










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.53 no.1 Pretoria Abr. 2023
http://dx.doi.org/10.17159/2310-3833/2023/vol53n1a11
RESEARCH ARTICLE
Occupational therapy rehabilitation managers' perspectives on community integration of persons with spinal cord injuries in Nairobi, Kenya
Evans Obara ObaigwaI, III; Catharina Jacoba Elizabeth UysII; Pragashnie GovenderI
IUniversity of KwaZulu-Natal, South Africa. Evans Obara Obaigwa: https://orcid.org/0000-0001-9742-6005; Pragashnie Govender: https://orcid.org/0000-0003-3155-3743
IIUniversity of Pretoria, South Africa. https://orcid.org/0000-0001-9722-9941
IIIPresbyterian University of East Africa: Kikuyu, Central, Kenya
ABSTRACT
INTRODUCTION: Spinal cord injuries (SCI) present complex clinical challenges requiring comprehensive rehabilitation management to facilitate adequate community reintegration. Rehabilitation managers are suitably positioned to enforce and enact policy related to holistic rehabilitation intervention, including preparing patients for community integration. However, due to discrepancies within the chain of care systems, they are unable to ensure individuals with SCI in Kenya are discharged to their respective communities fully prepared for effective community integration. Exploring their perspectives may therefore highlight potential barriers or enablers to ensuring more effective community integration for survivors of SCIs
METHODS: A qualitative, descriptive study was conducted via individual interviews with 12 purposively sampled rehabilitation managers. Data were audio-recorded and transcribed and underwent content analysis
FINDINGS: The study findings revealed inadequacies in the process of spear-heading and facilitating community integration of individuals that sustained a spinal cord injury. On the other hand, the study suggested possible strategies to reinforce community integration for individuals with spinal cord injuries by involving all stakeholders in decision making, addressing training gaps, facilitating research programmes and equipping rehabilitation centres with specialised spinal cord units
CONCLUSIONS: Implementing disability policies to minimise barriers to community integration and access to essential services is required. This includes developing clear guidelines on comprehensively managing individuals with spinal cord injuries in the community within the Kenyan context
Implications for practice
• Occupational therapy managers have a role to play in the facilitation of empowerment strategies aimed at influencing community (re) integration of survivors of SCIs.
• There is the need for the enactment of an effective rehabilitation framework to enforce the role of occupational therapists as a key role player in facilitating community (re) integration.
• Goodwill is required from the governmental political systems and organisations to spearhead the enforcement of the existing disability legislation if the welfare of survivors of SCIs are to be achieved.
Keywords: disability policies, access to essential services, spinal cord units, rehabilitation centres, chain of care system
INTRODUCTION
Spinal cord injuries (SCI) present complex clinical challenges, requiring comprehensive rehabilitation and adequate support to allow community reintegration1,2. In Sub-Saharan Africa (SSA), persons with SCI who survive their initial injury face difficulty and irreversible challenges accompanied by preventable complications and may finally die in the community due to low quality of care, unfriendly environments and lack of opportunities to participate in community activities3.
Interestingly, the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) articulates how survivors of SCI should be perceived in the global community through the lens of human rights and developmental levels3. In fact, among other concepts emphasised by the UNCRPD is community integration, an element strongly advocated for, to benefit survivors of SCIs3,4. Following discharge to the community, successful community integration is indirectly influenced by the hospital policies that support the preparation of these individuals for community integration by healthcare professionals training and interventional mechanisms within the hospital setting5,6. On the other hand, the macrosystem, which consists of the broader environmental systems surrounding these individuals like the political system and their policies, cultural and existing environment beliefs, will either facilitate or hinder the prospects of these individuals' involvement in community activities. These challenges may occur over a period of time, affecting the transition from a healthy individual to surviving an SCI disability throughout the rest of their life. This considers that the interaction with their respective environments will also be changing6,7. In this manner, the success of survivors of SCI community integration depends on several factors: the individual with SCI and society's readiness and willingness to accommodate and accept these individuals through available and implementable mechanisms3.
Globally, countries have been utilising domestic laws in matters related to disabilities which facilitated inconsistencies in how persons with disabilities are viewed8. The UNCRPD changed this type of discourse internationally by emphasising that state parties should facilitate the acceptance of persons with disabilities, including those with SCI, and provide an enabling environment for their full and effective participation in the community like any other member of the society. The enabling environment also includes access to all essential services3,9.
However, Kovacs and Gordon10 argue that access to essential services will not be achieved if community perceptions and practices towards persons with disabilities are not influenced by proper legislation and related policies geared towards facilitating this accessibility. These discrepancies can be noted in the Canadian Human Rights Act, which covers issues of comprehensive accessibility for all persons and not specifically to persons with disabilities. It is instead left to every province to implement disability policies10. In contrast, in Australia, unlike in Canada, one of the successes of disability policy is due to both national and local governments working concurrently on the issue of persons with disabilities11. The European Union (EU) likewise ratified the UNCRPD by encouraging the member states to acknowledge the environment as a contributing factor in allowing persons with disabilities, including those with SCI, to be fully involved in activities in their community4. Nakagawa and Blanck12 found that although UNCRPD ratified Japan's anti-discriminatory law, their laws mostly borrow from ideas in the medical model, which does not comprehensively address the environmental contribution as far as a person with disabilities community integration is concerned.
