










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.51 n.1 Pretoria Apr. 2021
http://dx.doi.org/10.17159/2310-3833/2021/vol51n1a3
ARTICLES
Promoting the development of foundation phase learners in under-resourced environments using Ayres Sensory Integration® principles and custom-designed, low-cost playgrounds
Annamarie van JaarsveldI, *; Erna LiebenbergII; Francois C. Van RooyenIII; Elize Janse van RensburgIV
IB.OT (UFS), M OT (UFS), PhD (UFS). https://orcid.org/000-0002-2357-0888; Lecturer, Department of Occupational Therapy, Faculty of Health Sciences, University of the Free State
IIB.Ed. Hon (Educational Psychology, UFS) M. Ed (Educational Psychology, UFS). https://orcid.org/0000-0002-5369-5569; Senior Education Specialist: Learner Support, Inclusive Education, Xhariep District
IIIM.Com (UFS). https://orcid.org/0000-0002-5092-2957 Biostatistician, Department of Biostatistics, University of the Free State
IVB.OT (UFS), M. OT (UFS). https://orcid.org/0000-0002-7232-0690; Occupational Therapist, Sensory Roots Occupational Therapy, Bloemfontein
ABSTRACT
INTRODUCTION: Children from under-resourced environments often lack opportunities to engage in sensory experiences that support developmental abilities and scholastic performance. "Back to Urth" playgrounds were designed to address the developmental needs of foundation phase learners in under-resourced communities. A 12-week sensory-motor programme, based on Ayres Sensory Integration® (ASI) principles, was developed, and educators were trained to present this programme on a "Back to Urth" playground at a rural school in the Free State. This study aimed to determine the effect of the programme on the development of Grade R and Grade 1 learners
METHOD: Learners from two comparable, no-fee schools were included in this experimental non-randomised pre-test-post-test control group design study. Learners from one school participated in the sensory-motor programme on the "Back to Urth" playground (n=40), and learners from the other school served as the control group (n=41). The effect of the programme was measured with the Bruininks-Oseretsky Test of Motor Proficiency 2nd Edition (Short Form), Revised Ayres-based Clinical Observations, and the Optima School Readiness Assessment
RESULTS: An improvement in scores for both groups, with the experimental group showing more significant improvement in their Revised Ayres-based Clinical Observations and Optima School Readiness Assessment total scores were indicated
CONCLUSION: This study provides evidence that sensory-motor components underlying learning can be improved when learners are exposed to a sensory-motor programme designed within the framework of ASI, presented by educators on a low cost "Back to Urth" playground
Keywords: Sensory-motor development, low-cost sustainable playground, sensory integration, educators
INTRODUCTION
Recent research on brain development casts new light on the formative influence of early childhood experience. In the first few years of life, a child's brain creates 700 to 1,000 new neural connections every second, a pace that later diminishes. These early connections set the foundation on which later connections are built1:50.
Involvement of the authors (including two occupational therapists and an educationalist) in rural communities in the Xhariep district, Free State, South Africa, led to the awareness of the developmental needs of children in the foundation phase of education. At the same time, there was also an outcry from educators for support with developmental stimulation programmes for children from under-resourced communities who were attending rural schools.
One of the efforts to address these needs was designing and constructing sustainable, low-cost "Back to Urth" playgrounds. The concept of the "Back to Urth" Playgrounds was developed by one of the researchers based on research done at the University of the Free State (UFS)2. This research indicated that children from under-resourced environments in South Africa experience developmental delays and consequent functional problems, which impact on their performance in school and other occupations2. These problems result in barriers to learning which can seldom be fully remediated.
"Back to Urth" playgrounds are designed to provide sensory-rich experiences, with an emphasis on the tactile-, vestibular- and proprioceptive systems that support sensory integration and thus function. The uniqueness of these playgrounds is that each part of the playground is designed using principles based on Ayres Sensory Integration® (ASI), as well as results from research done at the Occupational Therapy Department, UFS3. This research indicated that pre-school children from under-resourced communities were at higher risk of experiencing sensory integration problems. The most prevalent sensory integration problems identified were postural control and bilateral integration difficulties. The integration of primitive postural reflexes was also of concern. The design of the playgrounds is therefore done to ensure that definite balanced sensory experiences are provided, which support specific developmental components needed for successful scholastic performance, such as postural control and bilateral integration.
The main aim of the playgrounds is to provide children from under-resourced communities with access to play equipment, which offers balanced sensory-rich experiences that support development4. Key sections of the playgrounds are constructed with a low-cost, cob building method, making it a sustainable solution for communities lacking resources and infrastructure. The building of the playgrounds was initially done in collaboration with the Department of Development Studies, UFS and Qala Phelang Tala (QPT), a non-profit company working towards sustainable human settlements5. Venter5 introduced this sustainable building method to one of the researchers in 2014 who then recognised it as a constructing possibility for "Back to Urth" playgrounds. The building process works on the principle of community participation and collaboration between different stakeholders, where skill transfer is prioritised, and the relevant community's/school's involvement is a priority. This whole initiative forms part of a collaborative training platform of the Faculty of Health Sciences, UFS. Students, community members, existing private, public and third sector organisations/structures and volunteers come together to create pathways, partnerships and initiatives that enable skill development and service delivery to marginalised communities.
