










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.52 no.3 Pretoria Dez. 2022
http://dx.doi.org/10.17159/2310-3833/2022/vol52n3a2
RESEARCH ARTICLE
Comparison of the sensory integrative function of South African infants to normative data on two standardised tests
Marica BothaI; Denise FranzsenII; Lindsay KochIII
IUniversity of the Witwatersrand, Johannesburg, South Africa https://orcid.org/00 00-0002-6607-186X
IIUniversity of the Witwatersrand, Johannesburg, South Africa http://orcid.org/0000-0001-8295-6329
IIIUniversity of the Witwatersrand, Johannesburg, South Africa https://orcid.org/0000-0002-7440-2331
ABSTRACT
BACKGROUND: The Dunn Infant Toddler Sensory Profile and DeGangi's Test of Sensory Functions in Infants are two standardised tests that are widely used by South African therapists to assess sensory integrative function in infants. There is, however, no research available on the validation of these standardised tests for a South African population. This research determined whether the normative data established in the United States of America on the Infant Toddler Sensory Profile and the Test of Sensory Functions in Infants were valid for use with South African infants between the ages of 7 and 18 months.
METHODOLOGY: A quantitative cross-sectional, descriptive, correlation study design was used to investigate the equivalence between the normative data from the United States of America and a sample of typically developing South African infants.
FINDINGS: The results indicated that the mean scores for the South African sample in five of the six processing sections of the Infant Toddler Sensory Profile and all quadrant scores, were in the lower range of the typical performance according to the normative data of the United States of America. On the Oral Processing Section and the Sensation-Seeking Quadrant, test results should be interpreted with caution due to the medium effect size indicating clinical differences to the reported norms. A higher percentage of South African infants had a clear definite difference "more than others" score compared to normative data from the United States of America. On the Test of Sensory Functions in Infants, the means of the frequency distribution for deficient, at risk, and typical for all five sections and the Total Test Scores for the South African sample were significantly different from the normative data of the United States of America and the mean scores fell into the lower range or below the range for the typical performance reported in the test manual.
CONCLUSIONS AND RECOMMENDATIONS: The Infant Toddler Sensory Profile can be used without substantial re-norming based on the findings related to this South African sample. Due to significant differences in scores on the Test of Sensory Functions in Infants, the first author questions the use of the test and recommends further research on South African infants with a larger population group. However, it should be noted that this study had a small sample size and therefore the results should be interpreted with caution and cannot be generalised.
Keywords: Ayres Sensory Integration®, Infant Toddler Sensory Profile, Test of Sensory Functions in Infants, sensory integrative dysfunction, sensory processing.
INTRODUCTION
Assessment is an essential first step in the occupational therapy process and guides the planning, the type, and intensity of intervention1,2. An accurate and valid assessment is important and supports evidence-based practice2. Therapists should ask if standardised tests have been validated in the population they are treating, as research has shown that populations often differ in their normative data due to environmental and cultural influences in response to assessments3. Thus, it cannot be assumed that the norms of the test manual of a standardised test automatically apply to a different population.
However, before embarking on substantial re-norming of any standardised test, the applicability of the published norms to a specific population should be investigated.
Several researchers, including Anastasi and Urbina4, Downing5, and Streiner et al.7, have reinforced the importance that, in addition to the studies completed by the test authors, independent investigators conduct further psychometric tests on populations other than those assessed by the test authors. These investigations of standardised tests assist in confirming the validity of the published test norms for the population with which they will be used.
The Infant Toddler Sensory Profile (ITSP)6 and the Test of Sensory Functions in Infants (TSFI)7 are widely used by South African occupational therapists8-10. However, there appear to be no published studies on normative data for populations other than in the United States of America (USA), where the tests were developed. Some international studies have been published that consider the psychometric properties of the Sensory Profile for other populations of older children13. One such study conducted by Brown et.al11 in Australia, found differences between the USA norms reported in the test manual and their study group. This reinforces the need to investigate the diagnostic properties of ITSP6 and TSFI7 to establish evidence for the efficacy of these tests12 for the South African population where research indicates that the tests are used in both clinical practice and research10,13,14.
Literature Review
Sensory development begins during the prenatal period, with the tactile and vestibular systems playing a primary role in the early development of sensory integration. In 1972, Ayres15 defined sensory integration as "the neurological process that organizes sensation from one's own body and from the environment and makes it possible to use the body effectively within the environment"15:11. According to Ayres18, as information enters through the senses, sensory integration takes place, which leads to planning and organising of behaviour. This in turn leads to an adaptive response, as well as learning, and the emergence of occupational engagement and social participation16,17. Feedback that occurs leads to the process of restarting another cycle of sensory information intake and adaptation17. Actions are then planned according to the interpreted sensory input16-18. Each individual has a unique regulatory sensory processing profile, which implies that each person has a different response to sensations, and an individual's sensory processing profile influences the way sensations are interpreted and comprehended.
Therefore, sensory integration has a significant influence on development and is fundamental to the learning, perception, and action of any individual19. Inconsistencies in the central nervous system's ability to process sensations lead to poor sensory modulation and/or poor praxis17. This can result in difficulties with processing or organising the sensory information needed by the individual to understand their bodies and the world around them20. Such difficulties have been named sensory integrative dysfunction (SID). Dysfunction has been reported to occur in all or just some of the sensory systems. Sensory integrative dysfunction can be identified from a very early age and has been found to lead to the development of dysfunctional parent-infant interaction patterns. These dysfunctional interaction patterns, in turn, have been reported to be affected by the temperament of the infants and have an impact on later learning and emotional development21. Since SID has been reported to have consequences for normal development, an accurate assessment of SID in infants is important to correctly identify and treat from an early age, thus facilitating normal development22-24. Accurate assessment and early intervention can prevent or minimise the development of behavioural problems, participation restrictions in activities of daily living, and educational activities in childhood21.
