










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.52 n.2 Pretoria Aug. 2022
http://dx.doi.org/10.17159/2310-3833/2022/vol52n2a3
RESEARCH ARTICLE
Factors influencing prevention and early intervention within the disability claims management process: South African insurer's perspective
Kerri-Lee HowellI; Pragashnie GovenderII; Deshini NaidooIII, *
IPrivate Practice, Gauteng, South Africa https://orcid.org/0000-0002-8988-10211
IIDiscipline of Occupational Therapy, School of Health Sciences, University of KwaZulu-Natal, South Africa https://orcid.org/0000-0003-3155-3743
IIIDiscipline of Occupational Therapy, School of Health Sciences, University of KwaZulu-Natal, South Africa https://orcid.org/0000-0001-6276-221X
ABSTRACT
INTRODUCTION: The disability claims management process may be divided into four stages: prevention, early intervention, rehabilitation, and return to work. There are various stakeholders involved in the process and various factors that influence the process. Currently, there is a lack of literature that creates insight into the prevention and early intervention stages.
METHOD: An explorative qualitative study was conducted with 26 purpo-sively sampled stakeholders from the disability insurance sector. Qualitative data from virtual individual semi-structured interviews were inductively thematically analysed, using NVIVO Pro 12, to establish emergent themes.
RESULTS: Four inhibiting and four facilitating factors emerged from the data analysis. Inhibitors included: psycho-social-economic hardship, group insurer inhibitors, disability stigma and deconditioning and poor health, and disability understanding. Facilitators included: group insurer facilitators, a remain-at-work (RAW) approach, medical and vocational management, and social and occupational support. The overarching theme emphasised disability as a complex phenomenon influenced by various medical and non-medical factors
CONCLUSIONS: The complexity of a disability contributes to the disability claims management process, which lacks focus on prevention and early intervention. Despite this complexity, retaining an employee at work while receiving early intervention emerged as a meaningful approach to decreasing the likelihood of the employee's ill health progressing to long-term disability.
Keywords: remain-at-work, vocational management, disability income replacement insurance
INTRODUCTION
Key stakeholders within the disability management ecosystem are the employee and their community (family and friends), the employer (line manager and human resources), the employee assistance programme (EAP) services, the treating health professionals (medical, occupational health and occupational therapist) and the group disability insurer (disability claims managers and disability claims broker). These stakeholders exist within a disability ecosystem of intersecting environments and influencing factors are best described using Bronfenbrenner's model of human ecology1. In the context of this study, the micro-level environments include the direct relationships that the persons experiencing ill-health (the employee) have with their social networks, their workplace networks, and their health professional networks. The meso-level environments include the broader workplace, health professionals, and insurer stakeholders interacting with the micro-level environments. The macro-level environments include South African socio-economic environments such as the labour market, the health care system, and the social constructs surrounding disability. Within all these environments, there are various influencing factors.
Employee health and well-being occur along a continuum. During the opening prevention stage, an employee is healthy and at work2. During the early intervention stage, an employee has health risks or ill health symptoms at work2. If employees progress through these two stages, they experience ill-health resulting in short or long-term disability leave2. The high costs associated with short- and long-term disability absence drive a need for a proactive approach to wellness that leverages prevention and early intervention strategies3. Prevention of ill-health and disability in the workplace comprises strategies that aim to ensure independence in occupational performance4,5. If prevention is not achieved, the focus shifts to early intervention, which is the provision of support that assists an employee in navigating the options for rehabilitation and accommodation within the first 30 days following ill-health that may impact attendance and/ or work performance6.
Along the employee ill-health and disability continuum, several environments and stakeholders create an ecosystem that influences the cost and complexity of disability. Using a multistakeholder approach, the study aimed to explore factors that influence prevention and early intervention within the South African disability claims management process. Inhibiting and facilitating factors within the disability ecosystem were explored to create more significant insights into how these factors influence the prevention and early intervention of ill-health and disability.
Literature review
When considering productivity along with the employee ill-health and disability continuum, it was previously assumed that work attendance meant employees were productive. However, health-related costs of productivity are now being linked equally to employees showing up at work while experiencing ill-health (known as presenteeism) and when employees are not at work due to ill-health (known as absenteeism)7. In the absence of a disability management policy, procedure or programme, employer stakeholders such as managers and human resources use their discretion to monitor whether an employee's ill-health and/or disability impacts their productivity at work8. Due to a lack of knowledge regarding ill-health and disability9, the lack of utilising prevention and early intervention strategies4,10 and the complex factors influencing employee health and productivity at work, the likelihood of ill-health and long-term disability occurring remain high.
Within South Africa, various risk factors may inhibit employee health and well-being, including the risk of unemployment, the risk of unmanaged mental health and the risk of unmanaged non-communicable diseases11. The risk of unemployment in South Africa is seen in the prevalence of job insecurity in the employed population11. Job insecurity applies to both the employed and unemployed population as it includes the employed population who feel threatened by the risk of unemployments. Job insecurity is partly a product of South African work-life being subject to dramatic economic recessions, technology development and industrial restructuring11. The COVID-19 pandemic has worsened the prevalence of job insecurity as it has forced many companies to take austerity measures such as retrenchments and unpaid salaries that create further job insecurity for workers12. These changes result in organisations needing to remain profitable in an unpredictable environment either by increasing their gains or decreasing their costs12. The latter is often done by reducing the number of employees13. With this in mind, it is understandable that job insecurity is associated with high levels of burnout, depression, anxiety and psychosomatic complaints11,13.
