










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.53 n.1 Pretoria Apr. 2023
http://dx.doi.org/10.17159/2310-3833/2023/vol53n1a6
RESEARCH ARTICLE
Physical activity resource needs of occupational therapists in primary public health care in Gauteng, South Africa
Karin van NiekerkI; Sabrina Raquel da SilvaI, II; Clarette SwartI, III; Marnique HugoI, IV; Zolani Phiwokuhle FlatelaI, V; Ansa Janse van VuurenI, VI
IOccupational therapy department, University of Pretoria, South Africa. Karin van Niekerk: https://orcid.org/0000-0003-2952-1064; Sabrina Raquel da Silva: https://orcid.org/0000-0003-0783-449X; Clarette Swart: https://orcid.org/0000-0002-9260-1473; Marnique Hugo: https://orcid.org/0000-0001-9782-6244; Zolani Phiwokuhle Flatela: https://orcid.org/0000-0002-9501-2623; Ansa Janse van Vuuren: https://orcid.org/0000-0003-0568-1389;
IIPrivate practice (ASE Lifestem Occupational Therapy), South Africa
IIIKing George Hospital, South Africa
IVTintswalo Hospital, South Africa
VNelson Mandela Academic Hospital, South Africa
VIPrivate practice (Chrisna Goddefroy Occupational Therapists), South Africa
ABSTRACT
INTRODUCTION: Resource constraints in primary health care settings in South Africa give rise to challenges for occupational therapists. This study aimed to determine the physical activity resource needs (including objects used and space demands) of occupational therapists in the primary health care context of Gauteng, South Africa
METHOD: A qualitative, descriptive research design was used. The participants were occupational therapists working in primary health care settings in Gauteng. Convenience and snowball sampling were used. Data were collected through two online asynchronised focus groups, conducted over three days each. Thematic analysis was used to analyse the data
FINDINGS: Findings included the resource constraints experienced by occupational therapists and how the occupational therapists' adaptability helped them overcome these constraints. Space, resources for basic and instrumental activities of daily living, assistive devices, Bobath plinths and recyclable and low-cost materials were identified as being particularly useful physical activity resource needs
CONCLUSION: Although limited physical activity resources were available in the settings, therapists' skills in adaptability proved useful in using unconventional resources instead. This study's results identify physical resources deemed as most useful to provide occupational therapy services in primary health care. Furthermore, the results provide information to the education faculty in order to adapt the undergraduate curriculum to better prepare occupational therapy students for practice in primary health care
Implications for practice
• The findings can be communicated to management of primary health care facilities in order to procure or advocate for the procurement of resources deemed as essential in primary health care practice contexts.
• Innovation, problem-solving and adaptability can be valuable characteristics used in professional reasoning that may enable occupational therapists to overcome physical resource barriers.
• Faculty at tertiary educational institutions may utilise the findings in order to adapt curriculums to better prepare occupational therapists for work in the South African primary health care context.
• Occupational therapy students should gain experience in developing and adapting activities using recyclable and reusable materials for diverse clients, including children and adults.
Keywords: assistive devices, activities of daily living, Bobath, recyclable and low-cost material, unconventional resources, online asynchronous focus groups
INTRODUCTION AND LITERATURE REVIEW
The World Health Organisation states that Primary health care (PHC) facilities are an essential part of health care based on practical, scientifically sound and socially acceptable methods and technology made universally accessible to individuals and families in the community through their full participation and at a cost that the community and citizens afford to maintain1 p.42. In South Africa, the majority of the population has access to and makes use of public PHC facilities2. Rehabilitation services are provided in PHC as part of the continuum of care as set out by the National Department of Health3. This is aligned to the recommendations in the World Health Organization's Rehabilitation 2030: a call for action4.
South Africa is a resource-constrained context, where the rehabilitation workforce is stretched to provide services to the large population requiring their services56. Historically, rehabilitation services have not been a priority in the South African health system, with higher emphasis placed on medical and curative approaches57. This has contributed to limited resources available for rehabilitation services with therapists reporting limited budget allocation and difficulties in procurement7.
Occupational therapists work in PHC facilities alongside other members of the rehabilitation team8. Occupational therapists use activities during therapy and select these activities through professional reasoning9. The fourth edition of the Occupational Therapy Practice Framework (OTPF) explains that during professional reasoning, occupational therapists have to consider the activity demands of the activities they want to use10. Activity demands are what is commonly required in order to perform an activity or occupation. Among the many factors included in the activity demands are the objects used, as well as the space demands. The aforementioned objects include tools, supplies, equipment and resources used to carry out the activity10. In this study, these objects as well as the space demands are referred to as physical activity resources. Table 11 in the OTPF was used as a framework for this study as it encapsulates the relevance and importance of physical activity resources in occupational therapy intervention and describes how the absence of physical activity resources creates a barrier for occupational participation10. Table I (above) illustrates an adapted version of Table 11 of the OTPF.
