










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.49 n.1 Pretoria Apr. 2019
http://dx.doi.org/10.17159/2310-3833/2019/vol49n1a2
SCIENTIFIC ARTICLES
Screening fitness to drive by occupational therapists in Gauteng Public Healthcare - an Action Learning Action Research outcome
Hester van BiljonI; Daleen CasteleijnII; Simon RabothataIII; Sanetta HJ du ToitIV
IB Occ Ther (UFS), M Occ Ther (UFS), PhD (Wits) https://orcid.org/0000-0003-4433-6457 Private practitioner at Work-link Vocational Rehabilitation practice
IIB Occ Ther (Pret), B Occ Ther (Hons)(Medunsa), Dip Voc Rehab (Pret), DHETP (Pret), M Occ Ther (Pret), PhD (Pret) https://orcid.org/0000-0002-0611-8662 Associate Professor, University of the Witwatersrand, Faculty of Health Sciences, School of Therapeutic Sciences, Occupational Therapy Department
IIIB Occ Ther UL (Medunsa), Post Grad Dip Voc Rehab UP https://orcid.org/0000-0001-9102-9893 Assistant Director, Therapeutic & Medical Support Services, Gauteng Health Department, Johannesburg
IVB Occ Ther (UFS), M Occ Ther (UFS), MSc Occ Ther (University of Exeter, UK), PhD (UFS) https://orcid.org/0000-0003-1348-6313 Affiliated lecturer, University of the Free State, Department of Occupational Therapy. Lecturer, University of Sydney, Faculty of Health Sciences, Discipline of Occupational Therapy
ABSTRACT
INTRODUCTION: In South Africa, public healthcare users equate the ability to drive a motor vehicle to employability and access to essential services. When injury or illness threatens the ability to drive, the multi-professional medical team usually refer the problem to the occupational therapist who will make decisions about patients' fitness to drive a motor vehicle.
METHOD: Over the course of five years, a collaborative task team applied multiple Action Learning Action Research (ALAR) cycles to address the problem. Qualitative data collected included field notes, reflective journaling, meeting minutes and a survey.
RESULTS: ALAR cycles resulted in a user manual and tool to screen driver fitness for occupational therapists. A follow-up survey indicated that despite a low user ratio, clinicians were of the opinion that the screening tool was user-friendly and contextually relevant to their practices
CONCLUSION: ALAR was effective in addressing a practice problem and empowering clinicians to develop a structured approach to screen fitness to drive in patients accessing public healthcare. Screening, as a first step within the field of driving rehabilitation, is now available in Gauteng public healthcare.
Key words: Driving rehabilitation, driving screening, public healthcare, action research action learning.
INTRODUCTION
Driving is categorised as an instrumental activity of daily living (IADL)1. In South Africa, the ability to drive a motor vehicle is a venerated skill and popularly considered an entry to the labour market. Public healthcare serves 84% of South African healthcare users2, where heavy patient-loads at overburdened, understaffed and ill-equipped facilities often result in compromised healthcare quality3. At the time of this research there were no driving rehabilitation services in Gauteng public healthcare, despite it being one of South Africa's best healthcare resourced provinces4. Individual therapists working as driving experts and several private occupational therapy practices offered driving rehabilitation but these services were fiscally and physically inaccessible to public healthcare users.
The June 2014 National Household Travel Survey5 showed 12,6 million people resided in Gauteng and 40% of the older than 18 years population had drivers' licences. Drivers that use public healthcare are frequently employed in the formal or informal public transport industry. These drivers are often sole breadwinners for extended families, making them desperate to return to driving as it safeguards their income and ensures access to essential services, such as schools and clinics, and maintains their social status for themselves and their families.
Occupational therapy as a profession has an acknowledged role within the field of driving rehabilitation6. Internationally there are occupational therapy associations that provide clear driving rehabilitation practice guidelines7. In South Africa guidance to occupational therapists and/or position statements within the field of driving rehabilitation are still only developing and calls for investigation and clarity8.
In South African public healthcare, occupational therapists face challenges that are typically experienced in a developing economy9. In addition, they witness a high staff turnover and the bulk of clinical work is delivered by newly graduate community service occupational therapists with limited clinical experience10. The Gauteng Vocational Rehabilitation Task Team (VRTT) is an interest group of occupational therapists concerned with vocational rehabilitation services in Gauteng public healthcare. They took note of the problem that clinicians needed guidance on the nature and extent of addressing the driving ability of patients after injury or illness. Positioning driving rehabilitation, with its associated complexity, high level of responsibility and possible legal repercussions, within an already burdened public healthcare sector was problematic. In addition it would require commitment to a multi-level collaborative process to ensure guidance by experts and buy-in on service delivery level11.