A method to ensure a valid assessment of sensory integration is to use standardised tests. An advantage of standardised tests is objectivity and quantitative scores25. This allows for a valid assessment that leads to focused treatment to address specific dysfunction. A limited number of standardised tests are available to assess SID in infants. A systematic review by Eeles et al.28 found only three assessments of sensory processing function in the age group from birth to two years. These were the Infant Toddler Sensory Profile (ITSP)6, the Test of Sensory Functions in Infants (TSFI)7, and the Sensory Rating Scale for Infants and Young Children by Provost and Oeter26. All three tests evaluate slightly different constructs of sensory processing function, and therefore comparing the results of the tests is difficult27. The ITSP and the TSFI assess components of sensory processing and sensory modulation within sensory integrative function6,7.
The TSFI28 is based on the Ayres15 model of sensory processing and identifies adequate sensory processing and reactivity, in five areas of sensory functioning that develop over the first year of life. That is, tactile deep pressure and reactivity to vestibular stimulation that develop early in infancy and visual-tactile integration, adaptive motor responses, and ocular-motor control that develop slightly later. These subdomains were specifically chosen because they are clinically significant in identifying infants with sensory integrative dysfunction and, particularly, infants at risk of developmental delay, as well as those with difficult temperament28. The ITSP is based on Dunn's13 conceptual model and considers sensory modulation in five sensory processes, placing the interaction between the neurological threshold and the behavioural response on a continuum in four quadrants. The quadrants reflect the neurological threshold, or the number of stimuli needed for the central nervous system to notice or react to stimuli and activate a behavioural response, which indicates the manner in which the infant/child responds to the thresholds. At one end of the continuum, thresholds are high, and more stimulation is needed for the child to notice and react. On the other end of the continuum, the thresholds are low, and the amount of stimulation needed for a child to notice or react is low. Children respond to counteract their thresholds, and a child will either respond passively to the stimulus or exert excessive energy, to respond to the threshold. Quadrant 1: Low Registration and Quadrant 2: Sensation Seeking indicates different high-threshold responses. Quadrant 3: Sensory Sensitivity and Quadrant 4: Sensory Avoiding indicates different low threshold responses. The ITSP provides a profile of the effect of sensory processing on functional performance in the daily life of the infant29.
Both ITSP and TSFI are norm-referenced assessments, where the individual's performance is compared to the performance of other individuals or a normative group. Comparison with others in the reference group is important as both tests are based on observation of infant behaviours, which can only be objectively assessed compared to other infants to identify dysfunction. Although norm-referenced assessments are the most common form of standardised tests25, a disadvantage of this is that the norms provided do not necessarily reflect the normal population within all socio-economic backgrounds and cultures30. Therefore, it is important to determine whether a standardised test is appropriate for the population in which the therapist intends to use it.
This study investigated whether the normative data established in the USA on the standardised ITSP6 and TSFI7 tests to assess sensory integrative function in infants, could be applied to South African infants between the ages of 7 and 18 months.
METHODOLOGY
Study design
To address the purpose of this study, a quantitative cross-sectional, descriptive, correlation study design was used to investigate the equivalence between the normative data of the USA and a small sample of typically developing South African infants.
Study population
Convenient cluster sampling was used to recruit 60 typically developing infants between the ages of 7 and 18 months of age from 17 child day-care facilities in the East Rand area of Gauteng, South Africa. A sample size was calculated using the population of the possible number of infants (approximately 140 infants) in the 17 child day-care facilities. Cochrane's formula was used, to determine that a sample size of 60 participants was needed to represent the population with a 5% margin of error31.
Inclusion and Exclusion Criteria
Full-term infants, born between 37 and 42 weeks of gestation, were included in the study. Infants with a diagnosed birth defect or gestational illness were excluded.
Research Tools
Three research tools were used to collect data for this study. Demographic sheet - A demographic sheet developed by the first author was used to collect personal information from both parents and the infant. The information collected included parental history, information regarding pregnancy and birth, as well as the medical history of the infant. Infant/Toddler Sensory Profile - is a parent questionnaire that provides scores for infants between the ages of birth and 36 months. There are two classification systems for the ITSP, one for infants aged birth to 6 months and one for infants aged 7 to 36 months. Due to the lack of test-retest reliability and the low coefficient alpha scores for the birth-to-6-month age group, only infants from age 7 months were included in this study. As the TSFI can only be used up to the age of 18 months, infants older than 18 months were excluded from the study.
Parents completed the 48-item judgment-based questionnaire. Each item is judged on a five-point scale that reports the frequency with which infants respond to various sensory experiences. After the parents completed the form, the first author used the specified scoring procedure to complete a summary score sheet indicating both section and quadrant scores. The quadrant grid was completed by assigning scores to the different responses in the following way: a score of one to 'almost always', a score of two to 'frequently', a score of three to 'occasionally', a score of four to 'seldom, and a score of five to 'almost never. Scores were then added to calculate the total score for each section and quadrant. Once this step was completed, the scores were transferred to a quadrant summary to indicate the range each quadrant score fell within. Each quadrant score falls into the following ranges on a normal distribution (Gaussian) curve (Figure 1, page 9):
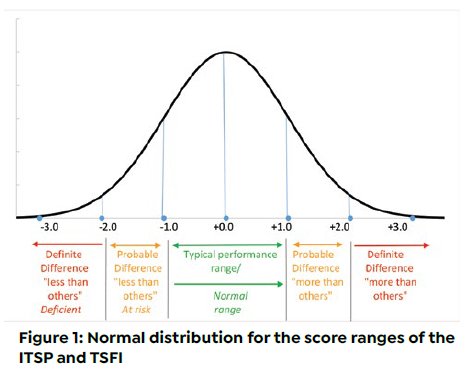
• Typical performance range: Scores between +1 SD and -1 SD.