The OTPF additionally explains that occupational therapists consider the activity demands during their professional reasoning and that these activity demands can potentially act as a barrier to participation in activities and occupations10. Physical activity resources are integral to the planning and execution of interventions - the availability of physical activity resources essentially govern which activities can be used.
Schell's Ecological Model of Professional Reasoning9 encapsulates the factors that an occupational therapist considers during professional reasoning. Some of the factors that are considered during professional reasoning and activity selection are payment options, working space and the equipment and resources available. Several studies have shown how these factors may pose challenges in South African PHC settings25, similar to how the OTPF describes how activity demands, which are also considered during professional reasoning, may act as a barrier10.
The availability of resources is one of the most influential factors on rehabilitation services in the rural environment11. In a study done by van Stormbroek and Buchanan12 on the practice of occupational therapists in rural health contexts, participants reported that limited resources prevented the occupational therapists from developing a professional identity. Participants felt they had to treat performance components in the same way physiotherapists do, instead of treating performance within occupations1,2. Additional challenges faced by occupational therapists in resource-constrained contexts (as noted by Toal-Sullivan13) include managing the load of patient responsibilities and struggling with professional reasoning .
In South Africa, newly qualified occupational therapists are typically placed in PHC settings in their first year of practice in order to complete their compulsory community service year14. It was reported by a therapist doing community service in rural Eastern Cape, South Africa, that many of the occupational therapy departments in PHC do not have allocated budgets14. Other participants in the same study reported using their own money as soon as the recyclable materials, out of which they made their own physical activity resources, were exhausted14. With regards to financial resources, De Beer et al. state that the absence of financial resources can lead occupational therapists to feel inadequate or frustrated as they cannot provide the service they want to provide, that can contribute to burn out15.
Literature thus illustrates how the scarcity of objects such as tools, supplies, equipment, and resources, as described by the OTPF, may act as a barrier during professional reasoning as it limits the possible activities and services that can be provided and may therefore limit the ability of occupational therapists to navigate PHC contexts in South Africa10. This is of particular concern as inexperienced community service therapists often have to navigate these challenging resource-constrained contexts.
Although several studies report on the scarcity of resources for occupational therapy services in PHC, it is not clear exactly what physical activity resources occupational therapists use and what they feel is necessary to provide effective rehabilitation services in PHC12,14. As this information is not available, it may be more difficult to advocate for additional resources to use in these contexts. Therefore, the aim of this study was to determine the physical activity resource needs of occupational therapists in the PHC context in the Gauteng province of South Africa. To achieve the aim of the study, the researchers formulated two objectives: to explore which physical activity resources are currently used by occupational therapists in PHC in Gauteng; and to explore which physical activity resources occupational therapists deem necessary to provide adequate intervention in their specific context.
METHOD
Study Design
This study was conducted using a qualitative, descriptive research design, as described by Lambert and Lambert16. Data were collected during two asynchronized online focus groups.
Population and Sample Selection
The population for this study were occupational therapists practising in PHC settings, in the Gauteng province of South Africa, during the year 2021. The researchers were based in Gauteng and therefore familiar with the context. As the PHC setting in South Africa consists of clinics and district-level hospitals, the inclusion criteria for the study were occupational therapists that work in PHC clinics or hospitals in Gauteng.
Non-probability sampling methods, convenience and snowball sampling were used. In terms of time and financial resources available, these sampling methods were the most suitable for this research study17,18. Participants were contacted through email via the alumni database of the University of Pretoria Occupational Therapy Department. Potential participants then passed the invitation on to colleagues who may meet the inclusion criteria, thereby employing snowball sampling. Occupational therapists that were interested to participate contacted the research team.
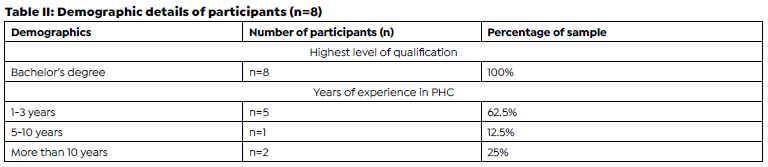
Five to eight participants are seen as the ideal number of participants to use for focus groups17,19. Although eight participants were recruited for the first focus group, only four participated. Therefore, a second focus group was held with an additional four participants. Potential participants were contacted via email and snowball sampling was used again to reach more participants that met the inclusion criteria. Participants of all ages and with varied years of experience were included to increase the diversity of perspectives. Table II (above) illustrates the demographic information of the participants.