The implementation of disability legislation is also dependent on government political systems and organisation, which further determine the effectiveness of the response towards the welfare of persons with disabilities. For instance, the United Kingdom (UK)allows the implementation of one national health system. In contrast, Canada, Australia, and USA are governed through a federal system; therefore, implementation of policies and programmes intended for persons with disabilities can be fragmented because of a long chain of bureaucracies11. As a result of such discrepancies, Friedner & Osborne13 reason that disability experts should steer the implementation of disability legislation. For instance, the Indian Disability Act is specific on enforceable guidelines in matters relating to accessibility. The law mentions that the physical environment should be accessible, but it does not indicate any consequences for those violating such laws14. However, the Americans with Disabilities Act (ADA) specifically addresses the needs of persons with a disability with enforceable regulations, and any complaints are dealt with accordingly11.
As noted by Van Rooy et al.15, Namibia has made good progress in accepting persons with disability in the community. This occurred as a result, among other measures, of a Policy on Orthopaedic Technical Services, which was established to facilitate community mobility, including a community-based rehabilitation (CBR) programme. However, this Policy could have been more effective if the Namibian government had also developed a policy about the role of occupational therapy services as a key role player in facilitating community integration. Schneider et al.16 concur that for such policies to succeed, all the needs of persons with disabilities should be addressed and specified.
A country's health care system can be measured, among others, by the quality of life of persons with SCI in the community. This may be translated to health policies that guide researchers and healthcare professionals on interventional measures 3. Reliable data on SCI is therefore crucial in formulating measures to monitor injury occurrences and continuous follow-up programmes starting from initial admission to post-injury community integration3,17,18. However, few countries across the globe have well-established SCI registry systems, a tool important in any country to monitor, formulate mechanisms and manage its population of persons with SCI. Canada is an excellent example of countries with an SCI registry via the Rick Hansen SCI Registry (RHSCIR)17. Like RHSCIR, the American SCI model database, the Australian SCI registry and the European Spinal Injury Federation provide their respective countries statistical evidence related to SCI17,18,19.
These SCI registries act as evidence to facilitate the development of long-term care of survivors of SCIs20. For instance, RHSCIR, established in 2004 in Canada, aimed at capturing records of survivors of SCIs from as early as admission, during the rehabilitation process, and up to ten years in the community. Though this model had a share of challenges, its benefits had been immense in obtaining internationally acceptable data and facilitating the development of evidence-based practices18,20. Such information has been of significant value in highlighting the epidemiology of survivors of SCI in these countries and predicting their quality of life while in the community 21,22. Unfortunately, developing countries in Africa and Asia do not have such a registry23. As noted by Leshota24 and Musubire et al.25 the lack of accurate SCI statistics in African countries affects policy implementation, particularly in facilitating community integration processes for persons with disabilities.
The most appropriate policies that consider challenges faced by persons with disabilities should address the social needs of these individuals. This is not to say there are no medical challenges but that social factors contribute primarily to community integration and participation26. Germany is a good example of a country that has achieved this with an advanced model of care for survivors of SCI. The country has 15 well equipped SCI Units, an established uniform SCI care guideline, a research centre at The German Medical Society of Paraplegia (DMGP) and implements strategies to reduce complications as a result of SCI and community participation post SCI27. The Ministry of Health and Social Welfare in Lesotho, through its National Disability and Rehabilitation Policy 2011, is another country that caters for both the medical and social needs of persons with disabilities; as a result, it provides comprehensive care24. In South Africa, however, where the government has established the National Rehabilitation Policy, based on the UNCRPD standard rules of maximum acknowledgement of the human rights of persons with disabilities, Mji et al.28 argue little attention has been given to avail enough resources for their full implementation and for the policy to benefit concerned parties in the community. This includes ensuring full accessibility and that persons with disabilities live comfortably and independently in the community free from physical barriers, access to rehabilitation, and provide health services. Therefore, it is not surprising that more recently, the United Nations appealed for a commitment from governments to the UNCRPD Articles by reappraising policy implementation and practice of institutions and professionals working with persons with disabilities26.
In Kenya, the 2010 constitution recognised the rights of persons with disabilities under Article 54. This followed the Persons with Disabilities Act, 2003, earlier ratified through the UNCRPD, in which Kenya was a signatory29. Among the Acts established due to Article 54 was the Employment Act, which prohibited discrimination against persons with disabilities in the labour sector and the National Disability Policy that seeks to develop comprehensive community integration of persons with disabilities, including those with SCI29. In the same spirit, The National Council for Persons with Disabilities was established to work collaboratively with relevant bodies to support persons with disabilities in advocacy, information provision, and community integration29.
The Kenya Health Policy 2014-2030 indicates that every citizen has the right to healthcare, social services and participation regardless of their disability. Still, there are challenges in the implementation30; for instance, there is a lack of specialised SCI hospital care and clear clinical guidelines for the treatment of SCI and inadequate resources allocated to coordinate follow-up of survivors of SCI to the community. In addition, the country faces other challenges, among them the scarcity of trained occupational therapists to facilitate these programmes31,32. Like other developing countries, Kenya does not have an SCI registry. There is no standard guideline to promote community integration of survivors of SCI. Institutional care for survivors of SCI is a challenge because, in a country of over 40 million people, only the National Spinal Injury Referral Hospital in Nairobi provides specialised services33. Also, current practice places sole responsibility for change upon the individual and pays little attention to the barriers that hinder their full integration into the community. Occupational therapy managers need to oversee their clients' human and occupational rights with SCI, which could be better achieved if available policies were utilised to advocate for and facilitate community integration for persons with SCI34,35,36. However, occupational therapists who are supposed to work within a team to initiate community integration programmes, are under-resourced. These therapists also rely on Western developed clinical guidelines in their interventions that do not necessarily address their clients' contextual needs 34,35, 36.