Each playground is uniquely designed depending on the space available, needs of the school/community, materials obtainable, human resources and finances available. After completion of a playground at a school, the educators receive training on the optimal use of the playgrounds.
Considering the given information, the question that arose was whether opportunities for exposure to a sensory-motor programme, based on ASI principles, presented on a "Back to Urth" playground by educators, would enhance the development of skills and functions needed for the learning process required in a mainstream school.
LITERATURE REVIEW
Some of the latest research1, on brain development in children indicates that 700 to 1,000 new neural connections per second are formed in a child's brain. This emphasises the importance of "the formative influence of early childhood experience"1, especially considering the fact that the pace of brain development slows down with age. This also confirms what Jean Ayres hypothesised 6:1-2: "...early (brain) connections set the foundation on which later connections are built". According to UNICEF1 "early childhood care, protection and stimulation can jumpstart brain development, strengthen children's ability to learn, help them develop psychological resilience and allow them to adapt to change"6,p1-2.
Statistics on learners' performance in primary education in South Africa confirm that educators' concerns and need for help are justified. A report on the annual national assessment of 2014 indicated that Grade 3 learners in South Africa obtained an average of only 56% for both literacy and numeracy7.
Looking at school assessment criteria (National Curriculum and Assessment Policy Statement (CAPS)), defined standards which learners need to achieve by the end of their Grade R year. It is expected that a Grade 1 learner should be physically, cognitively, affectively, normatively, socio-culturally and linguistically prepared for functioning on a certain standard when starting his/her school career8. In the September 2016 monthly report of the Xhariep District Based Support Team (DSBT) it was indicated that of the 39 referrals received from the foundation phase of one school in this district, 32 were from learners who by far did not meet the basic standards for their grades due to suspected developmental delays9.
The reality is that children who are raised in poverty or under-resourced environments often lack the opportunity for environmental stimulation and exploration and social interaction, which collectively impacts their development. These children's functional difficulties include poor use of their body in three-dimensional space, which can be seen in their poor gross- and fine motor performance2. These children fail to develop the abilities that support their writing- and reading skills, often resulting in poor school performance and school failure. A lack of successful school achievement feeds into the perpetuating cycle of poverty by limiting opportunities for gainful employment.
Basic performance components such as postural control, bilateral coordination, fine and gross motor coordination, praxis and visual perception are critical abilities a child requires for learning to read and write. These components depend heavily on sensory integration which, in turn, contributes to a child's capacity to learn and function6. Sensory integration is a framework constructed by Dr Jean Ayres and is based on her work on patterns of perceptual-motor dysfunctions. According to Ayres6, sensory integration can be defined as a neurological process that organises sensations from one's body and the environment and makes it possible to effectively use the body in the environment. Ayres strongly felt that "behaviour is linked to neurological processes, and that brainstem-level sensory processing enables higher neural centres to develop and specialise"62, thus influencing the development and successful participation in daily activities.
Many sensory-motor stimulation programmes exist and could have been considered for use in this context. However, the first author, who is trained in ASI and has many years of experience in the field, knew the importance and contribution of sensory integration in child development. The first author therefore decided to design unique sensory-motor programmes within the framework of ASI, that could be implemented in under-resourced communities where the Occupational Therapy Department of the UFS is involved. The first author used the 'The Wall Model Adapted Version'10 to guide the design of the programme within the framework of ASI. The Wall Model Adapted Version is designed according to Ayres' theory that "a child's development unfolds in a sequence and is influenced by the experiences a person has during development"11:7. The Wall Model Adapted Version includes the important sensory-motor components that subserve function and that are dependent on the integration of sensory information. Sensory-motor components included in this adapted version are muscle tone, motor control, integration of primitive postural reflexes, balance, postural control and stability, dissociation of movements, eye movements, fine motor components, bilateral coordination, laterality, crossing of midline, lateralisation and dominance, eye-hand coordination, sequencing, visual-motor integration, and praxis. The developmental components are theoretically arranged and indicate an approximated developmental trajectory accounting for each component's dependence on the other10. This model was designed for use in intervention planning. It supports the fact that a child's development is dependent on participation in activities of daily life inclusive of exposure to sensory-motor activities impacting on movement skills, cognitive, emotional and social development12. This model allows for clinical reasoning during intervention planning and grading and, as such, was an essential guiding model in the design of activities to implement on the different equipment pieces of a "Back to Urth" playground, ensuring that all the relevant sensory-motor components are addressed.
Sensory integration is regarded as a specialist field within the profession of occupational therapy. However, the authors argue that due to realities within the South African context, the majority of children growing up in under-resourced environments will very rarely be exposed to specialist occupational therapy services. Evidence exists that individual ASI intervention does impact positively on the development of South African toddlers from a low socio-economic setting who were born prematurely13. It is, however, not known what the impact will be when a programme based on ASI principles is presented by educators to a group of learners. A real-world problem of developmental challenges due to poor sensory integration in learners growing up in under resourced environments needed investigation. Building low-cost playgrounds, allowing for sensory-rich experiences, together with the development of balanced sensory enriched programmes to be implemented by educators, could result in addressing this problem.
