










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.53 n.1 Pretoria Apr. 2023
http://dx.doi.org/10.17159/2310-3833/2023/vol53n1a4
RESEARCH ARTICLE
Development and evaluation of face and content validity of a survey to examine wound management by occupational therapists in hand therapy practice within the South African context
Lezane EsterhuizenI; Pragashnie GovenderII; Deshini NaidooII
IGauteng Department of Health, South Africa. https://orcid.org/0000-0001-8237-5890
IIOccupational Therapy, College of Health Sciences, University of KwaZulu- Natal, South Africa. Pragashnie Govender: https://orcid.org/0000-0003-3155-3743; Deshini Naidoo: https://orcid.org/0000-0001-6276-221X;
ABSTRACT
BACKGROUND: Wound management is internationally recognised as part of hand therapy practice. However, the role of occupational therapists in this area of upper limb rehabilitation in South Africa is unclear
AIM: To develop and validate a survey to examine occupational therapists' wound management practices in hand therapy within the South African context
METHODS: A sequential exploratory mixed methods study design was utilised to develop a survey. Thereafter, a panel of 11 occupational therapists with relevant experience in the field rated the relevance of survey items to produce item-content validity indices (I-CVIs
RESULTS: An initial survey containing 27 questions containing 214 items was presented for review. Experts rated 171 items (69%) relevant with an I-CVI of 0.90-1.00. A further 32 items (13%) were rated relevant with an ICVI of >0.80 <0.90. A total of 45 items (18%) were irrelevant with I-CVIs <0.80. The final survey consisted of 19 questions containing 139 items, excluding those that obtained relevant demographic data
CONCLUSIONS: The survey demonstrated good content and face validity but is limited to use with occupational therapists in South Africa. Validation for use with different populations in different settings is recommended
Implications for practice
This article offers researchers within the field of occupational therapy methodology for the development and validation of a survey. Suggestions for improving the overall validity of the survey are given. The survey may be used in future studies with occupational therapists providing hand injury care in South Africa. Use of the survey with different populations requires validation using the intended target population.
Keywords: hand injuries, developing country, instrument development, research tool, survey development, survey review
INTRODUCTION
Wound management is internationally recognised as part of hand therapy practice1,2. The hand therapy practice profile, as presented by the International Federation of Societies for Hand Therapy, outlines wound management as a specialist therapeutic skill1. Furthermore, the American Society of Hand Therapists' position paper on hand therapists' scope of practice outlines that hand therapists assess characteristics of the wound and the impact of activities and positioning of the hand on wound healing2. A survey conducted with hand therapists across sixteen countries to determine contemporary upper limb rehabilitation practices further supports that wound management activities are part of holistic intervention3.
In South Africa, formal hand therapy accreditation is not a requirement for practice. Even though there is a demand placed on occupational therapists within the South African context to treat complex upper limb injuries4, there is limited literature on the practice profile or core skills for hand therapy practice in the country, including wound management.
Compared to global statistics, South Africa has a very high burden of injury5. Although statistics on the burden of hand injuries in South Africa are limited compared to global statistics, South Africa has higher rates of interpersonal violence and road accidents6, which have been reported to contribute to a greater prevalence of hand injuries7. High rates of hand injuries in a population of manual labourers contribute to hand injuries in a South African state hospital8. These work-related injuries, together with traumatic injuries8, firework-related hand injuries9 and tendon injuries10 treated in South African hospitals, indicate a high prevalence of hand wounds. Anecdotal evidence based on the first authors experience and engagement with colleagues in the field further suggests that in practice, occupational therapists in South Africa regularly encounter hand wounds during therapy interactions with patients with hand injuries.
The views of practising occupational therapists on their role in wound management in hand therapy within the South African context have not been determined. Furthermore, an in-depth investigation of the practices of occupational therapists in providing interventions related to wound management to hand injured patients and their level of preparedness to manage hand wounds in South Africa has not been conducted. Given the unique context, a need to examine wound management in hand therapy within the South African context was identified.
The authors developed a survey following similar stages to those reported by other scholars11 that involved reviewing relevant literature, conducting individual semi-structured interviews, thematic analysis of qualitative data, initial item generation, and review of generated items. To ensure the reporting of credible research findings, consideration was given to the rigorous development of the survey12. It is well understood and documented that drawing accurate and valid inferences from research findings relies upon the instrument's validity, in this case, the survey and that in the absence of rigorous development, the credibility of reported results may be disputed12, 13, 14, 15, 16.
The use of mixed methods research, in which qualitative data informs item generation, for developing an appropriate survey has been documented by authors such as Onwueg-buzie and colleagues17. Using qualitative findings to inform item generation enhances the survey's content validity11, 13, 16-19. Using qualitative findings enhances the value of generated items as they are obtained from the population of interest and reflect their opinions, perspectives, perceptions and experiences11, 16, 18.
The evaluation of generated items by individuals who are part of the target population and who are considered knowledgeable in the field is documented as a further means to enhance the overall validity of a survey11, 13, 18, 20-22. Qualitative feedback on the acceptability of a survey is a means to ensure face validity23, which has been described as the extent to which the items appear relevant, important, and interesting to the respondent17 (p,60). A described method of content validation by quantitative review involves rating the relevance of items to produce a content validity index (CVI) for each item11, 13, 22. Content validity has been described as the relevance and representativeness of items in an instrument for its intended setting and purpose11, 20. The minimum requirements for excellent content validity of an instrument, as reported by Pilot and Beck24 are I-CVIs >0.78 for a panel of six or more reviewers and a scale level CVI (S-CVI), calculable by adding the I-CVIs and dividing by the number of items to obtain an average, >0.90.
The aim of this paper is to describe the development of a survey for use with an occupational therapy population to examine wound management in hand therapy within the South African context. The process of evaluating the face and content validity of the survey by both qualitative and quantitative review by occupational therapists knowledgeable in the field is described in detail. Other aspects of validity, construct validity, were not assessed.