The aim of this article was to present an Action Learning Action Research (ALAR) process that resulted in the development of a Screening Fitness to Drive tool and user manual.
LITERATURE REVIEW
Driving can be described as an act of safely operating a motor vehicle to a goal-directed destination12. Inability to drive could have severe repercussions for drivers, passengers and the environment within which the driving takes place6. When considering fitness to drive, the synthesis between functional ability, skill, experience and behaviour is a complex one13. This gets more complex if impairment, disability, medication, vehicle adaptations, assistive devices and compensatory aids are added to the mix. The latter is the domain of driving rehabilitation.
Driving rehabilitation is an intervention to redress impairment related to the driving task and to facilitate fitness to drive14. The field comprises a multi-disciplinary approach15 of screening, assessment, intervention, accommodation, adaptations and modification to ensure safe driving. Screening tools are used to identify persons at risk of failing on-road assessments16. Driving evaluation consists of a clinical, off-road assessment followed by an on-road assessment17. Driving efficiency is improved with on-road driving rehabilitation18and a variety of interventions, such as computer-based driving simulator training, off-road skill-specific training and off-road education programmes19. Accommodation, adaptation and modification of motor vehicles are also prevalent interventions in the field20. Driver screening is thus the start of a multi-facetted service available to those whose driving ability is at risk21.
Occupational therapists' knowledge of pathology/injury/illness, combined with a knowledge of activity requirement, positions them to bridge the gap between healthcare institutions and the public sphere22 where driving takes place. Davis et al23 states that the skills, knowledge base, and scope of practice of occupational therapy, enhanced by advanced education in driving rehabilitation, places the profession in the vanguard of driving rehabilitation. They further state that driving rehabilitation warrants attention in all areas of occupational therapy practice. Occupational therapists are globally active in the field of driving rehabilitation6. They investigate and make complex decisions regarding fitness to drive24 and are involved in enablement of people with disabilities to drive motor vehicles19. There is also evidence to show that occupational therapists investigate the reliability of the tests25 and assessments26 that they commonly use in this field.
In South Africa, scientific evidence of the profession's involvement in driving rehabilitation is sparse. There is however prolific evidence of this in grey literature, such as in the official newsletter of the Occupational Therapy Association of South Africa27, other professional magazines28 and newspapers. A research study that explores the lived experiences of South African spinal cord injured drivers8 identified the lack of rehabilitation professionals' involvement in driving rehabilitation research. It calls for scientific evidence from South African occupational therapists in the field of driving rehabilitation.
Driving a motor vehicle in public, demands regulation29. The demand intensifies when people with disabilities, and the elderly, drive motor vehicles, as ethical issues related to the protection and rights of vulnerable persons, join the fray. South African occupational therapists need an awareness of the potential consequences of their decisions and interventions in driving rehabilitation. Alternatively, they should be aware of the repercussion when they avoid making decisions or refuse to offer intervention. A sound knowledge of South African legislation and national strategies, policies and protocols that have an impact on driving a motor vehicle are necessary. As driving is often linked with employment, a working knowledge of labour legislation is also needed. In addition, therapists have to continue to comply with their professional codes of conducts and their patients' rights.
It is within such complex and multifarious realities that Action Research was found to be an effective methodology30. In addition the methodology allows practitioners to address practice problems while generating contextually relevant knowledge31.
METHOD
Study design
This study was guided by the epistemology of action learning and action research (ALAR) during the five years of inquiry described in this article. The typical action research cycles32 of observe, plan, act and reflect was seen as cycles within cycles as it occurred on an individual and group basis. The ALAR design allowed learning33, emancipation and transformation34 to take place, as participants were included as fellow researchers35 generating knowledge within their clinical practices to which they and their patients could relate36.
Population and Sampling Procedure
In action research, the term stakeholders37 is used to describe populations who would be affected by or are able to affect practical change. In this study, stakeholders can be seen as insiders, research participants within public healthcare, or outsiders, (research participants who were not affiliated with public healthcare). There were five stakeholder groups.
