impact, is how technology is used, who uses it, and what it is used for. Technology can be highly advantageous as easily as it can be detrimental to society; it depends entirely on the user.
Perceived accessibility
External variables are essentially a variety of variables that are expected to influence users' technology acceptance and adoption. These factors include environmental factors, political factors, personal characteristics, organisational factors, etcetera45. External variables emerged as a dominant feature, specifically accessibility and feasibility within the South African context. Initially, the majority therapists perceived the technology as being 'out of reach,' and financially inaccessible. Post-exposure, majority of therapists reported that the technology was far more financially accessible than they initially thought, and more accessible in the south African context than they originally thought. The feasibility, however, of procuring a printer in the public healthcare system was still raised as an apprehension due to the financial and resource constraints within the system.
Additionally, what did not change was the queried feasibility of the technology; using a system that requires electricity to perform an essential service in a country accustomed to frequent power outages. Eskom is South Africa's dominant electricity supplier but is frequently unable to meet the electrical demands of the country, resulting in the implementation of 'Loadshedding,' a staged approach to power outages with the purpose of conservation. While private facilities and frequently secondary/ tertiary-level public hospitals are equipped with generators, smaller hospitals and clinics are often left in the dark46.
CONCLUSION
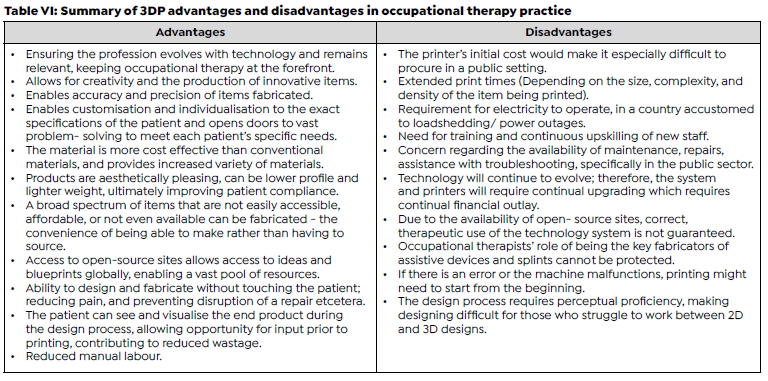
The study's findings reveal that engaging therapists in a workshop introducing them to the concept of 3DP at an introductory level, brings about a change in the therapists' perception of the technology system. Exposure to 3DP resulted in improved perception of the technology's usefulness, ease of use and attitude towards it, impacting their reported intention to use the technology in future practice. Table VI (page 16) shows a summary of the advantages and disadvantages of 3DP in occupational therapy practice.
Apprehensions
Open source sites and technology system use cannot be monitored or controlled. This is true with everything. In an article by Vogels et al44, the benefits and risks of technology advancements are discussed; what was noted is that from the beginning of time advancements have been two-fold. Fire, for example, can be used to cook just as easily as it can be used for destruction. The same is true for technology, it is neither inherently good nor bad, but entirely dependent on the user and how it is wielded. The occupational therapist's role is to ensure it is wielded for good. Several therapists have raised concerns about other disciplines encroaching on occupational therapy practice. However, despite the vast advancements in 3DP globally, South Africa is still at the exploratory phase, the profession therefore has the opportunity to take ownership and run with it, enabling the profession to evolve with technology and remain relevant, keeping occupational therapy at the forefront.
Recommendations
If the barriers to clinician uptake are overcome, the negative perceptions towards 3DP technology in occupational therapy practice may be mitigated, resulting in easier uptake and utility. The following recommendations would aid clinician uptake and overcoming of certain barriers.
3DP workshops
It is recommended that beginner, intermediate and advanced 3DP training courses are initiated, enabling upskilling of therapists. The courses should be geared towards incorporating theory and practice, enabling practical skills training.
Partnership and mentorship
It would benefit healthcare professionals to extend themselves beyond working in silos, and instead share resources, experience, and knowledge in 3DP. 3DP 'hubs' can be created for the sharing of resources. Smaller, poorly resourced clinics and hospitals should partner with better-resourced tertiary hospitals, and private practitioners should group together, pooling resources. To note, private and tertiary hospitals are equipped with generators46. Key therapists should be appointed as the point of call within each district, enabling mentorship and guidance.
Partnership with engineers utilising 3DP would be beneficial to enhance the applications and use of the technology system and guide troubleshooting, repairs, and maintenance.
Education
3DP should be incorporated into the occupational therapy undergraduate curriculum, together with continued studies on evolving technological advancements, ensuring the professions continual advancement is stimulated at a foundational level.
