










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.52 no.3 Pretoria Dez. 2022
http://dx.doi.org/10.17159/2310-3833/2022/vol52n3a5
RESEARCH ARTICLE
Occupational therapists' perceived ability to treat and assist bereaved individuals to find new meaning in life through engagement in therapeutic activities
Enos RamanoI, *; Wilmari PretoriusII, *; Marike de JagerIII, *; Tara OldfieldIV, *; Daniela ScribaV, *; Bridgit MoritiVI, *
IPrivate Practice, Soweto, South Africa https://orcid.org/0000-0002-9706-1162
IIPrivate Practice, East London, South Africa https://orcid.org/0000-0002-1599-1586
IIIPrivate Practice, Port Elizabeth, South Africa https://orcid.org/0000-0003-4093-7634
IVPrivate Practice, Pietermaritzburg, South Africa https://orcid.org/0000-0003-0005-5899
VLetaba Hospital, Tzaneen, Limpopo, South Africa https://orcid.org/0000-0002-5487-0517
VICharlotte Maxeke Johannesburg Academic Hospital, Johannesburg, South Africa https://orcid.org/0000-0002-7176-7394
ABSTRACT
INTRODUCTION: Previous studies on bereavement have focused on the implications for bereaved individuals from behavioural and psychological perspectives. Limited literature discusses occupational therapists' perceived ability to treat bereaved individuals and how activities can be used to create new meaning to their lives.
METHOD: A descriptive qualitative design was employed in the study to elicit occupational therapists' perceived ability to treat bereaved individuals find new meaning in their life. Thirty-five occupational therapists were recruited, and nine participated in two focus groups. Data collected were thematically analysed.
FINDINGS: Three themes emerged, namely: (1) activities used in occupational therapy creates opportunities for new meaning to life after loss of a loved one, (2) appropriate occupational therapists' helping skills and professional behaviour to assist and treat the bereaved, and (3) perceived barriers to positive outcomes in treating the bereaved.
CONCLUSION: Bereaved individuals often have impaired performance in occupations and emotional processing. The effects of bereavement were addressed using the appropriate occupational therapist helping skills and professional behaviour to guide holistic, occupation-based and client-centred treatment. Bereaved individuals were treated through purposeful activities, facilitation of therapeutic groups and self-management skills training which seemed to create opportunities for new meaning in their life. Occupational therapists need to be cognisant of the barriers that negatively influence the positive outcome of occupational therapy services.
Keywords: purposeful activity, therapeutic groups, occupation based, client centred, devastating life event
INTRODUCTION
Bereavement denotes the objective situation of a person who has experienced the loss of someone significant through death1. The objective situation of bereavement includes a range of grief and mourning responses1. Grief is a process in which cognitive, social and existential adjustment take place1.
Seven percent of bereaved individuals do not cope effectively with the loss, which develops into complicated grief2. Complicated grief afflicts bereaved individuals and is associated with severe disruption of functioning3. The situation of bereavement affects the quality of life by placing mental, physical, and emotional strain on a bereaved individual4. It further affects occupational engagement and participation, and the bereaved individual's life roles and body functions5, which indirectly affect their health and well-being. Bereavement also impacts on how bereaved individuals participate in occupations such as activities of daily living (ADL), leisure tasks, social participation and work6,7,8.
When bereaved individuals cannot function in their daily occupations, they tend to experience occupational imbalance, which indicates that they require occupational therapy intervention to restore their optimal occupational engagement and participation5. The bereaved individuals tend to struggle with the bewildering sense of meaninglessness1. Occupational therapists focus on meaning reconstruction5 and occupational participation68. Consequently, occupational therapists use occupations or therapeutic activities to create meaning for bereaved individuals9.
A study carried out in Australia proved that there is a lack of education amongst most health care professionals (including occupational therapists) on working with bereaved individuals and Breen11 advised that there is a need for up-to-date and easily accessible grief education for grief counsellors. Daddah, Bombarda, Frizzo and Joaquim9 were concerned that there was a shortage of publications produced by occupational therapists for bereaved individuals. Furthermore, a shortage of evidence-based research that guides education on needs of children with grief issues in school-based settings results in the potential lack of confidence and competencies among occupational therapists to treat bereaved individuals of all ages who suffer from unresolved grief12. The feeling of incompetence contributes to the general view among occupational therapists that grief should be addressed by other health care professionals12. In addition, this perspective acts as a barrier for occupational therapists to provide treatment for bereaved individuals.
Through a literature search, the researchers of this article found limited evidence that supports the use of occupational therapy in treating bereaved individuals6,9. Furthermore, there was a paucity of literature in the South African context which discusses occupational therapists' perceived ability to treat bereaved individuals find new meaning in life through engagement in therapeutic activities even though the death of someone significant is a painful and often devastating life event3. Therefore, the objectives of this study were to describe: (1) occupational therapists' ways of facilitating meaning for bereaved individuals, and (2) occupational therapists' perceived barriers in treating bereaved individuals.
Literature Review
Bereavement involves adjusting to an altered reality after loss13. The ways of adapting to altered reality cannot be generalized, as reactions to death are diverse and unique14. However, the impact of bereavement is gauged by the nature of the relationship with the deceased, the amount of support received, and the resilience of the bereaved person15. When these factors are unfavourable to the bereaved individual, it may result in complicated bereavement or prolonged grief disorder15. Complicated bereavement or prolonged grief disorder affects a bereaved individual's quality of life by causing mental, physical and emotional strain4. Individuals who experience the loss of close relationships may experience impairment in occupations and disruption of roles and be unable to perform certain activities associated with role fulfilment6. The impact of bereavement on roles, occupations and quality of life may lead to a need for occupational therapy intervention.
