










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.46 n.3 Pretoria Dec. 2016
http://dx.doi.org/10.17159/2310-3833/2016/v46n3a8
SCIENTIFIC ARTICLES
The development of an emotional regulation scale for adolescents***
Monique StraussI; Jacques E RaubenheimerII; Daleen CampherIII; Charika CoetzeeIII; Amorise DiedericksIII; Heidi GeversIII; Karla GreenIII; Sandré van NiekerkIII
IBOT (UFS), MOT (UFS). Junior Lecturer Occupational Therapy, Faculty of Health Sciences, University of the Free State
IIBA (UFS), BA Hons (Psychology) (UFS), B.Th (UFS), M.Th. (Practical Theology) (UP), M.A. (Reseach Psychology) (UFS), PhD (Research Psychology) (UFS). Lecturer Biostatistics, Faculty of Health Sciences, University of the Free State
IIIBOT (UFS). Students in the Department of Occupational Therapy at the University of the Free State at the time the study was conducted
ABSTRACT
Emotional regulation is an important skill enabling or disabling the occupational engagement of adolescent clients. Evaluation is a key concept in the occupational therapy process, informing treatment approaches and outcomes. The authors could not identify a scale measuring emotional regulation strategies used by adolescent in the literature. A quantitative, descriptive study was done following a process of scale development. A survey with 78 items was designed which 404 adolescents from a tertiary institution completed. From the results, a provisional scale was developed, measuring emotional regulation strategies used by adolescents. The scale has 39 items, consisting of five emotional regulation strategy categories, named Comfort and Sharing, Antisocial behaviour, Creative Activities, Physical Activities and Eating. A confirmatory factor analysis (CFA) model proved the provisional scale, as well as the items, to be reliable. Further research for the development and the refinement of this scale is recommended. The use of an emotional regulation scale could assist the occupational therapist in understanding the adolescent client's emotional regulation strategies or lack thereof.
Emotional regulation skills can either support or hinder a person's wellbeing and are influenced by the emotions experienced, as well as the individual's preference. Key challenges involved in regulating emotions are to choose which emotional regulation strategy to use, when to use it and how to implement it7,8.
Key words: Emotional regulation, Adolescents, Structural Equation Modelling
INTRODUCTION
The mental health of adolescents is a key concern. According to the World Health Organisation (WHO), 20% of children and adolescents worldwide suffer from disabling mental illnesses1. A report compiled by the WHO in 2014, states that self-harm is the third leading cause of death amongst children and adolescents worldwide. This cry for help is also reflected by a statistic from the same report which states that unipolar depressive disorders are the leading cause of disability-adjusted life years (DALY) amongst this population, ahead of HIV/AIDS and road accidents2. Adolescents have always been perceived as a highly stressed and confused group as they face challenges due to the physical, cognitive and social transitions in their development during this stage of life3. In the light of the prevalence of mental disorders in adolescents concerns regarding adolescent health, is crucial. If poor mental health of adolescents is left unmanaged, this will have an even greater impact on their lives as adults, as well as on the community.
A key concept in an adolescents' mental health and interpersonal relationships is the ability to regulate their emotions4. Emotional regulation skills describe the manner in which a person identifies, manages and expresses feelings whilst interacting with persons, situations or activities5. Adequate emotional regulation skills promote life skills and wellbeing in adolescents. In this study, an emotional regulation strategy specifically refers to the regulatory process and action that follows an activated emotional state6. An example of this could be the strategy of abusing substances, in an attempt to regulate anxiety.
Emotional dysregulation occurs when the adolescent is unable to effectively use strategies to regulate intense or overwhelming emotions experienced9 and as a result, has implications for mental health including prolonged mental illness, risky behaviour, admittance of adolescents into mental health facilities and suicide10,11. Emotional dysregulation also has a direct effect on occupational performance and could lead to occupational dysfunction5. For example, an ineffective strategy like substance abuse could have a negative impact on occupational performance areas like sleep and social participation.