If an employee experiences these various mental health symptoms, there is a compounding risk of not being managed optimally11,14. A statistic that reflects the risk of unmanaged mental health is that 60% of South Africans are likely suffering from post-traumatic stress14. The prevalence of poor mental health often results in absences in the workforce, illness at work and health-related early retirement, ultimately resulting in the country's productivity and creativity being hindered15. Freeman, Simmonds & Parry (2020)15 further highlight that within South Africa, social and community cohesion is deeply obstructed by financial and relationship pressure caused by mental and physical ill-health. Whether an employee experiences mental ill-health, physical ill-health, or a combination of the two, access to appropriate treatment for this ill-health remains a difficulty within South Africa16. This lack of access is linked to the decline of the national health system as less than 16% of South Africans can afford medical aid insurance, resulting in an over-burden on the public health care system16. Of the South African's who purchase medical insurance, most select hospital cover due to premium affordability16. This choice leads to over-utilisation of hospital services, fragmented care and a lack of investment in preventative and early intervention health care at a community level16. These factors increase the likelihood of an employee progressing along the health continuum from being healthy and at work to unhealthy and absent from work. As the employee progresses along the continuum, the bond to his or her workplace is often broken which can profoundly impact the individual, the employer and society as there is less receptiveness to the employee remaining or returning to the workplace2.
With the above in mind, one can understand that income replacement claims have doubled over the past ten years, denoting a continued hindrance of South Africa's productivity and creativity15, and unmanageable resource costs for employers and insurers7. Although these factors are not within the full control of one stakeholder within the disability ecosystem, research shows that having a disability management policy that focuses on prevention and early intervention strategies facilitates continued employment of employees experiencing ill-health within the work-place2,8,10. Within South Africa, there is various legislation on how ill-health and disability is to be considered in the workplace - the goal of the legislation is to promote the retention of employees who experience ill-health and disability17. In addition to legislation, key stakeholders may perform various activities to encourage prevention and early intervention. One of these key stakeholders is the group disability income replacement insurer who can collaborate with the employer stakeholders involved in the employee assistance programme and occupational health and safety programmes18. This collaboration aims to establish employee education programmes that assist employees in understanding how to maintain optimal health and productivity18. Another key stakeholder is healthcare providers, who may implement regular mental and physical health care screenings. Where necessary, they may encourage their patients to return to work shortly after ill-health, provided that return to work does not endanger the patient, their co-workers, or society19. Lastly, employers are critical stakeholders in that they may ensure all ill-health issues are handled sensitively and confidentially within a supportive and trusting working environment20. This type of environment decreases the fear and prejudice of disability and, where necessary, allows for accommodations to be provided for employees experiencing ill-health17,20.
Workplace attendance and absenteeism are complex, multidimensional issues that involve an intersection of employee, employer, work environment, social environment and economic environment factors. From the evidence available, the development of a disability management policy focusing on prevention and early intervention of ill-health and disability is considered a highly effective way to mitigate these complexities thereby ensuring employees remain healthy and, if they experience ill health, that they recover as effectively as possible2, =5, 6 10.
Disability-related legislation emphasises that employers are required to accommodate employees experiencing ill-health8, and vocational rehabilitation proposes strategies for those experiencing disabilities to return to work. However, there is a lack of research around prevention and early intervention for disabilities within the workplace2. This study aims to identify the factors that influence a preventative and early intervention approach to disability claims management within South Africa.
METHODOLOGY
The presentation of the study's methodology has been informed by the Consolidated Criteria for Reporting Qualitative Studies (COREQ) Guidelines21.
Study design and research team
The study explored each stakeholder's (participant's) experience and knowledge of the disability claims management process using an exploratory qualitative design. The study's research team comsisted of the first author, two co-authors and a co-facilitator. All four members of the team are qualified, female occupational therapists. The first author and co-facilitator were acquainted with most of the stakeholder's as they work in the disability insurance industry.
Selection and sampling strategy
The target sample included 40 identified stakeholders involved in private insurance disability claims management processes in South Africa, accessed via maximum variation purposive sampling. The stakeholders were selected based on their unique knowledge and experience within ill-health intervention and disability insurance. The first author was acquainted in a professional capacity with many of the stakeholders, but had, however, only worked closely with one stakeholder. Due precaution to manage bias was taken and is expanded on under the Trustworthiness section below. There were thus no relationships that unduly influenced the study recruitment and data collection processes. The stakeholders were informed of the aim of the study.
Stakeholders were required to have a minimum of two years' experience working in ill health intervention or disability insurance. The diversity of the stakeholders was ensured through recruitment from various companies and points within the disability claims management process. This variability added to the diversity of the study as each stakeholder brought their unique knowledge and experience. The experience and diversity of stakeholders were necessary for the study to capture a multi-stakeholder perspective.
