










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.48 n.3 Pretoria Dec. 2018
http://dx.doi.org/10.17159/2310-3833/2017/vol48n3a2
SCIENTIFIC ARTICLES
Hand health for all: Do undergraduate occupational therapy hand curricula respond to the call?
Kirsty van StormbroekI; Helen BuchananII
IBSc (Occ Ther) MSc (Occ Ther) UCT- Lecturer, Department of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand, Johannesburg, Republic of South Africa. During the research: Division of Occupational Therapy, Department of Health and Rehabilitation Sciences, University of Cape Town, Cape Town
IIBSc (Occ Ther) MSc (Occ Ther) PhD UCT- Associate Professor, Division of Occupational Therapy, Department of Health and Rehabilitation Sciences, University of Cape Town, Cape Town, Republic of South Africa
ABSTRACT
The call for higher education curricula to be responsive to the South African context is growing louder. Injuries to the hand are common in South Africa and intervention is often provided by novice occupational therapists who may work in complex practice contexts with limited supervision. Comprehensive hand health practice addresses both the biomedical and occupational dimensions of the human hand. Undergraduate education programmes should be responsive to this reality in preparing graduates adequately for hand practice. This article describes the content of hand curricula within occupational therapy undergraduate programmes in South Africa with the purpose of considering how they prepare graduates for the practice realities they may face during community service.
A descriptive cross-sectional survey design was used with an online questionnaire aimed at determining the nature and extent of hand curricula presented in South African undergraduate occupational therapy programmes (n=8). Data were analysed using Stata 12.
Time allocated to hand impairments varied considerably across universities. While assessment of biomedical performance components were taught by all universities, the occupational perspective was limited. The range and number of hand conditions and treatment modalities that were taught also varied.
Findings are discussed against the contextual realities of practice in South Africa, primary health care policy, and national and international minimum standards for the education of occupational therapists. Core aspects of a hand curriculum are proposed as a means to enhance comprehensive hand health practice.
Key words: Hand practice, occupational therapy education, hand health
INTRODUCTION
A key milestone towards "eliminate[ing] poverty and reduc[ing] inequality by 20304 is providing "affordable access to quality health care while promoting health and wellbeing"1:24. One initiative to improve the quality of health care is "increase[ing] the quantity and quality of health professionals to meet local needs"2:35. While substantial inroads have been made towards increasing the number of graduating health professionals in South Africa, questions as to whether graduates are receiving the necessary education to meet the health care needs of the population have been raised3-7. This article addresses this question in relation to occupational therapy graduate preparedness to meet the needs of people with hand impairments during their Community Service (CS) year. CS is a year of compulsory public sector practice undertaken by graduating health care professionals in South Africa. They are required to complete this year of service before being able to register as independent practitioners and work in settings of their choice. The article reports one aspect of a larger study that investigated the extent to which community service occupational therapists are equipped to treat patients with hand impairments. The larger study, parts of which have been published previously8,9, captured aspects of the general practice experience of the 2013 Community Service occupational therapists, as well as their perceived preparedness for treating patients with hand impairments.
Although hand injuries are common globally10, South African data is limited. Considering that two of the four contributors to the quadruple burden of disease potentially include conditions involving the hand, namely trauma and injuries and non-communicable diseases, it is likely that prevalence is relatively high. Studies suggest that violence-related and workplace injuries constitute a noteworthy burden in South Africa11-14. The high manual labourer population is likely to contribute to this burden considering the risks of sustaining hand impairments. Although prevalence data is limited, it is reasonable to suspect that the impact of hand impairments on rehabilitation services in South Africa is likely to be significant14.
Hand services within the South African health system may be provided in community health clinics, linked to basic orthopaedic surgery at secondary facilities and at large tertiary clinics with specialist hand surgeons, although the latter are generally available only in larger cities. Patients treated at tertiary level may be referred to secondary or primary levels of health care for further rehabilitation once specialist treatment is complete. As a result, occupational therapists employed at all levels within the health system may be tasked with providing services to patients with hand impairments. Therapists at tertiary level have the advantage of being able to develop expertise in this area due to the greater number of patients with hand impairments and the availability of more experienced health professionals, while those at secondary and primary level are required to be generalists and may have limited exposure to colleagues with experience in this area. Generalist occupational therapists require a range of knowledge and skills to deal with the multiple health conditions they may encounter; hence the acquisition of specialist knowledge is challenging.
A further concern is the bias towards the private sector and the largest two provinces (Gauteng and the Western Cape) as reflected in the 2015 membership figures for the South African hand surgery and therapy societies15-17. A review of these figures revealed that 86% of hand surgeons and 75% of therapists worked in the private sector with a few working across sectors. Hand surgeons were located in five of the nine provinces, and almost 80% of listed surgeons and 67% of therapists practiced in Gauteng and the Western Cape - the most urban provinces. This situation is alarming considering that 52% of South Africans live rurally4 and more than 70% are unable to access private health care18. As there is no data on health professionals providing hand services who are not members of these societies, or for generalists who treat hand impairments, it can only be concluded that health professionals with a special interest in treating hand impairments are predominantly urban-based and employed in the private sector. They also may, or may not, represent those with experience and expertise in this area, although de Klerk19 reported that more than 90% of therapists with more than five years' experience in hand rehabilitationa worked in the private sector. Furthermore, within the broader study in which this article is situated, CS occupational therapists confirmed the limited availability of hand surgery services and hand rehabilitation expertise in rural and underserved areas of South Africa8-9. It can therefore be surmised that many patients requiring this expert service are unlikely to be able to access it, and that services for the majority of the population fall predominantly to novice and inexperienced therapists such as CS occupational therapists.