The WHO Assessment Instrument for Mental health Systems (WHO-AIMS) report12 highlights strategies that can be meaningfully employed to improve mental health in South Africa. One of these strategies is to develop clinical protocols for the assessment of and intervention in Primary Health Care. Occupational Therapists deal with adolescents with mental health problems in a variety of health care settings13. The planning of such intervention is directed by the adolescents' goals and occupational needs; the adolescents' health and well-being; their performance skills and patterns; as well as the collective influence of the context, environment and client factors which affect the adolescents' life situations and intervention programs5. The occupational therapist focuses on lifestyle issues of the adolescent, which includes mental health concerns, in an attempt to ensure optimal functioning in the context of the everyday life of the adolescent, enabling the client to engage in meaningful occupation13. As previously indicated, the implementation of ineffective emotional regulation strategies could inhibit engagement in occupation14. This, together with the consideration that adolescence is characterised by fluctuating emotional states3 makes it necessary for the occupational therapist to identify effective and ineffective emotional regulation strategies used by the client, in order to understand the impact thereof on occupation and to ensure adequate, client-centered mental health care.
The questions that arise from this are: How can one measure an adolescent's ability to regulate his or her emotions and how can one identify emotional dysregulation? When investigating the literature it was found that limited literature exists on ways to measure emotional regulation strategies in adolescents and no suitable measurement tool could be found by the researchers.
This article will explore literature on emotional regulation in adolescents and describe the process of developing a scale for measuring the emotional regulation strategies used by South African adolescents.
LITERATURE REVIEW
On a micro level occupational therapists deal with adolescents with mental health problems on an individual out-patient level, in mental health care facilities, as well as in the community where the occupational therapist is part of the multi-disciplinary team involved in treating adolescents15. The focus of occupational therapy in these facilities is to assist adolescents with personal growth which may lead to improvement of their self-esteem, independent communication as well as social skills and eventually, meaningful community engagement. When engaging with an adolescent-client on any level, an evaluation is needed to determine the client's problems, strengths and therapeutic needs in order to provide a client-centred occupational therapy intervention. Within the evaluation process, occupational therapists employ assessment tools with the aim to observe, measure, and enquire about factors that support or hinder occupational performance in the adolescent13. The active involvement of the adolescent in prioritising goals and needs, facilitates the engagement of the client in the treatment process16.
The adolescent period (10 to 19 years2) is a developmental stage filled with emotional regulation challenges. Major developmental changes like the development of a sense of mastery, identity and intimacy occur during this confusing period. The challenges associated with these changes include: Shifts in relationships between adolescents and their parents, where the adolescents move from dependency to more mature and responsible positions in the family; exploration of new sexual and social roles; experiences of intimate relationships; identity formation on a personal and social level; planning the future and taking the steps to pursue those plans and acquiring the necessary skills and values to transition into adulthood. Successful management of all these challenges depends on the adolescents' psychological, physical and cognitive skills as well as their social support and the setting in which they can explore these challenges. These skills include confidence in one's ability, desires to engage in important activities, being socially connected, engaging in supportive organisations, and especially, having the ability to control and regulate ones emotions17. However, many adolescents have not been given the opportunity to acquire these skills or are severely influenced by their environment, and therefore struggle to overcome these challenges1.
Within the emerging field of emotional regulation research, one finds a variety of definitions of emotional regulation. Cole, Martin and Dennis6 ascribe this firstly to a historical difficulty to define "emotion" and secondly to the fact that emotions have the ability to "regulate" as well as to "be regulated". In this study the focus is on the emotion, i.e. the activated emotional state, as well as the regulatory process that follows the emotion, i.e. the emotional regulation strategy6. Within the Occupational Therapy Practice Framework, emotional regulation is categorised within the performance skills domain. Emotional regulation is defined as the manner in which a person identifies, manages and expresses feelings whilst interacting with persons or situations5. The value of emotional regulation, as a skill, is to facilitate powerful actions in order to overcome obstacles, solve problems and maintain well-being. An emotional regulation strategy refers to the specific action chosen to regulate a specific emotional state6.