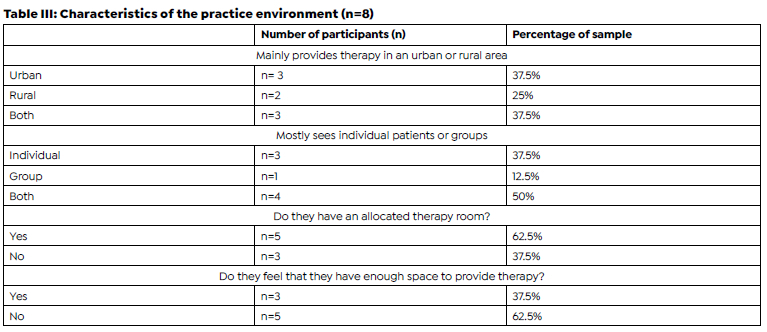
Table III (above) provides a summary of where and to whom services are provided by the participants.
Research Tools
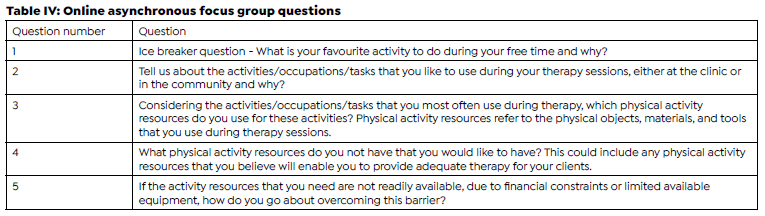
Before data were collected, two experts reviewed the proposed focus group questions. The experts were both academics with expertise in the PHC context. The feedback provided by the experts was primarily related to the wording of the questions. The suggested feedback enabled the researchers to adapt the questions before the focus groups could commence. Table IV (page 47) illustrates the focus group questions.
Data collection procedures
Data were collected for this study by means of two asynchronized online focus groups, each presented over three days. Asynchronized focus groups (where participants do not all have to be online at the same time), were preferred over synchronized focus groups where participants all meet online at the same time. Asynchronous groups were advantageous as it allowed the research participants time to reflect on the questions posted in written format by the facilitator before answering them, in writing. This provides opportunity for depth and accuracy in the presentation of their perspective2021. Furthermore, participants are also allowed the opportunity to respond to each other. The asynchronous groups could accommodate the research participants with limited time as they could respond to the questions and add to the discussion at any time that suited them best throughout the three days22. Additionally, by using an online focus group, the researchers could comply with the regulations imposed to curb the COVID-19 pandemic.
The focus groups were conducted via an online platform, Google Groups. Google groups provided a discussion platform where the focus groups could be hosted and where the data could be securely captured. Each participant was invited to the group through their email addresses. Access to the group forum was tested before the onset of the group to ensure that participants had access.
The focus groups were facilitated by the research supervisor. This was in alignment with the ethics committee requirement that the focus groups be facilitated by an experienced facilitator. On the first day, the participants were required to read the instructions of the focus group, complete a short questionnaire via a link contained within the instructions and answer an ice breaker question. The questionnaire included demographic questions, as well as questions pertaining to where and to whom services were provided, as reported in Table II and III. Additionally, on the first day, they received the first focus group question. Two focus group questions were posted on the second day followed by the final question that was posted on the third day. Participants responded to all questions in written format. The facilitator accessed the platform multiple times daily to ensure that optimal facilitation was provided throughout the discussion. Participants were encouraged to respond to each other's contributions in the focus group instructions as well as by the facilitator throughout the discussions.
Data Analysis
Thematic data analysis was used to analyse the data. The phases of thematic data analysis, as described by Braun and Clarke, were followed23. Phase 1 required the researchers to familiarise themselves with the data. Transcripts were obtained by copying the discussions from both online focus groups. ATLAS.ti software was used to assist with the organizing and coding of the data. Phase 2 consisted of generating initial codes. The coding was done by a group of two researchers on ATLAS.ti. The analysis was then discussed within the bigger group of six researchers and changes were incorporated based on consensus reached between the researchers. A framework for coding was created as the data emerged 24. Both focus groups produced similar codes, leading the researchers to believe that data saturation was reached.
During phase 3 the codes were collated and organised into themes and sub-themes. Thematic maps were used to illustrate how the codes were separated into themes and subthemes. This process was completed by two researchers that discussed the results with the bigger group. Phase 4 required the reviewing of the themes. The group of six researchers reviewed the themes and reached consensus on the identified themes and sub-themes. In phase 5 the identified themes were defined and named. The 6th and final phase consisted of producing the report.
Trustworthiness
The trustworthiness of the study was addressed by looking at four principles namely credibility, transferability, dependability and confirmability25. Credibility was ensured during the data collection process by making sure that the researchers used peer debriefing continuously. The researchers also developed an increased sensitivity to the participants' experiences through prolonged engagement and persistent observation during the research process as suggested Novell et al 26. The research group of six communicated multiple times daily during data collection and met weekly during data analysis.