CS occupational therapists also reported treating a range of health conditions including those to the hand which they reportedly see regularly (median: 20 per month; range: 0 to 225 per month)8-9. Conditions treated most frequently included bone and joint conditions, arthritic conditions, thermal injuries, tendon injuries, complex injuries, infections and peripheral nerve injuries8-9,19-20, many of which are caused by accidents or injury implying a significant need to refocus services towards prevention and promotion. Therapists use a variety of treatment modalities with home programmes, manual therapy, exercise, activity as a means/end, training in activities of daily living, strengthening and education being used most regularly8-9. Others, such as splinting, were used less frequently partly due to a lack of resources8-9.
In upper income countries such as America, hand therapy is considered a specialist area requiring advanced continuous professional development21. Anecdotal evidence suggests that many South African occupational therapy educators and clinicians similarly perceive this as a specialised area of practice, as do some novice occupational therapists22. The reality is however, that CS occupational therapists are required to treat a range of health conditions, including those related to the hand, often without adequate equipment, appropriate work areas and access to up-to-date evidence8-9. The situation is exacerbated by limited supervision from experienced colleagues and few opportunities for continuing professional development activities related to hand rehabilitation8-9. The lack of support and infrastructure along with the magnitude of the problems CS occupational therapists face in the area of hand rehabilitation may evoke contrasting emotions, for example feeling overwhelmed (42%) and feeling enthusiastic (48.4%), about this area of practice8-9,23.
CS occupational therapists encounter the additional challenge of communication difficulties, partly due to language discordance between patient and therapist, which may lead to a loss of meaning and therapeutic properties of the therapeutic relationship with the client which posed a hindrance to therapy8-9,23.
Acknowledging the contexts within which CS occupational therapists work and the services they are expected to deliver, it is critical to question whether the content of undergraduate occupational therapy programmes is appropriate and directed at meeting the needs of people with hand impairments in South Africa. Considering that the South African health system is based on a primary health care approach (PHC), occupational therapy curricula should reflect this approach. But what does this mean? With its strong health equity focus, a PHC approach entails preparing graduates to deliver services to people with limited or no access to hand health services and that such service be available to all. To enable graduates to develop the competencies required for providing hand health services, university curricula must prepare them for promoting hand healthb (for example, promoting mothers' ability to fulfil their roles effectively during the peri-partum period when they are at risk of developing carpal tunnel syndrome and De Quervains tenosynovitis), preventing hand impairments (for example, preventing hand injuries in factory workers or farm labourers at risk of degenerative, repetitive strain or traumatic hand conditions), and for curative and rehabilitative services to enable clients with hand impairments to achieve optimal health and well-being. A PHC approach suggests that occupational therapy students should learn to identify the social and occupational determinants of compromised hand health in order to provide contextually relevant interventions. Greater insights into the social and occupational determinants of hand impairments should also lead to occupational therapists taking a more active role in prevention and health promotion campaigns, for example raising awareness about unsafe working conditions that result in hand injuries. Preparing graduates to practice within a PHC framework thus suggests that hand curricula be positioned within a vision of hand health for all. In addition an occupational perspective would ensure that students consider the total being in his or her lived reality24.
Amongst other implications, it also mandates that graduates are prepared to develop and deliver services that are accessible to all South Africans and appropriate for diverse clients from diverse contexts. Extrapolating from the international and national Minimum Standards for the Education of Occupational Therapists documents25,26 to hand curricula, apart from considering the philosophical applications of a curriculum as a whole, is challenging. However, key concepts need to be considered as a backdrop for preparing graduates for comprehensive hand practice.
The 2016 revision of the World Federation of Occupational Therapists (WFOT) Minimum Standards document shows a major shift "...beyond education on bodily dysfunction" to "help[ing] populations, communities and individuals to live well"25:11. Social justice, occupational justice and equitable access to occupational therapy services also feature strongly. Local standards task undergraduate curricula with developing competent entry-level occupational therapists able to develop and deliver culturally and contextually relevant services to promote health, wellness and occupational justice for those at risk of occupational dysfunction26. The purpose of South African programmes is to graduate occupational therapists who have a robust understanding of the relationship between occupational engagement and health, and the impact of the environment on this relationship.
The capacity of curricula to develop therapists who are life-long learners, are sensitive to culture and diversity, and who pursue occupational justice in practice are described as fundamental characteristics. Core content includes knowledge of anatomy, physiology, human movement, clinical sciences, human behaviour and the social environment, PHC, health promotion and community development, research and an understanding of occupation and occupational therapy. The latter relates to the person-environment-occupation transaction and its relationship to health, therapeutic and professional relationships, the occupational therapy process and professional reasoning and behaviour26. Core practice content includes exposure to a comprehensive range of services and the use of individual, group/community and population approaches. A relative shift from individual-based intervention to population-based approaches is similarly reflected in the WFOT guideline along with the need for curricula to be both contextually responsive and anticipatory25. Exposure to diverse practice settings, and diverse clients, at risk of, or with acute or chronic health impairments is required. Interventions are to be directed at the person (singular or plural), the occupation, and the environment, with activity or occupation constituting the primary mode of intervention26. There is also a need to further delineate between undergraduate and postgraduate hand rehabilitation competencies with cognisance of the contextual demands on novice therapists in South Africa, the clinical reasoning capacity of undergraduates, and curriculum resources (for example, time and practice learning opportunities). The vision of hand health for all finds echo in the international and national Minimum Standards documents, yet current practice is skewed towards curative and rehabilitative services despite the adoption of the PHC approach in 199427 and the call for an occupational focus24.