MATERIALS AND METHODS
Process for survey development
The survey was developed in two stages: initial item generation and survey review. A sequential, exploratory mixed methods study design informed the development of the survey25. The process of using qualitative data for the development of a quantitative data collection tool - the survey - is described in detail in this paper.
Study setting
The survey was developed for use with occupational therapists providing interventions to patients with hand injuries in South Africa. South Africa has a total population of 57,73 million within nine provinces. Both public and private health care are available in South Africa.
Stage one: Initial item generation
Relevant literature and qualitative data from individual interviews with occupational therapists with appropriate work history and experience in the field of hand therapy informed the generation of initial survey items. Expert opinion was used as a source of information due to the dearth of evidence of the role of occupational therapy and current wound management practice in South Africa.
Review of relevant literature: Given that the purpose of the survey was to examine wound management with specific reference to hand injuries, literature on wounds resulting from pressure sores or ulcers and burn injuries was excluded from the review. A literature search was conducted using Google Scholar, and literature on the role of occupational therapy and current practice in wound management in hand therapy was identified. A minus sign is used in search strings to specifically exclude a word or phrase from the search, in this case burn, pressure and ulcer. The following are sample search strings that yielded the highest number of relevant results: 'occupational therapy OR therapist' AND 'wound treatment' -ulcer -burn; 'Hand therapy OR therapist' AN D 'wound management OR care' -pressure -ulcer; 'certified hand therapy OR therapist' AND 'wound management OR care'; 'hand rehabilitation' AND 'wound management OR care' -burn -pressure -ulcer; 'occupational therapy OR therapist' AND 'wound management OR care' AND 'Injured hand OR hands'; 'hand rehabilitation' AND 'wound management OR care' AND 'hand injury OR injuries'. Items were drawn from a position paper brought forward by the American Occupational Therapy Association (AOTA)26, which describes the role of occupational therapy in wound management, to partly examine what occupational therapists in South Africa perceive their role to be. Further items drawn from this paper were specified interventions that occupational therapists may perform to ameliorate wounds that AOTA states to be within the scope of practice of occupational therapists in United States of America. These were utilised in the survey to determine the wound care activities used by occupational therapists in South Africa to facilitate wound healing in patients with hand injuries. Specified interventions for wound healing as discussed by Keller et al.3 were further used to augment this section of the survey. These interventions were further used to partly inform specific areas of inquiry within the survey addressing the confidence of occupational therapists in using wound management interventions and when they acquired the knowledge and skill for using such interventions. Findings reported in Keller et al's3 study, also partially informed response scales in the survey examining when and how occupational therapists acquired the expertise to use wound management interventions.
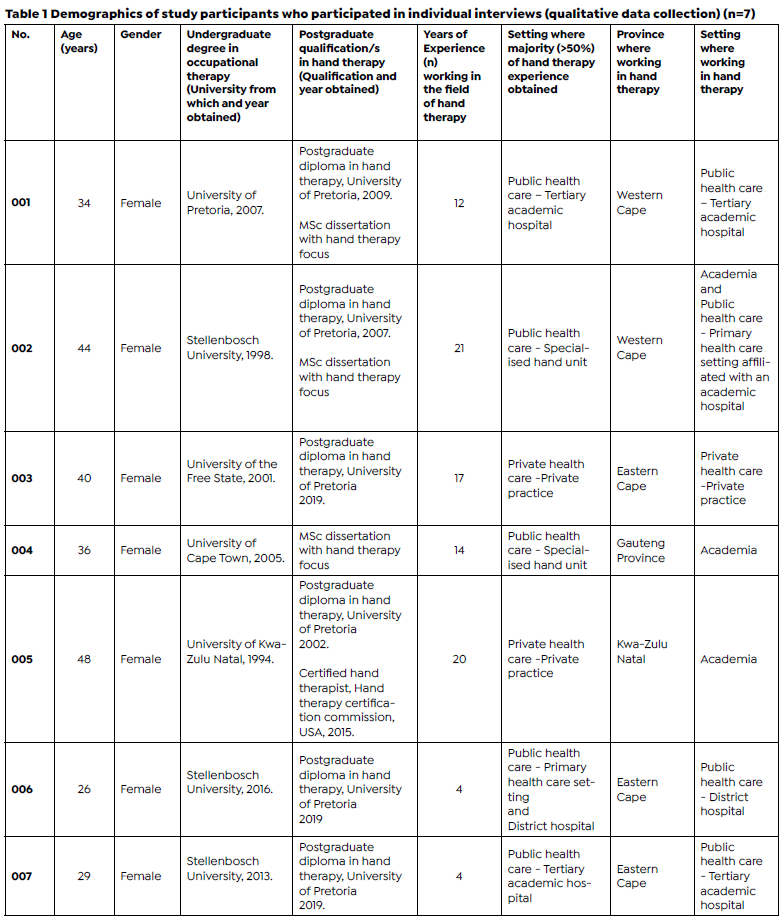
Qualitative data from individual interviews: A semi-structured interview guide was constructed following phases of development described by Kallio and colleagues27. Non-probability purposive sampling28, 29 was utilised to select knowledgeable and experienced participants in the South African context of hand therapy. Maximum variation sampling29, a purposive sampling technique, was employed to obtain varying points of view on the role of occupational therapy in wound management in hand therapy. Semi-structured interviews were conducted with seven occupational therapists meeting the predetermined selection criteria. The inclusion criteria were (i) qualified occupational therapist; (ii) registered with the HPCSA; (iii) working in the field of hand therapy and/ or an academic in the field of hand therapy; (iv) holds postgraduate qualification/s in hand therapy or has more than 15 years of experience in the field of hand therapy. In the view of the authors, holding a post-graduate qualification in hand therapy indicated that the individual participant would have the relevant experience in the field as post-graduate courses require that therapists have experience in hand therapy to enrol. Therapists also need to be treating hand injured patients throughout the course of their post-graduate studies. Occupational therapists who obtained the majority (more than fifty percent) of their expertise in hand therapy in a country other than South Africa were excluded. Interviews were conducted over a two-week period. Twenty occupational therapists were screened for eligibility, and 12 did not meet the selection criteria. Eight were invited to participate, and one occupational therapist declined due to reportedly not being involved in wound management in practice. Table I (page 23) illustrates the demographic profile of the participants. All (n=7) of the occupational therapists that were interviewed were female with a median age of 36 years (range 26-48 years). The median number of years of experience working in the field of hand therapy was 14 years (range 4-21 years). Postgraduate qualifications in hand therapy were held by all (n=7) of the participants. 71% (n=5) of the participants obtained most of their experience in hand therapy in public health care settings and 29% (n=2) in private practice. Participants hailed from four of the nine provinces in the country.