This study sought to explore the rehabilitation managers' perceived experience of community integration for persons with SCIs. Rehabilitation managers are suitably positioned to enforce and enact policy related to holistic rehabilitation intervention, including preparing patients for community integration. Their perspectives may highlight potential barriers or enablers to ensuring more effective community integration for survivors of SCIs.
METHOD
Setting
The study was conducted in Nairobi, Kenya.
Study design
This was a qualitative, descriptive phenomenological study37 that explored the experiences and perceptions of rehabilitation managers in Kenya via individual interviews. Rehabilitation managers were generally occupational therapists who oversee rehabilitation programmes for survivors of SCI at various levels. Phenomenology as a qualitative methodology allowed the participants to share their experiences with SCI and their concerns on service delivery and supported the capture of rich information37.
Study population and sampling strategy
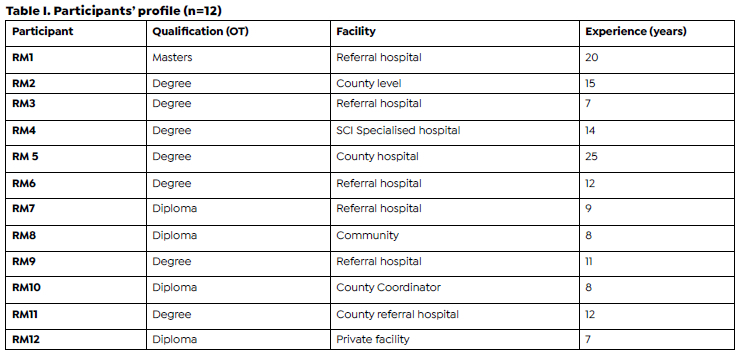
There were 48 rehabilitation managers in Nairobi, of which 12 managers, who qualified in occupational therapy, had worked for more than two years in their respective positions and were overseers of rehabilitation services, including rehabilitation of persons who sustained SCIs, were purposively sampled. Most managers held undergraduate degrees (n=9), and the remaining held diplomas (n=3). The interviews were conducted using an interview schedule37.
Data collection
Each interview session lasted approximately 90 minutes in a neutral place to ensure confidentiality37. The interviewer was careful to distinguish between the role of being a practitioner and researcher to avoid being influenced by his position, as this might have risked losing important data37. An interview guide was used during each interview, audio-recorded, and notes were taken to capture the respondents' experiences, including non-verbal expressions34. The interviewer ceased collecting data when data saturation was reached. Prior to the interviews, informed consent was obtained from the participants to record notes and audio-recording of the sessions37.
Data analysis
Content analysis was performed37. The data were transcribed verbatim before analysis was done. The researcher listened to recorded discussions and cross-checked the transcripts. The first author read the transcribed data to gain familiarity with the text. The interview question guide was instrumental in enabling the first author in organising and summarising the data. Ideas and concepts were identified. The QSR NVivo software version 10 was used to organise and analyse the field notes and recordings derived from the individual interviews34. Meaningful units were coded and then these were grouped into categories. Finally, the first author interpreted the findings and connections between categories were established and reduced into themes with assistance of the co-authors. All common themes were coded and categorised in a standard way using the tree node structure to make comparisons for ease of analysis. Summaries in tabular form per thematic area were developed. Verbatim quotes were used to support critical issues and messages37.
Ethical considerations
The study's ethical approval was obtained from the University of KwaZulu Natal Biomedical Research Ethics Committee (BREC Ref no: BE070/18) and The Kenyatta National Hospital, University of Nairobi Ethics Research Committee. All relevant principles of ethics were upheld during the study37, including the use of pseudonyms to protect the privacy of all participants, ensuring the accuracy of information by safeguarding the rigour and trustworthiness of the study through bracketing, peer debriefing and use of thick descriptions.
FINDINGS
Those who participated in these individual interviews were rehabilitation managers overseeing rehabilitation programmes for persons living with SCI at various levels. They both had wide experience ranging from 7-25 years in rehabilitation management and academic qualification in occupational therapy. Their qualifications ranged from a diploma in occupational therapy to a master of science in occupational therapy (Table I above).
The findings revealed three emergent subthemes and one central theme around rehabilitation managers' perceived experience of community integration for survivors of SCI (Figure 1 above).
The central theme described the rehabilitation managers' experiences in overseeing rehabilitation programmes for survivors of SCI at various levels. The managers highlighted their overall experience of facilitating the integration of survivors of SCI in the community as inadequate.
"...this where we fail in offering comprehensive care to our clients probably the reason why we don't do follow-up to the community" (RM11).
"My major role is to ensure sufficient rehabilitation of all clients including those with SCI because we don't have specific specialised hospital for SCI. Where possible we work with other stakeholders for community integration" (RM3).
Subtheme 1. The role of occupational therapy rehabilitation managers in spearheading community integration of survivors of SCI
The managers reported that the majority are aware of their role in facilitating empowerment strategies that will positively influence community integration of survivors of SCIs. They reported that they are also involved in direct service delivery in hospitals and other rehabilitation facilities, offering rehabilitation to survivors of SCI through rehabilitation equipment, assistive aids and to some extent, alternatives where assistive aids are lacking. The therapy activities include ADLs such as self-care, transfers, bladder and bowel control, environmental adjustment and adaptation to enhance independence. It also includes facilitating emotional and psychological adjustment and management of sexuality.
"As a supervisor, I also have to work to serve as a good example. I do supervise orthopaedics wards; this is where we have among the cases attended to our clients with SCI. My major role is to ensure my colleagues have enough treatment aids, the patients' needs are addressed and to work collaboratively with the rehabilitation team and family members to prepare the clients for possible discharge to the community. Sincere we don't have specialised SCI unit, when there is need for long term care, I facilitate referrals to National Spinal Cord Injury Hospital" (RM1).