A further consideration for practice and education within this area, is implementing evidence-based practice. Applying research findings from international studies is often problematic in South Africa for several reasons. Intervention approaches proven to be effective in developed contexts do not necessarily demonstrate more favourable outcomes in South Africa. For example, a study comparing the outcomes of flexor tendon rehabilitation protocols at a large urban hospital in South Africa, found similar results between early passive and early active mobilisation protocols28. Where the latter protocol has shown better outcomes globally, "non-compliance" (or the impact of complex contextual features in South Africa) was proposed as one of the reasons for the similarity in outcomes between the protocols. Similarly, another study on the same population of clients with flexor tendon injuries reported outcomes that were poorer than those reported in developed nations29. Understanding the nature and cause of these kind of discrepancies is critical to developing responsive curricula.
From a review of available evidence, hand rehabilitation services in South Africa appear skewed towards the private sector and urban provinces. It is clear that preventable trauma-based injuries are common, and hand rehabilitation services, despite being considered a specialist area of practice, are being delivered by novice occupational therapists in challenging environments. International and national standards for curricula should be used to inform and evaluate hand health content within the context of the overall curriculum. This article describes the content of hand curricula within occupational therapy undergraduate programmes in South Africa with the purpose of considering how they prepare graduates for the practice realities they may face during community service. A survey of hand curricula was situated in the larger project to understand the undergraduate preparation that novice therapists had received, and to create context for interpreting their perceived preparedness to treat patients with hand impairments.
METHODS
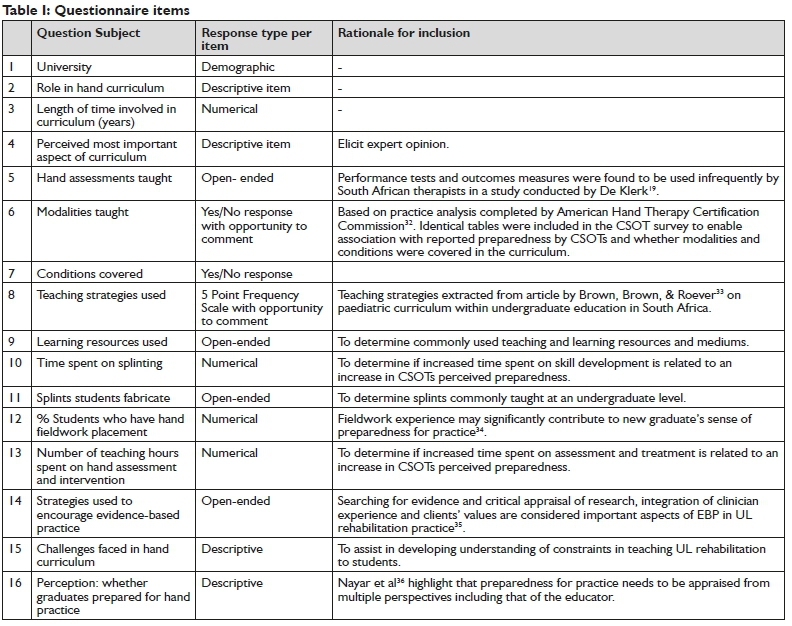
A descriptive cross-sectional survey design was used with a questionnaire designed to determine the content of hand curricula offered at each of the eight universities providing undergraduate occupational therapy education in South Africa (n=8). Questions explored conditions covered, treatment modalities taught, time spent on various knowledge and skill components, the proportion of students who had hand rehabilitation fieldwork placements and the teaching strategies used. Table I on page 6 provides an overview of the survey questions with the rationale for their inclusion.
To strengthen the content validity of the tool, three expert practitioners with more than 10 years clinical or educational experience in this area reviewed the questionnaire. The expert panel commented on the content of the questionnaire in terms of its ability to elicit the information required. Feedback although limited, was discussed with the second author to decide on the changes required. Changes included adding examples of treatment modalities (question 6), and types of injuries (question 7), and increasing the number of examples of learning resources (Question 9). A copy of the survey is available on request from the first author.
The survey was sent with an information sheet to the heads of the occupational therapy departments at the eight universities requesting participation. On permission from the head of department, the relevant staff member co-ordinating the hand curriculum completed the survey which was administered online using Fluid-surveys software30.
Surveys were allocated a number (1-8) and responses were dissociated from the name of the university. Frequencies and percentages were obtained using IBM Statistics 21.031 and responses to open ended questions were post-coded. Ethical clearance for the project was obtained from the University of Cape Town (HREC 551 / 2013).
RESULTS
Responses were received from educators at all universities (n=8). Two responses were initially received from one university where more than one educator involved in the hand curriculum responded. The researcher returned these responses to the university concerned, with the request to integrate them into a single response. This revised response was included in analysis.
Educators had been involved in teaching the programme for a median of 7 years (Range: 2-28). The median time apportioned to hand assessment and treatment was 30 hours (Range: 12-96), with a median of 22 hours (Range: 8-42) allocated to teaching splinting skills. In terms of fieldwork placements, an estimated average of 70% of students were placed in settings requiring provision of hand services, usually curative or rehabilitative in naturec. The most important aspects of the curriculum were considered to be assessment (n=5) and basic treatment of conditions (n=4). Educators from two universities considered scientific knowledge, splinting, treatment protocols, clinical reasoning and working with limited resources to be important. Mentioned less frequently (n=l for each) were contextual and occupational considerations, wound healing, the role of the occupational therapist in the hand multidisciplinary team, specialised treatment modalities, prioritising treatment aims, best practice, the ability to identify when to seek advice, and advocating for clients.