Interviews were audio-recorded and transcribed verbatim by the first author. Interviews focused on participants' views of the role of occupational therapy in wound management in hand therapy, the current wound management practices, and factors influencing the preparedness of participants to manage hand wounds. A thematic analysis30 of qualitative data from semi-structured interviews ensued by the first author. Debriefing with the second and third authors assisted in ensuring credibility31. The process of debriefing ensured that results were representative of data provided by participants32. An inductive approach allowed for data emerging from semi-structured interviews to inform the content of the survey (item-generation). Questions were structured, and items were grouped to reflect emerging themes. Qualitative data were used to identify factors related to specific areas of interest for which no literature was identified to draw on. For example, interviewed occupational therapists discussed factors that support or hinder their practice in the provision of wound management interventions to patients with hand injuries within their various practice settings, including access to supervision and mentorship and communication in the MDT. These factors were then used as items in the survey to determine to what extent a larger sample of the population experience these factors as barriers or enablers.
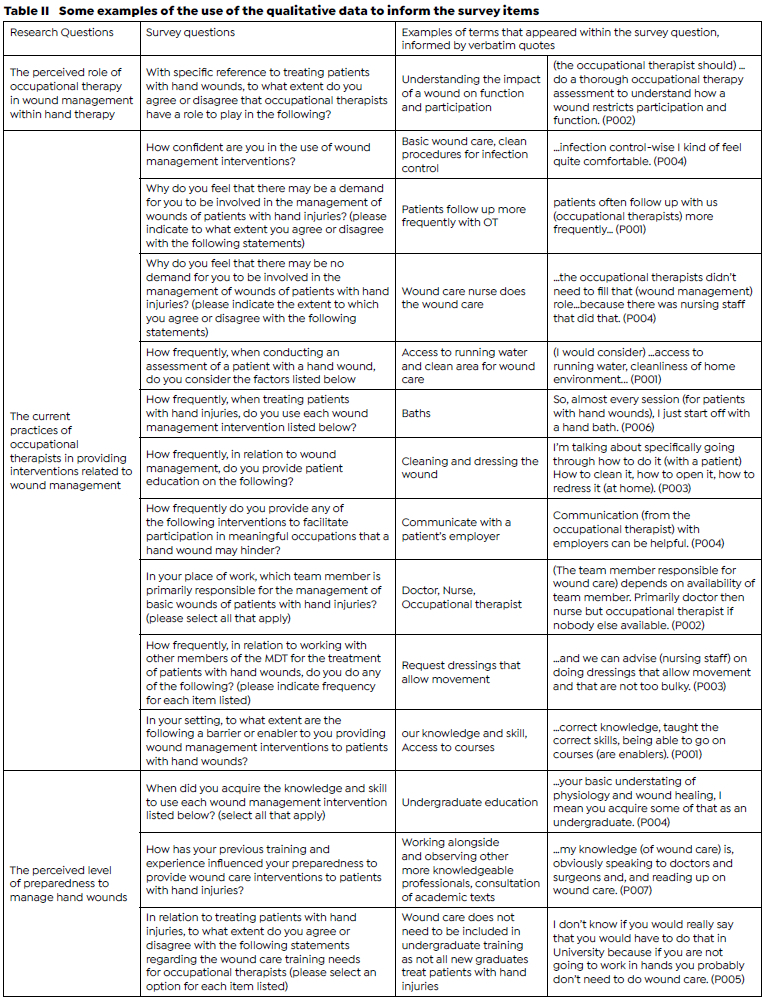
Data from the qualitative enquiry were also used to complement items drawn from literature. This enhanced the overall validity of the survey to obtain information from its intended target population. Items examining when occupational therapists acquired the knowledge and skill for the use of wound management interventions were developed using literature and findings from individual interviews. This also applied to items investigating any previous training and experience that might have influenced their level of pre-paredness for providing such interventions. Through using an inductive approach to thematic analysis, data were also used to further inform additional research objectives, such as examining the wound management training needs of occupational therapists, for example. Items generated from information provided in interviews were reflective of qualitative statements and included the language used by participants to enhance content validity18. Table II (page 24) illustrates the use of qualitative data to generate survey items. The survey, following development and review, contained 19 questions, excluding questions used to gather participant demographic data, and each question had several items included within. For example, question 15: With specific reference to treating patients with hand wounds, to what extent do you agree or disagree that occupational therapists have a role to play in the following? had 11 items, each requiring a response. Two item examples are cited: educating patients on wound care and providing sensory education to prevent wounds. Participants were required to select either agree, neither agree nor disagree, or disagree for each item in this question.