The managers added that they are also involved in planning, supervision, and monitoring rehabilitation services in hospitals and the community. This includes using the SOAP (subjective, objective, planning) approach and advocating for the role of occupational therapy in the management of SCIs in the community to enhance the participation of survivors of SCIs. The managers further reported that their role includes advocating for more fiscal allocations for the training of occupational therapists in the rehabilitation of survivors of SCI and ensuring budgets for rehabilitation equipment such as wheelchairs, commodes, and assistive aids.
Other managers like RM3 affirmed that I coordinate OT activities in the hospitals and community centres for people with SCIs. In contrast, others noted that for both inpatients and outpatients, they involve other rehabilitation managers, caregivers and stakeholders in the rehabilitation process of SCI. RM5 indicated that they work closely with partners, including family members, non-governmental organisations, religious organisations, and local administrative agencies, particularly for community integration and home-based care to facilitate the participation of survivors of SCI after discharge from hospital to the community.
"...(we) visit the home to assess the environment for adaptation and organise transport for the discharged patient and the staff accompanying the patient" (RM7).
The managers reported that they ensure appropriate referrals for specialised care and advocate for policy formulation and implementation regarding the management of SCI.
"(We) advocate for SCI specialised hospitals in Kenya, currently we have only one to train not only OTs(but) enough (other) health care workers" (RM9).
Subtheme 2. Occupational therapy rehabilitation managers' experiences in the aftermath of community integration of survivors of SCI
All managers confirmed having had experiences related to unsuccessful community integration of survivors of SCI. Among them were discrepancies observed was the preparation process for survivors of SCI to return to the community. A manager, RM11 lamented that a lack of clear guidelines on managing SCI contributes to increased complications and low community participation. Consequently, people with SCIs are discharged to the community without proper preparation, thus inhibiting their return to work. The managers noted that interventional procedures for community integration are crucial to guide occupational therapists on training survivors of SCIs to access services in the community with minimal difficulty. These include, for example, online shopping or partnering with chain supermarket owners and transport services to serve their unique needs and advocate for those who may be working from home since patients find it difficult to adjust to their working environment, which remains inaccessible if is not adapted to suit their disability. Occupational therapists are, however, unable to adequately attend to most patients at the community level.
It was revealed by a manager, RM8 that financial constraints hinder follow-up to the community. The majority of managers cited the lack of specialised SCI units resulting in inadequate support to address the needs of survivors of SCI comprehensively, lack of proper equipment and infrastructure, and training for occupational therapists as reasons why reasonable interventional procedures are never realised.
"Imagine one specialised SCI hospital to serve 47 counties and 40 million plus population, that's the greatest barrier. Am not sure even our specialised facility has enough trained OTs, financial resource is also another barrier, because without money you can't train, have proper treatment equipment, you will be less motivated consequently these individuals will be poorly discharged to the community where they will be dependent" (RM10).
Both poor interprofessional collaboration between local governments and hospitals and negative societal attitudes towards survivors of SCIs also negatively influence how people with SCI participate in community occupations. It was cited by the manager, RM9 that lack of interprofessional collaboration, coordination and teamwork was the main reason patients were being discharged before other team members could offer their services.
"The society's attitude, and when I talk of society, I also include OTs we are part of the society, we are not well informed to address the needs of these individuals" (RM5).
Spinal cord injuries are accidental, costly and require long term financial muscle to manage all accompanying challenges, with most medical insurance companies reluctant to compensate for related costs. Therefore, without such cover, the rehabilitation process is frequently disrupted.
"NHIF (national health insurance fund) does not cover OT services particularly for individual member contributors" (RM9).
To care for survivors of SCIs, rehabilitation personnel must possess broad skills and competencies in SCI intervention and evidence-based practice for relevant and appropriate management; however, managers reported inadequate skills training in SCIs and limited exposure.
"In the hospital, nobody has been trained on SCI rehabilitation, it's individuals' effort, you go for online classes, libraries, you Google because our training institutions, medical training colleges and universities there is no speciality not even for our doctors so when anyone who comes is shocked to realise you are not trained for this and also don't know what you are facing" (RM7).
This study found that inadequate formulation and implementation of policies and legislation on management and community care for survivors of SCIs have contributed to the lack of proper and special transport and mobility facilities, thus posing a significant challenge to participating in sports activities leisure. It was reported that it was challenging to realise the required adaptation of homes, work and recreational facilities.
"...most buildings lack ramps in our hospitals being a typical example. Lack of proper and special transport and mobility is a very big challenge for these people. There is also lack of proper adaptation of their homes (houses, toilets) work and recreational facilities. Most of them are not modified to suit those with SCIs. Their participation in activities such as sports and athletics is not fully exploited" (RM1).
Subtheme 3: Strategies to facilitate community integration of people with SCI
Through their experience, the managers suggested the perceived ways of improving the experience of living with SCIs both in care facilities and the community. They indicated the need to develop proper guidelines supported by stakeholders to ensure a holistic approach to managing survivors of SCI. It was also recommended that rehabilitation facilities be equipped with modern treatment aids and equipment. In the managers' view occupational therapists should be supported and be ready to learn best practices from other countries that have successfully implemented programmes for the rehabilitation and reintegration into the community of people with SCI.
It was suggested that more resources be allocated to the management of SCIs and the county health administrative boards, and the community be involved in making such decisions. These include training, conducting research to identify gaps in interventions, equipping rehabilitation centres, and establishing specialised units/facilities and programmes for survivors of SCI to prepare them for optimal reintegration into the community.