Resource pool
Occupational therapists need to be designing and uploading products onto open source sites such as Thingiverse, thus growing the profession-specific pool of resources.
During courses, therapists should be engaged in case studies that require practical designing of items, these can then be saved and uploaded to open source sites, contributing to resources.
Job security and conventional practices
As a profession, occupational therapists can also vouch for policy implementation, protecting the role of assistive devices and splint fabrication.
To combat the concern of extracting from core occupational therapy skill sets and specialities, coursework should include practical patient care, utilising the technology. This would enable therapists to determine whether the therapeutic relationship with a patient is affected due to the incorporation of the technology, and provide practice in navigating a new dynamic.
Limitations
Limitations to the study are multi-faceted. Firstly, the sample of participants was limited due to accessibility. For therapists to participate in the study they had to attend the in-person workshop, which limited the number of therapists as most of the therapists who did attend live in and around the eThekwini and uMgungundlovu districts, where the workshops were held. Secondly, the sample was also further limited by therapist's availability and willingness to participate in a two-hour in-person workshop. Although lack of interest cannot be assumed, the limited response and enthusiasm for the topic of 3DP may be indicative of such. Lastly, although the study is striving to ensure generalisability through the sample accurately portraying the population it represents, the study is limited to KwaZulu-Natal and therefore inevitably, it cannot be assumed that it will accurately represent the population outside of this region.
Author Contributions
Shelley Louise Barter was a Masters of Occupational Therapy student who contributed to the design, and was involved in the data collection, data analysis and writing up of this study. Alexander Jean Williams (Masters of Occupational Therapy candidate) and Pragashnie Govender were involved in the initial conceptualisation of the larger study on 3DP. Alexander Jean Williams assisted in the data collection for this study. Pragashnie Govender, Gina Rencken and Nonjabulo Ndaba were supervisors of the study and contributed to the design, provided supervision during the data collection process, and provided critique of the manuscript and assisted in revision of the manuscript for publication.
Conflicts of Interest
The authors have no conflict of interest to declare.
Acknowledgement
The authors would like to acknowledge Dr MO Ogunlana fo his assistance in the quantitative data analysis
REFERENCES
1. Ishengoma FR, Mtaho AB. 3D printing: developing countries perspectives. International Journal of Computer Applications. 2014;104(11):30-4. doi: https://doi.org/10.5120/18249-9329 [ Links ]
2. Matias E, Rao B. 3D Printing: on its historical evolution and the implications for business. Portland International Conference on Management of Engineering and Technology (PICMET). 2015; (15)551-8. doi: https://doi.org/10.1109/picmet.2015.7273052 [ Links ]
3. Fitzpatrick A. Design of a patient specific 3D printed arm cast. KnE Engineering. 2017;2(2): 135-42. doi: https://doi.org/10.18502/keg.v2i2.607 [ Links ]
4. Dodziuk H. Applications of 3D printing in healthcare. Polish Journal of Cardio-thoracic Surgery. 2016;13(3):283-93. doi: https://doi.org/10.5114/kitp.2016.62625 [ Links ]
5. Yan Q, Dong H, Su J, Han J, Song B, Wei Q, et al. A review of 3D printing technology for medical applications. Engineering. 2018;4(5):729-42. doi: https://doi.org/10.1016/j.eng.2018.07.021 [ Links ]
6. Paterson A, Donnison E, Bibb R, Campbell I. Computer aided design to support fabrication of wrist splints using 3D printing: a feasibility study. Hand Therapy. 2014;19(4):102-13. doi: https://doi.org/10.1177/1758998314544802 [ Links ]
7. Liu L. Occupational therapy in the fourth industrial revolution. Canadian Journal of Occupational Therapy. 2018;85(4):272-83. doi: https://doi.org/10.1177/0008417418815179 [ Links ]
8. Chuttur M. Overview of the Technology Acceptance Model: origins, developments and future directions. Sprouts: Working Papers on Information Systems. 2009;9(37):1-22 [ Links ]