Occupational therapists are responsible for enabling meaningful occupational engagement and creating occupation-based intervention8. According to Hoppes and Segal5, engagement in occupation is key to meaning reconstruction. Meaning reconstruction is the process of bereaved individuals' effort to find meaning1. Meaning is the transcription of the bereaved individuals' narratives, experiences and or values. Therefore, the use of meaningful activities has therapeutic and occupational value in organizing behaviour, which allows for a sense of individuality and contributes to the development of a sense of purpose16. Some obstacles may hinder a healthy grieving process. These include not acknowledging one's grief, not reflecting true feelings of grief, lack of social support systems, having inadequate time for grieving, and difficulty facing individual mortality9,10,11. Therefore, the study aimed to describe the occupational therapists' perceived ability to assist and treat bereaved individuals in finding new meaning in life through engagement in therapeutic activities11.
RESEARCH METHODOLOGY
Study design
A descriptive qualitative design17 was used to enhance the researchers' ability to contextualize bereavement in its complexity9. Using a descriptive qualitative design, we were able to describe the occupational therapists perceived ability to treat bereaved individuals and their experiences of using therapeutic activities in this context17. A descriptive qualitative design allowed for the description of multiple viewpoints from the perspective of the participants who took part in the study.
Study setting
The two focus groups were conducted at two venues located in Pretoria/Tshwane. All the occupational therapists worked in Gauteng Province and practised in mental health care settings. They treated patients with various psychiatric diagnoses, including major depressive disorder due to bereavement. The clinical occupational therapists provided both individual sessions and group therapy, whereas the academic occupational therapists included in the study taught and provided clinical supervision for the mental health module to undergraduate and postgraduate occupational therapy students.
Study population and sampling
The target population included qualified occupational therapists practicing in academic, public, and private psychiatric hospitals in the Gauteng Province of South Africa. All the occupational therapists were registered with the Health Professionals Council of South Africa (HPCSA). The researchers recruited participants using purposive sampling17. Purposive sampling17 was used to recruit occupational therapists working in mental health care facilities or teaching mental health. The researchers considered participants who had experience and knowledge of working in mental health. The inclusion criteria considered qualified occupational therapists registered with the Health Professions Council of South Africa (HPCSA) as independent practitioners, currently working in mental health care facilities or teaching mental health in Pretoria/Tshwane. The exclusion criteria were occupational therapists practicing in other fields such as pediatrics, physical, neurology, geriatrics, and vocational rehabilitation.
A recruitment invitation was formulated and sent to a list of known occupational therapists working at various private and public psychiatric practices and a university in Pretoria/Tshwane via email, SMS or WhatsApp. As there were no responses to any emails, the researchers telephonically contacted occupational therapists on the list to recruit them to participate in the study. Thirty-five occupational therapists were contacted and nine occupational therapists consented to participate in one of two focus groups.
Ethical clearance
This research was approved by the Research Ethics Committee of the Faculty of Health Science at the University of Pretoria (ethics clearance number 803/2019). All the ethical principles of respect for person, principles of justice, principles of beneficence and non-maleficence were adhered to throughout the study17. The participants completed an informed consent form prior to their participation in the study. The researchers ensured voluntary participation, anonymity and confidentiality of participants17. The researchers anonymized the names of participants with a participant number one to nine to protect the participants' identities.
Data collection procedure
All participants filled in demographic data forms. The demographic data form included their gender, ages, qualifications (undergraduate and postgraduate), years of experience working in mental health and psychiatry, and place of work. The researchers focused on the objectives of the study as guided by Brink, van der Walt and Rensburg17 to formulate questions for the focus group interview guide. The moderator, one of the researchers, is a qualitative researcher trained by the university to facilitate focus group discussions (FGDs). The first FGD was held at a university in Pretoria and the second one at a private clinic in Pretoria/Tshwane. The moderator used an interview guide with open-ended questions to facilitate the FGDs. The moderator clarified the participants' responses using probing questions to expand their perceptions and experiences. The moderator asked summarising and concluding questions to clarify what had been discussed and to allow for final thoughts on the topic17. Each focus group lasted approximately two hours and both focus groups were audio recorded. The other researchers took field notes during the FGDs.
Data analysis
The recordings were transcribed verbatim and analyzed the-matically. Data were analysed inductively using a bottom-up approach17. Data analysis occurred as suggested by Braun and Clarke18. The researchers read through the transcripts to familiarise themselves with the depth and breadth of the data18. Initial codes were individually generated. Lists of codes were identified across the data set. Similar incidents of codes were sorted and grouped and given the same name17,18. These codes were sorted, grouped and collated into categories18. Groups of categories gathered from quotes were pooled together to clearly define and name themes17,18. Potential themes were generated. Themes were reviewed and refined. The researchers identified the essence of each theme. The researchers defined and named the themes. The researchers interpreted the themes against the research aims, objectives and problem statement18. The researchers ensured that the themes were concise, coherent, logical and non-repetitive18. The researchers met face-to-face to discuss and agree on the themes, which were then finalized. Once the thematic analysis was completed, findings were sent to all the participants via email for member checking. All the participants agreed with the list of themes and quotes, and offered some minor alterations.
During the field notes, the other researchers wrote down their observations during FGDs in a descriptive manner as descriptive field notes. At the end of the FGDs, the researchers met and reflected on their thoughts and the meaning of their observations. The field notes were typed. The typed notes were coded and merged into the thematic analysis.