Stage two: Survey review
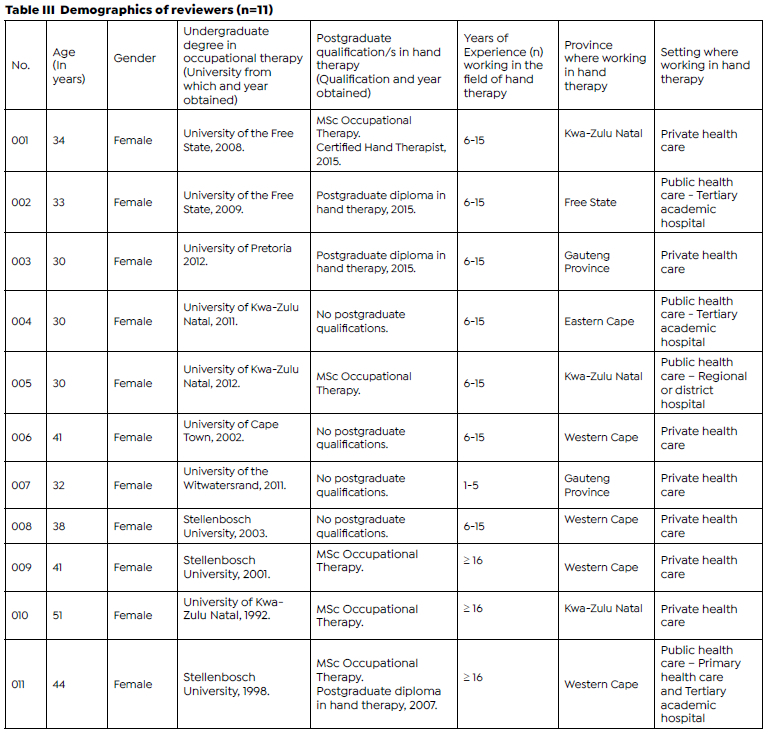
To assess the survey content and face validity, the initial pool of items was reviewed between a month period by a panel of occupational therapists meeting the predetermined selection criteria. Reviewers were more in number than those who participated in interviews for qualitative data collection and were not necessarily the same occupational therapists as those who were interviewed for initial item generation as mentioned in stage one. The inclusion criteria differed from the initial phase only in terms of two criteria, namely occupational therapists working in the field of hand therapy between 2015 and 2020 and those who held postgraduate qualification/s in hand therapy and/or had a minimum of five years' experience in the field of hand therapy. The exclusion remained as aforementioned. Reviewers were selected using non-probability maximum variation purposive sampling28, 29. A total of 27 occupational therapists were invited to review the survey, and 16 declined. A panel of 11 reviewers was acceptable as a minimum of three is recommended in literature24. Table III (page 25) illustrates the demographic profile of reviewers. 100% (n=11) of the reviewers were female with a median age of 34 years (range 30 - 51). 9% (n=1) had five years' experience in the field of hand therapy, and 91% (n=10) had six years or more experience. 64% (n=7) worked in private health care settings, and 36% (n=4) worked in public health care settings. Reviewers hailed from five provinces in the country. 36% (n=4) had obtained postgraduate qualifications in hand therapy, and 46% (n=5) held a Master's degree in occupational therapy. The panel (n=11) completed the survey online and provided quantitative and qualitative feedback which guided the survey revision prior to the presentation of the final survey.
Quantitative review: For review, survey questions and their related items were all considered items. Reviewers rated the relevance of each item within the survey on a four-point rating scale: 1-not relevant, 2-somewhat relevant, 3-quite relevant, 4-highly relevant24. A CVI calculation was used to determine the content validity of individual items (I-CVIs)13. The number of reviewers that rated an item as either quite relevant or highly relevant, thereby dichotomising the scale into relevant and not relevant, was divided by the total number of reviewers to produce an l-CVI for each item. For items to be considered relevant, they had to achieve a minimum l-CVI of 0.81, which is above the recommended CVI of 0.78 fora panel of six or more reviewers24. Items with an I-CVI of 0.80and lowerwere removed from the survey, except for two items (the reason for this is explained under survey review and validation below). Microsoft Excel was used to perform CVI calculations.
Qualitative review: Reviewers provided written feedback on the time necessary to complete the survey, the overall coherence of the content of the survey, the ease of using Google Survey as an online platform, any additional items identified as relevant for the survey, and any questions/items that were unclear orambiguous33. Reviewers were also invited with an open-ended question to provide any additional comments. All comments were considered forsurvey revision. Rating scales, demographic and work history information that was required were confirmed. Due to time constraints related to the predetermined quantitative data collection timeframe, the survey was not resubmitted to the panel following revision.
Ethical considerations
Ethical clearance for the study was obtained from the Biomedical Research Ethics Committee (approval number: BREC/00001029/2020) of the University of KwaZulu-Natal.
Participant confidentiality was ensured by de-identification of personal identifying information, and informed consent was obtained from all participants.
RESULTS
Survey description
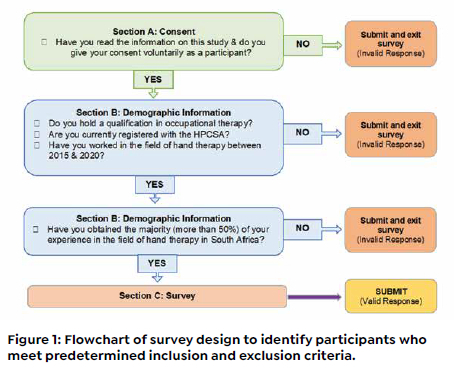
A self-administered electronic survey was developed using Google Forms, a survey administration application. The final survey presented for use in the study consisted of three sections indicated with headings to make the flow of the survey easy to follow. Section A obtained informed consent. Section B covered relevant demographic and work history, including information pertinent to identifying participants meeting the predetermined selection criteria for participation in the study. Qualitative feedback from a panel of reviewers led to minor changes to the demographic and work history information, including information related to the work setting within which therapists primarily provide wound care interventions. Before review, the survey inquired if participants work in the public or the private health care sector, for example, and reviewers indicated that allowance should be made for both as therapists may work in both sectors. Demographic information finally included respondents age, gender, undergraduate qualification information, registration status with the HPCSA, postgraduate qualification information, history of work experience, and information on respondents' work setting. Figure 1 (below) illustrates the flow of questions to identify individuals that did not meet the criteria who were then redirected to submit (exit the survey).