• Probable difference "less than others/more than others": Scores between -1 SD and -2 SD are described as probable difference "less than others" and this indicates under- responsiveness. Scores between + 1 SD and +2 SD are described as probable difference "more than others" and this indicates over-responsiveness.
• Definite difference "less than others/more than others": Scores less than -2 SD are described as definite difference "less than others" and this indicates under responsiveness. Scores above +2 SD are described as definite difference "more than others" and this indicates over responsiveness (Figure 1, page 9).
Test of Sensory Functions in Infants is a therapist-administered observational test. It is used as a screening tool for SID in infants and is especially valuable when used in conjunction with other developmental tests. This test was standardised for infants between the ages of 4 and 18 months and is specifically recommended for infants with regulatory disorders, developmental delays, and infants that could be at risk of developing sensory processing or learning disorders7. The test consists of 24 items divided into five sub-tests of sensory processing and reactivity. These sub-tests are Deep Pressure, Adaptive Motor Functions, Visual-Tactile Integration, Ocular-Motor Control, and Vestibular Stimulation7. Scores fall into the following ranges on a normal distribution (Gaussian) curve (Figure 1, page 9):
• "Normal" range: Scores above -1 SD.
• "At risk" range: Scores below -1 SD but above -2 SD.
• "Deficient" range: Scores below -2 SD.
Research Procedure
Ethical approval (M110830) for this study was obtained from the Human Research Ethics
Committee (Medical) at the University of the Witwatersrand. The managers of the 17 child day-care facilities granted permission for the research to take place in their facility. Managers and teachers handed envelopes to parents containing study information as defined in an approved information sheet and consent forms. Once parents consented to participate by signing the consent forms, they completed the biographical questionnaire and ITPS and these were returned to school in a sealed envelope. The first author then assessed all eligible infants using the TSFI with the help of the teacher of the infant. The teachers' assistance consisted of holding the child on their lap according to the test procedure set out in the test manual7. After collecting all data, the tests were scored according to the procedure in the test manuals67. The data were then transcribed into Excel spreadsheets for analysis.
Data Analysis
Demographic data, as well as raw scores from both ITSP and TSFI, were descriptively analysed. To compare the scores of ITSP and TSFI, the z-scores of both tests were used and the frequency data were calculated for each component. For both ITSP and TSFI, the mean scores of the South African sample were compared with the range of scores provided for typical infants and toddlers from the USA. This was done for each subtest according to the age bands in the manuals. The significant difference using a chi-square test as well as the effect size (Cohen d)31 was calculated for the means on the ITSP since the mean values were available in the manual. The effect sizes, which are independent of the sample sizes, confirmed the standardised clinical differences between the South African sample and the USA norms. Since no mean scores have been published for the TSFI, except those for dysfunctional infants32, it was not possible to calculate effect sizes (d, Cohen)33 for the raw score data.
For all sections and sub-tests on the two measures, the percentage of participants scoring in each of the standard deviations was compared to the normal distribution. The significance in the frequency of the scores according to typical, probable, or definite differences for the ITSP and typical or deficient (-2SD) or at risk (-1SD) for the TSFI were calculated using a chi-square test.
RESULTS
The study population consisted of 34 males (56,7%) and 26 females (43.3%). The participants were divided into four age groups. A small percentage (6.7%: n=4) of the participants were between the ages of 7 and 9 months, while 36.7% (n=22) were between 10 and 12 months. The age group between 13 and 15 months was slightly smaller (16.6%: n=10) than the age group of 16 to 18 months, it was the largest group with 40.0% of the participants (n = 24).
Comparison of mean scores on the tests for the South African sample with the USA data
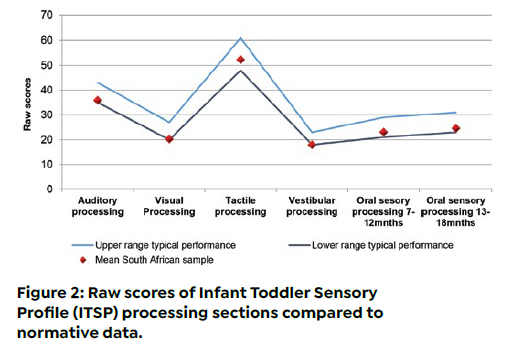
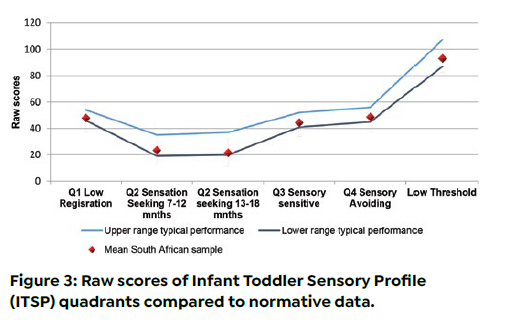
For ITSP, all sensory processing section scores (Figure 2, below) and quadrant scores (Figure 3, below) were found to be in the lower range of typical scores for infants and toddlers in the USA. Only the Tactile Processing Section score was similar to the scores reported in the ITSP manual, as the mean for South African infants fell at the centre of the range of scores for typical infants and toddlers in the USA.