Strategies like distraction; suppression; venting; cognitive reappraisal; downward social comparison; problem-directed action; self-reward; physical manipulations and withdrawal are linked to negative emotions. Strategies employed during positive affect include: gratitude; helping others; and expressing positive emotions in a variety of ways, e.g. creative expression. However, there are uncertainties with regard to what to measure about emotional regulation and how it can be measuredl8. Some measurement tools already exist to measure components of emotional regulation, e.g. the 'Difficulties in Emotion Regulation Scale' (DERS) of Weinberg and Klonsky11. This scale focuses on the awareness, understanding and acceptance of emotions and responding in a desired manner, but does not identify specific strategies used. Another related measurement tool is the "Adolescent Coping Orientation for Problem Experiences" (A-COPE)8 which focuses on the coping strategies that adolescents use when confronted with a difficult situation, but due to the date of publication, excludes the possibility of strategies linked to current technology like social media. Furthermore, these measurement tools are not designed to link those strategies used to regulate either positive or negative emotions, do not include strategies indicating self-harm and are not standardised for use on the South African population. Therefore the need to develop a scale to measure emotional regulations strategies used by South African adolescents became clear.
METHOD
A quantitative descriptive study was done by a group of fourth year occupational therapy student researchers, with the purpose of developing a scale which will describe the strategies used by adolescents in regulating their emotions.
The objectives formulated for this study were to: Investigate literature on emotional regulation in adolescence in order to discover strategies to use as questions in a survey; compile the survey and administer it to a selected adolescent population; and then to validate the designed scale as a measurement tool which measures adolescents' tendency toward strategies employed to regulate their emotions.
After an extensive literature review on the various strategies for emotional regulation, the researchers compiled a list of possible items coupling certain strategies for emotional regulation with plausible triggering emotions. This list was then reviewed by the researchers, and the items were whittled down through a process of literature matching, until a final list of 78 items was retained. These 78 items were compiled into a four-item Likert scale (l-Never, 2-Seldom, 3-Often and 4-Always). All of the items included an identified emotion (activated emotional state) linked to a regulatory process (emotional regulation strategy), e.g. 'When I am angry, I express it on social media'. Demographic items recorded age, gender, language, and whether respondents owned cell phones. Three broad emotional background items recorded whether respondents were experiencing emotional problems or not (with examples), whether they thought their home life happy or not, and whether they considered themselves as being introverted or extroverted.
The questionnaire contained two further open-ended questions, asking respondents to list 5 strategies they used when experiencing pleasant or unpleasant emotions. The results obtained from the open-ended section will be used for further refinement of the scale and will not be reported on in the results section of this article.
The population of the study included adolescent students of all races and both genders, between the ages of 18 and 19 years, enrolled across all three campuses at the University of the Free State (UFS). Convenience sampling was used by making use of the university's online teaching platform, Blackboard. All enrolled students use Blackboard on a regular basis and this was therefore a platform which gave easy access to the students.
The full questionnaire was then set up on Survey Monkey (www. surveymonkey.com), and piloted on five Occupational Therapy students at the UFS who met all the inclusion criteria of the population. The pilot study participants' data were excluded from the main study. Given the rule of thumb of having five times the number of participants than items for factor analytic studies19, the aim was to obtain 400 participants for the main study.
The link to the questionnaire was posted on the university's Blackboard page by the Centre of Teaching and Learning for the students to complete, and was removed before examinations commenced. All students on the system were automatically notified about the study via e-mail. Once the link was opened by the student, information regarding the study was given and they were made aware that by completing the survey, they were consenting to their participation. The participants were informed that their information would remain anonymous and would be stored confidentially, and that they would receive no compensation for participation.
Ethical approval was obtained from the ethical committee of the Faculty of Health Sciences (ECUFS 16/2014), UFS; the dean of the Faculty of Health Sciences, the head of the School for Allied Health Sciences, the dean of Student Affairs, the vice-rector of Academics, and the Centre of Teaching and Learning. Participation by students was voluntary and they could withdraw from the study at any time.