Dependability was promoted in that the researchers provided an in-depth description of the research process. The process was logical and clearly documented. This was done to familiarise readers with the process that was followed for them to make a judgement on the dependability of the study. To promote potential transferability, the researchers provided a clear and comprehensive description of the contexts of the participants in the research report as well as the findings. Therefore, readers can make their own judgement on the transferability of the study to their specific context.
Confirmability aims to ensure that the results obtained
could be confirmed by others26. This was facilitated by making use of reflexivity. The regular communication between all members of the research group and weekly group meetings enabled the researchers to reflect on their role in the research.
Ethics
Ethics approval (number 800/2020) was obtained from the Research Ethics Committee at the University of Pretoria which complies with ICH-GCP guidelines and has US Federal wide assurance. The fundamental ethical principles used in this study were: respect for persons, beneficence and justice27. The participants had the right to autonomy, through informed consent and voluntary participation. It was ensured that the participants were aware of their right to withdraw at any time during the study without negative consequences. All data collected during the focus group remained confidential and any identifying information was omitted during the process of data analysis.
FINDINGS
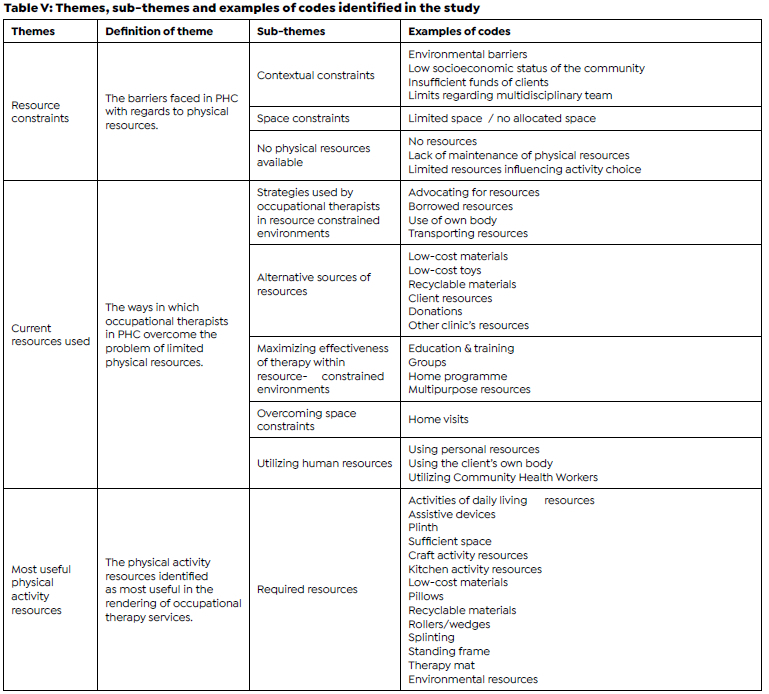
Three themes emerged during the process of data analysis. Table V (above) provides the definition of each of the themes, the subthemes and examples of codes included under each theme.
Theme one precedes the findings for the research objectives. To explore the resource needs of occupational therapists in PHC settings in Gauteng, it is important to first understand the resource constrained contexts of the participants.
Theme 1: Resource constraints
The first theme that emerged was resource constraints experienced in PHC workplaces. Several participants asserted that they had few physical resources and limited space available in their PHC setting, often compromising the extent of the services that they were able to render. The lack of physical activity resources acted as a barrier to occupational therapy services.
"This lack of space and limited equipment often prevented us from providing the best intervention we could to each client we saw" (P6, an occupational therapist working in urban and rural environments with less than three years of experience).
"I want to mention that we outreach to another clinic where we have nothing, and our rehab team (physio, OT, social worker, and STA) share one consultation room. At our 'main' clinic and outreach clinic space is really making it difficult to render services. ... It is also difficult to take all our equipment to our outreach clinic, so often we do not have anything to use" (P5, an occupational therapist with less than three years of experience, working in a rural setting).
Limited space as a resource constraint seemed to be the most problematic barrier faced by the participants in their PHC settings.
"A big problem within most of the clinics where I worked was space. Often, we were pushed into small offices and there was no equipment available" (P6)
Theme 2: Current resources and strategies used
The second theme that was identified highlighted the ways in which occupational therapists make adaptations to therapy in order to reach the same goal despite resource constraints. The findings show that there are many different sources of physical activity resources that occupational therapists use when activity resources are not available at the facility where they are employed. Two participants describe having to borrow or share resources from nearby clinics as well as having to transport resources such as wheelchairs when travelling between clinics.
"We are coping with what we have, but if the other clinic takes back the equipment, we will need similar equipment for muscle strength and ROM exercise" (P5)
"... we had to travel with equipment and often up to 5 wheelchairs in a car to ensure that we could provide intervention to our clients" (P6)
Due to the limited space, many therapists either did therapy outside or preferred to do home visits instead. Participant 4 (an occupational therapist working in urban and rural areas with more than 10 years of experience) said:
"We have limited space in all the clinics that I service. This contributes a lot to the choice of activities that I use for groups. We do our activities outdoors because there is no space indoors".