The first was a collaborative research group that consisted of an insider interest group, the Vocational Rehabilitation Task Team (VRTT), and an outsider, a PhD candidate (the first author). The VRTT was a group of occupational therapists with an interest in vocational rehabilitation, working at various levels in Gauteng's public healthcare sector. Their positions ranged from Head Office management to Community Service occupational therapists. Group membership changed continuously, fluctuating between five and 12. The PhD candidate, an outsider, was an honorary member of the VRTT. Her PhD, titled Transforming Vocational Rehabilitation in Occupational Therapy Departments in Gauteng's Public Healthcare through Action Research Action Learning, concurred with the VRTT vision.
For the Screening Fitness to Drive study, the collaborative research team incorporated additional insiders groups. The second stakeholder group was an insider group of occupational therapists who attended the 2014 Vocational Rehabilitation Orientation Workshop. They were predominantly community service occupational therapists who had graduated the previous year and needed to do a year of community service in a public healthcare institute of their choice38. These attendees were invited to become part of the research collaboration and 38 of them volunteered to take part.
The 2015 research cycles were the third stakeholder insider group, and consisted of 10 VRTT members and six clinical occupational therapists who worked together in clinical public healthcare settings.
The fourth was an outsider group of nine experts in the field of driving rehabilitation; they were enlisted as critical friends39 in the study for their opinions and comments. The selection criteria for this group were occupational therapists with previous or current experience in South Africa's public healthcare and with more than five years of experience in the field of driving rehabilitation.
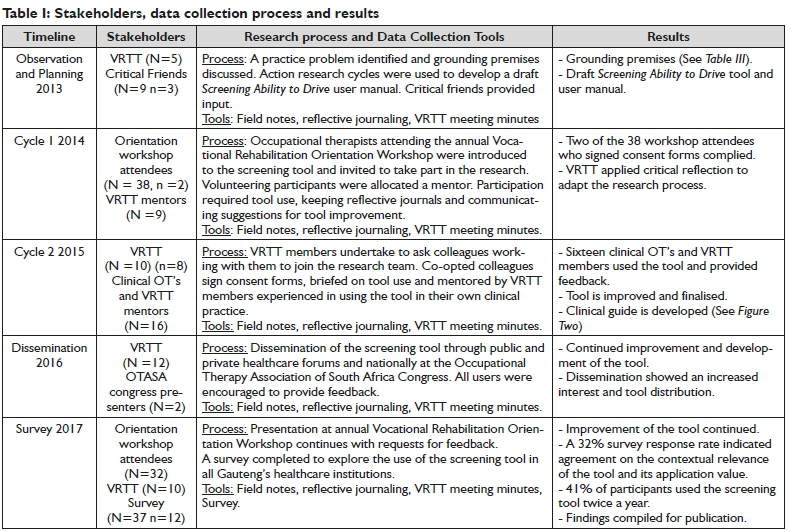
The fifth stakeholder group were insider occupational therapists who took part in a survey that was sent to 37 public healthcare institutions. Table l on page 6 shows how stakeholders fit into the data collection process and consequent results.
DATA COLLECTION
The data gathering process for this inquiry took place over five years, from September 2013 to April 2017, in the form of annual action research cycles. The VRTT used the first meeting of a year to plan. Throughout the year, planned actions took place, data was analysed, processed and reported back at each meeting. The last meeting of the year was used to critically reflect on the year's actions. Figure 1 on page 6 shows the process of the five year study.

When the PhD candidate joined the VRTT in 2013, one of the first practice problems tabled was the question of what should occupational therapists in public health be doing regarding driving rehabilitation. The problem was defined and a decision was made to address it with ALAR. Observation and planning to address the problem ensued.
The collaborative research team commissioned the PhD candidate to draw up a draft screening of fitness to drive user manual; she did so using individual action research cycles40. The course-work of a driving rehabilitation workshop and a driver-screening process, already in use by the candidate's private practice, was employed to develop the draft. This was sent to critical friends who were experts in the field of driving rehabilitation and their feedback and suggestions were worked into the draft. The draft screening fitness to drive user manual was presented to the VRTT at the last 2013 meeting. Collectively a decision was made to use it in public
healthcare, putting it through multiple cycles of planning, action and reflection.