AIM
The study aimed to determine the effect of a 12-week sensory-motor programme designed within the framework of ASI, presented by educators on a low cost "Back to Urth" playground, on the development of Grade R and Grade 1 learners attending a rural, mainstream school in the Free State.
METHODOLOGY
The study employed a quasi-experimental14 (non-randomised) pretest-post-test control group design15. A pilot study was conducted to ensure the feasibility of the use of the identified measuring instruments to test and refine the measurement procedures. Five learners were involved in the pilot study. Due to logistical and financial reasons, the learners involved in the pilot study were from another town and results were therefore not included in this study.
Participants
Two comparable schools were included in the study - one school served as the experimental school and the other as the control school. The schools are situated 10 km apart in two adjacent rural towns in the Free State. Both schools are classified as no-fee schools and had feeding schemes in place for learners, had a similar number of learners and educator-learner ratio, and both used Afrikaans as their language of teaching and learning. The demographic profile of the learners in both schools was similar in terms of gender, race, socio-economic background, and home language. A "Back to Urth" playground had been built at the experimental school in the year before the research. The playground was enclosed with a fence and learners of the school did not have access to the playground until the study commenced. The control school did not have access to a "Back to Urth" playground although the school did have some playground equipment to which the learners did have infrequent access during break times. The playground was not in the area of the classrooms. Considering the above information, the authors were of the opinion that the developmental experiences that the children were exposed to were fairly similar and comparable.
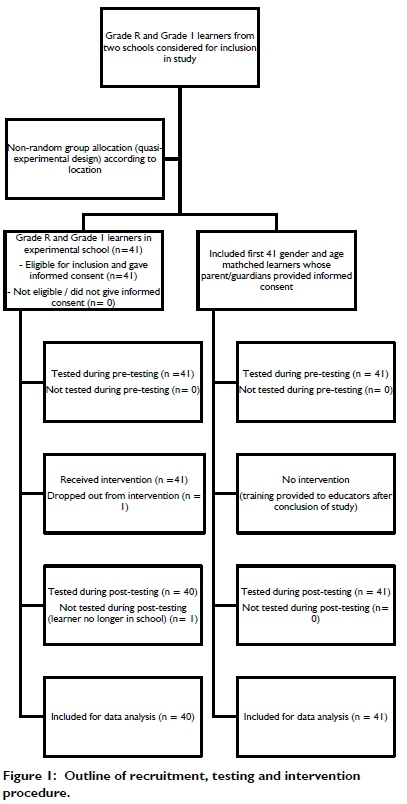
Learners of the schools were included in the study, in either the experimental or the control group, if they were enrolled in Grade R or Grade 1 for the first time in the year of the study. Their parents or legal guardians provided informed consent and the learner gave assent in an age-appropriate manner to participate in the research. Learners with diagnosed mental or physical disabilities and learners who were ill or absent from school at the time of the execution of the assessments were excluded from the study. All learners of the experimental school whose parents/legal guardians provided informed consent were included in the study. An exclusion criterion was set for learners who had not participated in at least 80% of the intervention sessions. At the control school, the same inclusion criteria were applied as for the experimental school, and testers continued testing until a number of participants similar to the experimental school in terms of age, gender and grade, was reached. Figure 1 (below) provides an outline of recruitment, testing and intervention process.
Measuring instruments
Learners from both the experimental and the control groups were assessed at the respective schools before the implementation of the sensory-motor programme, and again after the 12-week intervention period. Two measuring instruments assessing sensory-motor performance (the Bruininks-Oseretsky Test of Motor Proficiency 2nd Edition, Short Form (BOT-2 SF)16 and the Revised Ayres-based Clinical Observations17) and one assessing school performance (the Optima School Readiness Assessment1) were used.
The BOT-2 SF assesses motor proficiency and consists of 14 items drawn from the eight subtests of the complete Bruiniks-Oseretsky Test of Motor Proficiency 2nd Edition (BOT-2)16 representing a broad range of motor abilities. The BOT-2 SF provides a single, sufficiently reliable score of overall motor proficiency. Raw scores achieved by a learner on the 14 items are converted to point scores and then to a norm-referenced composite standard score. Since this norm-referenced test was standardised in North-America, standard scores achieved would not necessarily reflect the abilities of South African children in comparison to their peers, but rather to a contextually diverse normative sample. However, despite this limitation, the test did allow for reliable comparison of pre- and post-test scores of the experimental and control groups to one another. The BOT-2 SF has demonstrated good test-retest reliability (r=0.86 for ages 4-7) and excellent inter-rater reliability (r=0.98 for ages 4-7)16. The reliability of the BOT-2 SF was also investigated in rural communities in Australia, demonstrating acceptable reliability for use in rural communities19.