Measures to ensure trustworthiness
Fieldnotes and FGDs were means of collecting data to ensure maximum data uptake and triangulation. Field notes, FGDs and the findings were compared to existing literature17. Member checking and triangulation ensured the credibility of the data. As part of member checking, all the participating occupational therapists validated the findings and confirmed that the findings reflected their views17.
FINDINGS
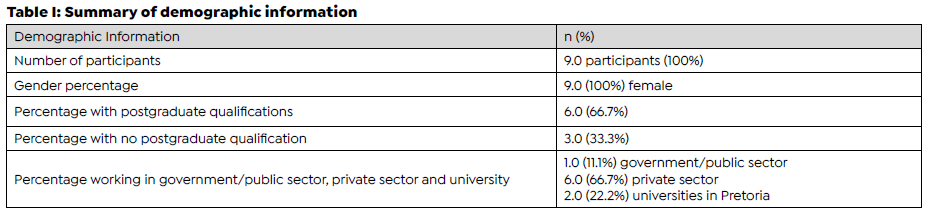
All nine participants were women. Their ages ranged from 24 to 73 years, with an average age of 41.3 years. Their average years of experience in psychiatry and mental health was 16.3 years, and six of the nine participants had 10 or more years of experience in this field. All participants had completed a Bachelor of Occupational Therapy degree. Two participants had an additional postgraduate diploma, and four had a master's qualification in occupational therapy. Six of the participants (66.7%) were employed in the private sector, one (11.1%) was employed in the public sector and two (22.2%) were working at a higher education institution (Table I, page 37).
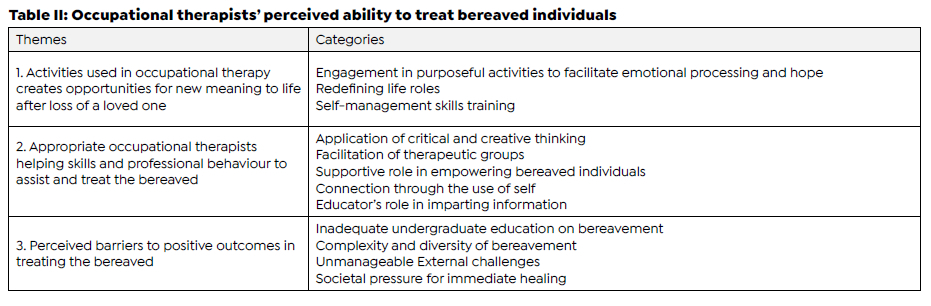
The three themes that emerged in the study are discussed as 1) activities used in occupational therapy create opportunities for new meaning to life after loss of a loved one, 2) appropriate occupational therapists helping skills and professional behaviour to assist and treat the bereaved, and 3) perceived barriers to positive outcomes in treating the bereaved. The themes and categories of this study are summarised in Table II (page 37 )
THEME 1: Activities used in occupational therapy create opportunities for new meaning to life after loss of a loved one
This theme deals with the opportunities facilitated by occupational therapists to enable bereaved individuals to create new meaning in their lives after loss of the loved one.
The theme highlights the creation of new meaning to life of bereaved individuals through engagement in purposeful activities to facilitate emotional processing and hope, redefining life roles, and self-management skills training.
Theme 1 Categories
Engagement in purposeful activities to facilitate emotional processing and hope
Participants felt that engagement in purposeful activities enabled bereaved individuals to recognise their vision for the future. Purposeful activities allowed for the creation of meaning, which gave them something to do and possibly something to love and look forward to. Occupational therapists should give bereaved individuals an opportunity to create hopeful meaning for themselves by allowing them the freedom of choice and to make their own decisions. Two participants alluded that occupational therapists created meaning of hope for bereaved individuals.
"We [occupational therapists] allow that person [bereaved individual] to find out that they can create hope themselves. I [occupational therapist] prefer that you give them [bereaved individuals] that space and opportunity to find that hope again". (Participant number 8)
"I'm just saying that there is an emotional part but there's a functional activity part. So, while they are doing that emotionally they are venting out, they are letting go you know it can be very emotional and get healing which gives them some hope." (Participant number 2)
Occupational therapists are equipped with unique skills such as therapeutic relationship skills and the use of self to guide bereaved individuals using purposeful activities that are important to the individual. The participants mentioned that using purposeful activities might effectively address the dysfunction engendered by emotional aspects of bereavement. This includes facilitating distraction and emotional processing:
"...the occupational therapist is a master of distraction. We [occupational therapists] always have been keeping their mind off things, transferring focus onto something else. It can be applied perfectly with your bereaved person to address their emotional aspect." (Participant number 7)
"...you help them to journaling, for instance, it's a very, very effective way writing letters. This writing of letters [goodbye letter to the deceased] might address the emotional aspect of bereavement" (Participant number 1)
Participants expressed that bereavement consists of a functional and emotional aspect. Both aspects influence one's occupational performance and psychological well-being. It was further expressed that the bereavement process is emotional due to overwhelming thoughts, questions, and feelings, which add to the complexity of bereavement. 'Crafts', 'mosaic', 'journaling', 'writing letters', 'making memorial boards', 'pot plants' and 'scrapbooking' were examples of activities that facilitated emotional expression in addressing the bereaved individuals' emotional and functional aspect as remarked by participants.