Data obtained were analysed by the department of Biostatistics, UFS. After they were defined (see results), the aggregate scores for each subscale were transformed as follows: Since the Likert scale used values of 1 for Always, to 4 for Never, the scores were first reversed and then also decreased by 1 (i.e., 0 for Never and 3 for Always), so that higher scores indicated a stronger preference for a factor. Furthermore, to ease comparisons between subscales with varying numbers of items, an individual's score was determined as the mean for the factor items multiplied by 100 divided by 3, giving each factor a possible range of zero to one hundred. The reliability of the new scale was determined through the calculation of Cronbach's alpha coefficients. The component structure of the items in the scale was investigated using exploratory maximum likelihood factor analysis (with orthogonal rotation) through the examination of scree plots and factor loadings. The construct validity of the scale was tested via confirmatory factor analysis (CFA) and Student's t-tests were used. Data analyses were performed with SAS/STAT software, Version 12.3 of the SAS System for Windows (Copyright © 2012 SAS Institute Inc., Cary, NC, USA) and LISREL, version 8.54 (Scientific Software International, Chicago, IL, USA).
The use of these statistics during the scale development process is explained in detail in the results section.
RESULTS
Within a three-week period, 404 respondents (94 male, 310 female) completed the questionnaire, which allowed the researchers to obtain the targeted number of participants. The respondents, in keeping with the sampling guidelines, were 18 (n = 163) or 19 (n=24l) years old. Most of the respondents had cellphones (n = 369/9l.3%), just more than half identified themselves as extroverts (n=216/53.5%) rather than introverts (n=l88,46.5%), and most of the respondents reported that they felt they had come from happy homes (n=346/85.6%), although almost a third (n=133/32.9%) reported experiencing emotional problems, with depression (n = 39/9.7%), anger (n=13/3.2%) and anxiety (n=l0,2.5%) being the most common.
The scale development process entailed three phases. The first was to eliminate any items showing poor reliability. When the reliability of the 78 Likert scale items was tested, an exceptionally high overall Cronbach's alpha of .895 was obtained. Furthermore, when looking at the resulting reliability should any individual item be removed, it was found that no individual items showed indications of low reliability (the alpha for the remaining items ranged between .892 and .896). Consequently, no items were removed at this stage.
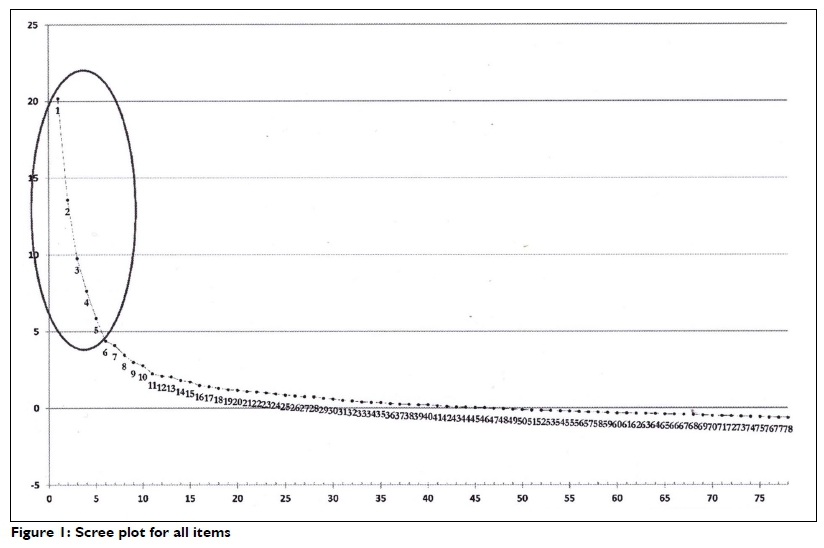
The second phase entailed determining the number of factors represented by the scale items. A scree plot (Figure 1 on the previous page) clearly indicated 5 factors.