Twelve sets of the Revised Ayres-based Clinical Observations that have been part of Ayres' original work in sensory integration20 were included in this study. These clinical observations have assisted occupational therapists over many years to distinguish typical sensory-motor developmental patterns from immature/delayed developmental patterns. The items included in the Revised Ayres-based Clinical Observations for this study were: asymmetrical tonic neck reflex, symmetrical tonic neck reflex, eye movements, forearm rotations, thumb-finger touching, finger to nose test, supine flexion posture, prone extension posture, equilibrium reactions, gaze stability, arm extension and trunk rotation, and midline crossing. Some observations contained more than one item (such as testing the left hand and right hand separately, and then bilaterally on the forearm rotation observation), resulting in a total of 30 sub-items that were rated for each learner. A five-point rating scale was used to rate each learner's performance according to the following classification:
1. totally unable to perform the action
2. attempts but only achieves partially
3. able to perform, poor control / not well integrated
4. good performance, slight inconsistencies and lacks some integration
5. executes with ease, good control / well integrated
The Optima School Readiness Assessment was developed by Le Roux18 to assist educators of foundation phase learners to obtain a "differentiated view of the level of school readiness of learners in [their] class"18:1. The Optima School Readiness Assessment, developed specifically for the South African context, is widely used by educators in the Xhariep District, including the Inclusive Education unit where one of the authors is employed. The results of this test can be used diagnostically by the educator to ascertain a learner's level of learning readiness and to assist those learners who experience learning challenges. The test consists of five sub-tests assessing the following functions: visual perception, spatial/number concept, auditory perception, socio-emotional development and fine/gross motor development. Most of the test items can be administered in small groups.
Measurement procedures
Parental informed consent forms were distributed by school staff, on behalf of the researchers, and returned to relevant educators. The same procedure was followed for the pre-test and the post-test at both the experimental and the control schools. The sensory-motor tests (BOT-2 SF and Revised Ayres-based Clinical Observations) were administered by two qualified occupational therapists who had received additional research-specific training by the authors. One occupational therapist administered the BOT-2 SF to all the learners, and the other occupational therapist administered the Revised Ayres-based Clinical Observations. Due to unforeseen circumstances, the occupational therapist who administered the BOT-2 SF was not available for the post-testing and another occupational therapist (who had received the same research-specific training) was recruited to administer the BOT-2 SF during post-testing. Inter-rater reliability for the BOT-2 SF is reported at .98 indicating very consistent inter-rater reliability.16 The Optima School Readiness Assessment was conducted by an educational specialist trained in the use of the Optima School Readiness Assessment. To limit rater bias, pre-intervention assessment results were not available to the test administrators when they did the post-tests. Additionally, pre- and post-tests were done at least 12 weeks apart making it difficult to remember the performance of a learner and limiting rater bias in the case of the Revised Ayres-based Clinical Observations. The nature of the study did not allow for blind testing of children of the experimental and control groups, as the location of their school determined group allocation. This was an inherent limitation of the study, linked to the quasi-experimental design, and this limitation must be taken into account when reporting on and interpreting the results of this study.
Testing of learners was done during school hours. Prior arrangements with the schools ensured that participation in the study did not result in any loss of learning opportunities for learners in the classroom. Learners were tested in a pre-arranged, suitable venue at their relevant schools. The relevant test administrator collected learners and established a rapport before they were individually tested. For the Optima School Readiness assessment, test items were presented in small groups except for the auditory memory and gross motor which were presented to learners individually.
Description of intervention
The experimental group participated in the sensory-motor programme that was presented by educators on the "Back to Urth" playground situated at the school. The intervention programme was compiled by the first author who was responsible for the design and development of the "Back to Urth" playground. The educators of the Grade R and Grade 1 classes attended a training workshop on the presentation of the programme. The actual activities were additionally provided in an instruction manual format to the educators. A third educator was also included in the training to allow for substitution in the case of absence of one of the two other educators. The researcher responsible for the design of the playground and intervention programme was available for support/ consultation throughout the intervention period.
The intervention programme consisted of sensory-motor activities designed using ASI principles and specifically for use on a "Back to Urth" playground. The pre-test results were also considered in the design of the intervention programme. The playground at the experimental school consisted of ten different constructed equipment "stations", each addressing different sensory-motor components included in the Wall Model Adapted Version. The "Tyre bridge", for example, was provided to provide especially vestibular and tactile input whilst an activity for example required balance reactions and postural control. The "Shongololo" on the other hand provided tactile, proprioceptive and vestibular input whilst an activity carried out on the "Shongololo" required (amongst others) bilateral coordination, midline crossing and sequencing. Other activities included crawling up- and rolling down a "mountain", balancing on a 4x4 see-saw, and swinging on swings in different positions and directions. The programme was graded twice during the intervention period. Grading allowed for variation in sensory experiences and required different and more advanced developmental abilities, and was guided by the Wall Model Adapted Version10, as learners progressed through the programme. Using the Wall Model Adapted Version to guide the grading ensured that a bottom-up approach in terms of development was adhered to. In the first set of activities, the focus was on developmental components such as balance, postural control, body scheme and dissociation of movements. In the second set of activities the focus was on the development of bilateral coordination, crossing of midline and lateralization. In the last set of activities, focus was placed on eye-hand coordination, sequencing, and praxis.
Learners of the Grade R and Grade 1 classes at the experimental school participated in the intervention programme for one or two sessions a week for twelve weeks, depending on the school programme. The duration of each session was more or less 40 minutes. The educators provided the children with instructions on what to do on the different pieces of equipment and determined the time spent on each piece of equipment. This was done to ensure that all the children played on all the different equipment according to the programme, during each session. The two educators divided their classes into groups, each with a leader. Each group was placed at an equipment "station" and they participated in the activity at a specific equipment station, according to the programme, for more or less ten minutes after which they rotated to the next "station". Although the performance of the learners was not recorded per session, the educators reported that they could see how the leaners' participation in the activities improved. An attendance record was kept to ensure that all learners in the study participated in at least 80% of the intervention programme sessions.