All universities taught performance component assessments with six covering hand function assessment. Half the programmes (n=4) included standardised and non-standardised tests (not specified) and three taught clinical observations of the hand. Few covered patient-rated assessment (n=2) and diagnostic tests (n=l). Educators from two universities made reference to assessing occupational performance.
Details of the conditions covered at the different universities are shown in Table II on page 6.
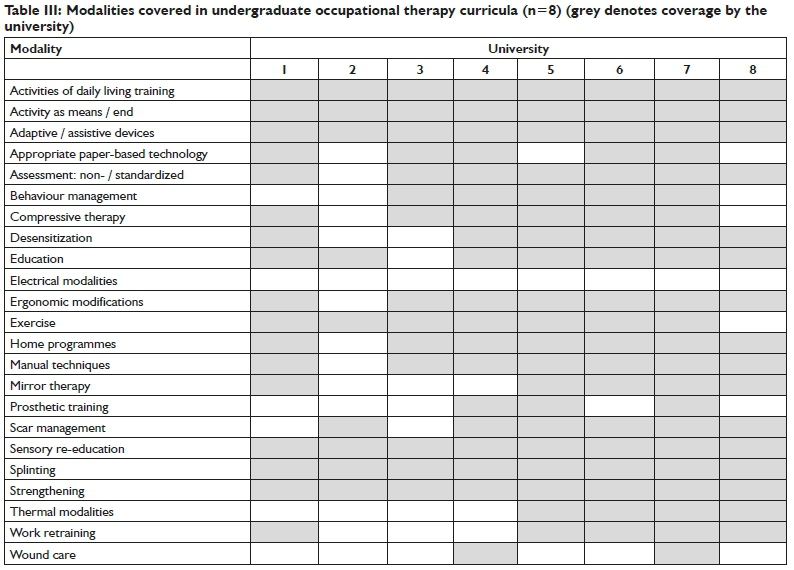
Activities of daily living training, activity as means/end, adaptive/ assistive devices, sensory re-education, splinting, and strengthening were taught at all universities (see Table III on page 7 for the modalities included in the different curricula).
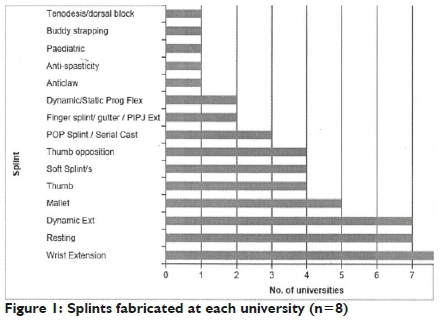
Universities covered a range of splints with almost all teaching their students to fabricate wrist extension (n=8), resting (n = 7) and dynamic extension (n = 7) splints. Refer to Figure 1 for splints fabricated by university.
The results reflect a wide variation in hand curricula across the different universities.
DISCUSSION AND IMPLICATIONS
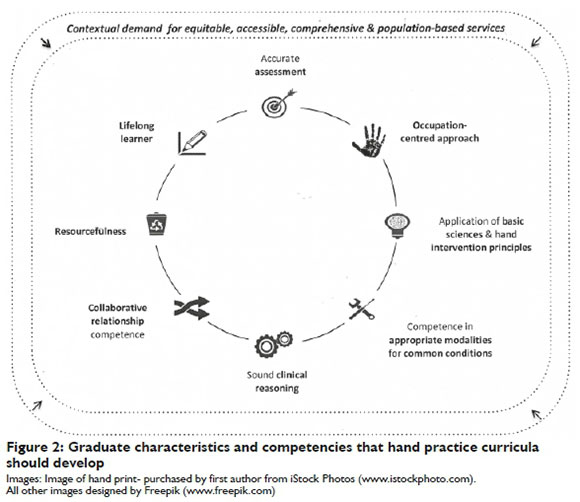
The study set out to describe the content of hand curricula delivered in undergraduate occupational therapy programmes in South Africa. This section begins by considering key contextual drivers that should guide hand curricula in order to respond to the needs of the population. The results of the study are then discussed in relation to international (WFOT) and national (HPCSA) minimum standards for the education of occupational therapists and other relevant literature. Recommendations for comprehensive hand curricula for undergraduate occupational therapy programmes are provided in each section of the discussion as illustrated in Figure 2 on page 8.
Contextual drivers
Policy1 and planning2 demand that comprehensive hand interventions are both equitable and accessible. International educational guidelines include equitable access to services as a core curriculum principle across all areas of occupational therapy practice25. South African educators need to be cognisant of the skewing of current hand services towards the private sector in urban centres15 and be willing to position curricula to equip graduates to deliver and develop services in rural and underserved areas. This would encompass equipping students with the competencies and characteristics required for working in such contexts37. Graduates should be equipped to factor accessibility barriers, such as remote locations, influence of weather, distance to facilities, cost of transportation and various system limitations38 into their interventions. Policy1,2 along with local26 and international educational guidelines25 speak to the development of hand services that are comprehensive. Graduates thus need to be able to use prevention, promotion, curative and rehabilitative approaches to address the hand health needs of individuals, groups and communities. This would require graduates to be able to identify the social and occupational determinants of compromised hand health and be able to adopt a population-based approach to hand interventionl,25. Furthermore, an occupational view would require a shift in emphasis to the implications of hand impairment on human doing, being and becoming in context39.
Characteristics and competencies that occupational therapy hand curricula should develop
In addition to being responsive to contextual imperatives, key graduate competencies and characteristics that were evident in educators' responses are discussed with reference to the literature.