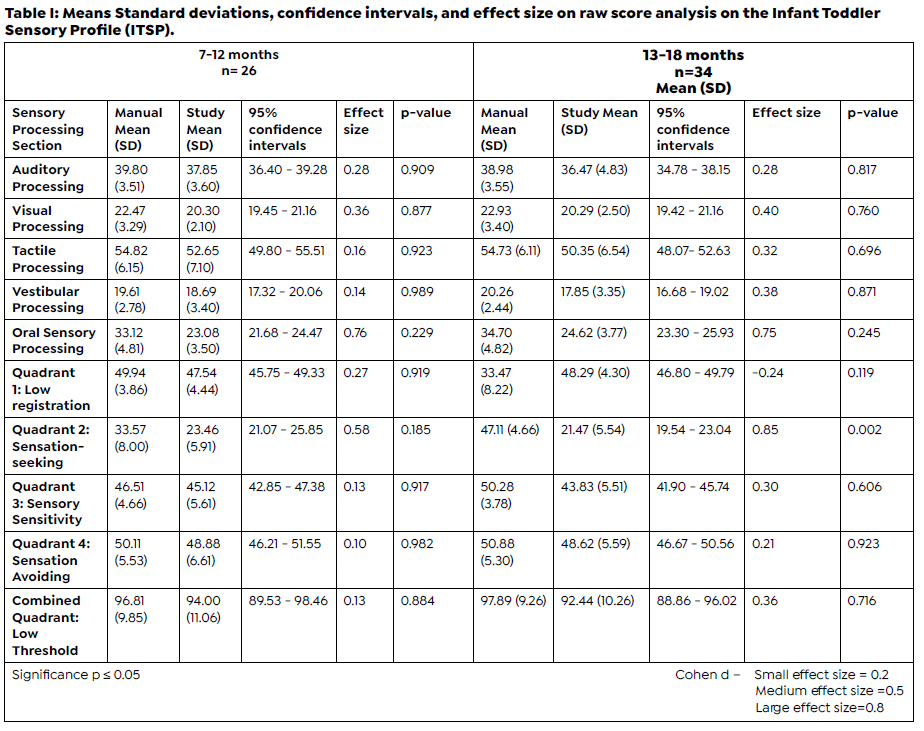
The mean scores provided in the ITSP manual and the mean scores of this study were compared for two age groups (7 to 12 months and 13 to 18 months). The effect size between the norms was calculated to confirm the standardised differences between the South African sample and the USA norms, to determine the clinical importance of interpreting dysfunction in the South African infant group. The results of this study indicated that all processing sections and quadrants had a small effect size, with the exception of Oral Processing and Quadrant 2: Sensation Seeking, which for both age groups had medium effect sizes (d > 0.5) (Table I, page 10).
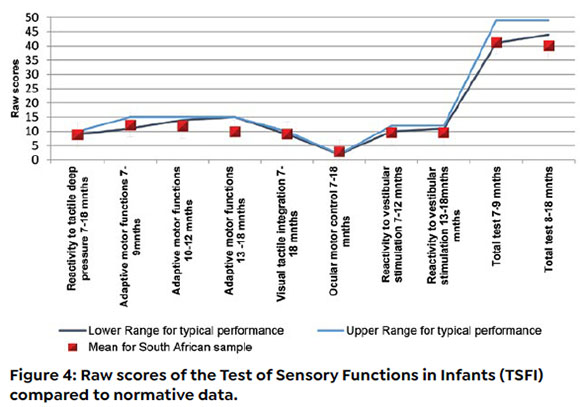
For the TSFI it was found that the scores for infants in South Africa on the sub-tests of Adaptive Motor Functions (10 - 12 months), Adaptive Motor Functions (13 - 18 months), as well as the Total Test Score (10 - 18 months) were equal to or below the lower range of scores reported for typical infants and toddlers in the USA (Figure 4, above).
Frequency of deficits identified in the tests for the South African sample
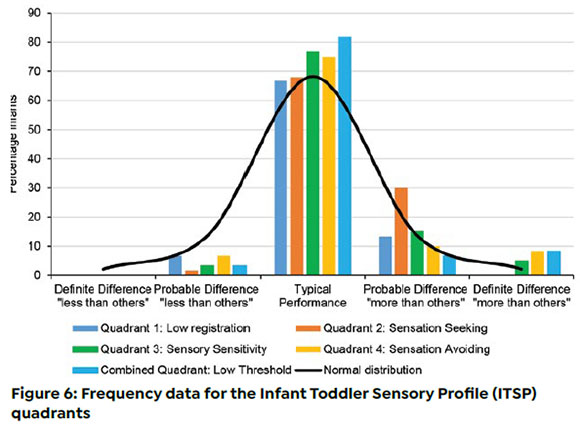
Mean scores cannot be considered ideal on the type of ordinal data obtained on the ITSP and the TSFI, and therefore the frequency distribution of the scores was determined and considered based on the Gaussian curve (normal distribution) as suggested in the test manual.The frequency data forthe ITSPand theTSFI indicated that significantly more South African infants tested within definite difference/deficient ranges according to the USA norms. In the ITSP, the frequency distributions for the South African sample show that a higher percentage of participants fell into the definite difference "more than others" score bracket in a normal distribution for the processing section (Figure 5, page 11) and quadrant scores (Figure 6, page 11). Very few infants fell into the probable difference "less than others" and the definite difference score bracket.