Learners at the control school continued with their normal educational programme at their school for the duration of the 12 weeks following pre-testing. After completion of the intervention, programme post-testing was done in the same manner as the pre-testing.
Data management and analysis
Demographic information and all the pre-test and post-test results were captured electronically on an Excel Spreadsheet by the test administrators. This was verified by one of the researchers who checked the transfer of data systematically for potential transfer errors. Continuous variables were summarised by medians, minimum, maximum or percentiles. Categorical variables were summarised by frequencies and percentages. Within-group changes were evaluated using the Singed Rank for paired data. Differences between groups were evaluated using the Wilcoxon Two-Sample test for unpaired data. The analysis was done by the Department of Biostatistics at the UFS, using Statistical Analyses Software (SAS 9.4).
Ethical considerations
The study was approved by the Health Sciences Research Ethics Committee (HSREC), University of the Free State (HSREC 167/2016) and permission for the study to be conducted at public schools was obtained from the Free State Department of Education, as well as the respective school principals. Participation in the study was voluntary. Learners' parents/guardians provided written informed consent, and learners gave assent. There was no remuneration for participation in the study. Information collected during the study was dealt with confidentially and participants' identities were protected by using participant numbers and storing documents with personal information such as consent forms separate from research data.
The educators of both schools received general feedback on the performance of the children, as a group, after the study was completed. In cases where a learner's test results were indicative of serious developmental- or functional skill problems that could result in poor school performance, more specific and detailed feedback was provided to the educators, as was agreed to in the parental consent form. Recommendations regarding possible support for these learners in the classroom were provided and arrangements with different stakeholders e.g., the Department of Health, were initiated.
The school acting as the control school was provided with a workshop for the foundation phase educators once the post-testing had been completed. The workshop aimed to provide them with knowledge on sensory-motor development of Grade R and Grade 1 learners. They did not have access to a "Back to Urth" playground like the one at the experimental school, thus an adapted programme was presented, with limitations due to the absence of a playground. This action was taken for the learners at the control school to also benefit from participation in sensory-rich motor activities.
RESULTS
Table I depicts the final number of participants in each grade and gender group for both the experimental and control schools. For the two sensory-motor tests, the results of 40 learners from the experimental school and 41 for the control school were included and calculated. All the learners of the experimental school attended more than 80% of the sessions. One of the learners of the experimental school relocated during the research period and had to be excluded.
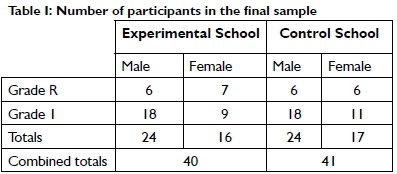
The distribution of Grade R learners to Grade 1 learners, as well as the distribution of male to female learners, were similar for both groups. The samples in both schools included more Grade 1 learners than Grade R learners, and more male than female learners. The ages at pre-testing at the experimental school varied between 4 years 10 months and 6 years 7 months for grade R and between 6 years 1 month and 8 years 9 months for Grade 1. At the control school, the pre-testing ages for Grade R varied between 5 years 3 months and 6 years 1 month whilst the Grade 1's ages varied between 6 years 0 months and 8 years 1 month.
Bruininks-Oseretsky Test of Motor Proficiency 2nd Edition Short Form
When administering the BOT-2 SF, a total point score is obtained, and a standard score is calculated by comparing the child's total point score to normative data of the test for children of the same age. The BOT-2 SF standard score has a mean of 50 and a standard deviation of 10. The median score obtained by the experimental and control groups on pre- and post-testing with the BOT-2 SF are reported in Table II.
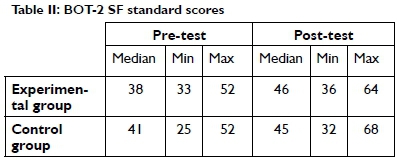
The difference between the experimental and control groups on pre-testing was not significant (p=0.81), demonstrating similarity and thus comparability of the two groups before the intervention commenced. Following intervention, both the experimental group and the control group showed an improvement in their median standard score from pre-testing to post-testing.
Comparison of the difference in median standard score from pre- to post testing showed an improvement of 8 points for the experimental group and only 4 points for the control group. However, the difference between the scores of the two groups was not significant (p=0.59).
Revised Ayres' Clinical Observations
Twelve observations, consisting of a total of 30 sub-items, were scored for each learner using the described five-point rating scale. Each learner could obtain a total rating score between 30 and l50. The median, minimum and maximum total rating score for the experimental and control groups on pre- and post-testing are depicted in Table III.
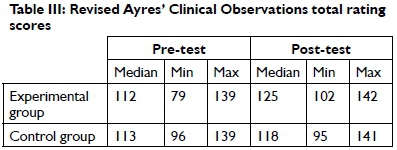
The median total rating score for the experimental and control groups was similar and thus comparable before the intervention. The experimental group's median total rating scale improved from 112 to 125 post-intervention, while the control group improved slightly from 113 to 118.