Accurate assessment
Educators believed assessment to be the most important aspect of a hand-care curriculum. This perception is shared by American hand therapists who rate assessment as being 'highly critical' to hand rehabilitation practice32. For the focus of intervention and modality choice to be appropriate, thorough assessment to discern the nature and underlying causes of clients' problems is required. Accurate assessment will enable novice graduates to understand the problems with which clients are presenting and suggest a point of departure for treatment. Accurate assessment also enables graduates to measure the success of interventions40 and will assist them in seeking support from colleagues or mentors with experience, as guidance for treatment planning and implementation can be provided if accurate assessment findings have been communicated.
Although educators considered assessment to be important, assessments taught within hand curricula were largely restricted to biomedical performance components, which has been reported as a concern by other authors19,41. Only two educators made reference to the assessment of occupational performance and one prioritised contextual and occupational considerations in assessment. This is not surprising as the return to an occupation-based, or an occupation-centred approach to hand practice is a relatively recent trend in the literature, and its implementation in South Africa is perceived as challenging19. Given the nature of hand practice, performance component assessment is essential, but may be insufficient. Hand intervention that focuses exclusively on performance components or body structures and functions, suggests a belief that these factors alone affect participation, potentially disregarding clients' occupational needs and goals, their readiness to participate in intervention and various personal and environmental factors25. This focus also runs the risk of shifting therapy away from collaborative practice where therapist and client co-author the process, as knowledge of body structures and function often lie with the therapist.
Occupation-centred approach
In describing an occupation-focused approach to practice, international education guidelines state that curricula should "go beyond education on bodily dysfunction"25:ll and advance participation by considering the occupational and social determinants of health25. A robust discussion on what constitutes occupation-centred or occupation-based hand practice is beyond the scope of this article but it suffices to acknowledge that the purpose of South African occupational therapy curricula is to qualify occupational therapists with a comprehensive understanding of the relationship between occupational engagement and health, and the impact of the environment on this relationship26. This necessitates an understanding of clients with hand intervention needs as occupational beings, a feature that has been described as essential to occupation-centred curricula42. Despite hand therapy practice often being situated within the biomedical model43, the American Society of Hand Therapists acknowledge the importance of function or participation in daily occupations as a key aspect of assessment44. Since the ultimate goal of occupational therapy in hand practice is occupational participation, an occupation-centred approach needs to define both assessment and intervention. Intervention should be directed at the person (group, community or population), the occupation and the environment with activity constituting the primary mode of intervention25.
Application of basic sciences and hand intervention principles
The holistic focus on occupational participation in occupation-centred hand intervention does not minimise the need to manage disruption to body structures and functions25 through the application of sound scientific and hand intervention principles - an aspect of curriculum prioritised by a number of participating educators. Core content of occupational therapy curricula described by the HPCSA includes knowledge of anatomy, physiology, human movement and clinical sciences26. Graduates' integration and application of basic sciences and hand intervention principles is thus an essential component of hand practice.
Competence in appropriate modalities for common conditions
Half the educators felt that the basic treatment of conditions is a curricular priority. Conditions covered appear to largely correlate with those that therapists have reported to treat frequently8-9,19-20 although the incidence of complex and cumulative trauma may suggest that these should be covered by all universities8-9. Some conditions (e.g. nail bed injuries) could arguably be omitted due to them being treated very rarely by novice therapists. Frequent modality use reported by graduates8 correlates largely to modalities taught. This could be a response to contextual need or may be linked to graduates having been prepared to use them. Reported modality use may suggest that home programmes, education and manual therapy should be taught in all curricula. Two educators felt that splinting was a curricular priority, although the relative infrequent use of splinting by South African graduates8 may challenge how educators include the learning of this skill in curricula. Low-cost splinting approaches are vital and the realities of working in rural and underserved contexts may justify a shift from a focus on splinting itself, to the development of the skill within a sound clinical reasoning approach that is directed by an understanding of clients as occupational beings. The philosophy of the profession prescribes that contextually appropriate activity and occupation remain the primary mode of intervention26 and contextual resources (e.g. absence/relative absence of surgical services; absence of thermoplastic material) and realities (clients travelling long distances to therapy and attending infrequently) be considered in selecting the modalities that are included in curricula. Competence in appropriate modalities for common conditions should thus also be considered a key aspect of undergraduate curriculum.
Sound clinical reasoning
While 25% of the educators felt that curricula should cover treatment protocols, it is important to note that these may restrict some aspects of practice45, and in South Africa factors beyond the protocol implementation appear to affect treatment outcomes28. Key principles of hand practice are embedded within protocols and may provide critical guidance for graduates with limited experience. However, a multitude of contextual factors (for example absence of hand surgery, late presentation of injuries, complex injuries to multiple structures, infrequent appointments, or role- demands of the client) may also limit the applicability or ease of application of protocols by South African graduates. Sound clinical reasoning, prioritised by two educators participating in the study, may be the key to allowing graduates to apply their undergraduate knowledge to diverse client presentations, drawing from the principles contained in protocols. Graduates with "enhanced clinical reasoning skills" are listed as an essential outcome of curricula in the international minimum standards (extracted from the World Health Organizations Report on increasing the Relevance of Education for Health Professionals, 1993)25. Local standards echo this priority in describing graduates who should be able to "interpret complex, unfamiliar and ill-defined situations" and respond creatively to them2610. Developing sound clinical reasoning ability around hand interventions should enable graduates to navigate the complexities of their clients, their environments and their occupations and to provide appropriate intervention. Sound clinical reasoning will enable graduates to cope with unusual or unfamiliar presentations and to consult evidence. It will also prompt them to seek support from supervisors and mentors when necessary and assist them in pursuing best practice - two further curricula priorities educators' highlighted.