"I do home visits to compromise for lack in space" (P5, a participant that has to share the therapy room she has access to with other professionals)
Participant 8 (with less than three years of experience) faced the same problem:
"... if anything I think my greatest challenge is the lack of enough space. I could always hold some parts of sessions outside".
Due to resource constraints, some therapists have to get creative by using environmental resources such as sand or stones. Participant 1 (with more than 10 years of experience working in an urban environment) said:
"I have to add, that being based in the community, I often have to use everyday objects for therapy. I've used rice grains, pasta, pegs, beans, wool, cotton wool and also flour from home. Even sand".
The other noise makers we and students have made, using toilet rolls filled with stones, sand, rice, etc. (P2, an occupational therapist with between 5 and 10 years of experience, working in urban and rural contexts)
"... bottles filled with sand for weight, balls sometimes we use old clothes to make one".(P4)
Within this theme the adaptability and innovativeness -particularly of more experienced participants - became evident. The participants described using recyclable and low-cost materials as physical activity resources.
"I use low cost recycled materials, such as the bottle caps, tins, toilet rolls, take away containers, etc. I have also used cut off pieces of sponge (leftover from the Buggy seatings) to do stacking activities, sorting them according to shape, size and colour. The toilet rolls are so versatile! I use them to make shakers, 'binoculars' for visual acuity, rolling them to one another, I cut them into smaller circles that can be used for threading necklaces... I have also used them as stamps by dipping the edges into paint and then stamp circles onto paper" (P2)
"So, I use stacking cups, wooden blocks, plastic bottle caps in various colours, plastic buckets for sorting, large, coloured beads, matching games and cards, scrap paper and crayons, and threading shapes and shoelaces" (P1)
Participant 2 took further initiative by organizing a fundraiser with her students:
"We received a donation of soft toys a few years back, which another group of students, as part of their project, sold to do fundraising for needed resources. With the funds they bought blocks, noise makers, small flashlights, ingredients to make homemade playdough with, rice, beans, bean bags, and cellophane".
Many participants have relied on donations from organizations and fellow colleagues.
"I am also fortunate to have access to ., which provides resources to therapists in need if it helps in any way with patient services or therapy". (P3, an occupational therapist with less than three years of experience, working in the urban environment)
"I also was aware of getting access to free/scrap materials in the hospital and my own community and encouraged other colleagues to bring second hand items which they weren't using, such as an old baggy t-shirt for dressing activities" (P7, an occupational therapist with less than three years of experience working in a rural context)
Other therapists asked patients to bring their own equipment and materials to use during therapy.
"For the ADL activities I will ask everyone to bring shoes with laces, a shirt with buttons, etc." (P2)
"I also took my own equipment such as blocks and cars as this was not available at the clinics. I learned that it is important to be adaptable and context specific within therapy therefore I also asked caregivers to bring the toys they have available at home." (P6)
Theme 3: Most useful physical activity resources
The third theme created was the physical activity resources identified as most useful in the rendering of occupational therapy services. Certain objects, equipment, tools and resources seemed to stand out amongst others, either for being very useful and often utilized in the participants' context or for creating a strong barrier in the absence of the object or resource.
Naturally, the absence of space proved to be the barrier most often faced by the participants as described in theme one.
"I must first have space and then the rest will follow (P4, occupational therapist working in urban and rural areas without access to an occupational therapy treatment room), implying that space forms the foundation for the rendering of occupational therapy services".
Furthermore, many participants mentioned that they desire to have more resources that are used in rehabilitation for clients who face difficulties within their basic and instrumental activities of daily living.
"Tools and equipment ... to be able to engage in occupation [sic] such as BADL and IADL like cooking, activities to be used for leisure ..." (P5)
"I would have liked ... more ADL tools, such as clothes, kitchen equipment, etc. as most of the kitchen equipment were [sic] missing or broken" (P6)
Assistive devices and Bobath plinths were often mentioned by the participants. Assistive devices were either often used by the participants or solutions had to be found to compensate for the absence of these assistive devices.
"For example, I often used rolled-up bed sheets or blankets for positioning or educated families on what they could make or buy at home" (P7)
"... we had to travel with equipment and often up to 5 wheelchairs in a car to ensure that we could provide intervention to our clients" (P6)
"I use the physio mats and physio balls, rollers and wedges during our developmental delay group ... I use the paediatric standing frame as well, especially when the physio and I have joint sessions. This works extremely well to reach our objectives together" (P2)
"I often made use of a Bobath plinth, ... and wheelchairs or walking frames ..." (P6)
"I also very often make use of the therapy mats and Physio ball for gross motor activities" (P2)
The physical activity resources that were most often discussed were recyclable and low-cost materials. It is exactly these resources that are creatively utilized by occupational therapists when typical resources are not available.