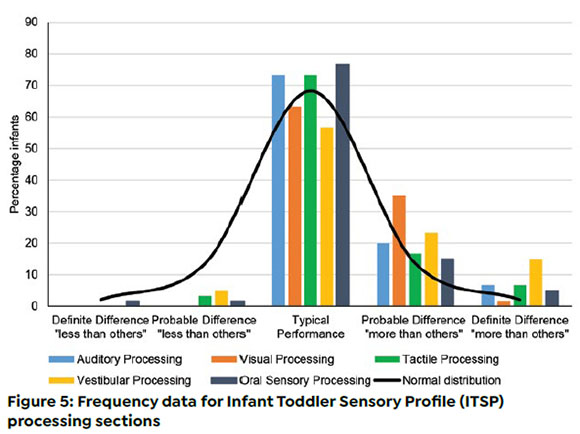
Vestibular Processing differed significantly from the normal distribution (p = 0.001), with a higher percentage of participants having a definite difference "more than others", as did Quadrant 1: Low Registration. It is important to note the percentage of infants that fall into the range of definite difference "more than others" in the Vestibular Processing Section (15.0%), as it is much higher than the expected percentage of 4.2% in the normal distribution.
For Oral and Auditory Processing, it also differed significantly from the normal distribution (p = 0.04), with a higher percentage of participants scoring in the typical performance range. A higher percentage of participants also scored in the range of probable difference "more than others" for Oral Processing.
The frequencies for three quadrants differed significantly (p= 0.001 to 0.010) from the normal distribution. These three quadrants, Quadrant 1: Low Registration (13.3%), Quadrant 4: Sensation Avoiding and Combined Quadrant: Low Threshold (8.3%) had a higher percentage of participants who scored in the range of definite difference "more than others". Quadrant 2; Sensation Seeking had a higher percentage of participants with a probable difference "more than others" at 30% compared to the expected 13.5% at this point on the normal distribution.
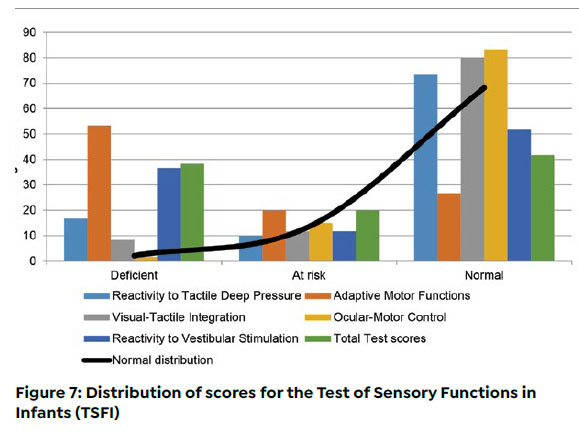
For the TSFI, the five sub-tests and the Total Test Score differed significantly (p=0.001) from the normal distribution (Figure 7, adjacent). As plotted on the left side of the Gaussian curve (normal distribution), Adaptive Motor Functions (53.3%), Reactivity to Vestibular Stimulation (36.6%) and Total Test Scores (38.3%) had much higher percentages than the expected 2.1% in the deficient range (-2SD), indicating problems with these components in the participants accessed. Sub-tests where a higher percentage of participants scored in the typical range included Reactivity to Tactile Deep Pressure (73.3%), Visual- Tactile Integration (80.0%) and Ocular-Motor Control (83.3%) which was higher than the expected 68.2%.
For both tests, it was observed that the sections related to vestibular processing had high percentages of infants that tested within the definite difference/ deficient ranges.
DISCUSSION
The USA sample for ITSP totalled 589 infants, with 301 males (51.1%) and 287 females (48.7%), while the USA sample for TSFI had 288 infants, with 130 males (45,1%) and 158 females (54,9%). Therefore, the gender distribution in the South African sample of 60 infants was similar to the male-female distribution in the USA samples for the ITSP, although the sample size was smaller. The age groups of the infants could not be stratified with a similar number in each of the age ranges of two months. This can be attributed to the fact that child day-care facilities have fewer infants under 9 months, since this age group requires a higher infant-to-carer ratio. Due to inclusion and exclusion criteria, the study participants were considered typical infants with no reports of major medical problems since birth.
Infant/Toddler Sensory Profile (ITSP)
The mean scores for the South African sample were in the lower ranges of the typical performance range according to the normative data found in the ITSP. The positive effect sizes of the South African sample mean that the scores were all lower than those of the USA sample with the exception of Quadrant 1: Low Registration for infants 13 to 18 months of age. These children may present as more passive because they do not notice or detect changes in sensory situations to a greater extent than the younger children in the sample. This may lead to infants appearing content and not receiving stimulation from caregivers, when, in fact, they need more stimulation.
Except for Quadrant 2; Sensation Seeking, none of the means for the South African sample differed from the mean scores for the USA sample. This was confirmed by effect sizes of d <0.4, which is considered acceptable as it indicates that the groups have a 70% overlap. This was confirmed in a study by van Jaarsveld et al.34 on the use of the Sensory Integration and Praxis Test in the South African population where they indicated that an effect size of d > 0.4 presented challenges in terms of interpretation of test results and the test had to be adjusted for the South African population34. The results of this study indicated that only in the Oral Processing Section (0.76 and 0.75) and the quadrant score for Quadrant 2: Sensation Seeking (0.58 and 0.65), there might be some challenges in interpreting the test results on this South African sample. Therefore, the ITSP could be used on similar South African samples, as there is less than half a standard deviation between the means.