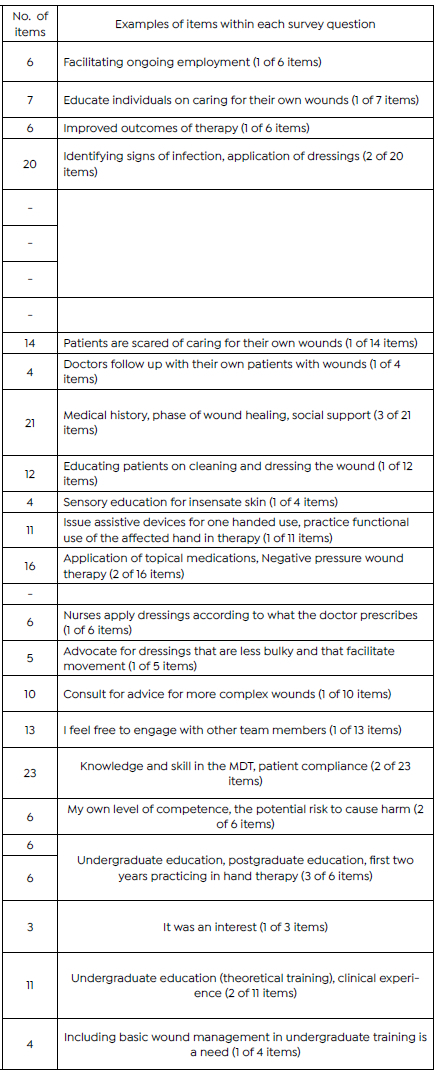
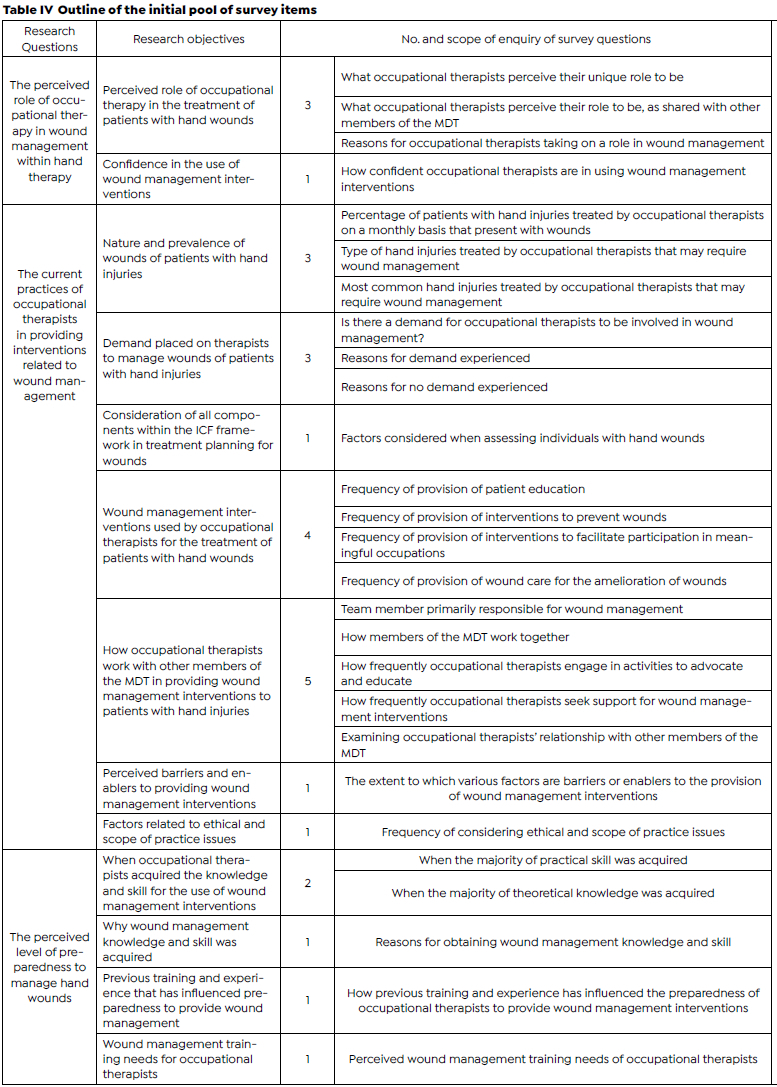
Section C captured information relevant to the purpose of the study. Survey questions were categorised according to different fields of inquiry related to the research objectives. Response types included closed multiple choice and checkbox answers, scaled items as well as open short answers allowing for elaboration, justification or specification33. All questions apart from the latter required a response. Following initial item generation, this section consisted of 27 questions containing a total of 214 items both drawn from literature as well as qualitative data obtained from interviews and a further seven items prompting respondents to clarify, specify or elaborate upon their answers within specific fields of inquiry, as outlined in Table IV (page 26). Following a review of the initial survey, the number of questions in section C was reduced to 19, containing a reduced number of 139 items.
Survey review and validation
Quantitative review
An I-CVI was calculable based on reviewer ratings of the relevance of individual items24. To calculate I-CVI's, individual questions and their related items were all considered items. Reviewers agreed that 203 items (82%) were relevant. A total of 171 items (69%) were awarded an I-CVI of 0.90 - 1.00, of which 129 (52%) were awarded an I-CVI of 1.00. A further 32 items (13%) were deemed relevant with an I-CVI of >0.80 <0.90. 45 items (18%) were considered irrelevant, having an I-CVI <0.80. These items were not revised and resubmitted to reviewers for re-evaluation. The majority, 43 items (I-CVI = 0.56-0.80), were removed from the survey. One question with an I-CVI of 0.75 remained as all four related items had I-CVIs of 1.00. A second question with an I-CVI of 0.75 remained as nine associated items had an I-CVI of either 0.90 or 1.00. Following the removal of 43 items, further revision of the survey was guided by reviewer commentary and feedback from the second and third authors.
Qualitative review
Reviewers provided commentary on the use of language and items that were unclear, ambiguous, repetitive or redundant. They also suggested items that they deemed relevant but were missing from the survey and items for removal. They further provided feedback on demographic information to be obtained and one confusing response scale. All comments were considered whilst finalising the survey.