Collaborative relationship competence
Only one educator felt that "understanding the client within their context" was a priority in hand curricula, echoing a recommendation from an Australian study that described therapists' appreciation of context in enhancing collaboration and effective communication with clients46. The WFOT MSEOTs speak extensively to the concept of 'contextual responsiveness' which involves understanding clients as occupational beings (individuals, groups or communities) within their local context and encompasses appreciating multiple contextual and environmental factors affecting clients' health needs, and health and social systems. Culture is emphasised as it "influences beliefs about the relative importance of various health conditions or threats to health and well-being, as well as perceptions about whether occupational therapy will be helpfu ... Cultural beliefs influence local understandings about the relationships between occupation, health conditions and physical, mental, social and spiritual well-being, and therefore influence what occupations are perceived as harmful or helping people."25:22.
Applying an understanding of clients in their own contexts to intervention plans requires essential soft skills described in the WFOT MSEOTs and include interpersonal relationships, affective sensitivity, communication and political awareness, people-centeredness and collaboration, treating people with respect and building trust, listening actively, communicating effectively, demonstrating cultural sensitivity and determining client readiness for occupational therapy25,47. Many of these features resonate with the experiences of new graduates in South Africa who reported the extensive impact of communication difficulties on the quality of hand interventions and the importance of cultural competence9. It is thus imperative that hand curricula do not neglect developing collaborative relationship competence in graduates.
Resourcefulness
Two educators felt that one of the most important aspects of hand curricula was equipping graduates to work with limited resources. Resourcefulness, defined as "creativity in the construction or conceptualisation of practical solutions", is described as a required professional behaviour of South African graduates in the HPCSA minimum standards26:10. Resourcefulness is arguably an essential skill in the delivery of hand intervention given that 73% of a sample of CS occupational therapists lacked the necessary equipment to treat hand impairments, that hand-injured clients may present late when surgical intervention is no longer possible, and that various other human and non-human resource limitations impact on practice8.
Life-long learning
One educator felt that learning "specialised techniques" for hand intervention was very important. As developing specialised skills requires time, this aspiration is unrealistic at undergraduate level. It does, however, highlight the need to delineate between undergraduate and postgraduate competencies required for hand interventions with due consideration of what context demands of novice therapists in South Africa, the clinical reasoning capacity of undergraduates, and curricular resources (for example, time and practice learning opportunities). Accepting the responsibility for life-long learning is one of the fundamental characteristics of the South African minimum standards for graduating occupational therapists26 and is thus also a graduate characteristic essential for ensuring competence in delivering appropriate hand services. Two educators reported focusing on the importance of life-long learning in order to develop evidence-based practices in their students. How life-long learners are developed warrants more extensive discussion than can be provided in this article, but strategies may include educators modeling themselves as continual learners, students being required to take responsibility for their own learning, communicating the value of acquiring mentors, and pursuing continuous professional development opportunities.
A further aspect that may drive life-long learning is enjoying the area of practice. Enjoying hand practice emerged as a significant factor in the broader study8-9, within which this project was situated. A statistically significant association between the university from which a therapist had graduated and whether they felt equipped to treat some hand conditions and use some modalities was noted. These associations could not, however, merely be explained by whether or not the condition or modality was covered in a curriculum or by the number of teaching hours. To develop a profile of a prepared graduate, 25 factors were analysed against competence and confidence, and those with a significant univariate association were included in a logistic regression. Perceived competence, enjoying treating hand clients and having an undergraduate hand fieldwork placement were most significantly associated with competence. Similarly, therapists who reported feeling confident, were more likely to report having adequate skills, enjoying hand practice and having had a hand fieldwork placement. A majority (80.2%) of these therapists also perceived that an improved practical component in undergraduate hand curricula was necessary. Further exploration into how hand practice learning opportunities can creatively be incorporated into curricula and how an enjoyment of hand practice can be fostered is thus required.
This study is the first to report on undergraduate hand curricula offered within South African occupational therapy programmes. It is acknowledged as a limitation that the research instrument was built on a limited review of the literature and underwent limited piloting. Furthermore, the questionnaire may have under-captured latent curricular content impacting on hand curricula, and changes to curricula may have occurred since data collection. The questionnaire focused more intensively on the rehabilitative aspects of practice and may thus have substantially under-captured prevention and promotion approaches within curricula.
CONCLUSION
In a poverty-burdened context, promotion of hand health, prevention of impairment and rehabilitation after hand injury is critical, as is the maintenance of occupational well-being. Appropriate preparation of therapists for this task is important. The mandate of undergraduate hand curricula is not to produce specialised hand therapists, but rather therapists who are able to intervene with people whose occupational health or well-being is being compromised, or is at risk of being compromised by a hand impairment. Graduates need to be able to follow the occupational therapy process with clients with, or at risk of developing, hand impairments. Curricula need to be shaped by local policy and local and international minimum standards of education in order to be responsive to the hand health needs of the population. Various competencies and characteristics are proposed as curricula priorities in order to develop graduates that are able to contribute to the vision of hand health for all.
Ethics Clearance
University of Cape Town Faculty of Health Sciences Human Research Ethics Committee (HREC REF: 551/2013)
1. Funding statement
Funding for this study was obtained through the KW Johnstone Award, the University Research Committee, University of Cape Town, and the Faculty of Health Sciences Postgraduate Publication Incentive Fund, University of Cape Town.
2. Acknowledgements
The occupational therapists who participated in the pilot process and the study participants and their respective universities are sincerely thanked for participating.