An expression of interest email was sent to five stakeholders per stakeholder group (n=40), of which 26 stakeholders responded. The stakeholders who responded included human resource managers (n=4), employee wellness specialists (n=3), occupational health medical practitioners (n=4), group insurance disability claims brokers (n=3), health risk managers (HRM) (n=3), group insurance disability claims assessors (n=3), vocational/case management occupational therapists (n=3) and group insurance reinsurance disability claims managers (n=3). All stakeholders who responded were included in the study for an interview.
Data collection procedure
The study accounted for the heterogeneity of the stakeholders, using semi-structured individual interviews as these types of interviews elicit deep discussions of one's knowledge and experiences. Before the interviews, open-ended questions were prepared based on international and South African literature focusing on factors influencing prevention and intervention within disability claims management22. The questions were refined through a peer debriefing with the study's co-authors and a pilot study conducted with three stakeholders. The pilot study highlighted that restructuring of the first question was required. The question was then adapted to be more succinct. Where necessary, probing questions were asked during the interviews23.
The stakeholder interviews were conducted in English by the first author and a co-facilitator who has experience in the field of disability management. Member (stakeholder) checking and validation occurred during the interviews, with paraphrasing and summarising of the stakeholder's responses. The interviews occurred on a virtual platform (Microsoft Teams) and lasted for approximately 60 minutes. Interviews were audio-recorded and transcribed verbatim.
Data analysis
The initial data analysis involved the first author, a co-author, and the co-facilitator of the interviews, each individually reviewing a transcript for coding. These three individuals then discussed their coding to decide on a coding approach. Following this, the transcripts for each interview were uploaded onto NVIVO 12 Pro24. An inductive thematic analysis process by the first author ensued25. The first step involved the first author reading and re-reading the transcribed information to generate initial explicit and interpretive codes for as many potential themes as possible25. The next step involved refo-cusing the analysis to broader themes by considering whether the codes should be combined or become sub-themes25. The themes were then reviewed to form a coherent pattern that captured each theme's essences while ensuring that the themes were not too broad or complex. During these steps, peer-debriefing took place through the co-authors auditing the coding process. The final step involved compiling a concise, coherent, and interesting account of data across the themes with data extracts embedded in the analytical narrative to demonstrate the prevalence of the theme.
Trustworthiness
The first author engaged in reflexivity throughout the research process, specifically, by suspending judgment, analytical memos (information notes about bias, perspectives, observations and details about the interviews), data checking and peer debriefing25. Reflexivity was necessary to ensure that any potential for bias was managed.
Credibility was established through the purposive sampling of stakeholders who were able to contribute to the research question26, and through emphasising concepts of confidentiality and anonymity to encourage honest and open responses. Transferability was confirmed by providing thick descriptions25 and dependability was ensured by applying a logical, traceable, and documented research process26. The transcripts and themes underwent investigator triangulation to ensure quality data analysis. Stakeholders from various fields and points within the disability management process who participated in the study achieved exposure and understanding of the phenomenon. Confirmability of the study was achieved by ensuring credibility, transferability, dependability and triangulation, thus highlighting data that correctly represented information the stakeholders provided, preventing researcher bias.
Ethical clearance and considerations
The University of KwaZulu-Natal Humanities and Social Sciences Research Ethics Committee provided ethical approval for the study (reference number HSSREC/00002870/2021). An information letter outlining the details of the research study and a consent form were subsequently sent to the stakeholders. In soliciting informed consent, stakeholders were aware that their participation was autonomous and voluntary, with a right to withdraw from the study at any point. Throughout the study, restricted data access, anonymity, and confidentiality principles, informed by the Protection of Personal Information Act (POPIA), were followed to ensure high-quality data protection processes.
FINDINGS
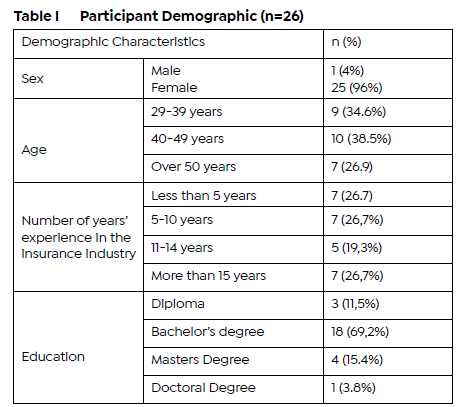
The demographic profiles of the participants in this study are presented in Table I (below).
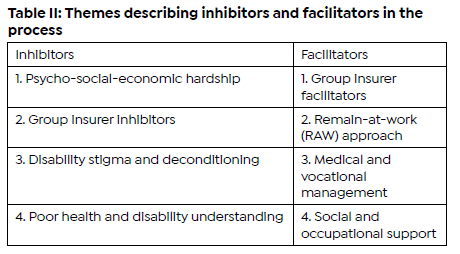
Emergent Themes: Two main themes emerged from the data, namely, factors that inhibit prevention and early intervention and factors that promote prevention and early intervention. Each theme had four associated subthemes which have been described using verbatim quotes from the stakeholders. Table II (below) highlights the themes and subthemes in descending order of the frequency each theme was mentioned by the stakeholders. The frequency order was determined by the number of stakeholders whose opinions spoke to each subtheme.