"...you can use things like creative arts, you can use things like mosaic for instance...as long they are meaningful and culturally relevant" (Participant number 2)
"...the activity because you need to find something, where you can kind of release the emotional component and work through it and get it out there where you can deal with it and usually journaling, is some of the best ways to do it or to create something like scrapbooking or a memory board" (Participant number 1)
Redefining life roles
There was consensus amongst the participants that bereavement affects bereaved individuals' roles, habits, routines and rituals. Bereavement deprives people of the meaning attached to their life roles, habits or routines, and rituals. Occupational therapy interventions refine the roles, habits or routines of bereaved individuals as highlighted by the participants:
"...you have to help [the bereaved individual] to find meaning in this role or that role or change the way [they] do it so that it's still meaningful." (Participant number 3) "I think [occupational therapy] is the most unique and equipped profession through certain activities [sic] give meaning back to people. To get them to refocus, refine, and define their roles and through that give new meaning in their lives." (Participant number 1)
Self-management skills training
The participants emphasized self-management skills-training as an important part of occupational therapy interventions with bereaved individuals. They further expressed that occupational therapists could coach bereaved individuals about self-management skills while enabling them to engage in activities to address their occupational disruption. One participant listed various self-management skills and the avoidance of overwhelming emotions. Specific self-management skills that occupational therapists used with bereaved individuals included mindfulness, exercise, yoga, stress management, assertiveness skills and boundaries, which formed part of the occupational therapy sessions that facilitated adaptive emotional outlets. This is highlighted by two participants who said:
"...if you give someone a specific technique that they do and teach stress management, mindfulness, exercise, yoga - a specific technique." (Participant number 7)
"Assertive in a sense that if you want to grieve, if you feel like I want to cry it doesn't matter what the society prescribes for you at the time has lapsed you know. That you are able to own that today I don't feel okay I want to cry and also that you know you are able to access other support groups." (Participant number 2)
THEME 2: Appropriate occupational therapists helping skills and professional behaviour to assist and treat the bereaved
This theme deals with the appropriate occupational therapists helping skills and professional behaviour to assist bereaved individuals. The theme focuses on the helping skills and professional behaviour described by the participants that occupational therapists need to provide to bereaved individuals. These helping skills and professional behaviour of occupational therapists are: the application of critical and creative thinking, facilitation of therapeutic groups in occupational therapy, supportive role to empower bereaved individuals, connection through the use of self, and educator role in imparting information.
Theme 2 Categories
Application of critical and creative thinking
Under this category, findings are that occupational therapists required the application of critical and creative thinking as there was no specific method to treat bereaved individuals. The occupational therapist should be able to select, adapt, and use activities that are purposeful and relevant by consistently applying their critical and creative thinking. Application of critical and creative thinking were further highlighted by participants as important because bereavement is a complex process that cannot be treated in isolation. As a member of a multidisciplinar/ team, occupational therapists should have helping skills such as empathy, encouragement and patience which relates to critical and creative thinking. They should allow the bereaved individuals to process their challenges during their grieving journey. This was echoed by participants who remarked as follows:
".bereavement is a complex cognitive thing that you need to be able to reason about. It must have that [critical] reasoning ability and the emotional maturity to deal with it and that people know that, that it will not be fixed or [use a] recipe that you can apply." (Participant number 1)
".it's part of the narrative [reasoning] - there's triggers, there's stressors - this is something, a challenge that has come into their lives, and now they can't process it well enough so that they can continue." (Participant number 8)
Facilitation of therapeutic groups
Therapeutic groups in occupational therapy is used to enable the bereaved individuals to learn from other group members while creating new meaning for themselves. The participants supported the use of therapeutic groups. They cited that therapeutic groups in occupational therapy facilitated social participation and interaction and allowed the bereaved individuals to give and receive feedback in a safe environment.
"That is something that we can do [with bereaved individuals] in a support group or [.] an environment that we can share because people also tend to share nicely with people who have been through similar... if you have experienced or you have you can relate it helps... " (Participant number 3)
"...a huge one might be the universality; to know that you are not alone, knowing that the therapist is there with me, or another group member [.] it's creating that connection [group cohesiveness] .. " (Participant number 9)
Supportive role in empower bereaved individual
In the FGDs, the supportive role of an occupational therapist was identified as an enabler that empowers bereaved individuals. This is supported by the participants who said:
"To allow them to speak up about their loss and accept help [for] them by going out to the right people to support and help them in their environment, to get the right people involved." (Participant number 1)
"...so, I feel it's the [occupational therapists] role to be there and advocate and empower them [bereaved individuals]" (Participant number 2)
Connection through the use of self
The participants shared that the use of self is important as it allows the bereaved individual to feel connected and comforted by the occupational therapist during occupational therapy intervention. Occupational therapists should use facilitation skills during therapy to build rapport and therapeutic relationship with the bereaved individual. This could be guided by the client-centred approach as it allows the occupational therapists to have respect, rapport, empathy and collaboration. This approach also allows bereaved individuals to make their own decisions and to be able to connect with the occupational therapist to have a sense of comfort. This is supported by the participants whose utterances follow:
"All the skills that you should be developing like listening, being available and understanding your role as yourself [occupational therapist] in the process are important" (Participant number 8)
"...use of self is very important. Sometimes it's just comfort that you want to give [.] you need to be able to restrain yourself from giving a solution and just sit and listen and let them bring it while you are there with them." (Participant number 2)
Educator's role in imparting information
From the FGDs, it was suggested that occupational therapists should fulfil an educator's role in educating bereaved individuals on the bereavement process and how to engage and cope with the emotional aspects of bereavement. This is highlighted by the participants who stated that:
"...clients need at least the knowledge to know what the process [of bereavement] entails, and that people will go through the process in different ways." (Participant number 1)
"...you at least discuss the grieving process and how it fits in at different places and stages." (Participant number 5)
THEME 3: Perceived barriers to positive outcomes in treating the bereaved
This theme highlights the perceived barriers to the positive outcome of occupational therapy to treat the bereaved individuals. These barriers comprised of occupational therapists' inadequate undergraduate education and training, complexity and diversity of bereavement, unmanageable external challenges and societal pressure for immediate healing.