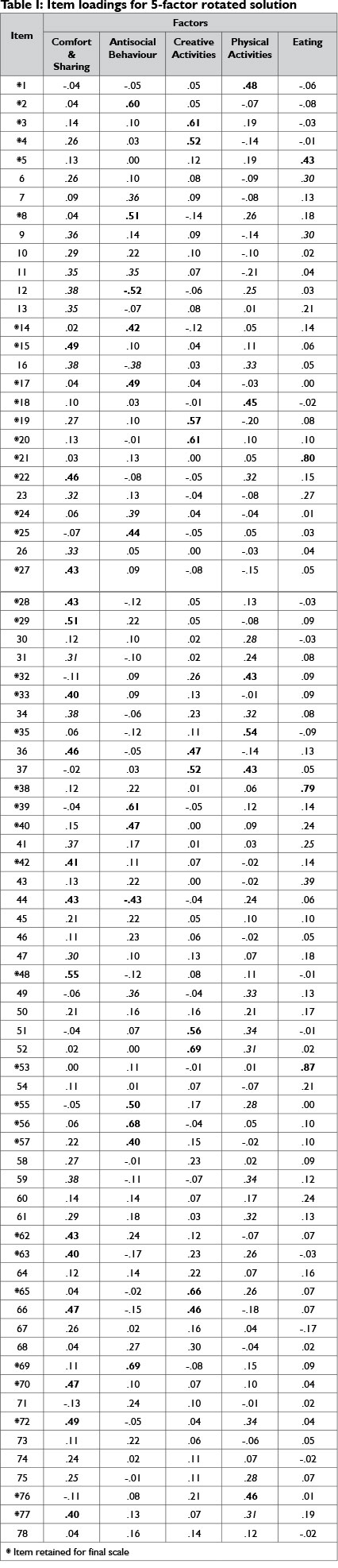
A maximum likelihood factor analysis with orthomax rotation was then performed, specifying the extraction of 5 factors. In order to satisfy the demands of convergent validity20, prominent loadings on a factor >|.40| were considered (this was relaxed slightly if the item loadings on all other factors were very low) and for divergent validity, items had to have low loadings on all four of the remaining factors <|.25| (this was again relaxed if the intended item loading was very high, and only one loading on another factor was slightly above the limit). Items were therefore retained if they showed high loadings on one factor, as well as low loadings on all other factors. The item loadings of the items on each of the factors are shown in Table I, with an indication of which items were retained. The five factors were named Comfort & Sharing, Antisocial Behaviour, Creative Activities, Physical Activities, and Eating. High loadings (i.e., close to or >|.40|) on an item's intended factor in Table I are marked in bold. Moderate-to-high loadings (i.e., >|.25|) on other factors are marked in italics. In total, 39 of the original 78 items were retained.
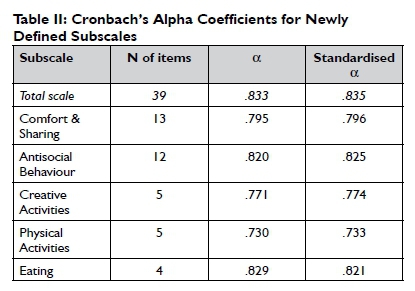
The items for each of the newly defined subscales were then averaged and transformed to give subscale scores ranging from 0 to 100. The reliabilities of the subscales are shown in Table II. Considering the small number of items in some of the subscales, the reliabilities were very high, with .73 for Physical Activities being the lowest.