Theme 1: Inhibitors of prevention and early Intervention in the disability management process
Psycho-social-economic hardship
Stakeholders noted that the current recession of the South African economy leads to a lack of employment availability. The focus on the economy was often followed by a focus on the negative political climate within South Africa.
"Our political climate makes people despondent and has a massive impact on emotional well-being" (stakeholder13, vocational/case management occupational therapist).
Another frequently mentioned factor was barriers or delays in South Africans accessing medical and occupational health care when they experience ill-health thereby complicating their recovery.
Stakeholders further elaborated that many South Africans experience stress from pressure to remain at work while ill. Conversely, stakeholders noted that for many South Africans in receipt of a disability income replacement benefit, there is increased stress from being over-reliant on their disability income replacement, limiting their ability to focus positively on their recovery.
Group insurer inhibitors
This sub-theme describes data revealing factors that inhibit prevention and early intervention in the group disability insurance industry. Stakeholders mentioned that insurers are not proactive in the disability process as they lack engagement and leveraging of the relationship they have with employers to whom they provide insurance. This lack of proactivity was considered to be compounded by insurers being unwilling to innovate their policies and processes due to the competitive industry (like-for-like comparison of various companies offering group insurance disability products). Stakeholders expressly noted that, "We need to change the way we manage ongoing disability - bring more behavioural economics into the whole practice." (stakeholder 19, group insurance reinsurance disability claims manager)
Disability stigma and deconditioning
Stakeholders highlighted two exacerbating issues within this theme. The first was a lack of disability disclosure due to fear of judgement, resulting in employees waiting too long before seeking help (disability stigma). The second was a deconditioning that occurs when some employees are no longer in the work environment as they adopt a disability mindset that lacks the incentive to return to work. Moreover, many individuals receiving a disability income replacement benefit are afraid of losing their benefit, which drives them to exaggerate their symptoms to remain disabled. However, stakeholders noted that not all individuals receiving a disability income replacement benefit are concerned about stigma or are subject to deconditioning - rather, these individuals are focused on remaining or returning to work by overcoming their ill-health symptoms.
Poor health and disability understanding
Stakeholders described how employer stakeholders within the disability process have a poor understanding of optimising and maintaining good health by preventing and intervening on disability within the workplace. Stakeholders pointed out that often the focus is on employee performance management rather than on intervention to support the employee remaining at work. This poor understanding often leads to a strained relationship between the employee and the employer.
"For employers, there isn't enough capacity to understand what early identification is and more often it goes straight from poor performance into a performance management." (stakeholder 16, group insurance reinsurance disability claims management).
Stakeholders noted doctors can be an inhibiting influence when they do not support employees remaining or returning to work despite impairment in the employees functioning.
"If doctors support the person not working, it if incredibly difficult to get them to work." (stakeholder 18, group insurance reinsurance disability claims manager).
Lastly, stakeholders noted occupational therapists can be an inhibiting influence in that they are "unrealistic about what they can expect an employer to do in terms of accommodating a person" (stakeholder 16, group insurance reinsurance disability claims manager).
Theme 2: Facilitators of prevention and early intervention in the disability management process
Group insurer influences
Several stakeholders noted a facilitating factor was group disability insurers who provide funding for rehabilitation, who have a good relationship with their client (employer) and who have occupational therapists and/or multi-disciplinary teams as claims handlers. Additional facilitating influences were brokers involved in planning and communication, and objective third party occupational therapists who fit the client's (employer) needs.
"Insurers need to understand what the employer looks like, what HR looks like, what services they have within the insurer can draw from. If you do a lot of work upfront, you've got a whole lot of less work going forward" (stakeholder 22, Group insurance reinsurance disability claims manager).
Remain-at-work (RAW) approach
The RAW approach emerged as a theme from stakeholders emphasising the importance of the employer stakeholders and medical practitioners implementing risk strategies to identify employees with signs and symptoms of disability; and following this identification with intervention strategies to improve these signs and symptoms. Within this identification, stakeholders expressly noted the value of an occupational therapist conducting a workplace assessment to identify areas that may be improved with rehabilitation.
"HR contacts the OT and says we've identified these difficulties and then the OT goes into the workplace to assess for areas that may improve with rehabilitation" (stakeholder 7, group insurance disability claims assessor)
Additional emphasis was placed on how stakeholders improve the vocational prognosis when demonstrating a supportive attitude to the employee remaining at work while experiencing and recovering from a medical condition.
"I don't think waiting for maximal medical improvement should be an obstacle in returning somebody to work, we should be doing it while they are at work". (stakeholder 12, group insurance disability claims assessor)
Social and occupational support
Stakeholders identified social and occupational support as a faciltiating factor for prevention and early intervention. When this support is in place, it facilitates employees well-being during their illness and injury recovery.
Social support was identified as families, peers and communities showing support through encouragement and knowledge sharing on healthy behaviours.
"One's community can play an integral part when it comes to early intervention and prevention because knowledge spreads within communities" (stakeholder 12, occupational health medical practitioner).
Occupational support included employees accessing EAP counselling services and line managers expressing appreciation and understanding for the employees ill-health recovery.