"I use the bottle caps to do sorting activities - size and colour sorting. The tins I use for stacking, as well as using them to sort the caps into. ... I also bring things from home sometimes but try to recycle/upcycle 'trash' to make low cost toys with. I also brought a bunch of old magazines to the clinic to use during therapy" (P2)
"I make use of ... different coloured plastic bottles with matching rings, ... chalk to draw a tandem line (for dynamic balance)" (P8)
These recyclable and reusable items are found to be distinctly valuable in the under-resourced practice contexts in which the participants render therapy.
DISCUSSION
Firstly, the findings suggest that the PHC practice contexts where the participants are employed are under-resourced. This supports previous studies where participants have highlighted the limited physical resources they have available to provide rehabilitation services in PHC12,14. The available space as well as the objects, tools and materials needed are important considerations in the activity selection and professional reasoning process9. Therefore, limited access to space and other physical activity resources will invariably influence the intervention provided by therapists.
Not surprisingly, several participants in this study experienced the limited availability of physical resources as a barrier to their service provision in PHC. Inexperienced therapists have been described to experience the influence of aspects pertaining to the environment (such as available resources) as more influential on their practice than more experienced therapists28. Experienced therapists are said to view environmental factors not so much as barriers, but rather as merely among the many factors to be considered in the professional reasoning process29. As most participants in this study were relatively inexperienced, this may - at least in part - have contributed to the experience that resource constraints were such a barrier.This insight is important for managers to keep in mind when supervising and managing inexperienced professionals (that often work in PHC) to guide them to develop the ability to recognise the opportunities and strengths within the resource constrained PHC context.
Aspects pertaining to the resource limitations as reported in Theme 1 enable the reader to understand the context in which the participants work. Reporting on the context is important in order to increase the potential transferability of the findings to other contexts. Therefore Theme 1 essentially preludes the objectives of this study that aimed to identify the resources and strategies that occupational therapists in PHC utilise and those physical activity resources they deem to be most important to ensure effective services can be provided.
Several authors5,7, 12,14 have called for adequate resources for rehabilitation. It is hoped that the findings reported in Themes 2 and 3 will assist managers to advocate for additional resources for occupational therapy services in PHC.
Theme two indicates the resources and strategies that occupational therapists in PHC currently use. This theme answers objective 1 of this study (current resources used). The resources consist of a combination of typical occupational therapy resources and unconventional resources used to compensate for limited resources. Invariably linked to the resources used at the time of this study are the strategies occupational therapists utilise to adapt to the limited resources in their practice context. Contexts with limited resources appear to create opportunities for creativity and resourcefulness. The adaptability and resourcefulness of therapists have also been reported by van Niekerk 6.
The use of recyclable materials was highlighted as an important resource. The use of recyclables aligns with sustainable and environmentally responsible practice30. By linking with established community recycling projects or developing such projects can provide occupational therapists with the required recyclable resources for their practice and support participants in the recycling projects.
Importantly, students should be trained to provide services in resource constrained environments during their studies. Lorenzo et al. reported that there is a misalignment between undergraduate training and the demands of PHC contexts31. This corresponds with van Stormbroek and Buchanan's research in which a participant stated that they felt that most of the training they received during undergraduate studies was difficult to apply in a resource-constrained environment14. Training undergraduate students to be adaptable and resourceful may better enable inexperienced community service therapists to cope with the challenges posed by the PHC context.
The second objective was to explore which physical activity resources occupational therapists deem necessary in order to provide adequate intervention in their specific context. This objective is primarily answered by Theme 3. However, without the availability of the resources mentioned in theme 2, the possibility of rendering adequate intervention in resource-constrained contexts would be substantially limited. These resources, first and foremost, include space, basic and instrumental activities of daily living resources, assistive devices, plinths, recyclable and low-cost materials. These resources cannot be compensated for, as they have been identified as either most useful within occupational therapy intervention or are used by occupational therapists to overcome resource barriers.
Limitations
The study had a limited sample size. There are few PHC clinics in Gauteng and many of these facilities do not employ occupational therapists. A second focus group was conducted due to the attrition in the first focus group. The target population was sampled as planned, but the findings of this study cannot be generalised and do not reflect the situation in any of the other 8 provinces in South Africa. Additional limitations included that participants were difficult to recruit and had limited time available to participate in the study.
CONCLUSION
The consideration of physical activity resource demands during professional reasoning is an integral part of planning intervention. In the absence of physical activity resources such as objects and space, occupational therapists may experience various barriers related to their professional identity and self-esteem15. It is evident that the PHC context is under-resourced compelling occupational therapists to use unconventional resources to overcome contextual barriers. Certain physical activity resources have been identified to be particularly useful in occupational therapy intervention in PHC.