Theme 3 Categories
Inadequate undergraduate education on bereavement
Most participants voiced that formal learning and practical training on bereavement were not adequately taught at undergraduate level. The participants' comments below bear witness to that:
"I feel that [bereavement] wasn't touched on enough in my training... maybe it wasn't taught in a way that allowed us to have this understanding." (Participant number 9) ".I think still it would make things so much easier [for the occupational therapist] to have a point of reference to work from regarding bereavement." (Participant number 1)
Two participants stated that bereavement is not a linear process in contrast to what is taught at undergraduate level. The focus is on the Kübler Ross model and other different models are not taught. Inadequate understanding of the process of bereavement created a shortfall in the occupational therapists' competency to address bereavement:
"... [occupational therapists] would only be with that client for a very short part of the bereavement journey. It's a long journey, and it's not a linear one." (Participant number 7)
"It must be an interactive approach that doesn't reinforce this 'stuck'.... For me, it's integrative - the interaction of different therapeutic modalities and models." (Participant number 9)
Complexity and diversity of bereavement
The treatment of bereavement is complicated by the complex and diverse nature of bereavement. Bereaved individuals experience the process uniquely as their construct of death differs. This is supported by the participants' observations:
". it's so individual, everybody is an individual and it depends on what and where they are in the grief process." (Participant number 3)
"... [occupational therapists] must also have space to debrief, so they can continually give the best care, because I think sometimes the reason for 'avoiding', is that I don't have the capacity at the time to be with the patient in this, but if I'm monitoring myself, making sure that I'm meeting my own needs and constantly debriefing and be sure that I'm not holding onto the patient's stuff, will give me a better opportunity to be there." (Participant number 9)
Unmanageable external challenges
It was noted that unmanageable external challenges hindered effective occupational therapy intervention. Some challenges included occupational therapists' limited time and resources. Occupational therapists working in the private sector experienced additional pressure as treatment depended on a bereaved individuals' medical-aid funds and available financial resources. This point is elaborated by participants who said:
"...there's time and money [needed], we must progress [recover], we must go home quickly [discharge from hospital], and we must think of our goals." (Participant number 8)
".if your medical aid is depleted [in private facilities] it means I'm [occupational therapist] not available." (Participant number 2)
Societal pressure for immediate healing
It was opined that certain societal expectations negatively influenced the success of occupational therapy. These social expectations influence a bereaved individual's ability to adjust to change, their capacity to cope and their well-being. Society is known to avoid coping with loss, which can influence the healing process. This societal pressure impacted on occupational therapy treatment and bereaved individual ways of healing. These were supported by the participants who elaborated that:
"...I'm thinking of society's idea of 'move on'..." (Participant number 9)
".internally they did not mourn properly, and people [bereaved individuals] are left to do their mourning and bereavement alone." (Participant number 4)
"...death is an awkward thing for everybody in that group. Nobody wants to speak about it. Nobody wants to talk with you." (Participant number 7)
The evidence from the societal pressure highlights the need for support for the bereaved individuals and education to the society at large as society needs to understand bereavement meaningfully.
DISCUSSION AND IMPLICATIONS
This study provided insight into the occupational therapists' perceived ability to treat bereaved individuals to find new meaning in life through engagement in therapeutic activities. Overall, the findings highlight that occupational therapists are in the ideal position to facilitate the opportunity for bereaved individuals to create new meaning to their life through engaging in purposeful activities to address emotional processing and hope. According to Neimeyer19, an involuntary search for meaning is essential to adapt to the altered reality after the loss of a loved one. Occupational therapists can guide and ease this involuntary search for meaning to life by engaging bereaved individuals in purposeful activities. Bereavement affects one's meaning attached to life and occupational engagement in purposeful activities. Freitas20 indicated that bereavement leads to a loss in the sense of life and imposes the demand to create new meaning.
The findings from the present study suggest that activities provide hope and that doing creates meaning, which corroborates the idea that meaning emerges from occupations that bring purpose to life8. This is further supported by Frankl's21 idea that meaning emerges when one has something to do, something to love, and something to look forward to. This agrees with the findings of this study which advises that activities should be meaningful, client-centred, and relevant to the bereaved individual's individuality, circumstances and environment. This is further supported by the Occupational Therapy Practice Framework8 which has a core belief in the connection between occupation and health as well as the use of occupation to create meaning.
It was evident from the findings that occupational therapists need to consider the importance of functional and emotional aspects of bereavement. Kersting and Wagner22 found that reactions to bereavement include impairment in day-to-day functioning and emotional processing. Hence, the findings of this present study support the concepts of occupation-centred practice as bereavement leads to regression and disengagement in occupations. A study by Hoppes and Segal5 which focused on reconstructing meaning through occupation after the death of a family member: accommodation, assimilation and continuing bonds found that bereaved individuals do not adjust to the way they perform occupations, but rather, alter certain occupations. The use of practical activities to address occupational needs was recommended by the participants of this present study.