REFERENCES
1. National Planning Commission. National Development Plan 2030. Our future - make it work. 2012. Executive summary. The Presidency, Republic of South Africa. <https://www.gov.za/sites/default/files/Executive%20Summary-NDP%202030%20-%20Our%20future%20-%20make%20it%20work.pdf> (13 March 2018) [ Links ]
2. Department of Health Republic of South Africa (2017). National health insurance for South Africa. Towards universal health coverage. [ Links ]
3. Reid SJ, Couper ID, Volmink J. Educational factors that influence the urban-rural distribution of health professionals in South Africa: a case-control study. S Afr Med J [Internet], 20ll;l0l(l):29-33. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21626978 [ Links ]
4. Reid SJ. Rural health and transformation in South Africa. S Afr Med J [Internet], 2006; 96(8):676-7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21721301 [ Links ]
5. Wilson NW, Couper ID, De Vries E, Reid S, Fish T, Marais BJ. A critical review of interventions to redress the inequitable distribution of healthcare professionals to rural and remote areas. Rural Remote Health [Internet], 2009; 9(2):l-2l. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19530891 [ Links ]
6. Burch V, Reid S. Fit for purpose? The appropriate education of health professionals in South Africa. S Afr Med J [Internet], 2011; 101(1):25-6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/21626976 [ Links ]
7. Pillay M, Kathard H. Decolonizing health professionals' education: audiology and speech therapy in South Africa. African J Rhetor, 2015;7:193-227. [ Links ]
8. Van Stormbroek K, Buchanan H. Novice therapists in a developing context: Extending the reach of hand rehabilitation. Br J Hand Ther, 2017; 22(4): 141-152. [ Links ]
9. van Stormbroek K. The extent which Community Service occupational therapists are equipped to treat patients with upper limb injuries and conditions [Internet]. The University of Cape Town; 2015. Available from: https://open.uct.ac.za/handle/11427/13807 [ Links ]
10. Dias JJ, Garcia-Elias M. Hand injury costs. Injury [Internet], 2006; 37(11):1071-7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/17045996 [ Links ]
11. Norman R Matzopoulos R, Bradshaw D. The high burden of injuries in South Africa. Bulletin of the World Health Organisation, 2007; 85:695-702. Available at: https://www.scielosp.org/pdf/bwho/2007.v85n9/695-702/en [ Links ]
12. Schultz G, Mostert K, Rothmann I. Repetitive strain injury among South African employees: The relationship with burnout and work engagement. Int J Ind Ergon [Internet], 20l2; 42(5):449-56. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0169814112000613 [ Links ]
13. Industrial Health Resource Group. Organising for Health and Safety. A guide for trade unions. 2nd ed: Section 8 Compensation for injured or ill workers [Internet]. 2011. Available from: http://www.ihrg.org.za/oid/downloads/4/10_8_6_47_31_AM_Section08-Compensation(Final).pdf [ Links ]
14. Jeebhay M, Jacobs B. Occupational health services in South Africa. South African Health Review [Internet], 1999;29(19):257-76. Available from: ftp://apollo.hst.org.za/pubs/sahr/l999/chapterl9.pdf [ Links ]
15. van Stormbroek K. Hand-care for all: towards strategic conversations. In: South African Society of Surgery for the Hand 46th Congress. Drakensburg; 2015. [ Links ]
16. SASSH. South African Society of Surgery to the Hand [Internet]. 2014 [cited 20l6 Nov 7]. Available from: http://www.sassh.co.za/ [ Links ]
17. SASHT. South African Society of Hand Therapists [Internet]. 2014 [cited 2016 Nov 7]. Available from: www.sasht.org.za [ Links ]
18. STATSSA. Statistics South Africa [Internet]. 2014. Available from: http://beta2.statssa.gov.za/?s=GHS&sitem=publications [ Links ]
19. De Klerk S. Occupational Therapy Assessment of the Upper Limb : Trends in South Africa. Stellenbosch University; 20l4. [ Links ]
20. Pietrobon C. Hand Therapy Trends in a Changing South Africa. J Hand Ther [Internet], 1996; 9(4):299-302. Available from: http://linkinghub.elsevier.com/retrieve/pii/S0894113096800330 [ Links ]
21. American Society of Surgery of the Hand (ASSH).Hand therapy. [Cited 2017 Apr 25] Available from: http://assh.org/handcare/What-is-a-Hand-Therapist [ Links ]
22. Fitzpatrick N. Through The Maze : The Development of a Learning Pathway Through a Six-Month Hand Therapy Rotation. Br J Hand Ther, 2006;11(2):36-40. [ Links ]
23. Van Stormbroek K, Buchanan H. Community service occupational therapists: thriving or just surviving? S Afr J Occ Ther [Internet], 20l6; 46(3): 63-72. Available at: http://www.scielo.org.za/pdf/sajot/v46n3/11.pdf [ Links ]
24. Robinson LS, Brown T, O'Brien L. Embracing an occupational perspective: occupation-based interventions in hand therapy practice. Aust Occup Ther J [Internet]. 2016; 63(4): 293-296. Available at: https://onlinelibrary.wiley.com/doi/pdf/10.1111/1440-1630.12268 [ Links ]
25. World Federation of Occupational Therapists. Minimum Standards for the Education of Occupational Therapists Revised 2016. World Federation of Occupational Therapists. [ Links ]
26. Health Professions Council of South Africa. The Minimum Standards for the Training of Occupational Therapists. 2009. [ Links ]