When comparing the frequency data with the expected normal distribution, a significant difference was found for five of the nine sections and/or quadrants. To determine the clinical importance of these differences in interpreting dysfunction in South African infants, it was therefore important to establish if these differences indicated a higher percentage of participants with a probable and definite difference on the Gaussian curve (normal distribution) relative to the USA sample. The SA sample was found to tend to the "more than others" scores on the ITSP, indicating over responsiveness to sensory input. Particularly for probable and definite differences for the Vestibular Processing Section at 38%, which significantly deviates from the normal expected 15.7% on the normal distribution when the definite and probable difference "more than others" sections are combined. This section tests the infant's ability to process movement inputs and the infant's response to movement6. As the results of the Vestibular Processing Section deviated significantly from the normal distribution, the results from this section should be interpreted with care in South African samples.
Significant differences were also found between the expected and actual frequency for the Auditory and Oral Processing Sections, with more of the South African sample scoring in the typical range. For Oral Processing, more participants (23%) also tested within the probable and definite difference range "more than others". Oral processing tests the infant's ability to process sensations within the mouth thus the infant's response to taste and touch stimuli in the mouth6. Difficulties with oral sensory processing can lead to feeding problems, as it is found that children with these difficulties often have a diet of limited variety because they avoid food with certain textures16,17. Separate norms for the interpretation of the results could be required, and thus the results of the Oral Processing Section on the ITSP should be interpreted with caution in South African samples.
The Combined Quadrant: Low Threshold scores showed a significant difference from the expected USA frequencies in the normal distribution, with more participants in the South African sample falling into the typical performance range. A significant difference was found for the frequency of the scores for Quadrant 1: Low Registration and Quadrant 4: Sensation Avoiding with percentage scores in both quadrants tending towards the "more than others" ranges. Thus, participants in this sample showed more dysfunction in the low-threshold quadrants. Therefore, this aspect needs to be further researched since a significant difference was found for the South African sample for Quadrant 2: Sensation Seeking when the means were compared for the different age groups. This confirms the need to investigate the difference between the age groups.
For the interpretation of quadrant scores, Dunn's theoretical model of sensory processing, based on the infant's neurological thresholds, was used with passive response (low registration and sensory sensitivity) and active response (sensory seeking and avoidance of sensation) that usually results in one quadrant appearing to dominate when reacting to sensory input. The interaction between the continua may be seen with the other patterns of responsiveness also present6. Therefore, it is important to remember that behaviour of infants/toddlers consistent with one of the quadrants, on its own, is not sufficient to conclude that dysfunction is present. In the presence of performance difficulties in activities of daily living, behaviour consistent with the quadrants can help identify the reasons for their behaviour and also help to find ways to address the problem6.
Test of Sensory Function in Infants (TSFI)
The raw scores obtained from the South African sample were compared with the normative data found on the TSFI score sheet. The sub-tests that scored in the lower ranges of typical performance were Reactivity to Tactile Deep Pressure (7 - 18 months), Adaptive Motor Functions (7 - 9 months), Visual-Tactile Integration (7 - 18 months), Ocular-Motor Control (7 - 18 months), and Reactivity to Vestibular Stimulation (7 - 12 months). Other sub-tests, namely, Adaptive Motor Functions (10 - 12 months) and (13 - 18 months), Reactivity to Vestibular Stimulation (13 - 18 months), and the Total Test Score (8 - 18 months) scored below the normal range. Reactivity to Vestibular Stimulation subtest assesses the infant's reaction to different movements. According to the interpretation information, an infant with a deficient score may be considered posturally insecure and should be referred to an occupational therapist for further testing of neuromotor functions and other vestibular-based functions9. Since the mean score for the South African sample fell outside the range of typical infants in the USA, these infants would therefore be identified as deficient if assessed with this test.
Comparing the frequency data with the expected normal distribution, determining the frequency of participants scoring deficiencies, at risk, or typical, confirmed the results discussed above, with higher percentages of participants scoring as deficient. It is expected that only 2.1% of children will have scores within the deficient range. However, the results showed that the frequency scores for the Adaptive Motor Functions Subtest, the Reactivity to Vestibular Stimulation Subtest, and the Total Test Score were significantly higher. The Adaptive Motor Functions Subtest reflects the infant's ability to initiate and motor plan exploratory movements when handling textured toys. According to the information used for the interpretation of the test scores, these infants with poor adaptive motor functions would also be further tested for abnormal neuromotor functions and delayed motor skills7.
According to the test developer, if an infant obtains scores below the cut-off scores for the 'normal' range in the Total Test Score, it is indicative of potential problems. According to these criteria, 58,3% of the test population would therefore have scores indicative of potential problems. These children can be considered to be at risk for, or even considered to have abnormal sensory reactivity and processing. If an infant then also has delays in cognitive or motor skills, they should be referred to an occupational therapist to determine if intervention is needed. It is also recommended that infants with 'deficient' scores on the total test score or particular subtest scores be monitored throughout their preschool years for deficits in other areas of sensory integration, such as motor planning, visual motor skills, or bilateral motor coordination7. Therefore, it is important to know if the test accurately assesses an infant. If not, unnecessary referrals and further testing will be performed.
Since all sub-tests and the Total Test Score of the TSFI differed significantly from the population of the USA, this may result in unnecessary referrals and assessments when using the TSFI in South Africa. Therefore, the use of the test on South African samples is questioned. To use the TSFI with accuracy in South Africa, the sub-tests would need to be standardised on the population. The test items themselves may also be at fault since research by Jirikowic et al.32 suggest that TSFI scores should be interpreted with caution and should only be used in conjunction with other tests. The findings of this research study support this suggestion.