Reviewers made several suggestions regarding the use of language. For example, with reference to the frequency of provision of patient education (refer to Table IV, page 26), one reviewer suggested changing the item smoking cessation advice and commented that
"I would rather say information as advice is something that is offered when asked for it. We don't advise persons to stop smoking, we inform them of the risks and then they have to decide." (Reviewer 011)
Reviewers also identified items that lacked clarity. For example, concerning factors considered when assessing individuals with hand wounds (refer to Table IV, page 26), one reviewer stated that it was unclear if the item social support was referred to as support within the patient's home environment. The question asking participants to specify which team member (was) primarily responsible for wound management (refer to Table IV, page 26) was seen as too vague. A suggestion was made to either clarify if the question refers to basic or complex wounds or to break the question down to differentiate between basic and complex wounds.
Questions that were very similar and that could be integrated were identified. For example, with reference to the nature and prevalence of wounds of patients with hand injuries (refer to Table IV, page 26), reviewers felt that the difference between what type of hand injuries do you treat... and what are the most common hand injuries that you treat., was too subtle and that the response to both questions was likely to be the same. They recommended choosing one and expressed a preference for the latter.
Eight items were added on the recommendation of reviewers. These included access to wound management supplies/consumables and access to wound management instruments to items related to the extent to which various factors are barriers orenablers to the provision of wound management interventions (refer to Table IV, page adjacent). Reviewers felt it beneficial to differentiate between availability and access. One reviewer stated
"occupational therapists don't always have access to wound care items as it is presumably not within our scope of practice. So, it's always a struggle to order sterile items, dressings, etc., and to procure equipment such as forceps, hand baths, etc"(Reviewer 005).
In addition to removing items based on I-CVI calculations, comments of reviewers were also considered. Negative pressure wound therapy and application of physical agent modalities including whirlpool, electrical stimulation and ultrasound are examples of items removed from those listed to investigate the frequency of provision of wound care activities for the amelioration of wounds (refer to Table IV, page 26). Reviewers primarily reported that they did not know what these interventions were. Thus, they were deemed irrelevant to the population for which the survey was designed.
Discussion
This paper focused on the development and content validation of a survey for use as a quantitative data collection instrument. The survey was developed as no research instruments that would adequately address the aims of the study were identified. The aims included examining the perceived role of occupational therapy, the current practice of occupational therapists, and the perceived level of preparedness of occupational therapists in providing interventions related to wound management (within hand rehabilitation) within the South African context. The authors of the current paper endeavoured to achieve a survey that will collect data that will be useful for its intended purpose by considering aspects of validity in both the process of generating survey items as well as the process of evaluating generated items.
Generating survey items
Several strategies were employed to ensure rigour in qualitative inquiry to enhance the content validity of the survey18. As little is known about wound management in hand therapy in the South African context, a sequential exploratory mixed methods design18 was selected as the most appropriate study design. Using maximum variation, purposive sam-pling34 ensured the selection of appropriate participants with the necessary qualifications and experience in the field of hand therapy. The use of a semi-structured interview guide allowed for engagement in discussion arising from questions35 and allowed for participants to freely provide an in-depth account of their experiences and views18.
The rigorous development of a semi-structured interview guide further enhanced credibility and included pilot interviews, critical self-evaluation by the researcher36, and review of the semi-structured interview guide by the third and second authors37. Further measures that were taken in data collection included being well-prepared for interviews31 and accurate verbatim transcription38. To enhance credibility in data analysis, a rigorous process of thematic analysis was undertan35. Through tabulating coded data, an assessment could be made of the extent to which categories created encapsulated and adequately incorporated all relevant data36. A process of debriefing31 ensured that results were representative of data provided by participants32. Finally, a reflexive journal was kept to document and acknowledge biases and assumptions throughout the research process39, 40.
Evaluating survey items
The evaluation of the survey involved a qualitative and quantitative review. Reviewers provided qualitative feedback on the acceptability of the research tool. The commentary was used to revise demographic information to be obtained to be more relevant, the structure of response scales for ease of use, the use of language to be more appropriate, and items to be more transparent and eliminate ambiguity. The commentary was also used to remove items not relevant to the study setting and add items that were relevant to the setting. These actions were taken to enhance the acceptability of the survey to the intended respondent.
Quantitative review involved rating the relevance of items to produce a CVI for each item as a method of content validation11, 13, 22. Content validity Index calculations were performed at an item level, and the content validity was not calculated for the survey as a whole. All the items which appeared in the final survey received a minimum I-CVI of 0.81 with the exception of eight items that were added on the recommendation of a panel of reviewers. Two questions with low I-CVIs were retained, one of which, for example, enquired why therapists may feel that there is no demand for them to be involved in the management of wounds of patients with hand injuries within their setting. This question was deemed essential as qualitative inquiry, as well as anecdotal evidence based on experience of the first author and engagement with colleagues in the field revealed that not all therapists experience a demand to be involved in wound management in practice and that the demand is frequently related to various contextual factors. One reviewer commented that the question felt repetitive of the previous question, which enquired as to the reasons why therapists do experience this demand in practice. The question was retained, and the flow of the survey was designed for therapists to answer only one of the questions by first asking if they experience a demand requiring a yes, no response.
Limitations
Respondent validation, whereby the interpretation of qualitative findings is presented to individuals who participated in interviews to confirm if the interpretation of the information they provided is correct41 was not conducted, which should be considered a limitation of this study. A second limitation that should be considered is that due to time constraints, interviews were unable to continue until a point of data saturation, where further interviews were not anticipated to obtain any new information, had been achieved11,18. A third limitation of this study is that the survey was not re-submitted to reviewers following revisions to re-evaluate face and content validity. Although possible to calculate, a S-CVI would not have been indicative of the validity of the final survey due to revisions following qualitative review of the initial survey. Furthermore, items that were removed based on I-CVI calculations might have also benefited from revision. For example, the item the occupational therapist being in charge of the wound management improves the outcomes of therapy scored low and reviewers expressed that occupational therapists don't have the training to be in charge of a wound. The item needed to be revised to convey the intended meaning of interview participants, which was that they felt that the functional outcomes for patients might be improved if they provided interventions to facilitate healing, thereby being in charge of the wound care, such as suture removal because they had insight into the necessary precautions required to protect structures that were repaired, for example. Further limitations of this study that need to be considered include the limitations of the literature review. Excluding the word burn in the search strings may have excluded relevant studies for consideration within the item generation phase of the survey.