9. Rensburg R. Healthcare in South Africa: how inequity is contributing to inefficiency. The Conversation Africa, Inc. 2021 [accessed 2022 Nov]. https://theconversation.com/healthcare-in-south-africa-how-inequity-is-contributing-to-inefficiency-163753#:~:text=South%20Africa%20has%20a%20two-tiered%2C%20and%20highly%20-unequal%2C,insurance%2C%20and%20serves%20around%2027%25%20of%20the%20population. [ Links ]
10. Jejelaye A, Maseko L, Franzsen D. Occupational therapy services and perception of integration of these at primary healthcare level in South Africa. South African Journal of Occupational Therapy. 2019;49(3):46-53. doi: https://doi.org/10.17159/2310-3833/2019/vol49n3a8 [ Links ]
11. Buehler E, Branham S, Ali A, Chang JJ, Hofmann MK, Hurst A, Kane SK. Sharing is caring: assistive technology designs on Thingiverse. Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems. 2015;525-34. doi: https://doi.org/10.1145/2702123.2702525 [ Links ]
12. Visagie S, Scheffler E, Seymour N, Mji G. Assistive Technology Service Delivery in South Africa: Conceptualising a Systems Approach. South African Health Review. 2020;(1)120- 7. doi: https://journals.co.za/doi/abs/10.10520/ejc-healthr-v2020-n1-a15 [ Links ]
13. OECD. National Development Plan 2030: Our future-make it work. Executive Summary. 2012 [accessed 2022 October]. https://www.gov.za/sites/default/files/gcis_document/201409/ndp-2030-our-future-make-it-workr.pdf. [ Links ]
14. Hale L, Linley E, Kalaskar D. A digital workflow for design and fabrictaion of bespoke orthoses using 3D scanning and 3D printing, a patient- based case study. Scientific Reports. 2020;10(1). doi: https://doi.org/10.1038/s41598-020-63937-1 [ Links ]
15. Li J, Tanaka H. Rapid Customization system for 3D-printed splint using programmable modeling technique - a practical approach. 3D Printing in Medicine. 2018;4(1):5 doi: https://doi.org/10.1186/s41205-018-0027-6 [ Links ]
16. Davis CP. MedicineNet. 2021 [accessed 2022 October]. https://www.medicinenet.com/assistive_device/definition.htm. [ Links ]
17. Day SJ, Riley SP. Utilising three-dimensional printing techniques when providing unique assistive devices: a case report. Prosthetics & Orthotics International. 2018;42(1):45-9. doi: https://doi.org/10.1177/0309364617741776 [ Links ]
18. Lee Y, Kozar KA, Larsen KRT. The Technology Acceptance Model: Past, Present, and Future. Communications of the Association for Information Systems. 2003;2:752-80. doi: https://doi.org/10.17705/1CAIS.01250 [ Links ]
19. Chen SC, Li SH, Li CY. Recent related Research in Technology Acceptance Model: a literature review. Australian Journal of Business Management and Research. 2011;1(9): 124-7. doi: https://doi.org/10.52283/nswrca.ajbmr.20110109a14 [ Links ]
20. Vaezi H, Moonaghi HK, Golbaf R. Design-Based Research: definition, characteristics, application and challenges. Journal of Education in Black Sea Region. 2019;5(1):26-35. doi: https://doi.org/10.31578/jebs.v5i1.185 [ Links ]
21. Scott EE, Wenderoth MP, Doherty JH. Design-Based Research: a methodology to extend and enrich biology education. CBE-Life Sciences Education. 2020;19(3):1-12. doi: https://doi.org/10.1187/cbe.19-11-0245 [ Links ]
22. Ford C, McNally D, Ford K. Using Design- Based Research in higher education innovation. Online Learning. 2017;21(3):50-67. doi: https://doi.org/10.24059/olj.v21i3.1232 [ Links ]
23. Armstrong M, Dopp C, Welsh J. Students' guide to learning design and Research. 2018 [accessed 2022 October]. https://edtechbooks.org/studentguide [ Links ]
24. Naumann E. Perspectives on Africa's trade and integration. TralacBlog. 2020 [accessed 2022 October]. https://www.tralac.org/blog/article/14567-south-africa-s-new-status-as-a-developed-country-for-purposes-of-united-states-subsidies-and-countervailing-duty-investigations.html. [ Links ]
25. The World Bank Group. The World Bank in South Africa. 2021 [accessed 2022 October]. https://www.worldbank.org/en/country/southafrica/overview [ Links ]
26. Young M. Western Michigan University - Scholarworks@WMU. 2016 [accessed 2022 November]. https://scholarworks.wmich.edu/honors_theses/2741. [ Links ]
27. Phillips G. Who owns whom. Africa Business Information. 2022 [accessed 2022 November]. https://www.whoownswhom.co.za/report-store/healthcare-sector-south-africa-2022/. [ Links ]
28. Benham S, San S. Student technology acceptance of 3D printing in occupational therapy education. American Journal of Occupational Therapy. 2020;74(3):1-7. doi: https://doi.org/10.5014/ajot.2020.035402 [ Links ]