"To reinforce community participation, it should involve the strengthening of partnerships with stakeholders, government, employers, NGO'S, religious organisations, school's/learning institutions and the general community in addressing the needs of people with SCI" (RM5).
The managers also suggested the need to revise the college syllabus to include specialised programmes on SCI to equip health professionals on intervention skills, SCI management, rehabilitation and community integration in addition to programmes meant to educate the community on SCI for attitude transformation and sensitisation of the rights of survivors of SCIs.
"...this can be done through movements such as scouts, girl guides, presentational award schemes and total involvement voluntary care of SCI and other PWDs while in the hospital and at home" (RM9).
DISCUSSION
This study aimed to describe the perception of experiences of rehabilitation managers on factors that influence community integration of survivors of SCIs. The findings confirmed that obstacles faced are related to the discrepancies during the preparation of these individuals for return to the community. A lack of clear guidelines for the management of SCIs contributes to increased complications and poor community participation. This influences occupational therapists' interventional processes, which may fail to rehabilitate these individuals for community reintegration effectively. While Harvey38 concurred that the absence of clear guidance compromises the rehabilitation process in SCI, Fehlings and colleagues39 and Wong et al.40 observed that clinical practice guidelines could promote standardised care and improve a gradual return to community participation. Baradaran-Seyed and colleagues41 and Samuelsson and Wressle42 indicate that the lack of clinical practice guideline development to ensure the quality of SCI rehabilitation process in Kenya, can be attributed to a lack of individual responsibility and commitment facilitated by a lack of supervision and guidance. This is additionally compounded by the lack of specialised units for SCI at health facilities.
New et al.43 established that patients with SCI who were not under the care for SCI specialised units had worse outcomes. Thus, the lack of specialised units for SCI also contributed to the absence of organisational support, which resulted in inefficient efforts to address the needs of survivors of SCIs. Other contributing factors included deficient equipment and infrastructure, no specialisation training in SCI for occupational therapists, and scarcity of resources to follow-up on patients and coordinate various activities. Consequently, people with SCI were poorly prepared before being discharged to the community and follow-ups to facilitate community integration were also compromised. Guilcher et al.44 and Goodridge et. al.45 similarly observed the role of the macro health system and environmental networks' in influencing the care of survivors of SCI. Therefore, the healthcare system should consider these factors in determining potential solutions that meet the rehabilitation needs of survivors of SCIs. These solutions should include strong stakeholder involvement in the hospital and the community. This is important because rehabilitation is intended to prepare survivors of SCI for community participation even though, according to Van Loo et. al.46, rehabilitation does not typically realise this intended goal. Specific barriers related specifically to a lack of specialised skills training also mean the call for occupational therapists' training and education to handle the needs of people with SCI becomes paramount 32,47,48.
On the other hand, societal attitudes such as viewing people with SCIs as incapable of participating in or contributing to society can negatively influence how survivors of SCI participate in community occupations. Such attitudes may result from a lack of interprofessional collaboration, coordination, and teamwork, leading to patients discharge before occupational therapists can offer their services. These findings align with those of Ünver et al.49 and Falk et al.50, who acknowledge that working together prevents isolated and fragmented approaches to patient intervention, develops positive attitudes and facilitates knowledge sharing to improve care skills. This was supported by Kraft et al.51, who also emphasised the importance of leadership and organisational structures for stimulating communication and promoting collaboration between team members. In contrast, Higgins et al.52 have stated that it is challenging to achieve sufficient depth of understanding of the complexity of collaborative practice. They recommended that managers encourage collaboration within their area of jurisdiction.
This study also established that weak policies and implementation initiatives hamper the facilitation of community integration. As a result, several recommendations were suggested. Occupational therapy rehabilitation managers should develop proper guidelines supported by other rehabilitation teams to ensure a holistic approach to managing SCI survivors. This should include stakeholder involvement towards enhancing interventional skills within occupational therapy practice and implementing rehabilitation (in line with policy) to ensure community participation without hindrances.
Rehabilitation facilities should be equipped with modern treatment aids and equipment with rehabilitation managers to make field visits on the ground. Similarly, Guy et al.53 and Moreno et al.54 acknowledge that a lack of standardised guidelines impedes SCI rehabilitation. In contrast, Guilcher et al.44 indicated that overall failure of policies inhibits a holistic approach to the care of survivors of SCI. Therefore, the solution is to tailor health system structures and review rigid policies.
The study suggested allocating more resources for management in SCIs and involvement of all the stakeholders in decision-making to address the training gaps, facilitate research programmes, and equip rehabilitation centres with specialised SCI units. These efforts include implementing the Disability Act and ensuring, among other aspects, medical comprehensive insurance cover for survivors of SCIs by partnering with insurance companies to cover the interventional relevant costs45. Locatelli et al.55 noted that facility leadership support is required for appropriate resource allocation in line with these findings. At the same time, Kruger et al.56 and Ziesmann et al.57 emphasised creating a multidisciplinary curriculum through established healthcare institutions policies towards educating medical professionals on managing individuals with SCI.
CONCLUSION
This study has confirmed inadequacies in community integration of survivors of SCI due to discrepancies within the care system, including the rehabilitation centres, and a lack of clear guidelines and goodwill from the community. However, the study made suggestions on facilitating an enabling environment for community participation, including reinforcement of community participation for SCI survivors. This includes the involvement of all stakeholders in decisionmaking, addressing training gaps, facilitating research programmes, and equipping rehabilitation centres with specialised SCI units. Additionally, implementing disability policies to minimise barriers to community participation and access to essential services, including comprehensive insurance cover for survivors of SCIs, was recommended. Consequently, developing clear and context-specific guidelines on comprehensively managing people with SCI becomes necessary.