"The disability process is anxiety provoking so if they have contact with the EAP they are more likely to feel supported." (stakeholder 23, employee wellness specialist).
Medical and vocational management
The importance of early rehabilitation and chronic disease management programmes for employees at risk of experiencing long term disabilities was emphasised by stakeholders. The treating doctors and occupational health medical practitioners were noted as key stakeholders in ensuring this 'pre-hab" (holistic medical and vocational management that occurs during prevention and early intervention stages while the employee is at work)..
Within vocational management, emphasis was placed on occupational therapists having the necessary vocational skills and being able to understand the work context, medical information and ability to provide advise on reasonable accommodations.
DISCUSSION
The impact of long-term disability on disabled individuals and their communities, employers, colleagues, disability insurers and society at large is of great concern for stakeholders involved in the disability claims management process7,18. Although evidence shows that prevention and early intervention help mitigate the risk and impact of long-term disability2,10, South Africa currently lacks a preventative and early intervention approach to disability.
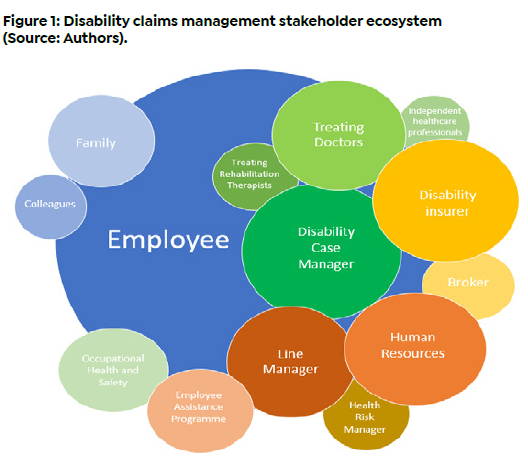
Considering the disability claims management stakeholders mentioned by the stakeholdersparticipants in this study, it is possible to schematically represent them in an ecosystem (Figure 1 below). Within this ecosystem: the size of the circle depicts the emphasis that stakeholders place on the role of the stakeholder; the proximity of the stakeholder's circle to other circles represents the level of engagement the connecting stakeholders have with each other; while the colours represent the group to which the stakeholder belongs (Blue: individual non-insurance stakeholders; Green: health professionals; Yellow: insurance stakeholders; Bronze: employer stakeholders). This ecosystem supports the key role players identified in the literature1-10.
The employee disability continuum
In this study, factors influencing prevention and early intervention of disability within the workplace were explored. Figure 2 (page ) depicts a continuum along which employee disability occurs and highlights that while employees are at work, intervention should promote good health and retain employees at work2,3,4,7,10. If an employee experiences ill-health, there should be early intervention to improve this ill-health. Of particular emphasis by stakeholders was that the employee should remain at work while the intervention occurs. Following prevention and early intervention is rehabilitation for acute and chronic illness. Rehabilitation lies towards the end of the continuum and is a well-established treatment modality for disability27.
A focus on psycho-social-economic factors
The majority of the stakeholders focused on how psycho-social-economic hardship experienced by South Africans is an inhibitor to prevention and early intervention14,15,28. For some South African's, the stakeholders pointed out, the chronicity of this hardship has a cumulative impact of deterioration on any physical or mental infirmities one may be experiencing leading to absenteeism and/or presentee-ism7,28. However, the stakeholders expressed that these hardships build resilience and motivation to remain productive at work for other South Africans. Enslin29 supports the view that resilience is a key characteristic determining once's ability to remain or return to work following ill-health. Although this is a keen insight, Enslin29 notes that an individual's resilience fluctuates over time and is influenced by several factors.
A number of the stakeholders mentioned the stressful work environment within South Africa since many companies must apply various austerity measures to remain operationally viable - this leads to job insecurity as the labour market contracts and the unemployment rate rises30. A further compounding factor reported by stakeholders was the negative impact the COVID-19 pandemic has had on many individual's mental health - this is supported by Harris31 who noted that COVID-19 intensified the rise of mental health claims. Forced isolation and fear of infection can have a profound social and psychological impact. The nature of these stress factors is likely to antagonise the disability claims management process.
Most of the stakeholders indicated a lack of understanding and collaboration regarding health and disability management. This leads to a fragmented management process wherein human resources and line managers are often the decision-makers of accommodations for employees who experience ill health; however, considering their lack of understanding, often these accommodations are inappropriate. This contributes to a relationship breakdown between an employee and an employer, which further decreases the likelihood of prevention and early intervention being successful32. This highlights the important role of human resources and line managers in prevention and early intervention stages33.
If anyone were to experience a medical condition that impacted their work performance, the findings revealed a paradox. Some South Africans appear hesitant to disclose their medical condition due to social disability stigma20 and/or the fear of losing their jobs9. In contrast, other South Africans see receiving a disability benefit as a way out of their challenging work environments since they still receive a secure income should they remain disabled34. For individuals within the latter group, stakeholders noted an increased likelihood of exaggerating symptoms as their income (disability income replacement benefit) is dependent on them remaining disabled35. Regardless of whether an individual is initially incentivised to remain in or to leave the work environment and receive a disability benefit, many stakeholders highlighted that once an individual leaves the work environment, they often experience deconditioning in their level of function and reduced motivation to improve their function and therefore their employability36.