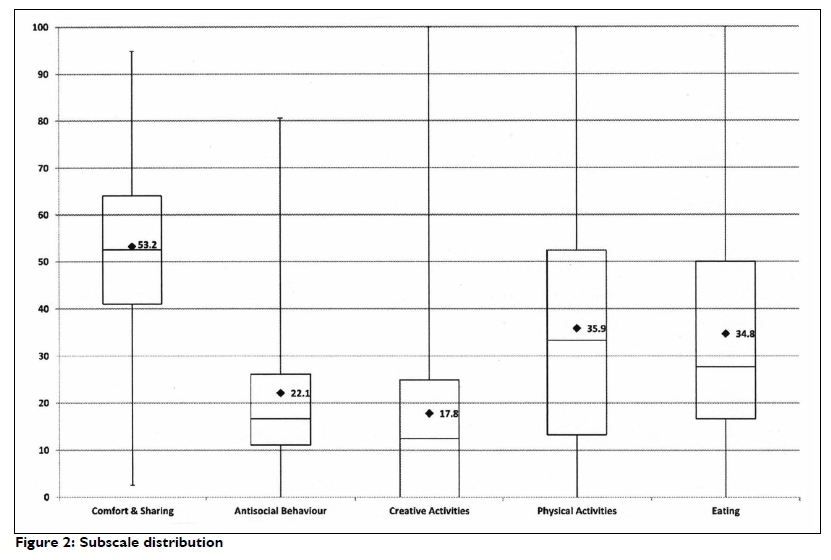
The distribution of the scores for the five subscales is shown in Figure 2. When considering the actual strategies, the distributions are quite understandable. Comfort and Sharing could be seen as a commonly used strategy, and so it was that the lower quartile for this subscale was 41.0, the highest of all the subscales, and close to, or higher than the upper quartile of all the others (the upper quartile for Physical Activities was 53.3, and for Eating, 50.0). Antisocial behaviour had the smallest range of all the subscales (IQR: II.I-30.6), and the second-lowest lowest mean (22.1) and median (19.4) values. The Creative Activities scores were also very low, with a lower quartile of 0, a mean of I7.8 and a median of 13.3.
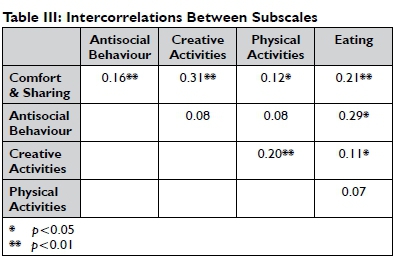
The intercorrelations between the various subscales are shown in Table III. Antisocial Behaviour did not correlate strongly with any of the other subscales, except for Eating. There was also no correlation between Physical Activities and Eating. While seven of the ten possible intercorrelations were statistically significant, none of them was so large as to be of concern for the issue of multi-collinearity. Despite there being some low correlations, there were no negative correlations.
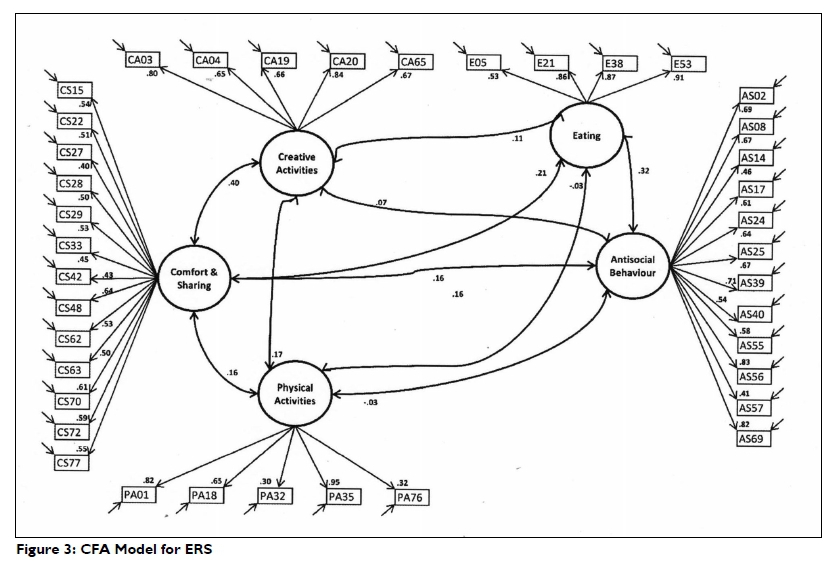
The item set and its proposed model were then tested with confirmatory factor analysis (CFA) performed with LISREL. The completely standardized solution is shown in Figure 3 on page 46.