The VRTT decided to use the 2014 Vocational Rehabilitation Orientation Workshop to launch the first ALAR cycle of the driver-screening user manual. Attendees of this workshop were invited to use the Screening Fitness to Drive tool with their patients and provide feedback in the form of critical reflections. At the orientation workshop, the dynamics of ALAR cycles were explained, the draft user manual was presented and a screening demonstrated. Attendees who volunteered to participate in the research signed consent forms, were assigned a mentor (one of the VRTT members) and followed up on a regular basis. Feedback of progress was given at each VRTT meeting and this continued until the end of the year. Results informed the VRTT that the plan was not working. Therapists were not using the tool and very little feedback was received. The decision was made to attempt a new approach in 2015.
At the first meeting, in 2015, the VRTT decided that all VRTT members were to use the Screening Fitness to Drive tool with their patients and invited colleagues working with them to join the second ALAR cycle. They would teach colleagues to use the screening tool, mentor them and capture critical reflections and suggestions to feedback at the VRTT meetings. This feedback was used to improve the tool and user manual. By the end of the year, the tool and user manual were improved and the decision was taken to finalise them. The PhD candidate did this, again sending them to critical friends whose feedback was incorporated. It was sent for language editing and compiled into an easy to use, bound, hard copy manual and an electronic format.
In 2016, the user manual was disseminated through official public healthcare channels to all clinical occupational therapists working in Gauteng. The annual presentation and practical demonstration at the Vocational Rehabilitation Orientation workshop continued, introducing it to occupational therapists entering Gauteng public healthcare. All critical friends received a copy, and it was shared with private practitioners, academic institutions and public healthcare managers from other provinces who expressed interest. At the National Occupational Therapy Association of South Africa Congress, 2016, an oral presentation was given41.
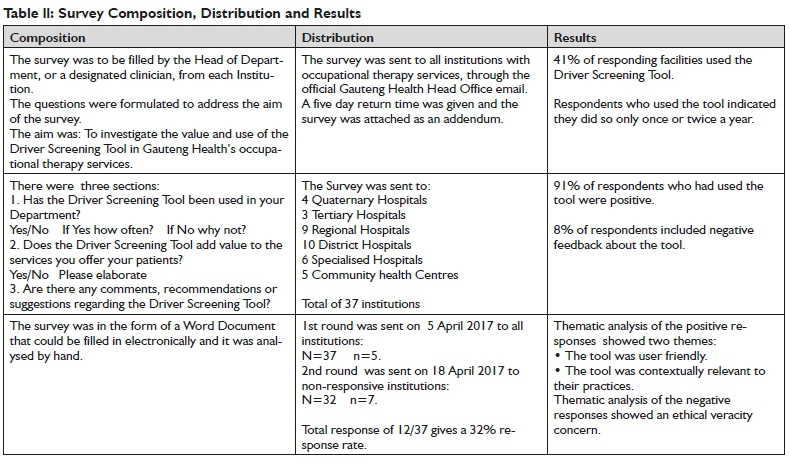
In 2017, the VRTT launched a survey to explore if clinical occupational therapists were using the tool. The survey was sent to all Gauteng public healthcare institutions that employed occupational therapists involved in adult rehabilitation. Table ll above shows the composition, distribution and results of the survey.
Data Gathering Tools and Analysis
The field notes, reflective journaling and meeting minutes were systematically analysed by the researchers. In keeping with good practice analysis, and in support of action research principles11,42, the raw data were manually checked and analysed immediately after gathering, throughout the process. Data were summarised and categorised, and these summaries drove and dictated the next ALAR cycles and research stages.
Care was taken to process all decision making through the VRTT and to avoid power relationships that could jeopardise the emancipatory nature of action research43. Data were captured in the form of VRTT meeting minutes, field notes and reflective journaling. The researcher kept her own reflective journal. While participants were using the user manual, they were followed up by a designated mentor who summarised presented feedback at VRTT meetings, where it was captured in meeting minutes.
Credibility, Transferability, Dependability and Conformability
Confidence in the credibility, transferability, dependability and conformability of the findings were pursued throughout. The collaborative nature of action research ensures built in checks for credibility and conformability consideration. In this study, outsider experts on the subject matter were used as critical friends and insider critical reflection was routinely employed to ensure confidence in the results of the inquiry. Data analysis of the survey results saw two of the authors, working independently of each other, transcribe and thematically analysed the data. They compared their interpretations and confirmed a consensus opinion for use in this paper. Using insiders as co-researchers and developing the driver screening tool within the context it will be used ensures high dependability value. For the same reason caution should be exercised when considering transferability of the knowledge generated in this study.