Examples of preventative strategies suggested by stakeholders to mitigate these inhibiting factors include easy access to workplace support structures such as the EAP services for counselling on emotional, legal and/or financial issues19; a supportive line manager and team culture33; personal support structures such as positive family involvement; leveraging off medical aid routine health screenings followed by chronic disease management programmes where necessary18; and having an occupational therapist at the workplace to perform workplace assessments and provide supportive interventions and accommodations while the employee is still at work36,37. These preventative strategies highlight the need for a holistic understanding of the precipitating and perpetuating factors that contribute to employees' health. Enslin29 supports this holistic understanding and proposes that a bio-psycho-social model is valuable when seeking a holistic understanding of employee health.
If the employee's symptoms become too severe to continue working, and if the employer and employee stakeholders have disability income replacement insurance in place, the disability claim process is initiated. Stakeholders noted the following factors within the disability claims process that compound the already existing lack and/or delay of access to medical and rehabilitative treatment: a lack of proactive insurer involvement resulting in an inefficient claims process, a lack of innovation regarding the disability policy due to a highly competitive group insurance environment, a lack of communication between the stakeholders leading to misinterpretation of the process and policy, and a lack of insurer funding of medical management.
One can appreciate that a "one size fits all" approach is not sufficient to mitigate the factors that inhibit prevention and early intervention within the disability ecosystem. However, prevention and early intervention are among the most effective ways to manage the inhibiting factors and promote the employee remaining at work.
A focus on the RAW approach
The most common enabler mentioned by stakeholders was that of insurers partnering with third party occupational therapists who specialise in vocational rehabilitation to assist with supporting the medical and vocational co-ordination of the disability process. This partnership involves the insurer funding rehabilitation to improve the employee's vocational prognosis. Many stakeholders noted that most insurers only utilise the vocational occupational therapy services when the employee is no longer in the workplace. Although this is valuable, stakeholders believe that vocational occupational therapy services in isolation are not sufficient to improve an employee's vocational prognosis. This highlights the importance of situating medical and vocational management as part of the prevention and early intervention stages with the ultimate goal of keeping the employee within the work environment3.
For the RAW approach to be successful, many stakeholders emphasised that monitoring of absenteeism and presente-eism needs to be applied3,4,7 where employer stakeholders work together to investigate and support employees showing ill-health signs and symptoms.
As mentioned earlier, it is critical that employer stakeholders understand the relationship between poor employee performance because of a medical condition and how best to accommodate the impact this has on the employee and the business35. Examples of reasonable accommodations mentioned by stakeholders included decreased workload, approved time off to attend medical and rehabilitative treatment, and possible realignment into an alternate role during the period of recovery37.
Considering many RAW approach activities take place within the workplace, it's implied that the workplace stakeholders are largely responsible. However, literature and stakeholders' responses support insurers being incentivised to invest in the RAW approach as it decreases the likelihood of a disability claim2,10,18, which in turn reduces time and money spent on managing a disability income replacement claim2,10,18. For the RAW approach to be effective, stakeholders emphasised that the relationship between the insurer and the employer needs to be strengthened. A strengthened insurer-employer relationship would require the insurer to innovate the disability policy and process.
An additional benefit of a RAW approach is that employers and insurers will have greater confidence in the appropriateness of employees following a disability process, which will allow them to better manage resources between those who can remain at work while recovering from the medical condition and those who require a prolonged period off work to recover. Lastly, investing in a RAW approach reduces the risk of deconditioning once an employee is no longer in the work environment2.
CONCLUSION
The overarching theme within the study was that disability is a complex phenomenon influenced by various medical and non-medical factors. This complexity may contribute to a lack of prevention and early intervention in that stakeholders are uncertain which factor is most modifiable and impactful for them to allocate resources for development. This study has allowed for deeper insight into the inhibiting and facilitating factors within the disability claims management process. Inhibitors included: psycho-social-economic hardship, group insurer inhibitors, disability stigma and deconditioning, and poor health and disability understanding. Facilitators included: group insurer facilitators, RAW approach, medical and vocational management, and social and occupational support.
A RAW approach to ill-health emerged as a promising one for stakeholders interested in investing in a meaningful contribution to improving the experience and outcome of disability claims. A RAW approach utilises prevention to maintain employees' health and, when ill-health begins to occur, it utilises early intervention in a timely and appropriate manner. For this approach to be as impactful as possible, it was emphasised that all stakeholders need to see the value in a RAW approach and be committed to education and collaboration within prevention and early intervention stages.
AUTHOR CONTRIBUTIONS
Kerri-Lee Howell completed this study towards a Masters in occupational therapy degree and was responsible for the conceptualisation of the study, data collection, analysis and drafting of the original manuscript. Pragashnie Govender & Deshini Naidoo were supervisors of the study and guided the process from conceptualisation and design of the study to drafting and revision of the manuscript. All authors approved the manuscript for publication.
Conflicts of interest and bias declaration
The authors have no conflicts of interest to declare.
Data availability statement
Upon reasonable request, the data may be made available by the corresponding author.