Limitations of the study
The results of this study must be viewed with caution, as it was limited by the very specific homogeneous sample as all participants attend child day-care facilities in a geographical area with middle to high income. This makes it difficult to generalise the findings to other infant groups in South Africa. The study had a small sample size. Therefore, the results should be interpreted with caution and cannot be generalised.
Due to the lack of a gold standard assessment tool for SID for this age group, the tests were compared to scoring on a normal distribution based on research on a sample, based in the USA.
CONCLUSION AND RECOMMENDATIONS
The mean scores for the ITSP fell into the lower typical range of the USA data. The mean scores for the age group 13 to 18 months differed significantly from the USA means and the means for the Oral Sensory Processing Section and Quadrant 2: Sensation Seeking, showed clinical differences from the USA means with a medium effect size. The frequency differed significantly compared to the normal distribution for five of the nine sections and quadrants. The high percentage for the definite and probable difference "more than others" for Vestibular Processing Section and Quadrant 1: Low Registration indicates that a typical SA sample can be identified with problems in these components that appear to differ from those reported for infants in the USA. This further indicates that the scores from these sections should be interpreted with caution in South African samples.
The results of this study indicated that using the USA normative data to score the TSFI on South African samples is even more problematic. The infants in the South African sample scored outside the lower ranges in the sections for Adaptive Motor Functions (age groups 10 to 12 months and 13 to 18 months), Reactivity to Vestibular Stimulation (13 to 18 months), as well as the Total Test Score (8 to 18 months) compared to the sample from the USA. A significant difference was found for the frequency of the deficient, at risk and typical percentages on a normal distribution for all the sub-tests and the Total Test Scores. According to the results of this study, to use the TSFI with confidence in South Africa, the sub-tests would need to be standardised for this specific population.
Therefore, the following recommendations are made in accordance with the findings of this study:
• It is recommended that further research be done on the use of ITSP and TSFI in a South African population.
• As the study had a small sample, it could be inaccurate to generalise the findings, and it is therefore recommended to do the study on a larger South African sample. This needs to include participants from a diverse demographic and socioeconomic population.
• It is recommended that further research is needed on the influence of the child's day-care environment on the development of sensory integration function in infants.
Author contributions
Marica Botha completed this study towards a Master's degree in occupational therapy and was responsible for the conceptualisation of the study, data collection, and analysis. She drafted the original manuscript, edited the manuscript, and approved the final version to be published. Denise Franzsen was a study supervisor, guided conceptualisation and design of the study and was an expert in data analysis and interpretation supervision. She revised it critically for intellectual content, supervised the writing and revision of the manuscript and approval of the final version to be published. Lyndsay Koch was a study supervisor and guided the process from the conceptualisation and design of the study and revising it critically for important intellectual content. Approval of the final version to be published. The authors agree to be responsible for all aspects of the work and to resolve all questions related to the accuracy and integrity of any part of the work.
Conflicts of interests
The authors have no conflicts of interests to declare
REFERENCES
1. Stewart KB. Occupational Therapy Evaluation in Pediatrics. In: Case-Smith J, O'Brien JC (eds.) Occupational Therapy for Children. 6th ed. Missouri: Mosby Elsevier; 2017. p. 193-215. [ Links ]
2. American Occupational Therapy Association. Occupational therapy practice framework: Domain and process (4th ed.). American Journal of Occupational Therapy. [Online] 2020;74(Suppl 2: 1-87. Available from: https://doi.org/10.5014/ajot.2020.74S2001 [ Links ]
3. Dunn W. Performance of typical children on the Sensory Profile: an item analysis. The American journal of occupational therapy. [Online] 1994;48(11): 967-974. Available from: https://doi.org/10.5014/ajot.48.11.967 [ Links ]
4. Anastasi A, Urbina S. Psychological testing. 7th ed. Upper Saddle River, New Jersey: Prentice Hall International; 1997. [ Links ]
5. Downing S. Validity: on the meaningful interpretation of assessment data. Medical Education. [Online] 2003; Available from: https://doi/10.1046/j.1365-2923.2003.01594.x [ Links ]
6. Dunn W. Infant/Toddler Sensory Profile User's Manual. San Antonio: Psychological Corporation; 2002. [ Links ]
7. DeGangi G., Greenspan S. Test of Sensory Functions in Infants User's Manual. [Online] Los Angeles, California: Western Psychological Services; 1989. Available from: https://doi.org/10.5014/ajot.45.2.188c [ Links ]