Acknowledgements
The authors would like to acknowledge the participants who shared their work experiences while supervising rehabilitation of persons who sustained SCI during the data collection phase.
Declaration of conflicting interests
The authors state that they have no conflict of interest to declare in this study.
Authors' contributions
Evans Obara Obaigwa was the primary researcher in this study, which forms part of a postgraduate degree requirement. Pragashnie Govender and Catharina Jacoba Elizabeth Uys were supervisors of the study and contributed to the conceptualisation of the study and critical review of the paper.
REFERENCES
1. Burns AS, O' Connell C. The challenge of spinal cord injury care in the developing world. The Journal of Spinal Cord Medicine. 2012 1;35(1):3-8. https://doi.org/10.1179/2045772311Y.0000000043 [ Links ]
2. Ropper AE, Neal MT, Theodore N. Acute management of traumatic cervical spinal cord injury. Practical Neurology. 2015 1;15(4):266-272. https://doi.org/10.1136/practneurol-2015-001094 [ Links ]
3. World Health Organization, International Spinal Cord Society. International perspectives on spinal cord injury. World Health Organization; 2013. [ Links ]
4. Clifford J. The UN disability convention and its impact on European equality law. The Equal Rights Review. 2011; 6:11-25. [ Links ]
5. Espelage DL. Ecological theory: Preventing youth bullying, aggression, and victimisation. Theory into Practice. 2014;53(4):257-264. https://doi.org/10.1080/00405841.2014.947216 [ Links ]
6. Geldenhuys JL, Wevers NE. Ecological aspects influencing the implementation of inclusive education in mainstream primary schools in the Eastern Cape, South Africa. South African Journal of Education. 2013 7;33(3):Article #688. https://doi.org/10.15700/201503070804 [ Links ]
7. Duerden MD, Witt PA. An ecological systems theory perspective on youth programming. Journal of Park and Recreation Administration. 2010;28(2):108-120. [ Links ]
8. Parker S, Fisher K. Facilitators and barriers in Australian disability housing support policies: using a human rights framework. Disability Studies Quarterly. 2010;30(3/4). https://doi.org/10.18061/dsq.v30i3/4.1283 [ Links ]
9. Madans JH, Loeb ME, Altman BM. Measuring disability and monitoring the UN Convention on the Rights of Persons with Disabilities: the work of the Washington Group on Disability Statistics. BMC Public Health 2011; 11(4):1-8. https://doi.org/10.1186/1471-2458-11-S4-S4 [ Links ]
10. Kovacs Burns K, Gordon GL. Analysing the impact of disability legislation in Canada and the United States. Journal of Disability Policy Studies. 2010;20(4):205-218. https://doi.org/10.1177/1044207309344562 [ Links ]
11. Prince MJ. What about a disability rights act for Canada? Practices and lessons from America, Australia, and the United Kingdom. Canadian Public Policy. 2010 Jun;36(2):199-214. https://doi.org/10.3138/cpp.36.2.199 [ Links ]
12. Friedner M, Osborne J. Audit bodies: embodied participation, disability universalism, and accessibility in India. Antipode. 2013;45(1):43-60 https://doi.org/10.1111/j.1467-8330.2012.00990.x [ Links ]
13. Nakagawa J, Blanck P. Future Disability Law in Japan: Employment and Accommodation.Loyola of Los Angeles International and Comparative Law Review. 2010; 33(1):173 http://dgtalcommons.lmu.edu/lr/vol33/ss1/6 [ Links ]
14. Math SB, Gowda GS, Basavaraju V, Manjunatha N, Kumar CN, Philip S, Gowda M. The rights of persons with disability act, 2016: Challenges and opportunities. Indian Journal of Psychiatry. 2019:61(Suppl 4):S809 https://doi.org/10.4103/psychiatry.IndianJPsychiatry_105_19 [ Links ]
15. VanRooy G, Amadhila E, Mannan H, McVeigh J, MacLachlan M, Amin M. Core concepts of human rights and inclusion of vulnerable groups in the Namibian Policy on Orthopaedic Technical Services. Disability, CBR & Inclusive Development. 2012 Dec 5;23(3):24-47. https://doi.org/10.5463/dcid.v23i3.132 [ Links ]
16. Schneider M, MacLachlan M, Eide AH, Amin M, Mannan H. Inclusion of vulnerable groups in health policies: Regional policies on health priorities in Africa. African Journal of Disability. 2013;2(1):1-9. https://doi.org/10.4102/ajod.v2i1.40 [ Links ]
17. Dvorak MF, Cheng CL, Fallah N, Santos A, Atkins D, Humphreys S, Rivers CS, White BA, Ho C, Ahn H, Kwon BK. Spinal cord injury clinical registries: improving care across the SCI care continuum by identifying knowledge gaps. Journal of Neurotrauma. 2017 15;34(20):2924-2933. https://doi.org/10.1089/neu.2016.4937 [ Links ]
18. Noonan VK, Kwon BK, Soril L, Fehlings MG, Hurlbert RJ, Townson A, Johnson M, Dvorak MF. The Rick Hansen spinal cord injury registry (RHSCIR): A national patient-registry. Spinal Cord. 2012;50(1):22-27 https://doi.org/10.1038/sc.2011.109 [ Links ]
19. Ronca E, Scheel-Sailer A, Eriks-Hoogland I, Brach M, Debecker I, Gemperli A. Factors influencing specialised health care utilisation by individuals with spinal cord injury: a cross-sectional survey. Spinal cord. 2021;59(4):381-388. https://doi.org/10.1038/s41393-020-00581-6 [ Links ]