REFERENCES
1. Bronfenbrenner, U. Toward an experimental ecology of human development. American Psychologist. 1977;32(7):513-531. doi: http://dx.doi.org/10.1037/0003-066x.32.7.513. [ Links ]
2. Chenier, L. Creating an effective workplace disability management program. [Internet]. Canada: The Conference Board of Canada; 2013 [updated 2013; cited 2021 November 12]. Available from: https://www.sunlife.ca/static/canada/Sponsor/About%20Group%20Benefits/Group %20benefits%20products%20and%20services/The%20Conversation/Disability/Creatin-gAnEffectiveWorkplace_SUNLIFE_EN.PDF [ Links ]
3. Baker-McClearn D, Greasley K, Dale K, Griffith F. Absence management and presenteeism: the pressures on employees to attend work and the impact of attendance on performance. Human Resource Management Journal. 2010;20(3):311-328 doi: http://dx.doi.org/10.1111/j.1748-8583.2009.00118.x [ Links ]
4. Munir F, Yarker J, Haslam C. Sickness absence management: encouraging attendance or 'risk-taking' presenteeism in employees with chronic illness? Disability and Rehabilitation. 2008;30(19):1461-1472. doi: http://dx.doi.org/1080/09638280701637380 [ Links ]
5. Bade S, Eckert J. Occupational Therapists' expertise in work rehabilitation and ergonomic. Work. 2008;31(1):101-111. [ Links ]
6. Zaparinuk L. Analysis of an Early Intervention Disability Program. [Internet]. Canada; 2013 April 14 [updated 2013; cited 2021 November 12]. Available from: https://core.ac.uk/download/pdf/84871663.pdf [ Links ]
7. Gosselin L. Presenteeism and absenteeism: Differentiated understanding of related phenomena. Journal of Occupational Health Psychology. 2013;18(1):75-86 doi: https://dx.doi.org/10.1037/a0030932 [ Links ]
8. Govender R. Govender P. Mpanza D. Medical incapacity Management in the South African Private Industrial Sector: The Role of the Occupational Therapist. South African Journal of Occupational Therapy, 49(3), 31-37. Available from: https://dx.doi.org/10.17159/2310-3833/2019/vol49n3a6 [ Links ]
9. Maja, P., Mann, W., Sing, S., Steyn, A., & Naidoo, P. Employing people with disabilities in South Africa. South African Journal of Occupational Therapy. 2011; 41(1):24-32. Available from: https://www.researchgate.net/publication/237188507_Employ-ing_people_with_disabilities_in_South_Africa [ Links ]
10. Shepell M. Integration EAP disability management programs fosters better disability outcomes. [Internet]. Canada; 2014 [updated 2014; cited 2021 November 12]. Available from:https://lifeworks.com/en/resource/integration-eap-disability-man-agement-programs-fosters-better-disability-outcomes-and [ Links ]
11. HartleyJ,Jacobson D, Klandermans B, et al. Job insecurity: Coping with jobs at risk. Sage publication. Journal of Organisational Behaviour. 1991;14(3):297-298. doi: https://doi.org/10.1002/job.4030140310 [ Links ]
12. Tetrick E. Quick J. Prevention at work: Public health in occupation settings. Handbook of occupational health psychology. doi: https://doi.org/10.1037/10474-000 [ Links ]
13. Statistics of South Africa. Statistics of South Africa on respondents losing jobs or businesses due to Coronavirus Covid-19 Lockdown. [Internet]. 2020 [updated 2020; cited 2020 November 12]. Available from: https://www.gov.za/speeches/respondents-lost-jobs-20-may-2020-0000 [ Links ]
14. South African College of Applied Psychology. The shocking state of mental health in South Africa in 2018. [Internet]. 2018 [updated 2018; cited 2021 November 12]. Available from: https://www.sacap.edu.za/blog/counselling/mental-health-south-africa/ [ Links ]
15. Freeman M, Simmonds J, Parry C. Where are we with non-communicable diseases health promotion in South Africa, where we should be, and how can we get to where we need to be? [Internet]. Cape Town: South African Medical Research Council. 2020 [updated 2020; cited 2021 Nov 12]. Available from: https://www.samrc.ac.za/sites/defaults/files/files/2020-06029/NoncommunicableDiseases.p [ Links ]
16. Ruff B. Board of Healthcare Funders. Board of Healthcare Funders: Latest News. [Internet]. Southern Africa; January 2018 [updated 2018; cited 12 November 2021). Available from: https://www.bhfglobal.com/2018/01/10/private-healthcare-in-sa-continued-decline-and-a-solution/ [ Links ]
17. South African Government. Employment Equity Act 55 of 1998. South Africa: Republic of South Africa; October 1998. Available from: http://www.Jabour.gov.za/DocumentCenter/Acts/Em-ployment%20Equity/Act%20-%20Employment%20Equity%201998.pdf [ Links ]
18. Martin G. Income protection and the economic Cycle. [Internet]. Australia: ClearView. ; 2019 [updated 2019; cited 2021 November 12]. Available from: https://www.clearview.com.au/documents/ebooks/Income-protevtion-white-paper [ Links ]