This study is relevant to the clinical practice of occupational therapy in that it contributes to the body of knowledge regarding the physical activity resource needs of occupational therapists in PHC. The research may contribute to the preparation of newly qualified occupational therapists for the PHC context. It further creates a base of knowledge from which future studies can be conducted regarding what occupational therapists regard as essential resources in PHC as well as studies on how available funds can be maximised.
Acknowledgement
The authors would like to extend our sincerest gratitude to all the participants for their insightful, valuable and in-depth contributions made towards this study.
Authors' contributions
Karin van Niekerk was the supervisor of the study and conceptualised the study. She guided design of the study, performed the data collection, and assisted with data analysis and interpretation and edited the manuscript. Sabrina Raquel da Silva, Clarette Swart, Marnique Hugo, Zolani Phiwokuhle Flatela, and Ansa Janse van Vuuren were investigators in this study and were responsible for the study design, sourcing relevant literature, recruiting participants, analysing the data and interpretation of the results. They were primarily responsible for drafting of the manuscript.
Conflicts of interest and bias declaration
The researchers declare no conflicts of interest. The views expressed in the article are the authors' own and not an official position of the relevant institution.
REFERENCES
1. World Health Organization, UNICEF. Declaration of Alma Ata. International Conference on Primary Health Care. Alma-Ata, Ussr, 6-12 September 1978.Social Medicine:1978; 2(1):42-43 [Accessed 2 July 2020]. https://www.who.int/publications/almaata_declaration_en.pdf?ua=1 [ Links ]
2. Naidoo D, van Wyk J, Waggie F. Occupational therapy graduates' reflections on their ability to cope with primary health-care and rural practice during community service. South African Journal of Occupational Therapy.2017; 47(3):39-45. doi:http://dx.doi.org/10.17159/2310-3833/2017/v47n3a7 [ Links ]
3. National Department of Health. Framework and Strategy for Disability and Rehabilitation Services in South Africa 2015-2020. 2015. [Accessed June 2022] Available from: http://ilifalabantwana.co.za/wp-content/uploads/2016/07/Framework-25-may_1_3.docx [ Links ]
4. Gimigliano F, Negrini S. The World Health Organization Rehabilitation 2030-a call for action. European Journal of Physical and Rehabilitation Medicine. Eur J Phys Rehabil Med. 2017; 53: 155-168. doi:https://doi.org/10.23736/s1973-9087.17.04746-3 [ Links ]
5. Morris L. D , Grimmer K. A , Twizeyemariya A , Coetzee M , Leibbrandt C. D , Louw Q.A. Health system challenges affecting rehabilitation services in South Africa. Disability and Rehabilitation. 2021; 43(6):877-883, doi: https://doi.org/10.1080/09638288.2019.1641851 [ Links ]
6. van Niekerk K , Dada S, Tönsing K. Influences on selection of assistive technology for young children in South Africa: perspectives from rehabilitation professionals. Disability and Rehabilitation. 2019; 41(8):912-925, doi: https://doi.org/10.1080/09638288.2017.1416500 [ Links ]
7. Sherry K. Disability and rehabilitation:Essential considerations for equitable, accessible and poverty-reducing health care in South Africa. Disability and Rehabilitation. 2014; 7:89-99. doi: https://hdl.handle.net/10520/EJC189294 [ Links ]
8. Reid S. Community service for health professionals: human resources. South African health review. 2002;2002(1):135-160. doi:https://10520/EJC35385 [ Links ]
9. Boyt Schell B. Gillen G. Scaffa ME. In: Barbara A. Boyt Schell B.Gillen G. Scaffa ME. Chapter 30, Professional Reasoning in Practice. In: Willard & Spackman's Occupational Therapy. 12th edn. Ellen S. Cohn, Consulting Editor. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2014: 393-395. [ Links ]
10. American Occupational Therapy Association. Occupational Therapy Practice Framework: Domain and Process. The American Journal of Occupational Therapy. 2020; 74(2): 1-87. doi:https://doi.org/10.5014/ajot.2017.74S3offdoc [ Links ]
11. Maseko JL, Erasmus A, Di Rago T, Hooper J, O'Reilly J. Factors that influence choice of placement for community service among occupational therapists in South Africa. South African Journal of Occupational Therapy. 2014; 44(1):36-41. [ Links ]
12. van Stormbroek K, Buchanan H, Novice occupational therapists: Navigating complex practice contexts in South Africa. Australian Occupational Therapy Journal. 2019; 66(4): 469-481. doi:https://doi.org/10.1111/1440-1630.12564 [ Links ]