Ethical Clearance, Informed Consent and Bias Declaration
Ethical clearance of the research and informed consent of all participants fell under the larger PhD study with the ethical clearance number M130649. There is no bias to declare.
RESULTS AND DISCUSSION
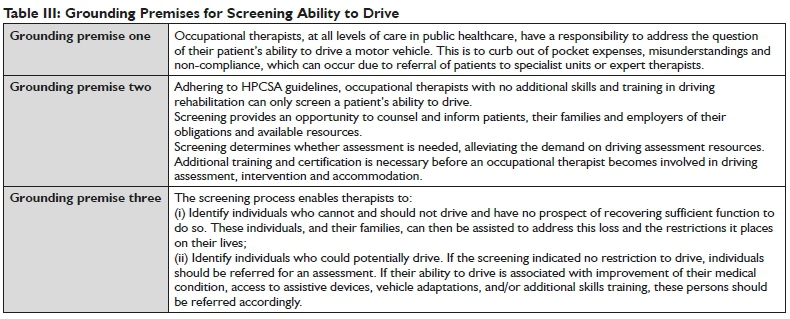
The observation that driving rehabilitation was the first concern, tabled within the collaborative research group, could be indicative of the urgency of the problem. There was also awareness in the group of a social justice factor due to the lack of accessibility and available of driving rehabilitation for injured and/or disabled drivers who are dependent on public healthcare. In planning to address the practice problem Mtetwa et al's8 call for South African occupational therapists to do research and publish in the field of driving rehabilitation came to light, confirming the VRTT's resolve to approach the problem systematically. Considering the problems praxis the VRTT realised that international driving rehabilitation practices could not be drafted directly into the South African context. In addition they found that as the field was sparsely researched in South Africa there were basic underlying principles missing. Grounding premises were decided on to guide the development of a contextually relevant Driver Screening Tool and are shown in Table lll on page 8.
Using these premises, a draft user manual to screen fitness to drive was developed by the PhD candidate who saw it through multiple individual cycles of planning-acting-reflecting-improving. The manual was designed to be easy to read and use by clinical occupational therapists in adult practices at all levels of public healthcare in Gauteng.
Critical reflection at the end of Cycle One showed that two out of 38 workshop attendees used the tool and no feedback was given. The VRTT therefore decided on a new action cycle, demonstrating the democratic validity44 of ALAR as an inherent part of the study. Cycle Two saw 16 VRTT members and their colleagues use the tool in their clinical practices, critically reflect on it and provide this as feedback to enable improvement of the tool. The improvement reported to be of most practical value was the development of a clinical guide that therapists could laminate and use in clinical settings. The clinical guide can be found in Appendix 1 at the end of this article.
The VRTT agreed to finalise the Screening Fitness to Drive user manual, which was written assuming basic level occupational therapy skills. The user manual consisted of a cover letter, background and general information, legal and ethical considerations, a step-by-step guide, conclusion, recourses, skills training and suggested readings and references. The dissemination of this screening tool and user manual saw a growing interest beyond Gauteng Province.
Three years after the driver-screening tool had been in use in Gauteng public healthcare sector, the VRTT decided to investigate its use. A user survey was developed. The results showed that 41% of responding facilities used the driver screening tool, but only once or twice a year. Opinion on the usefulness of the tool showed that 91% of respondents were positive about the tool. They felt it was a good tool to have, relevant to their patient profile, easy to use and understand and they planned to use it in future. The 8% who included negative feedback indicated that having screened their patients, they had created an awareness of and a hope for driving rehabilitation intervention in their patients. These patients could not access private driving rehabilitation services due to the costs involved and within the Gauteng public healthcare, there were no driving rehabilitation resources to which they could be referred.
LIMITATIONS AND ANTICIPATED FUTURE ALAR CYCLES
Without incorporating the voice of injured and/or disabled drivers the relevance and sustainability of a driving rehabilitation service or intervention needs to be questioned. All future enquiries by South African occupational therapists need to start with this in mind.
Screening and creating an awareness of driving rehabilitation without having accessible referral sources impacts on the veracity of occupational therapy practice and is an ethical concern. Future research to inform and motivate policy makers to address this void within public healthcare should be seen as a matter of urgency, especially as it demonstrates compliance with the South African Constitution45 and NHI46 goals.