To ascertain whether the improvement in the experimental group was significantly greater than that of the control group, the difference between the total rating score for each learner on pre- and post-testing was calculated by subtracting the pre-test score from the post-test score. A positive value would thus indicate improvement, and a negative value would indicate a decline in performance. The difference for the experimental and control groups was then compared, and a 95% confidence interval was calculated to determine the significance of the difference. The results are depicted in Table IV (above).
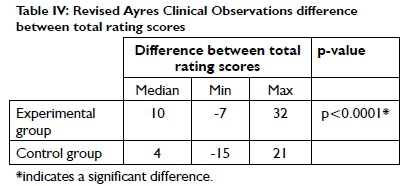
Both groups showed improvement in the median difference between the pre-test and post-test total rating scores. The improvement in the experimental group was, however, significantly more than that of the control group (p<0.0001).
Optima School Readiness Test
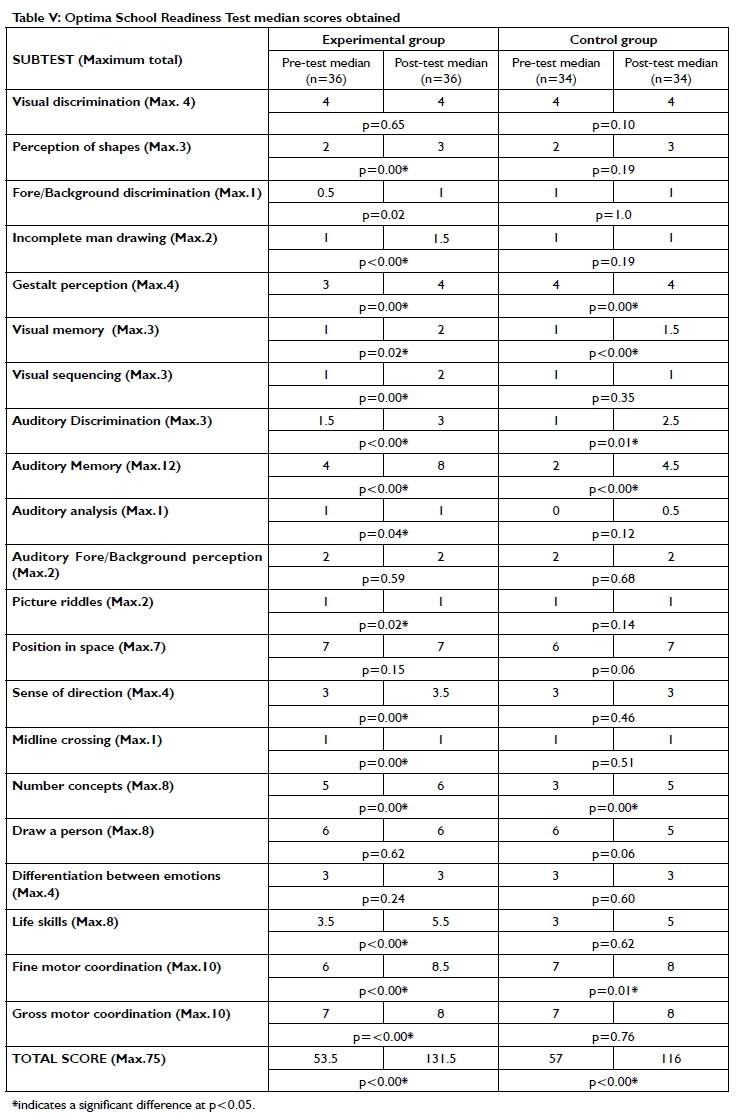
The Optima School Readiness Test was conducted on different days from the motor tests (BOT-2 SF and Revised Ayres' Clinical Observations). As a result, some learners were not included in the results for the Optima School Readiness Test due to absenteeism. There were complete test results for 36 learners in the experimental group and 34 learners in the control group. Table V (p15) depicts the median scores obtained by the experimental and the control groups on pre- and post-testing respectively, for each subtest of the Optima School Readiness Test. The p-value, calculated by means of the signed-rank test for paired non-parametric data, for the difference between the median pre- and post-test scores for each group is also indicated.
Results indicate that the experimental group obtained significantly better results on l5 of the 2l subtests, as well as on the total score after the intervention. Although the control group also obtained significantly better results on the total score on post-testing, their subtests scores only showed significant improvement in six of the 21 subtests. Both groups performed better in these six tests on post-testing, namely Gestalt perception, visual memory, discrimination, memory, number concepts and fine motor skills. Subtests in which the experimental group improved significantly, but not the control group, were perception of shapes, incomplete man, visual sequencing, auditory analysis, picture riddles, sense of direction, midline crossing, life skills and gross motor skills.
The difference between the pre- and post-test scores for the two groups on the Optima School Readiness Test was calculated to evaluate whether the experimental group showed significantly more improvement in their pre- and post- difference of the total test score. The p-value [p<0.00], indicated that the experimental group showed a significantly greater improvement in performance than the control group.