20. Furlan JC, Fehlings MG. The National Trauma Registry as a Canadian spine trauma database: a validation study using an institutional clinical database. Neuroepidemiology. 2011;37(2):96-101 https://doi.org/10.1159/000330835 [ Links ]
21. Fekete C, Wahrendorf M, Reinhardt JD, Post MW, Siegrist J. Work stress and quality of life in persons with disabilities from four European countries: the case of spinal cord injury. Quality of Life Research. 2014;23(5):1661-71. https://doi.org/10.1007/s11136-013-0610-7 [ Links ]
22. Jazayeri SB, Beygi S, Shokraneh F, Hagen EM, Rahimi-Movaghar V. Incidence of traumatic spinal cord injury worldwide: a systematic review. European spine journal. 2015;24(5):905-918 https://doi.org/10.1007/s00586-014-3424-6 [ Links ]
23. Joseph C, Delcarme A, Vlok I, Wahman K, Phillips J, Wikmar LN. Incidence and aetiology of traumatic spinal cord injury in Cape Town, South Africa: a prospective, population-based study. Spinal Cord. 2015 Sep;53(9):692-696. https://doi.org/10.1038/sc.2015.51 [ Links ]
24. Leshota LP. Reading the National Disability and Rehabilitation Policy in the light of Foucault's technologies of power. African Journal of Disability. 2013;2(1):1-7. https://doi.org/10.4102/ajod.v2i1.41 [ Links ]
25. Musubire AK, Meya DB, Bohjanen PR, Katabira ET, Barasukana P, Boulware DR, Meyer AC. A systematic review of nontraumatic spinal cord injuries in sub-Saharan Africa and a proposed diagnostic algorithm for resource-limited settings. Frontiers in Neurology. 2017; 8:Article 618. https://doi.org/10.3389/fneur.2017.00618 [ Links ]
26. Mittler P. The UN Convention on the Rights of Persons with Disabilities: Implementing a Paradigm Shift. Journal of Policy and Practice in Intellectual Disabilities. 2015;12(2):79-89. https://doi.org/10.1111/jppi.12118 [ Links ]
27. Blumenthal M, Egen C, Gutenbrunner C, Geng V. People with Spinal Cord Injury in Germany. American Journal of Physical Medicine & Rehabilitation 2017;96: S66-70. https://doi.org/10.1097/PHM.0000000000000584 [ Links ]
28. Mji G, Chappell P, Statham S, Mlenzana N, Goliath C, De Wet C, Rhoda A. Understanding the current discourse of rehabilitation: With reference to disability models and rehabilitation policies for evaluation research in the South African Setting. South African Journal of Physiotherapy. 2013;69(2) 4-9 [ Links ]
29. Kamundia E. Choice, support and inclusion: Implementing article 19 of the Convention on the Rights of Persons with Disabilities in Kenya. African Disability Rights Yearbook. 2013;1:49. [ Links ]
30. Republic of Kenya, Kenya Health Policy 2014-2030. Towards attaining highest standards of health, Ministry of Health, Afya House Cathedral Road, Nairobi. 2014 [ Links ]
31. Kenya Occupational Therapists Association 2021., KOTA Background, [accessed 2021 March 12], available from http://www.kotakenya.org/index.php/about/kota-background [ Links ]
32. Cloete LG, Obaigwa EO. Lived experiences of caregivers of children with autism spectrum disorder in Kenya. African Journal of Disability 2019;8:1-9. https://doi.org/10.4102/ajod.v8i0.435 [ Links ]
33. Kenya National Bureau of Statistics. Kenya facts and figures, [internet] (accessed 2020 June 2] from Available from https://www.knbs.or.ke/download/kenya-facts-2015 [ Links ]
34. Hammell KW. Quality of life, participation and occupational rights: A capabilities perspective. Australian occupational therapy journal. 2015;62(2):78-85. https://doi.org/10.1111/1440-1630.12183 [ Links ]
35. Hocking C, Townsend E. Driving social change: Occupational therapists' contributions to occupational justice. World Federation of Occupational Therapists Bulletin. 2015;1;71(2):68-71. https://doi.org/10.1179/2056607715Y.0000000002 [ Links ]
36. van Vuuren JJ, Okyere C, Aldersey H. The role of Occupational Therapy in Africa: A scoping review. South African Journal of Occupational Therapy. 2020;50(3):3-21. https://www.sajot.co.za/index.php/sajot/article/view/652 [ Links ]
37. Ritchie J, Lewis J, Nicholls CM, Ormston R, editors. Qualitative research practice: A guide for social science students and researchers. Sage; 2013. [ Links ]
38. Harvey LA. Physiotherapy rehabilitation for people with spinal cord injuries. Journal of Physiotherapy. 2016 1;62(1):4-11. https://doi.org/10.1016/j.jphys.2015.11.004 [ Links ]
39. Fehlings MG, Tetreault LA, Wilson JR, Kwon BK, Burns AS, Martin AR, Hawryluk G, Harrop JS. A clinical practice guideline for the management of acute spinal cord injury: introduction, rationale, and scope. Global Spine Journal. 2017; 7(3S) 84S-94S [ Links ]
40. Wong JJ, Côté P, Shearer HM, Carroll LJ, Yu H, Varatharajan S, Southerst D, van der Velde G, Jacobs C, Taylor-Vaisey A. Clinical practice guidelines for the management of conditions related to traffic collisions: a systematic review by the OPTIMa Collaboration. Disability and Rehabilitation. 2015;37(6):471-489. https://doi.org/10.3109/09638288.2014.932448 [ Links ]