The CFA model indicated good fit, with an RMSEA value of .059 (90% CI: .055-.062).
DISCUSSION
Results from the Cronbach alpha indicated that all 78 scale items (a statement consisting of an activated emotional state linked to an emotional regulation strategy) proved to be reliable. This indicated that all items developed, could be incorporated into the refined scale. A scree plot (Figure 1) indicated that five factors (emotional regulation strategies) should be extracted. The items which loaded under a particular category were examined and the category names (Comfort & Sharing, Anti-social Behaviour, Creative Activities, Physical Activities and Eating) were then derived from the wording and content of the questions.
When measuring the appropriateness of the categories against literature, they were all found to be relevant. Sharing and Comfort activities, including activities like sharing with a friend or engaging in a passive, comforting activity showed to be the highest preferred category. Methods included in the items ranged from traditional strategies like sharing with a friend, to making use of social media, linking to developmental theory stating that adolescents deem relationships with peers as most important3. Social media is an emerging platform for the sharing of emotion. De Choundry & Gamon21 wrote that one can predict emotional behaviour and even diagnose depression when analysing an adolescent's social media posts. In contrast, Valkenburg et al.22 stated that feedback received on a social media post (e.g. amount of "likes") could in return have a direct impact on an adolescent's emotions, indicating that this type of expression could act as an emotional regulation strategy, but could also impact emotions experienced. Other comfort-related activities, like television watching and music listening have also been linked to both positive, as well as negative emotional experiences23.
Anti-social behaviours are linked to activities like substance abuse and violent acts. It is important to understand that this type of behaviour is often co-morbid to mental health problemsI. Poor development of emotional regulation skills during childhood, as well as the adolescent's environment play a major role in the development of this emotional regulation strategy24.
The activity of Eating is frequently connected to an emotional response and is indicated to have the ability to regulate emotions, but eating could also be regulated by emotions25. In a study by Sim & Zeman26 on adolescent girls, a clear link was found between disorganised eating and negative emotions.
The use of the correct physical activity as an emotional regulation tool could have multiple positive effects on emotional health27. However, literature indicates that excessive physical activities in adolescent boys and girls could also be an indicator of depressed mood, dissatisfaction with body image and low self-esteem28.
Creative activities have been linked to positive emotional regulation strategies7. Literature indicates that specific strategies like journaling, could assist an adolescent in identifying and regulating negative emotions29.
Even though the above-mentioned categories relate to strategies found in literature, some items loaded on more than one factor (Figure 1), e.g. "painting" categorised under physical activity as well as creative activities. This indicates the complexity of each category and the activity choices clustered under these. As seen in the above sections, several activities can be used as strategies to regulate emotions, but at the same time have the ability to act as the regulator of activity choice, e.g. eating. These findings could pose a challenge for the researcher in the refinement of the scale.
Items loading on more than one factor were excluded from final scale. A provisional scale, consisting of 39 items which together measure five strategies for emotional regulation was therefore developed.
The items and subscales appear usable, but no indication exists at present as to what should be considered "normal" or "functional scores" on the identified strategies. For instance, it is desirable that adolescents show low levels of antisocial behaviour, but it is not clear from the Antisocial Behaviour scale derived in this study, what would be considered "acceptably low". Furthermore, respondents showed the full range of scores for Creative Activities, and the use of this strategy would probably be tied to the interest of the individual. Perhaps, it would be of more use to the occupational therapist to know how much a person is inclined to use a specific strategy (e.g., Antisocial Behaviour or Creative Activities), than to attempt to classify what would be "acceptable." More studies are needed to take the scale values that adolescents might obtain on the various defined strategies, and relate them to effective occupation, showing how an occupational therapist could work with the particular tendencies of the individual in a way to allow them to effectively regulate their emotions while interacting with persons, situations or activities, and to do so without dysregulation. In the current state, this scale has the ability to identify emotional regulation strategies used by the adolescent when experiencing positive and negative emotions, but not yet the measurement thereof.