The ALAR design used in this research enriched the professional lives of therapists and created a service that was not previously available to patients in public healthcare. It did so incorporating input to the body of knowledge from the inexperienced occupational therapist as well as acknowledged experts in the field. The result was contextually relevant and for this reasons it was suggested as a design for future research and development of the field of driving rehabilitation within public healthcare. Continued ALAR cycles will also be necessary to ensure evolvement of the screening tool to keep up with ever changing legislation, healthcare environments and client and practitioner needs.
With any action research done as insider-outsider collaboration, the justification of knowledge claims and how power and control over the research process were distributed needs, to be a con-cern44. Even though all efforts were made to reduce the negative impact of power relations, it could still have been operative as the insider group consisted predominantly of inexperienced therapists and the outsiders were seen as experienced experts in the field of driving rehabilitation.
CONCLUSIONS
The use of the ALAR methodology was directly linked to the willingness of the collaborative research group to take on a practice problem they perceived to be complex and daunting. The research resulted in the development of a contextually relevant screening tool and user manual that allows drivers, who use public healthcare in Gauteng, access to the preliminary stage of driving rehabilitation. Clinical occupational therapists in Gauteng public healthcare now have a standard approach to screen their patients' fitness to drive a motor vehicle and ALAR cycles continue to improve and update the service.
Screening Fitness to Drive is a valuable resource as it reduces the pressure on scarce and expensive assessment resources. Used within public healthcare the screening tool has the additional benefit of creating awareness of intervention and rehabilitation that can enable driving independence and all its associated benefits and opportunities. However, there can be no meaningful impact unless it is efficiently linked with driving assessment and other driving rehabilitation services. To achieve this occupational therapist will have to cross the boundaries of private-public healthcare and extend their practices into other sectors, such as transport, labour and legislature.
ACKNOWLEDGEMENTS
Stakeholders and members of the VRTT: Simon Rabothata, Ashley Magner, Naazneen Ebrahim, Claudette Parkinson, Mashudu Mpho-honi, Catherine Couvaras, Buhle Moleofane, Lynn Soulsby, Madidi-malo Mogale, Marlene Robus, Mariaan Jacklin, Zakkiya Akhalwaya, Siphosethu Nxumalo, Alta Voster, July Masango
The experts and critical friends who contributed towards the finalisation of the user manual: Caroline Rule, Lee Randall, Tania Buys, Megan Spavins, Janine Schoeman, Derryn Brummer, Megan Townshend, Jane Baker, all members of the Driving Interest Group, the Skills Basket and Work-Link.
The 2013 Faculty of Health Sciences Development Grant from the University of the Witwatersrand.
REFERENCES
1. Sherman FT. Driving: the ultimate IADL. Geriatrics. 2006; 61(10): 9-10. http://worldcat.org/issn/00I6867X. [ Links ]
2. Motsoaledi A. 84% of South Africans get 2nd rate healthcare. News 24. 2013. [ Links ]
3. van Rensburg HCJ. South Africa's protracted struggle for equal distribution and equitable access - still not there. Human Resources for Health. 2014; 12(26). https://doi.org/10.1186/I478-4491-12-26. [ Links ]
4. Stuckler D, Basu S, McKee M. Health care capacity and allocations among South Africa's provinces: infrastructure-inequality traps after the end of apartheid. American Journal of Public Health. 2011; 101(1): 165-72. http://doi.org/10.2105/AJPH.2009.I84895. [ Links ]
5. Lehohla P National Household Travel Survey - Gauteng Profile. June 2014, Pretoria: Statistics South Africa; 2015. [ Links ]
6. Golisz K. Occupational Therapy Interventions to Improve Driving Performance in Older Adults: A Systematic Review. American Journal of Occupational Therapy. 2014; 68: 662-9. http://doi.org/10.5014/ajot.2014.011247. [ Links ]
7. Canadian Association of Occupational Therapists (CAOT). CAOT Position Statement Occupational Therapy and Driver Rehabilitation. 3704; 2009. [ Links ]
8. Mtetwa L, Classen S, van Niekerk L. The lived experience of drivers with a spinal cord injury: A qualitative inquiry. South African Journal of Occupational Therapy. 2016; 46(3): 55-62. http://dx.doi.org/10.17159/2310-3833/2016/v46n3a10. [ Links ]
9. van Biljon H, Casteleijn D, du Toit S, Soulsby L. Opinions of Occupational Therapists on the Positioning of Vocational Rehabilitation Services in Gauteng Public Healthcare. South African Journal of Occupational Therapy. 2016; 1(1): 45-53. http://dx.doi.org/10.17159/2310-3833/2016/v46n1a10. [ Links ]
10. van Biljon H, Casteleijn D, du Toit S. Developing a vocational rehabilitation report writing protocol - a collaborative action research process. South African Journal of Occupational Therapy. 2015; 45(2): 15-21. http://dx.doi.org/10.17159/2310-3833/2015/V45N2A4. [ Links ]
11. McNiff J. Concise Advice for New and Experienced Action Researchers. Action Research for Professional Development. Dorset: September Books; 2010. [ Links ] .