Bereavement deprives the bereaved individuals the meaning attached to their life roles, habits or routines and rituals, which indicates that occupational therapists should aim to address and transform bereaved individuals to redefine their roles in treatment as stated in the present study. Batista et al.23 found that some bereaved individuals tend to isolate themselves from social situations and others feel a sense of guilt when performing leisure tasks. The findings of this present study also pointed out that some activities no longer held the same meaning and were therefore discontinued. Hoppes and Segal5 concur with the findings of this present study when they point out that individuals may change their career, perspective of work, or increase work engagement as a coping strategy.
It was evident from the participants' discourses that occupational therapists should assist bereaved individuals in redefining their roles, habits, routines, and rituals because they might influence what they opt to do, love, and look forward to in their lives. The findings of this present study strongly suggest that it was part of the occupational therapist's role to intervene when bereaved individuals struggled to adapt to their changed performance patterns. This concurs with findings by Dahdah and Joaquim,6 that bereavement causes a change in lifestyle, abandonment of roles or an inability to perform co-occupations by the bereaved individual. Furthermore, Dahdah et al.9 alert us that a bereaved individual might experience a need to continue to fulfil their prior roles and daily routines. This is, however, not always possible when one loses a loved one9. The participants from the present study suggested that an occupational therapist should guide bereaved individuals to redefine their roles and routines according to their values, interests and abilities, so that they can adopt new habits.
In the findings of the present study, the occupational therapists agreed with each other that emotional venting was essential in treating the bereaved individual. It was also noted in the FGDs that bereaved individuals may find meaning, which is linked to their involvement in purposeful activities. The participants of this present study mentioned that activities could be used as a source of distraction to shift one's focus from the preoccupation with thoughts associated with the loss. Additionally, they mentioned that activities aid in the emotional processing of the loss by dealing with feelings expressively. Similar findings also cite expressive activities to help bereaved individuals to understand loss and distract them from overwhelming feelings6. Activity examples mentioned by the participants of this present study included mosaic, pot plants, journaling, writing goodbye letters, making memorial boards, memory boxes and scrapbooking. This is consistent with Neimeyer and Thompson25 who stated that music, poetry, and visual arts are effective treatment modalities.
Suppression of emotions impedes healing; therefore, the approach should rather be to empower the bereaved individual to process uncomfortable feelings9. The findings of this present study emphasise that coping skills should not be used to suppress emotions, but rather allow bereaved individuals to experience and process uncomfortable emotions. These findings suggest that occupational therapists can transfer self-management skills through coaching so that bereaved individuals can manage the functional and emotional consequences of bereavement. In the present study, some examples of self-management skills that might be used as part of the therapy sessions were identified and included mindfulness, exercise, yoga, stress management, assertiveness skills and boundaries.
The findings further indicate that occupational therapists need to possess the application of critical and creative thinking to guide the success of occupational therapists' ability to treat the bereavement individual and provide holistic assessment, use of activities, and work within an interprofessional team. The findings further highlight that applying critical and creative thinking enabled the occupational therapists to form an integral, holistic understanding of the bereaved individual and facilitate a client-centred occupational therapy intervention. The American Occupational Therapy Association (AOTA)8 asserts that occupational therapists are skilled in evaluating all aspects of a client related to the context of the environment. Hence, the supportive role of the occupational therapist to empower bereaved individuals is significant in a supportive environment that enables provision of effective treatment services in helping the bereaved individuals. As Dhillon et al.27 stated, the occupational therapists provide education, services, support, and improve function.
These findings are further supported by the benefit of facilitating therapeutic groups that enhance social inclusion, support, and activity participation. Consequently, the findings corroborate with Ramano, de Beer and Roos26 who found that occupational therapy groups offer feelings of belonging, sharing and opening up as part of support and healing.
It emerged from this present study, that occupational therapists have an educator role, which necessitates imparting information during the treatment of bereavement. These findings indicate that the educator role involves the use of psychoeducational approaches to teach the bereaved individual on what the bereavement process entails. It is important to educate the bereaved individuals that bereavement is not a linear process. Therefore, the education role is strengthened by the continuous therapeutic relationship that allows the bereaved individual not to feel alone during the bereavement process. There is a significant link between therapeutic relationships and treatment outcomes in various settings, specifically in occupational therapy in mental health28. The participants of this present study echoed the importance of connecting with the bereaved individual through the use of self and building rapport with the bereaved individual. Research shows that the development of rapport is crucial to occupational therapy success8.
There are perceived barriers to the positive outcome of occupational therapy to treat the bereaved individuals. The findings of the present study pointed out barriers to positive outcome such as inadequate undergraduate training on bereavement. This led to lack of confidence amongst the occupational therapists with no point of reference to help the bereaved individuals. Alers29 questions whether the existing competencies of occupational therapy graduates match the demands of the profession. This highlights the lack of sufficient education on bereavement in occupational therapy where the study took place. Breen30 raised a concern that insufficient education causes most clinicians to make use of stage-based theories. The Kübler Ross31 grief model is taught in undergraduate education and most occupational therapists use this model to understand and guide bereavement. None of the participants in this present study mentioned any contemporary models, such as the Dual-Process model32. The Dual-Process Model describes the oscillation between confronting and denying emotions associated with grief between the phases of bereavement32.
Bereavement is diverse and complex as bereaved individuals experience the process uniquely and seek treatment at different points in the process of bereavement. A participant in this present study warned that an occupational therapist who uses their own experience of death as guidance for the intervention might miss the unique needs of a bereaved individual. The findings of this present study are consistent with a systematic review by Dahdah et al.9 which reported that bereavement is a complex event that is different for each bereaved individual. One's construct of death also influences how one processes loss9. Additionally, time and resources are unmanageable external challenges that affect the success of occupational therapy. Poverty and resource limitations in South Africa restrain occupational therapists from providing services adequately29.