DISCUSSION
The study aimed to investigate the effect of a sensory-motor programme, designed within the framework of ASI, presented by educators on a sustainable, low-cost playground, on the development and performance of foundation phase learners. The post-test results of the BOT2-SF did not indicate a significant difference in the sub-test scores or the total test scores for both groups. Clinically, the experimental group did appear to improve more than the control group. However, this change was not large enough to demonstrate significance as was the case in the other assessment instruments used.
The Revised Ayres' Clinical Observations' results showed an improvement for both groups. Although both groups showed improvement in the median difference between the pre-test and post-test total rating scores, the difference for the experimental group was significantly more than for the control group, providing evidence of the effect of the intervention. It is noteworthy to report that in the breakdown of scores, items related to functions supported by the vestibular system and specifically balance, showed the most significant improvements. The vestibular system is stimulated by moving through three-dimensional space in different planes and the equipment of a "Back to Urth" playground is designed to allow for activities that require moving through the different planes.
The results of the Revised Ayres' Clinical Observations are promising and in support of the positive effect that a sensory-motor stimulation programme, designed within the framework of ASI, and presented by educators on a sustainable, low-cost playground, can have on the sensory-motor development of foundation phase learners attending rural schools.
Results of the Optima School Readiness Test showed an improvement for both groups on six tests during post-testing. The test items for Gestalt perception, visual memory, discrimination, memory, number concepts and fine motor skills are all targeted abilities that receive attention in the classroom and could, therefore, explain why both groups performed better. The test items for sense of direction, midline crossing, and gross motor skills, where the experimental school performed significantly better can directly be attributed to the intervention as it were abilities that were addressed in the programme. Perception of shapes, incomplete man, visual sequencing, auditory analysis, picture riddles, and life skills are amongst the test items commonly linked to higher cognitive functions. Ayres already hypothesised in the 1960s that higher cognitive functions are dependent on lower brain function and then specifically sensory integration6 with mounting evidence, supporting this hypothesis12. Results of this study support evidence for improved sensory integration in learners of the experimental group which could have contributed to improved performance on these test items.
LIMITATIONS
The study had a limited number of participants and results of bigger samples of learners are needed. This study only investigated the short-term impact of an intervention (over three months). Blinding of fieldworkers conducting the pre- and post-assessments were not possible, as the experimental and control groups were from two different schools.
CONCLUSION AND RECOMMENDATIONS
Sensory integration theory allows for the explanation of function, assessment and the planning of intervention. In this study, knowledge from an ASI framework was used to develop sensory-rich activities that support the development of specific sensory-motor components. These activities were designed to be presented by educators, to learners, on a specifically designed playground. The authors predicted that function could change due to the intervention, knowing that exposure to purposeful, enriched foundational body-centred sensory activities can impact on learning and de-velopmentl2,2l. This study provides evidence that sensory-motor components underlying learning can be improved when learners are exposed to a sensory-motor programme designed within the framework of ASI, presented by educators on a low cost "Back to Urth" playground. Learning barriers can, therefore, potentially be prevented with consistent exposure to the playground.
This study contributed to the knowledge and practice field of sensory integration in occupational therapy. It contributed to the real-world challenge of a scarcity of occupational therapy services in under-resourced communities in South Africa where the majority of children are growing up. Building low-cost playgrounds, allowing for sensory enriched experiences, together with the knowledge and skill transfer to educators to implement programmes, such as the one used in this study, can assist in addressing the developmental challenges experienced, due to poor sensory integration, and have a positive impact on school performance.
A longitudinal study on the long-term impact of such a programme on a Back to Urth playground is needed as this study was done under controlled conditions and research is needed on what the impact will be if a programme is presented within the normal realities of a school programme and over a prolonged time.
Research investigating the difference between a programme as implemented in this study versus individual ASI intervention is also recommended.
A final recommendation is for the necessary advocacy by occupational therapists working in the field of paediatrics to ensure that all schools in South Africa have access to playgrounds and resources that can promote the development of foundational skills for learning in early childhood.
ACKNOWLEDGEMENTS
The research was made possible through funding received from the Research Development Directorate at Research Development Directorate at the University of the Free State. The principals of the two schools are acknowledged for their willingness to participate in the research as well as parents and especially the learners. Fieldworkers who were responsible for the collection of data are acknowledged for their important contribution towards the collecting of the data. The two foundation phase educators who were involved in the implementation of the intervention programme need special mention as without their willingness and commitment to execute the intervention programme the research would not have been possible. The researchers also want to acknowledge the South African Institute for Sensory Integration's financial contribution towards the maintenance that was needed on some of the equipment after the conclusion of the research.
ROLE OF AUTHORS
Annamarie van Jaarsveld was lead researcher in the conception and design of the study, involved in the planning and design of the intervention part of the study and contributed to the interpretation of data. The author also took the lead in the writing of the article and the revision thereof and therefor approve of the version that is submitted as well as any revised version following the review process. E. Liebenberg contributed to the conception and design of the study, the acquisition of data and the interpretation thereof. She also participated in the drafting and revising of the article prior to submission. She gave final approval of the version that is submitted as well as any revised version following the review process. F.C. van Rooyen contributed to the conception and design of the study, data analysis and the interpretation thereof. He also participated in the drafting and revising of the article prior to submission. He gave final approval of the version that is submitted as well as any revised version following the review process. E. Janse van Rensburg contributed to the design of the study, data analysis and the interpretation thereof. She also participated in the drafting and revising of the article prior to submission. She gave final approval of the version that is submitted as well as any revised version following the review process.