12. Wiegand DM, Hickman JS, Geller ES. Automobile Safety During Adulthood. New York: Springer US; 2014. [ Links ]
13. Wolfe PL, Lehockey KA. Neuropsychological Assessment of Driving Capacity. Archives of Clinical Neurospsychology. 2016; 31(6): 5I7-29. [ Links ]
14. Harkey D, Griffith M, Staplin L, Ross L. Taxonomy and Terms for Stakeholders in Senior Mobility E-C2II; 2016. [ Links ]
15. Carr D, Schmader K, Bergman C, Simon TC, Jackson TW, Haviland S, et al. A Multidisciplinary Approach in the Evaluation of Demented Drivers Referred to Geriatric Assessment Centers. Journal of the American Geriatrics Society. 1991; 39(11): 1132-6. https://onlineli-brary.wiley.com/doi/abs/10.1111/j.I532-54I5.1991.tb02882.x. [ Links ]
16. Jerome L, Segal A. Prediction of Driving Accident Risk in Novice Drivers in Ontario: The Development of a Screening Instrument. Dr. Lisa Dorn, editor. London: Routledge; 2017. [ Links ]
17. Vrkljan BH, Myers AM, Blanchard RA, Crizzle AM, Marshall S. Practices Used by Occupational Therapists and Others in Driving Assessment Centers for Determining Fitness-to-Drive: A Case-Based Approach. Physical & Occupational Therapy In Geriatrics. 2015; 33(2): 163-74. https://www.tandfonline.com/doi/abs/I0.3109/0270318I.2015.I0I6647. [ Links ]
18. Imhoff S, Lavallière M, Teasdale N, Fait P Driving assessment and rehabilitation using a driving simulator in individuals with traumatic brain injury: A scoping review. NeuroRehabilitation, 2016; 39(2): 239-5I. https://www.ncbi.nlm.nih.gov/pubmed/27372359.http://doi.org/I0.3233/NRE-I6I354. [ Links ]
19. Unsworth CA, Bakera A. Driver rehabilitation: A systematic review of the types and effectiveness of interventions used by occupational therapists to improve on-road fitness-to-drive. Accident Analysis and Prevention, 2014; 71: 106-14. https://www.ncbi.nlm.nih.gov/pubmed/24906I64. http://doi.org/I0.I0I6/j.aap.2014.04.017. [ Links ]
20. Di Stefano M, Stuckey R. Ergonomic Considerations for Vehicle Driver-Cabin Configurations: Optimizing the Fit Between Drivers with a Disability and Motor Vehicles. Sõderback I, editor. Cham: Springer; 2015. [ Links ]
21. Devos H, Akinwuntan AE, Nieuwboer A, Truijen S, Tant M, De Weerdt W. Screening for fitness to drive after stroke. A systematic review and meta-analysis. Neurology. 2011; 76(8): 747-56. https://doi.org/10.1212/WNL.0b0I3e31820d6300. [ Links ]
22. Kielhofner G. Conceptual Foundations of Occupational Therapy Practice. Philadelphia: F A Davis Company; 2009. ISBN: 9780803620704. [ Links ]
23. Davis ES, Stav WB, Womack J, Kannenberg K. Driving and community mobility. American Journal of Occupational Therapy. 2016; 70(64S112). Epub 10.5014/ajot.2010.64S112. http://search.pro- quest.com/docview/2080983138. [ Links ]
24. Unsworth CA, Harries P Davies M. Using Social Judgment Theory method to examine how experienced occupational therapy driver assessors use information to make fitness-to-drive recommendations. British Journal of Occupational Therapy. 2015; 78(2): I09-20. https://doi.org/10.1177/03080226I4562396. [ Links ]
25. Bruce C, Unsworth CA, Tay R Dillon MP Development and validation of the Occupational Therapy Risk Propensity Test (OT-RiPT) for drivers with disability. Scandinavian Journal of Occupational Therapy. 2015; 22(2): 147-52. https://doi.org/10.3109/11038128.2014.992952. [ Links ]
26. Dickerson AE, Meuel DB, Ridenour CD, Cooper K. Assessment Tools Predicting Fitness to Drive in Older Adults: A Systematic Review. American Journal of Occupational Therapy. 2014; 68: 670-80. https://doi.org/I0.50I4/ajot.2014.0II833. [ Links ]