41. Baradaran-Seyed Z, Nedjat S, Yazdizadeh B, Nedjat S, Majdzadeh R. Barriers of clinical practice guidelines development and implementation in developing countries: a case study in Iran. International Journal of Preventive Medicine. 2013;4(3):340-348. [ Links ]
42. Samuelsson K, Wressle E. Turning evidence into practice: Barriers to research use among occupational therapists. British Journal of Occupational Therapy. 2015;78(3):175-181. https://doi.org/10.1177/0308022615569511 [ Links ]
43. New PW, Simmonds F, Stevermuer T. Comparison of patients managed in specialised spinal rehabilitation units with those managed in non-specialised rehabilitation units. Spinal Cord. 2011 Aug;49(8):909-916. https://doi.org/10.1038/sc.2011.29 [ Links ]
44. Guilcher SJ, Craven BC, Lemieux-Charles L, Casciaro T, McColl MA, Jaglal SB. Secondary health conditions and spinal cord injury: an uphill battle in the journey of care. Disability and Rehabilitation. 2013;1;35(11):894-906. https://doi.org/10.3109/09638288.2012.721048 [ Links ]
45. Goodridge D, Rogers M, Klassen L, Jeffery B, Knox K, Rohatinsky N, Linassi G. Access to health and support services: perspectives of people living with a long-term traumatic spinal cord injury in rural and urban areas. Disability and Rehabilitation. 2015;37(16):1401-10. https://doi.org/10.3109/09638288.2014.972593 [ Links ]
46. Van Loo MA, Post MW, Bloemen JH, Van Asbeck FW. Care needs of persons with long-term spinal cord injury living at home in the Netherlands. Spinal Cord. 2010;48(5):423-428. https://doi.org/10.1038/sc.2009.142 [ Links ]
47. Hyland A, Mc Grath M. Sexuality and occupational therapy in Ireland-a case of ambivalence? Disability and Rehabilitation. 2013;35(1):73-80. https://doi.org/10.3109/09638288.2012.688920 [ Links ]
48. Britton L, Rosenwax L, McNamara B. Occupational therapy practice in acute physical hospital settings: Evidence from a scoping review. Australian Occupational Therapy Journal. 2015 2(6):370-7. https://doi.org/10.1111/1440-1630.12227 [ Links ]
49. Ünver S, Findik ÜY, Özkan ZK, Sürücü Ç. Attitudes of surgical nurses towards pressure ulcer prevention. Journal of tissue viability. 2017;26(4):277-281. https://doi.org/10.1016/j.jtv.2017.09.001 [ Links ]
50. Falk AL, Hopwood N, Dahlgren MA. Unfolding practices: A so-ciomaterial view of interprofessional collaboration in health care. Professions and Professionalism 2017;7(2):1-14 http://doi.org/10.7577/pp.1699 [ Links ]
51. Kraft M, Blomberg K, Hedman AM. The health care professionals' perspectives of collaboration in rehabilitation-an interview study. International Journal of Older People Nursing. 2014;9(3):209-216. https://doi.org/10.1111/opn.12020 [ Links ]
52. Higgins R, Murphy B, Worcester M, Daffey A. Supporting chronic disease self-management: translating policies and principles into clinical practice. Australian Journal of Primary Health. 2012;18(1):80-87.https://doi.org/10.1071/PY11006 [ Links ]
53. Guy SD, Mehta S, Harvey D, Lau B, Middleton JW, O'Connell C, Townson A, Truchon C, Wolfe D, Bradbury CL, Bryce TN. The CanPain SCI clinical practice guideline for rehabilitation management of neuropathic pain after spinal cord: recommendations for model systems of care. Spinal Cord. 2016 ;54(1): S24-27. https://doi.org/10.1038/sc.2016.91 [ Links ]
54. Moreno A, Zidarov D, Raju C, Boruff J, Ahmed S. Integrating the perspectives of individuals with spinal cord injuries, their family caregivers and healthcare professionals from the time of rehabilitation admission to community reintegration: protocol for a scoping study on SCI needs. BMJ Open. 2017;7(8): e014331. https://doi.org/10.1136/bmjopen-2016-014331 [ Links ]
55. Locatelli S, Gerber B, Goldstein B, Weaver F, LaVela S. Health care provider practices, barriers, and facilitators for weight management for individuals with spinal cord injuries and disorders. Topics in Spinal Cord Injury Rehabilitation. 2014;20(4):329-37. https://doi.org/10.1310/sci2004-329 [ Links ]
56. Kruger EA, Pires M, Ngann Y, Sterling M, Rubayi S. Comprehensive management of pressure ulcers in spinal cord injury: current concepts and future trends. The Journal of Spinal Cord Medicine. 2013 Nov 1;36(6):572-585. https://doi.org/10.1179/2045772313Y.0000000093 [ Links ]
57. Ziesmann MT, Widder S, Park J, Kortbeek JB, Brindley P, Hameed M, Paton-Gay JD, Engels PT, Hicks C, Fata P, Ball CG. STARTT: development of a national, multidisciplinary trauma crisis resource management curriculum-results from the pilot course. Journal of Trauma and Acute Care Surgery. 2013 Nov 1;75(5):753-758. https://doi.org/10.1097/TA.0b013e3182a925df [ Links ]
 Correspondence:
Correspondence:
Pragashnie Govender
naidoopg@ukzn.ac.za
Received: August 2021
Peer review: November 2021
Revised: January 2022
Accepted: June 2022
Published: April 2023
Editor: Blanche Pretorius: https://orcid.org/0000-0002-3543-0743
Funding: EOO received tuition remission from the University of KwaZulu-Natal, South Africa, towards a PhD degree. This paper emanated from this stream of study.


{kind=link}
{kind=link}