CONCLUSIONS
The rigorous development of a survey was identified as a crucial step in obtaining information that would be useful in addressing an identified gap in scientific knowledge as well as in informing relevant audiences about the need for education, training and mentorship for occupational therapists treating patients with hand injuries and conditions in South Africa. This survey demonstrated good content and face validity for use in a population of occupational therapy practitioners within the South African context. It cannot be extrapolated to different groups in different settings. Other ways to improve the overall validity of the survey for future studies include the use of focus groups to complement individual interviews18, and conducting cognitive interviews, which involves conducting a pilot study and receiving verbal feedback from participants to determine if the intended meaning of questions is understood by respondents11, 42.
Acknowledgements
The authors acknowledge the occupational therapists who participated in the study.
Declaration of conflicting interests
The authors have no conflict of interests to declare.
Authors contributions
Lezanne Esterhuizen was the primary researcher as a Master of Occupational Therapy candidate and was involved in the conceptualization of the study, instrument development, data collection and analysis and drafting of the manuscript. Pragashnie Govender and Deshini Naidoo served as supervisors of the study and provided critical input into research design, concept development, design of the instrument and review and critique of the article and in writing assistance.
REFERENCES
1. International Federation of Societies for Hand Therapy. IFSHT Hand Therapy Practice Profile. [Internet]. [cited 2020 Sept 10]. Available from: https://ifsht.org/sites/default/flles/IFSHT_Hand_Therapy_Profile_FINALJUNe%202010.pdf. [ Links ]
2. American Society of Hand Therapists. Position Paper on Hand Therapists' Scope of Practice 11/08/2011. [Internet]. [cited 2020 Sept 10]. Available from: https://www.ashtorg/sites/default/files/images/Practice/ASHT%20Scope%20of%20Practice.pdf [ Links ]
3. Keller JL, Caro CM, Dimick MP, et al. Thirty years of hand therapy: the 2014 practice analysis. J Hand Ther. 2016;29(3):222-234. https://doi.org/10.1016/j.jht.2016.02.011 [ Links ]
4. van Stormbroek K, Buchanan H. Novice therapists in a developing context: extending the reach of hand rehabilitation. Hand Ther. 2017;22(4):141-152. https://doi.org/10.1177/1758998317720951 [ Links ]
5. Seedat M, Van Niekerk A, Jewkes R, et al. Violence and injuries in South Africa: prioritising an agenda for prevention. Lancet. 2009;374(9694):1011-1022. https://doi.org/10.1016/s0140-6736(09)60948-x [ Links ]
6. Norman R. The high burden of injuries in South Africa. Bull. World Health Organ. 2007;85(09):695-702. https://doi.org/10.2471/blt.06.037184 [ Links ]
7. Makobore P, Galukande M, Kalanzi E, et al. The burden of hand injuries at a tertiary hospital in sub-saharan Africa. Emerg Med Int. 2015;2015:1-5. https://doi.org/10.1155/2015/838572 [ Links ]
8. Stewart A, Biddulph G, Firth GB. The aetiology of acute traumatic occupational hand injuries seen at a South African state hospital. SA orthop. j. 2017;16(4). https://doi.org/10.17159/2309-8309/2017/v16n4a8 [ Links ]
9. Pilling T, Govender P. Profile and management of the firework-injured hand. S Afr Fam Pract (2004). 2016;58(2):48-53. https://doi.org/10.1080/20786190.2015.1125167 [ Links ]
10. Mottay N, Govender P, Mpanza D. The use of the ICAM splint programme in zone IV to VII extensor tendon repairs: patient outcomes and clinician experiences in a specialised hand unit in SA. S. Afr. j. occup. ther. 2020;50(2):23-34. https://doi.org/10.17159/2310-3833/2020/vol50no2a4 [ Links ]
11. Ricci L, Lanfranchi J, Lemetayer F, et al. Qualitative methods used to generate questionnaire items: a systematic review. Qual Health Res. 2019;29(1):149-156. https://doi.org/10.1177/1049732318783186 [ Links ]
12. Kelley K, Clark B, Brown V, et al. Good practice in the conduct and reporting of survey research. Int J Qual Health Care. 2003;15(3):261-266. https://doi.org/10.1093/intqhc/mzg031 [ Links ]
13. Bertea PE, ZaiÇ A. Scale validity in exploratory stages of research. Management & Marketing. 2013;XI(1):38-46. https://www.researchgate.net/publication/266025023_Scale_Validity_In_Exploratory_Stages_Of_Research Accessed September 25, 2020. [ Links ]
14. Morse JM, Barrett M, Mayan M, et al. Verification strategies for establishing reliability and validity in qualitative research. Int J Qual Methods. 2002;1(2):13-22. https://doi.org/10.1177/160940690200100202 [ Links ]
15. Cabatan MCC, Grajo LC, Sana EA. Development and content validation of the adaptation process in academia questionnaire for occupational therapy educators. Acta Med Philipp. 2020;54(2):142-150. https://actamedicaphilippina.upm.edu.ph/index.php/acta/article/view/1537 Accessed September 25, 2020. [ Links ]
16. Kember D, Leung DYP. Establishing the validity and reliability of course evaluation questionnaires. Assess Eval High Edu. 2008;33(4):341-353. https://doi.org/10.1080/02602930701563070 [ Links ]
17. Onwuegbuzie AJ, Bustamante RM, Nelson JA. Mixed research as a tool for developing quantitative instruments. J Mix Methods Res. 2010;4(1):56-78. https://doi.org/10.1177/1558689809355805 [ Links ]
18. Brod M, Tesler LE, Christensen TL. Qualitative research and content validity: developing best practices based on science and experience. Qual Life Res. 2009;18(9):1263-1278. https://doi.org/10.1007/s11136-009-9540-9 [ Links ]