27. National Department of Health (NDOH), Republic of South Africa. White Paper for the transformation of the health system in South Africa. 1997. <http://www.info.gov.za/whitepapers/l997/health.htm> (13 March 2018) [ Links ]
28. Wentzel R, van Velze C, Rudman E. Comparison of the Outcomes of 2 Rehabilitation Protocols After Flexor Tendon Repair of the Hand at Chris Hani Baragwanath Academic Hospital, Johannesburg, South Africa. Hand. 2016;11(1 suppl):139S-139S. [ Links ]
29. Spark T, Ntsiea V Godlana L. The Impairments and Functional Outcomes of Patients Post Flexor Tendon Repair of the Hand. Hand. 2016;11(1 Suppl):141S-141S. [ Links ]
30. Fluidsurveys. Online and Mobile Surveys. [Cited 20I4 Nov 19] Available from: www.fluidsurveys.com. [ Links ]
31. IBM. SPSS Statistics. [Cited 20I8 Jul 30]. Available from: www.ibm.com/software/products/en/spss-statisticsIBM. SPSS Statistics, IBM. 2016. [ Links ]
32. Muenzen PM, Kasch MC, Greenberg S, Fullenwider L, Taylor PA, Dimick MP? A new practice analysis of hand therapy. J Hand Ther [Internet]. 2002;15(3):215-25. Available from: http://www.ncbi.nlm.nih.gov/pubmed/12206324 [ Links ]
33. Brown GT, Brown A, Roever C. A review of paediatric occupational therapy curricula in South Africa : Part two. Int J Ther Rehabil. 2006;13(4):151-8. [ Links ]
34. Lloyd C, King R, Ryan L. The Challenge of Working in Mental Health Settings: Perceptions of Newly Graduated. 2007;70(Octo-ber):460-70. [ Links ]
35. MacDermid JC. An introduction to evidence-based practice for hand therapists. J Hand Ther [Internet]. 2004 [cited 2014 Jul 23];17(2):105-17. Available from: http://www.ncbi.nlm.nih.gov/pubmed/15162099 [ Links ]
36. Nayar S, Gray M, Blijlevens H. The competency of New Zealand new graduate occupational therapists: perceived strengths and weaknesses. Aust Occup Ther J [Internet]. 2013 Jun [cited 2014 Jan 22];60(3):189-96. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23730784 [ Links ]
37. Strasser, R., Couper, I., Wynn-Jones, J., Rourke, J., Chater, A. B., & Reid, S. Education for rural practice in rural practice. Education for Primary Care, 20I6; 27(1), 10-14. [ Links ]
38. Sherry K. Disability and rehabilitation: essential considerations for equitable, accessible and poverty-reducing health care in South Africa. South African Heal Rev 2014/2015 [Internet]. 2015;89-100. Available from: http://www.hst.org.za/sites/default/files/7_Disability.pdf [ Links ]
39. Wilcock AA. Reflections on doing, being and becoming. Aust Occup Ther J [Internet], 1999; 46:I-II. Available at: https://onlinelibrary.wiley.com/doi/epdf/10.1046/j.1440-1630.1999.00174.x [ Links ]
40. Law M. Measurement in occupational therapy: Scientific criteria for evaluation. Can J Occup Ther, 1987; 54(3):133-8. [ Links ]
41. Grice KO. The Use of Occupation-based Assessments and Intervention in the Hand Therapy Setting - A Survey. J Hand Ther [Internet]. 2015; 28(3):300-6. Available at: https://ac.els-cdn.com/S089411301500023X/1-s2.0-S089411301500023X-main.pdf?_tid=6a6580c0-c85e-496e-9427-aI9a245f55f5&acdnat=1533646521_2c60990a048f77deed20c2da65efb0f9 [ Links ]
42. Whiteford GE, Wilcock AA. Centralizing occupation in occupational therapy curricula: imperative of the new millenium. Occup Ther Int. 2001; 8(2):81-5. [ Links ]
43. Fitzpatrick N, Presnell S. Can occupational therapists be hand therapists? Br J Occup Ther. 2004;67(11):508-10. [ Links ]
44. The American Society of Hand Therapists. Clinical Assessment Recommendations [Internet]. [cited 20I8 Feb 2I]. Available from: https://www.asht.org/practice/clinical-assessment-recommendations. [ Links ]
45. Colaianni D, Provident I. The Benefits of and Challenges to the Use of Occupation in Hand Therapy. Occup Ther Heal Care [Internet]. 20I0;24(2):I30-46. Available at: https://www.tandfonline.com/doi/pdf/10.3109/07380570903349378?needAccess=true [ Links ]
46. Kingston GA, Judd J, Gray MA. The experience of medical and rehabilitation intervention for traumatic hand injuries in rural and remote North Queensland: a qualitative study. Disabil Rehabil. 2015;37(5):423-9. [ Links ]
47. Fortune T, Ryan S, Adamson L. Transition to practice in supercomplex environments: are occupational therapy graduates adequately prepared? Aust Occup Ther J [Internet]. 2013 Jun [cited 2014 Jan 22];60(3):217-20. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23730787 [ Links ]
 Correspondence:
Correspondence:
Kirsty van Stormbroek
kirsty.vanstormbroek@wits.ac.za
a Hand rehabilitation refers to occupational therapy intervention for individuals, groups or communities with injuries or conditions affecting the Within hand therapy/rehabilitation, the upper quarter refers to the entire shoulder girdle and upper limb. For the purposes of this article, hand rehabilitation is preferred over hand therapy, which may suggest a postgraduate qualification.
b The term hand health is used in this article to indicate a comprehensive approach to health service provision and a specific shift in emphasis to include promotion and prevention, in line with a PHC approach.
c This could be related to upper or lower motor neuron lesions.


{kind=link}
{kind=link}
{kind=link}