27. Rule C. Positioning and set-up of the vehicle for drivers with spinal cord injury. FOCUS - Official Newsletter of OTASA. 2014; 3: 40-3. [ Links ]
28. Ebrahim N. Disability and Driving. An Intersectorial Workshop. South African Psychiatry. 2018; 15:47-49. Epub http://www.south-africanpsychiatry.co.za. [ Links ]
29. Republic of South Africa. Amendment of the National Road Traffic Regulations. National Road Traffic Act; 1996 (ACT NO. 93 OF I996); 2014. [ Links ]
30. Ozerdem A, Bowd R. Participatory Research Methodologies. Development and Post-Disaster/Conflict Reconstruction. Ist ed. London: Routledge; 2016. https://doi.org/I0.4324/978I3155995I9. [ Links ]
31. Townsend A. Action Research: The Challenges Of Changing And Researching Practice. UK: Open University Press; 2013 isbn = 0335244432. [ Links ]
32. Stringer ET. Action Research. California: SAGE; 2014. isbn=I483320731. [ Links ]
33. Brook C. Action Learning in Healthcare. Dilworth RL, Bohyk Y editors. Hampshire: Palgrave Macmillan; 2010. [ Links ]
34. Reason P Bradbury H. Handbook of Action Research. London: SAGE Publications Ltd; 2007. isbn=1412920302. [ Links ]
35. Marsick V O' Neil J. The Many Faces of Action Learning. Management Learning. 2010; 30(2): 159-76. https://doi.org/10.1177/I350507699302004. [ Links ]
36. Zuber-Skerritt O. Action Learning and Action Research. Songlines through Interviews. Rotterdam, Netherlands: Sense Publishers; 2009. [ Links ]
37. Dick B. Entry and Contracting. Action research and evaluation online. Australia: www.aral.com.au/areol; 2013. [ Links ]
38. Maseko L, Erasmus A, Di Rago T, Hooper J, O' Reilly J. Factors that influence choice of placement for community service among occupational therapists in South Africa. South African Journal of Occupational Therapy, 2014; 44(1): 36-40. http://dx.doi.org/10.17159/2310=3833/2016/v46n3a1. [ Links ]
39. Costa A, Kallick B. Through the lens of a critical friend. Educational Leadership. 1993; 51(2): 49-51. [ Links ]
40. van Biljon HM. Transforming the Vocational Rehabilitation Services of Occupational Therapists in Gauteng Public Healthcare through Action Learning Action Research. Parktown, Johannesburg: University of the Witwatersrand; 2016. [ Links ]
41. van Biljon HM, Rabothata S. Screening ability to drive in occupational therapy. 35th National Congress of the Occupational Therapy Association of South Africa; Birchwood Hotel & Conference Centre Johannesburg; 2016. [ Links ]
42. Creswell J. Qualitative inquiry and research design (2nd ed). CA Sage: Thousand Oaks; 2007. https://psycnet.apa.org/re-cord/2006-13099-000 [ Links ]
43. du Toit S, Wilkinson A. Research and Reflection: Potential Impact on the Professional Development of Undergraduate Occupational Therapy Students. Springer Science + Business Media; 2010; 23(Sys-tematic Practical Action Research): 387-404. Epub 5 February 2010. http://doi.org/10.1007/s11213-010-9165-5. [ Links ]
44. Herr K, Anderson GL. The Action Research Dissertation: A Guide for Students and Faculty. United States of America: SAGE; 2005. http://dx.doi.org/10.4135/9781452226644. [ Links ]
45. Republic of South Africa. The Constitution of the Republic of South Africa, Act 108 of 1996; 1996. [ Links ]
46. Republic of South Africa. National Health Insurance (NHI) White Paper. Pretoria; Government Printers; 2017. [ Links ]
 Correspondence:
Correspondence:
H van Biljon
HesterMvanBiljon@gmail.com
Clinical Guide to Screen fitness to Drive



{kind=link}
{kind=link}
{kind=link}