19. Al-Muallem A, Elzubeir M, Roberts C, et al. Development and initial testing of an instrument for evaluating needs and inferring readiness of research supervisors: a mixed methods approach. Health Professions Education. 2016;2(2):138-147. https://doi.org/10.1016/j.hpe.2016.03.001 [ Links ]
20. Roberts P, Priest H, Traynor M. Reliability and validity in research. Nurs Stand. 2006;20(44):41-45. https://doi.org/10.7748/ns2006.07.20.44.41.c6560 [ Links ]
21. Drost EA. Validity and reliability in social science research. Education Research and Perspectives. 2011;38(1):105-123. https://www.researchgate.net/proflle/Ellen_Drost3/pub-lication/261473819_Validity_and_Reliability_in_Social_Science_Research/links/5500abd50cf2aee14b56edb2/Validity-and-Reliability-in-Social-Science-Research.pdf Accessed September 25, 2020. [ Links ]
22. Bolarinwa OA. Principles and methods of validity and reliability testing of questionnaires used in social and health science researches. Niger Postgrad Med J. 2015;22(4):195-201. https://doi.org/10.4103/1117-1936.173959 [ Links ]
23. Williams A. How to ... write and analyse a questionnaire. J Orthod. 2003;30(3):245-252. https://doi.org/10.1093/ortho/30.3.245 [ Links ]
24. Polit DF, Beck CT. The content validity index: Are you sure you know what's being reported? critique and recommendations. Res Nurs Health. 2006;29(5):489-497. https://doi.org./10.1002/nur.20147 [ Links ]
25. Greene JC, Caracelli VJ, Graham WF. Toward a conceptual framework for mixed-method evaluation designs. Educ Eval Policy Anal. 1989;11(3):255-274. https://doi.org/10.3102/01623737011003255 [ Links ]
26. American Occupational Therapy Association. Role of occupational therapy in wound management. Am J of Occup Ther. 2018; 72(Supplement_2): 7212410057p1. http://dx.doi.org/10.5014/ajot.2018.72s212 [ Links ]
27. Kallio H, Pietilä A, Johnson M, et al. Systematic methodological review: developing a framework for a qualitative semi-structured interview guide. J Adv Nurs. 2016;72(12):2954-2965. https://doi.org/10.1111/jan.13031 [ Links ]
28. Onwuegbuzie AJ, Collins KM. A Typology of mixed methods sampling designs in social science research. Qual. Rep. 2007;12(2):281-316. https://nsuworks.nova.edu/tqr/vol12/iss2/9 Accessed September 25,2020. [ Links ]
29. Tongco MDC. Purposive sampling as a tool for informant selection. Ethnobot. Res. Appl. 2007;5:147-158. https://doi.org/10.17348/era.5.0.147-158 [ Links ]
30. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77-101. https://doi.org/10.1191/1478088706qp063oa [ Links ]
31. Shenton A. Strategies for ensuring trustworthiness in qualitative research projects. Education for Information. 2004;22(2):63-75. https://doi.org/10.3233/efi-2004-22201 [ Links ]
32. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105-112. https://doi.org/10.1016/j.nedt.2003.10.001 [ Links ]
33. Wilkinson D, Birmingham P. Using Research Instruments - A Guide For Researchers. London: RoutledgeFalmer; 2003. [ Links ]
34. Etikan I, Musa SA, Alkassim RS. Comparison of convenience sampling and purposive sampling. American Journal of Theoretical and Applied Statistics. 2016;5(1):1-4. https://doi.org/10.11648/j.ajtas.20160501.11 [ Links ]
35. Cohen D, Crabtree B. Semi-structured Interviews. Robert Wood Johnson Foundation qualitative research guidelines project. 2008. http://www.sswm.info/sites/default/files/reference_attachments/COHEN%202006%20Semistructured%20Interview.pdf. Accessed June 27, 2020. [ Links ]
36. Elo S, Kààriàinen M, Kanste O, et al. Qualitative content analysis: A focus on trustworthiness. Sage Open. 2014;4(1):215824401452263. https://doi.org/10.1177/2158244014522633 [ Links ]
37. Anney VN. Ensuring the quality of the findings of qualitative research: looking at trustworthiness criteria. Journal of Emerging Trends in Educational Research and Policy Studies (JETERAPS). 2014;5(2):272-281. http://196.44.162.10:8080/xmlui/handle/123456789/256 Accessed September 25, 2020. [ Links ]
38. Witcher CSG. Negotiating transcription as a relative insider: implications for rigor. Int J Qual Methods. 2010;9(2):122-132. https://doi.org/10.1177/160940691000900201 [ Links ]
39. Poggenpoel M, Myburgh C. The researcher as research instrument in educational research: a possible threat to trustworthiness? (A:research_instrument). Education. 2003;124(2):418-421. https://www.questia.com/library/journal/1G1-112480018/the-researcher-as-research-instrument-in-educational Accessed September 25, 2020. [ Links ]
40. Curtin M, Fossey E. Appraising the trustworthiness of qualitative studies: guidelines for occupational therapists. Aust Occup Ther J. 2007;54(2):88-94. https://doi.org/10.1111/j.1440-1630.2007.00661.x [ Links ]
41. Torrance H. Triangulation, respondent validation, and democratic participation in mixed methods research. Journal of mixed methods research. 2012; 6(2):111-123. https://doi.org/10.1177/1558689812437185 [ Links ]
42. Lenzner T. Neuert C. Otto W. GESIS Survey Guidelines. Cognitive pretesting. GESIS - Leibniz-Institute for the Social Sciences. 2016. https://doi.org/10.15465/gesis-sg_en_010 [ Links ]
 Correspondence:
Correspondence:
Lezane Esterhuizen
Lezane.esterhuizen@gmail.com
Received: March 2021
Peer review: May 2021
Revised: May 2022
Accepted: August 2022
Published: April 2023
Editor: Janine van der Linde: https://orcid.org/0000-0003-1067-9494
Funding: The University of KwaZulu-Natal, South Africa offered the corresponding author fee remission for completion of a Master of Occupational Therapy degree from which this research and paper emanated.


{kind=link}
{kind=link}
{kind=link}
{kind=link}