19. Goetzel R, Long S, Ozminkowski R, Hawkin K, Wang S, Lynch, W. Health, Absence, Disability, and Presenteeism Cost Estimates of Certain Physical and Mental Conditions Affecting U.S Employees. Journal of Occupational and Environmental Medicine. 2004;46(4):398-412. https://doi.org/10.1097/01.jom.0000121151.40413 [ Links ]
20. Govender R, Govender P, Naidoo D. Disability management in a public-private health care facility in South Africa: an organisational perspective. African Health Sciences. 2021;21(3): 1140-1450. doi: https://dx.doi.org/10.4313/abs.v21i3.5. September 2021 [ Links ]
21. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. International Journal of Quality in Health Care. 2007;19:349-357. https://doi.org/10.5014/ajot.2014.682006 [ Links ]
22. Jamshed S. Qualitative research method-interviewing and observation. Journal of Basic and Clinical Pharmacy. 2014;5(4):87-88. doi: https://doi.org/10.4103/097-0105.141942 [ Links ]
23. Harrell M, Bradley M. Data collection methods: semi-structured interviews and focus groups. RAND: National Defense Research Insitute. [Internet]. Santa Monica: RAND Corporation; 2009 [updated 2009; cited 2021 November 12]. Available from: https://www.rand.org/content/dam/rand/pubs/technical_re-ports/2009/RAND_TR718.pdf [ Links ]
24. QSR International. NVIVO 12 pro Qualitative Data Analysis Software [Software]. 1999. Available from: https://qsrinternational.com/nvivo/nvivo-products/ [ Links ]
25. Braun V, Clarke V. Using thematic analysis in psychology. Qualitative Research in Psychology. 2006; 3: 77-101. doi: https://doi.org/10.1191/1478088706qp063oa [ Links ]
26. Patton M. Qualitative Research & Evaluation Methods. London, United States of America: Sage Publications; 2002 [ Links ]
27. Russo D, Innes E. An Organisational case study of the case manager's role in a client's return-to-work programme in Australia. Occupational Therapy I nternational. 2005;9(1):57-75. doi: https://doi.org/10.1002.oti.156 [ Links ]
28. Pillay Y. State of mental health and illness in South Africa. South African Journal of Psychology. 2019; 49(9):463-466. doi: https://doi.org/10.1177/0081246319857527 [ Links ]
29. Enslin M. The role of resilience and self-efficacy in mental health claims management. Risk Matters. Gen Re, Cologne; July 2021 [updated 2021; cited 2021 November 12]. Available from https://www.genre.com/knowledge/publications/rm21-3-en.html July 2021 [ Links ]
30. The World Bank. The World Bank in South Africa. [Internet]. South Africa; 2019 [updated 2019; cited 2021 November 12]. Available from: https://www.worldbank.org/en/country/southafrica/overview [ Links ]
31. Harris N. COVID-19 and mental health claims: A guide for claims case managers. [Internet]. Reinsurance Group of America Australia; June 2020 [updated 2020; cited 2021 November 12]. Available from: https://www.rgare.com/knowledge-center/media/covid-19/covid-19-and-mental-health-claims-a-guide-for-claims-case-managers [ Links ]
32. Reinsurance Group of America. Global claims views: Return-to-work in the context of COVID-19. [Internet]. Australia; May 2020 [updated 2020; cited 2021 November 12]. Available from: https://www.rgare.com/docs/default-source/marketing/rtw-in-the-context-of-covid-19--a-guidance-note_global-claims-views_flnal.pdf [ Links ]
33. Haafkens JA, Kopnina H, Meerman MG, van Dijk FJ. Facilitating job retention for chronically ill employees: perspectives of line managers and human resource managers. BMC Health Services Research. Springer Science and Business Media LLC. 2011; 11(1). doi: http://dx.doi.org/10.1186/1472-6963-11-104 [ Links ]
34. Wells L, Barret P. Disability income: What can we learn from other markets? [Internet]. Reinsurance Group of America: South Africa; 2013 [updated 2013; cited 2021 November 12]. Available from: http://www.africanagenda.com/convention2013registration/ papersZ42-7f37a2a802344242b0059edb114ef263.pdf [ Links ]
35. Lenkoe M, Enslin M. Occupational Disability Claims Re-Imagined. [Internet]. GenRe: Cologne; 2017 [updated 2017; cited 2021 November 12]. Available from: https://www/genre.com/knowledge/publications/cflh17-2-lenkoe-enslin-en.html [ Links ]
36. American Association of Occupational Therapy. Occupational Therapy practice framework: Domain and process. American Journal of Occupatioanl Therapy. 2014;68(1):S1-S48. doi: https://doi.org/10.5014/ajot.2014.682006 [ Links ]
37. Main L, Haig J. Occupational Therapy and Vocational Rehabilitation: an audit of an outpatient Occupational Therapy service. British Journal of Occupational Therapy. 2006; 69(6): 288-292. [ Links ]
Submitted: 9 December 2021
Reviewed: 13 January 2022
Revised: 15 March 2022
Accepted: 27 March 2022
DATA AVAILABILITY: On request from corresponding author
FUNDING: None received
* Corresponding author: Deshini Naidoo: naidoodes@ukzn.ac.za


{kind=link}