13. Toal-Sullivan D. 'New Graduates' Experiences of Learning to Practise Occupational Therapy. British Journal of Occupational Therapy. 2006; 69(11):513-524. doi: https://doi.org/10.1177/030802260606901105 [ Links ]
14. van Stormbroek K, Buchanan H. Community service occupational therapists: thriving or just surviving? South African Journal of Occupational Therapy. 2016;46(3):69. doi: http://dx.doi.org/10.17159/23103833/2016/v46n3a11 [ Links ]
15. De Beer LT, Pienaar J, Rothmann S. Job Burnout, Work Engagement and Self-reported Treatment for Health Conditions in South Africa. Stress and Health. 2014;32(1):36-46. doi:https://doi.org/10.1002/smi.2576 [ Links ]
16. Lambert VA, Lambert CE. Qualitative Descriptive Research: An Acceptable Design. Pacific Rim International Journal of Nursing Research. 2012 October- December.;16(4):255-256. doi:https://he02.tci-thaijo.org/index.php/PRIJNR/article/view/5805 [ Links ]
17. Stewart DW. Shamdasani PN. Rook DW. Chapter 3, Focus Groups and the Research Toolbox. In: Focus Groups. 2nd edn. Thousand Oaks, CA: SAGE Publications, Ltd;2007:37-50. doi:https://dx.doi.org/10.4135/9781412991841.d16 [ Links ]
18. Brink H, van der Walt C, van Rensburg G. Fundamentals of Research Methodology for Healthcare Professionals. 4th edn. Cape Town: Juta and Company (Pty) Ltd; 2018. [ Links ]
19. Krueger RA, Casey MA, Chapter 4, Participants in a Focus Group. In: Focus groups: A practical guide for applied research, 5th ed. Thousand Oaks, California: Sage Publications Inc; 2015:77-102. doi:https://doi.org/10.2307/3172912 [ Links ]
20. Gordon AR, Calzo JP, Eiduson R, Sharp K, Silverstein S, Lopez E, et al. Asynchronous Online Focus Groups for Health Research: Case Study and Lessons Learned. Int J Qual Methods. 2021;20:1-13. https://doi:10.1177/1609406921990489 [ Links ]
21. Zwaanswijk M, van Dulmen S. Advantages of asynchronous online focus groups and face-to-face focus groups as perceived by child, adolescent and adult participants: a survey study. BMC Research Notes. 2014;7:756. doi:https://doi.org/10.1186/1756-0500-7-756 [ Links ]
22. LaForge K, Gray M, Stack E, Livingston CJ, Hildebran C. Using Asynchronous Online Focus Groups to Capture Healthcare Professional Opinions. Int J Qual Methods. 2022;21:1-9. doi: https://10.1177/16094069221095658 [ Links ]
23. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology.2006; 3(2):77-101. doi:https://10.1191/1478088706qp063o [ Links ]
24. Vaismoradi M, Turunen H, Bondas T. Content analysis and thematic analysis: Implications for conducting a qualitative descriptive study. Nursing Health Sciences. 2013;15(3):398-405. doi:https://doi.org/10.1111/nhs.12048 [ Links ]
25. Shenton AK. Strategies for ensuring trustworthiness in qualitative research projects. Education for Information. 2004; 22(2):63-75. doi: https://10.3233/EFI-2004-2220 [ Links ]
26. Nowell LS, Norris JM, White DE, Moules NJ. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. International Journal of Qualitative Methods. 2017; 16:1-13. doi: https://doi.org/10.1177/1609406917733847 [ Links ]
27. Department of Health, Education, and Welfare, & National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research.The Belmont Report: Ethical principles and guidelines for the protection of human subjects of research. 1979 [accessed 11 June 2022]. https://www.hhs.gov/ohrp/sites/default/flles/the-belmont-report-508c_FINAL.pdf [ Links ]
28. van Niekerk K. Perspectives of rehabilitation professionals on assistive technology provision for young children with disabilities in South Africa. University of Pretoria; 2019. [ Links ]
29. Schell BA, Cervero RM. Clinical reasoning in occupational therapy: An integrative review. Am J Occup Ther. 1993;47(3):605-10. [ Links ]
30. Smith DL, Fleming K, Brown L, Allen A, Baker J, Gallagher M. Occupational Therapy and Environmental Sustainability: A Scoping Review. Annals of International Occupational Therapy. 2020; 3(3): 136-143. doi: https://doi.org/10.3928/24761222-20200116-02 [ Links ]
31. Lorenzo T, Duncan M, Buchanan H, Alsop A. Practice and Service Learning In Occupational Therapy: Enhancing Potential In Context. Chichester: Whurr Publishers Limited; 2006:1-50. [ Links ]
 Correspondence:
Correspondence:
Sabrina Raquel da Silva
sabrinads97@gmail.com
Received: Febreuary 2022
Peer review: april 2022
Revised: July 2022
Accepted: September 2022
Published: April 2023
Editor: Hester van Biljon: https://orcid.org/0000-0003-4433-6457
Funding: No funding was obtained to conduct this research


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}