It has been found that adverse social pressure for immediate healing acts as a barrier to one's ability to cope with bereavement. Participants agreed that society is known to take an avoidance and awkward approach towards coping with a loss, which in turn influences the healing process. An unsupportive social environment and dysfunctional family dynamics are associated with more significant psychological distress and complicated grief symptomatology9. This is a further challenge as a bereaved individual's progress might be impacted by lack of social support and follow-ups.
Limitations
A limitation to this study is that it only focused on occupational therapists practicing in Tshwane/Pretoria in Gauteng.
CONCLUSION
It is evident from the findings that occupational therapists perceived engagement in therapeutic activities as essential to creating opportunities for new meaning for bereaved individuals. Engagement in therapeutic activities offer bereaved individuals an opportunity to adapt to their altered reality. Due to the diverse emotional and functional challenges associated with bereavement, occupational therapists perceived ability to help bereaved individuals should be occupation-based, holistic and client centred. Occupational therapists can also help to redefine the life roles of bereaved individuals by helping them to adapt to their routines, roles, habits and rituals. The facilitation of therapeutic groups might allow bereaved individuals to experience support and equip them with self-management skills that might enable them to cope with their loss. Occupational therapists were concerned that perceived barriers to positive outcome of occupational therapy in treating bereaved individuals was associated with inadequate undergraduate education and training on bereavement, the complexity and diversity of bereavement, unmanageable external challenges, and societal pressure for immediate healing. Feedback from the participants about occupational therapy perceived ability to treat bereaved individuals was valuable to improve the possible positive outcome of occupational therapists to help the bereaved individuals. It might be essential for undergraduate occupational therapy education and training to include the treatment of bereaved individuals. The authors of this study encourage more occupational therapy research that focuses on the effectiveness of various occupational therapy interventions to help bereaved individuals.
Acknowledgements
The authors would like to thank the research participants for voluntarily participating in this study.
Author Contribution
Marike de Jager, Wilmari Pretorius, Tara Oldfield, Daniela Scriba and Bridget Moriti were 4th Year students in the year 2020 and the main study was completed as part of their 4th year research project and Enos Ramano was their research supervisor. All the authors contributed to this manuscript for publication.
Conflict of Interest (COI)
The authors have no conflict of interest to declare.
REFERENCES
1. Hibberd R. Meaning Reconstruction in Bereavement: Sense and Significance. Death Studies. 2013; 37: 670-690. http://dx.doi.org/:10.1080/07481187.2012.692453 [ Links ]
2. Shear MK, Ghesquiere A. Bereavement and complicated grief in older adults. Late-life mood disorders. 2013; 220-235. http://dx.doi.org/:10.1093/med/9780199796816.003.0013 [ Links ]
3. Malgaroli M, Maccallum F, Bonanno GA. Symptoms of persistent complex bereavement disorder, depression and PTSD in a conjugally bereaved sample: A network analysis. Psychological Medicine. 2018; 48(14): 2439-2448. https://dx.doi.org/:10.1017/S0033291718001769 [ Links ]
4. Carter PA. Bereaved caregivers descriptions of sleep: Impact on Daily Life and the Bereavement Process. Oncology Nursing Forum. 2006; 32(4): E70-E75. http://dx.doi.org/:10.1188/05.onf.e70-e75. [ Links ]
5. Hoppes S, Segal R. Reconstructing Meaning Through Occupation After the Death of a Family Member: Accommodation, Assimilation and Continuing Bonds. American Journal of Occupational Therapy. 2010; 64(1): 133-141. http://dx.doi.org/:10.5014/ajot.64.1.133. [ Links ]
6. Dahdah DF, Joaquim RHVT. Occupational Therapy in the bereavement process: A meta-synthesis. South African Journal of Occupational Therapy. 2018; 48(3): 12-18. http://dx.doi.org/:10.17159/2310-3833/2017/vol48n3a3. [ Links ]
7. Rosenwax L, Malajczuk S, Ciccarelli M. Change in carers' activities after the death of their partners. Supportive Care in Cancer. 2014; 22(3): 619-626. http://dx.doi.org/:10.1007/s00520-013-2014-1. [ Links ]
8. American Occupational Therapy Association. Occupational therapy practice framework: Domain and process. The American Journal of Occupational Therapy. 2014; 68(Suppl. 1): S1-S48. http://dx.doi.org/:10.5014/ajot.2014.682006. [ Links ]
9. Dahdah DF, Bombarda TB, Frizzo HCF, Joaquim RHVT. Systematic review about bereavement and occupational therapy. Brazilian Journal of Occupational Therapy. 2019; 27(1): 186-196. http://dx.doi.org/:10.4322/2526-8910.ctoAR1079. [ Links ]
10. Breen LJ, Fernandez M, O'Connor M, Pember AJ. The Preparation of Graduate Health Professionals for Working with Bereaved Clients: An Australian Perspective. OMEGA - Journal of Death and Dying. 2013; 66(4): 313-332. http://dx.doi.org/:10.2190/OM.66.4.c. [ Links ]