8. Lecuona E, Van Jaarsveld A, Raubenheimer J, Van Heerden R. Sensory integration intervention and the development of the premature infant: A controlled trial. South African Medical Journal. [Online] South African Medical Association; 2017;107(11): 976-982. Available from: https://doi.org/10.7196/SAMJ.2017.v107i11.12393 [ Links ]
9. Lecuona ER, van Jaarsveld A, van Heerden R, Raubenheimer J. The developmental status and prevalence of sensory integration difficulties in premature infants in a tertiary hospital in Bloemfontein, South Africa. South African Journal of Occupational Therapy. [Online] The Occupational Therapy Association of South Africa (OTASA); 2016;46(1): 15-19. [ Links ]
10. Jorge J, de Witt PA, Franzsen D. The effect of a two-week sensory diet on fussy infants with regulatory sensory processing disorder. South African Journal of Occupational Therapy. 2013;43(3): 28-34. [ Links ]
11. Brown T, Morrison IC, Stagnitti K. The reliability of two Sensory Processing scales used with school-age children: Comparing the response consistency of mothers, fathers, and classroom teachers rating the same child. Journal of Occupational Therapy, Schools, and Early Intervention. [Online] 2010;3(4): 331-347. Available from: doi:https://doi.org/10.1080/19411243.2010.541775 [ Links ]
12. Crawford SG, Wilson BN, Dewey D. Identifying Developmental Coordination Disorder: Consistency Between Tests. Physical & Occupational Therapy In Pediatrics. [Online] 2001;20(2-3): 29-50. Available from: https://doi.org/10.1080/J006v20n02_03 [ Links ]
13. Nieder-Heitmann E. Impact of a sensory developmental care programme for very low birth weight preterm infants in the neonatal intensive care unit. University of Stellenbosch; 2010. [ Links ]
14. Lecuona E. Sensory Integration Intervention and the Development of Extremely Low to Very Low Birth Weight Premature Infants. University of the Free State; 2012. [ Links ]
15. Ayres AJ. Sensory integration and learning disorders,. Western Psychological Services; 1972. 294 p. [ Links ]
16. Parham LD, Mailloux Z. Sensory Integration. In: O'Brien JC, Kuhaneck HM (eds.) Case-Smith's Occupational Therapy for Children and Adolescents. 8th ed. St. Louise, Missouri: Elsevier; 2020. p. 516-549. [ Links ]
17. Bundy AC, Lane SJ. Sensory Integration Theory and Practice. 3rd ed. Philadelphia: F.A. Davis; 2020. [ Links ]
18. Ayres AJ. Sensory integration and learning disorders,. Western Psychological Services; 1972. 294 p. [ Links ]
19. Kandel ER, Schwartz JH, Jessell TM. Principles of Neural Science.. 5th ed. Philadelphia: McGraw-Hill; 2000. [ Links ]
20. Coleman GG, Mailloux Z, Smith Roley S. Sensory Integration Answers for Parents. Santa Rosa, CA: Crestport Press; 2004. [ Links ]
21. Dipietro JA, Greenspan SI, Porges SW. Psychophysiological Characteristics of the Regulatory Disordered Infant GEORGIA A. DEGANGI Regional Center for Infants and Young Children. [Online] Available from: https://doi.org/10.1016/0163-6383(91)90053-U. [ Links ]
22. DeGangi GA, Sickel R, Wierner A, Kaplan E. Fussy babies: Do treat or not do treat? British Journal of Occupational Therapy. [Online] 1996;56(10): 457-464. Available from: doi:Available from: https://doi/10.1177/030802269605901003 [ Links ]
23. Wierner A, Long T, DeGangi GA, Dataille B. Sensory processing of infants born prematurely or with regulatory disorder. Physical & Occupational Therapy In Pediatrics. 1996;16(4): 1-17. [ Links ]
24. Harris S., Daniels L. Content validity of the Harris Infant Neuromotor Test. Physical Therapy. 1996;76(7): 727-737. [ Links ]
25. Miller LJ. Developing Norm-Referenced Standardized Tests. Miller LJ (ed.) New York: The Haworth Press; 1989. 226 p. [ Links ]
26. Provost B, Oetter P. The Sensory Rating Scale for Infants and Young Children. Physical & Occupational Therapy In Pediatrics. [Online] 1994;13(4): 15-35. Available from: 10.1080/J006v13n04_02 [ Links ]
27. Eeles AL, Spittle AJ, Anderson PJ, Brown N, Lee KJ, Boyd RN, et al. Assessments of sensory processing in infants: A systematic review. Developmental Medicine and Child Neurology. [Online] 2013;55(4): 314-326. Available from: 10.1111/j.1469-8749.2012.04434.x [ Links ]
28. DeGangi G., Greenspan S. Test of Sensory Functions in Infants User's Manual. Los Angeles, California: Western Psychological Services; [ Links ]
29. Dunn W. Sensory Profile User's Manual. San Antonio: The Psychological Corporation; 1999. [ Links ]
30. Hegde M, Pomaville F. Standardized Assessment. Assessment of Communication Disorder in Children: Resources and Protocols. 2nd ed. San Diego: Plural Publishing Inc.; 2012. p. 41-66. [ Links ]
31. Bartlett JE, Kotrlik JW, Higgins CC. Organizational research: Determining appropriate sample size in survey research. Information Technology, Learning, and Performance Journal. [ Links ]
32. Jirikowic TL, Engel JM, Jean C. The Test of Sensory Functions in Infants: Test-Retest Reliability for Infants With Developmental Delays. The American Journal of Occupational Therapy. [Online] 1997;51(9): 733-738. Available from: 10.5014/ajot.51.9.733 [ Links ]
33. Cohen J. Power Primer. Psychological Bulletin. 1992;112(1): 155-159. [ Links ]
34. van Jaarsveld A-M, Mailloux Z, Herzberg DS. The Use of the Sensory Integration and Praxis tests with South African Children. South African Journal of Occupational Therapy. 2012;42(3): 12-18. [ Links ]
Submitted: 5 February 2021
Reviewed: 3 September 2021
Revised: 16 November 2021
Accepted: 3 December 2021
Corresponding author: Marica Botha marica.botha@wits.ac.za
EDITOR: Blanche Pretorius
DATA AVAILABILITY: Upon reasonable request, available from corresponding author
FUNDING: No funding was obtained for this study


{kind=link}