REFERENCES
1. UNICEF "UNICEF The State of the World's Children 2016," June 2016. [Online]. <http://www.unicef.org/> [Accessed 22 July 2016]. [ Links ]
2. Van Jaarsveld A. Sensory Integration and Socio-Economic Environments. SAISI Newsletter, 2010; 20(2): 8-13. [ Links ]
3. Van Jaarsveld A, Venter A, Joubert G, Van Vuuren S. The effect of a sensory integration-orientated stimulation programme on three-to five-year-old pre-school children in semi-structured pre-school programmes in Mangaung, Bloemfontein. South African Journal of Occupational Therapy, 2001; 31(3): 9-13. [ Links ]
4. Van Jaarsveld A. "The realities of SI assessment and intervention in third world settings". Keynote address, European Sensory Integration Congress, Birmingham, 2015. [ Links ]
5. Venter A. "Start Living Green, Qala Phelang Tala," 15 June 2012. [Online]. <http://www.startlivinggreen.co.za/Home/> [Accessed 17 March 2015]. [ Links ]
6. Schaaf RC, Smith Roley S. Sensory Integration: Applying Clinical Reasoning to Practice with Diverse Populations, Austin, Texas: Pro-ed, 2006. [ Links ]
7. Department of Basic Education. "Report on the Annual National Assessments of 2014." Pretoria: Republic of South Africa, 2014. <http://www.saqa.org.za/docs/rep_annual/20l4/REPORT%20ON%20THE%20ANA%20OF%202014.pdf> [Accessed 11 February 2020]. [ Links ]
8. Department: Basic Education, "Curriculum and Assessment Policy Statement For Foundation Phase," Pretoria: Republic of South Africa, 2011. <https://www.education.gov.za/Curriculum/CurriculumAssessmentPolicyStatements(CAPS)/CAPSFoundation.aspx> [Accessed 11 February 2020]. [ Links ]
9. Liebenberg HS. "Monthly Report," Bloemfontein: Free State Department of Education, 21 September 2016. [ Links ]
10. Van Jaarsveld A, Janse van Rensburg E. The Wall Model Adapted Version, Bloemfontein: Department of Occupational Therapy, University of the Free State, 2020. [ Links ]
11. Schaaf RC, Mailloux Z. Clinician's guide for Implementing Ayres Sensory Integration: Promoting Participation for Children with Autism, Bethesda, USA: AOTA Press, 2015. https://doi.org/10.7139/2017.978-1-56900-433-3 [ Links ]
12. Lane SJ, Mailloux Z, Schoen S, Bundy A, May-Benson TA, Parham DL, Smith Roley S, Schaaf RC. "Neural Foundations of Ayres Sensory Integration®," Brain Sciences, 2019; 9: 153. https://doi.org/10.3390/brainsci9070153 [ Links ]
13. Lecuona E, Van Jaarsveld A, Raubenheimer J, Van Heerden R, "Sensory integration intervention and the development of the premature infant: A controlled trial," South African Medical Journal, 2017; 107(11): 976-982. https://doi.org/10.7196/samj.2017.v107i11.12393) [ Links ]
14. Creswell, JW. Research Design: Qualitative, Quantitative and Mixed Methods Approaches, 3rd Edition, California: Sage Publications Inc., 2009. [ Links ]
15. Fouché, CB, Delport, CSL, De Vos, AS. "Quantitative Research Designs". In: AS de Vos, H Strydom, CB Fouché, CSL Delport (Eds.). Research at Grass Roots: For the Social Sciences and Human Service Professions, 4th Edition, Pretoria: Van Schaik Publishers, 2011. [ Links ]
16. Bruininks R, Bruininks B. Bruininks-Oseretsky Test of Motor Proficiency, Second Edition, Minneapolis: NCS Pearson, 2005. [ Links ]
17. SAISI, Revised Clinical Observations based on Ayres, South African Institute for Sensory Integration (SAISI), 2015. [ Links ]
18. Le Roux SS. "Optima School Readiness Assessment", Optima School Readiness Assessment Manual and Correction Key, 2010. [ Links ]
19. Lucas BR, Latimer J, Doney R, Ferreira ML, Adams R, Hawkes G, Fitzpatrick JP Hand M, Oscar J, Carter M, Elliott EJ. "The Bruininks-Oseretsky Test of Motor Proficiency - Short Form is reliable in children living in remote Australian aboriginal communities," BMC Pediatrics, 2013; 13(135). https://doi.org/10.1186/1471-2431-13-135 [ Links ]
20. South African Institute for Sensory Integration (SAISI). Clinical Observations Adapted from J Ayres. South Africa: South African Institute for Sensory Integration, 2005. [ Links ]
21. Smith Roley S, Mailloux Z, Miller-Kuhaneck M, Glennon T. "Understanding Ayres Sensory Integration®," OT Practice, 2007; 17:CE-1-CE-8. [ Links ]
* Corresponding Author: Annamarie van Jaarsveld. Email: gnatnavj@ufs.ac.za


{kind=link}