11. Breen LJ. Professionals' Experiences of Grief counselling: Implications for Bridging the Gap between Research and Practice. Journal of Death and Dying. 2011; 62(3): 285-303. http://dx.doi.org/:10.2190/OM.62.3e [ Links ]
12. Milliken B, Goodman G, Flinn S. Establishing a Case for Occupational therapy in meeting the needs of children with grief issues in school-based settings. Occupational Therapy in Mental Health. 2007; 23(2): 75-100. http://dx.doi.org:10.1300/J004v23n02_04. [ Links ]
13. Gillies J, Neimeyer R. Loss, Grief, and the Search for Significance: Toward a Model of Meaning Reconstruction in Bereavement. Journal of Constructivist Psychology. 2006; 19(1): 31-65. http://dx.doi.org/:10.1080/10720530500311182 [ Links ]
14. Barreto P, Yi P, Soler C. Predictores de duelo complicado. Psicooncologia. 2008; 5(2-3): 383-400. [ Links ]
15. Boyd-Webb N. Play therapy for bereaved children: Adapting strategies to community, school, and home settings. School Psychology International. 2011; 32(2): 132-140. http://dx.doi.org/:10.1177/0143034311400832. [ Links ]
16. Ikiugu MN, Hoyme AK, Mueller BA, Reinke RR. Meaningful occupation clarified: Thoughts about the relationship between meaningful and psychologically rewarding occupations. South African Journal of Occupational Therapy. 2015; 45(1): 47-50. http://dx.doi.org/:10.17159/2310-3833/2015/v45no1a8. [ Links ]
17. Brink H, van der Walt C, van Rensburg, G. Fundamentals of research methodology for healthcare professionals. 4th Ed. Singh J, editor. Cape Town: Juta and Company (Pty) Ltd; 2018. [ Links ]
18. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006; 3(2): 77-101. http://dx.doi.org/:10.1191/1478088706qp063oa. [ Links ]
19. Neimeyer R. Meaning reconstruction and the experience of loss. Washington DC: American Psychological Association; 2001. [ Links ]
20. Freitas J. Luto e fenomenología: uma proposta compreensiva. Phenomenological Studies- Revista da Abordagem Gestaltica. 2013: 19(1): 97-105. [ Links ]
21. Frankl VE. Man's search for meaning. New York: Washington Square Press; 1984. [ Links ]
22. Kersting A, Wagner B. Complicated grief after perinatal loss. Dialogues in Clinical Neuroscience. 2012; 14(2): 187-194. http://dx.doi.org/:10.31887/dcns.2012.14.2/akersting [ Links ]
23. Batista MPP, Rebelo JE, Carvalho RT, Almeida MHM, Lancman S. Widow's perception of their marital relationship and its influence on their restoration-oriented everyday occupations in the first six months after the death of the spouse: A thematic analysis. Australian Occupational Therapy Journal. 2019; 66(6): 700-710. http://dx.doi.org/:10.1111/1440-1630.12609. [ Links ]
24. Wortmann JH, Park CL. Religion/spirituality and change in meaning after bereavement: Qualitative evidence for the meaning making model. Journal of Loss and Trauma. 2009; 14(1): 17-34. http://dx.doi.org/:10.1080/15325020802173876. [ Links ]
25. Neimeyer RA, Thompson BE. Meaning making and the art of grief therapy. In Neimeyer RA, Thompson BE, editors. Grief and the expressive arts: Practices for creating meaning. New York: Routledge. 2014; 3-13. [ Links ]
26. Ramano EM, de Beer M, Roos JL. The perceptions of adult psychiatric inpatients with major depressive disorder towards occupational therapy activity-based groups. South African Journal of Psychiatry. 2021; 27(0): 1-8. http://dx.doi.org/:10.4102/sajpsychiatry.v27i0.1612. [ Links ]
27. Dhillon SK, Wilkins S, Law M, Stewart DA. Advocacy in occupational therapy: Exploring clinicians' reasons and experiences of advocacy. Canadian Journal of Occupational Therapy. 2010; 77(4): 241-248. http://dx.doi.org/:10.2182/cjot.2010.77.4.6 [ Links ]
28. Morrison T, Smith J. Working alliance development in occupational therapy: a cross-case analysis. Australian Occupational Therapy Journal. 2013; 60: 326-333. http://dx.doi.org/:10.1111/1440-1630.12053 [ Links ]
29. Alers V. The 20th Vona du Toit Memorial Lecture 2007: proposing the social atom of occupational therapy: dealing with trauma as part of an integrated inclusive intervention. South African Journal of Occupational Therapy. 2008; 38(3): 3-10. [ Links ]
30. Breen LJ. Professionals' experiences of grief counselling: Implications for bridging the gap between research and practice. Omega: Journal of Death and Dying. 2011; 62: 285-303. http://dx.doi.org/:10.2190/OM.62.3.e [ Links ]
31. Kübler-Ross E. Questions and answers on death and dying. New York: Macmillian; 1975. [ Links ]
32. Lister S, Pushkar D, Connolly K. Current bereavement theory: Implications for art therapy practice. Arts in Psychotherapy. 2008; 35(4): 245-250. http://dx.doi.org/:10.1016/j.aip.2008.06.006 [ Links ]
Submitted: 29 September 2021
1st Review: 18 January 2022
Re-submitted: 31 March 2022
2nd Review: 13 May 2022
Revised: 21 July 2022
Accepted: 4 August 2022
Corresponding author: Enos Ramano enosramano33@gmail.com
EDITOR: Blanche Pretorius
DATA AVAILABILITY: Upon reasonable request, available from corresponding author.
FUNDING: There was no funding for this study.
* Final year Occupational Therapy students at the time of the study
** Master's degree student at the time of the study


{kind=link}
{kind=link}