29. Shek DT, Zhu X. Pretest-posttest designs. In B. Frey (Ed.), The SAGE EncyclopediaEncyclopedia of Educational Research, Measurement, and Evaluation. SAGE Publications, Inc. 2018:1293-5 doi: https://dx.doi.org/10.4135/9781506326139.n538 [ Links ]
30. Piasta SB, Justice IM. Encyclopedia of Research Design. Salkind NJ, editor. SAGE Publications, Inc; 2010.181-85. doi: https://dx.doi.org/10.4135/9781412961288 [ Links ]
31. Campbell MJ, Swinscow TDV. Statistics at Square One. Wiley-Blackwell: BMJ. 2009; 11th(Ed). [ Links ]
32. Miceli S. Reproducibility and Replicability in Research. The National Academies In Focus, 2019 [accessed 2022 November]. https://www.nationalacademies.org/news/2019/09/reproducibility-and-replicability-in-research#:~:text=Replicability%20means%20obtaining%20consistent%20results,about%20replicability%20are%20more-%20nuanced. [ Links ]
33. Brown JD. Characteristics of sound quantitative Research. Shiken. 2015;19(2):24-8. [ Links ]
34. Patton MQ. Qualitative Research & Evaluation Methods: Integrating Theory and Practice. 4th edition. California: SAGE Publications, Inc; 2015. [ Links ]
35. Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Frontiers in Psychology. 2013;4(863):1-12. doi: https://doi.org/10.3389/fpsyg.2013.00863 [ Links ]
36. Egan M, Brosseau L, Farmer M, Ouimet M, Rees S, Tugwell P, et al. Splints and Orthosis for treating rheumatoid arthritis. Cochrane Database of Systematic Reviews. 2001;2010(7):1-5 . doi: https://doi.org/10.1002/14651858.cd004018 [ Links ]
37. Willett AK, 3D Printing and Occupational Therapy: The Process of 3D Printing Adaptive Devices. Eastern Kentucky University, Department of Occupational Science and Occupational Therapy. Honors Theses. 2019;654. https://encompass.eku.edu/honors_theses/654 [ Links ]
38. Venkatesh V, Davis FD. A Model of the antecedents of percieved ease of use: development and test. A Journal of the Decision Sciences Institute. 1996;27(3):451-81. doi: https://doi.org/10.1111/j.1540-5915.1996.tb00860.x [ Links ]
39. Heslin PA, Klehe UC. Self- Efficacy. In S. G. Rogelberg (Ed.), Encyclopedia of Industrial and Organizational Psychology. 2006;(2):705-8. [ Links ]
40. Compeau D, Higgins C. Computer self-efficacy: development of a measure and initial test. MIS Quarterly. 1995;19(2):189-211. doi: https://doi.org/10.2307/249688 [ Links ]
41. Czaja SJ, Charness N, Fisk AD, Hertzog C, Nair SN, Rogers WA, et al. Factors Predicting the Use of Technology: Findings From the Center for Research and Education on Aging and Technology Enhancement (CREATE). Psychology and Aging. 2006;21(2):333-52. doi: https://doi.org/10.1037/0882-7974.21.2.333 [ Links ]
42. Holzinger A, Searle G, Wernbacher M. The effect of previous exposure to technology on acceptance and its importance in usability and accessibility engineering. Universal Access in the Information Society. 2011;10(3):245-60. doi: https://doi.org/10.1007/s10209-010-0212-x [ Links ]
43. Frey CB, Osborne MA. The future of employment: how susceptible are jobs to computerisation? Technological Forecasting and Social Change. 2013;114:254-80. doi: https://doi.org/10.1016/j.techfore.2016.08.019 [ Links ]
44. Vogels EA, Rainie L, Anderson J. Experts predict more digital innovation by 2030 aimed at enhancing democracy. Pew Research Center. 2020. Report No:ED609129:133 [ Links ]
45. Holden H, Roy R. Understanding the influence of perceived usability and technology self-efficacy on teachers' technology acceptance. Journal of Research on Technology in Education. 2011;43(4):343-67. doi: https://doi.org/10.1080/15391523.2011.10782576 [ Links ]
46. Laher AE, Van Aardt BJ, Craythorne AD, Van Welie M, Malinga DM, Madi S. 'Getting out of the dark': implications of load shedding on healthcare in South Africa and strategies to enhance preparedness. South African Medical Journal. 2019;109(12):899-901. doi: https://doi.org/10.7196/samj.2019.v109i12.14322 [ Links ]
 Correspondence:
Correspondence:
Pragashnie Govender
naidoopg@ukzn.ac.za
Submitted: December 2022
Reviewed: April 2023
Revised: April 2023
Accepted: April 2023
Published: August 2023
Editor: Hester Van Biljon: https://orcid.org/0000-0003-4433-6457
Funding: The First Author, Shelley Louise Barter, Received Tuition Remission Towards The Study From Which This Paper Emanates.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}