Limitations
Though 78 items items proved reliable, there are still some discrepancies with regard to items that had to be discarded due to them loading on two different factors. Some strategies identified by participants were difficult to categorise into one specific dimension, e.g. strategies relating to spiritual activities. During a future refinement process, the categories should be re-evaluated, possibly renamed, and specific indicators for each category should be defined.
The study population was limited, consisting only of adolescents in a late adolescent phase in a tertiary institution, and therefore not representative of the whole adolescent population. Specifically taking into account that adolescence consists of different stages and is characterised by rapid change. The refined scale should be tested on a wider population group, consisting of different ages and a variety of culture groups and environments.
CONCLUSION
Emotional regulation is a key concept in the mental health of adolescents and emotional dysregulation can also present in occupational dysfunction. From literature, researchers could not identify a suitable measuring tool to measure emotional regulation strategies or identify emotional dysregulation, used by South African adolescents. In order to address this need, the process of designing a scale for this purpose was started by the researchers.
Three steps were followed in the developmental process and results firstly indicated that all items that were designed from literature were reliable and five categories were defined: Sharing and Comfort, Eating, Physical Activity, Creative Activities and Anti-social Behaviour. These categories were described in literature, confirming the appropriateness thereof. A CFA model confirmed the validity of the five categories, and the final reliability of the 39 items within the current scale was confirmed. Thus, a provisional scale for the identification of emotional regulation strategies was developed.
Even though the scale that was developed was found to be reliable and valid, the authors intend continuing further development and refinement of the scale, and it is not yet suitable for measurement at this stage. Considerations such as some items loading on more than one factor need to be investigated and the scale tested on a wider population. This scale is only a first step in the measurement of emotional regulation strategies.
As this scale is developed for understanding the link between emotional regulation and occupational dysfunction, the refined scale should also be structured in such a way that it could inform an occupational therapist to firstly understand her client's specific emotional regulation strategies and skills, as well as to be able to identify emotional dysregulation.
The use of an emotional regulation scale could be valuable in understanding emotional regulation strategies that enable or disable occupational engagement, assisting in identifying appropriate treatment outcomes and approaches.
REFERENCES
1. World Health Organization (WHO). Caring for Children and Adolescents with Mental Disorders [Internet]. Geneva; 2003 [cited 2016 Aug 25]. p. 27. Available from: http://www.who.int/mental_health/media/en/785.pdf. [ Links ]
2. World Health Organization (WHO). Health for the World's Adolescents- A second chance in the second decade (Summary) [Internet]. 2014 [cited 2016 Aug 25]. 1-14. Available from: http://apps.who.int/adolescent/second-decade/. [ Links ]
3. Louw D, Louw A. Child and Adolescent Development. Bloemfontein: Psychology Publications; 2007: 413. [ Links ]
4. Whitehill JM, Brockman LN, Moreno MA. Just talk to me: Communicating with college students about depression disclosures on Facebook. J Adolesc Heal. 2013; 52(1): 122-7. [ Links ]
5. American Occupational Therapy AAssociation. Framework : Domain & Process (3rd ed.). Am J Occup Ther. 2014; 68(Suppl 1): S1-48. [ Links ]
6. Cole PM, Marin SE, Dennis TA. Emotion regulation as a scientific construct: methodological challenges for child development research. Child Dev. 2004; 75(2): 317-33. [ Links ]
7. Webb TL, Schweiger Gallo I, Miles E, Gollwitzer PM, Sheeran P Effective regulation of affect: An action control perspective on emotion regulation. Eur Rev Soc Psychol. 2012; 23(October): 143-86. [ Links ]
8. Patterson JM, McCubbin HI. A-Cope. Adolescent-coping orientation for problem experiences. Madison; 1981. [ Links ]
9. Hilt LM, Hanson JL, Pollak SD. Emotion Dysregulation. In: Encyclopedia of Adolescence. Springer Science & Business Media; 2011: 160-9. [ Links ]
10. Bjärehed J, Lundh L-G. Deliberate self-harm in 14-year-old adolescents: how frequent is it, and how is it associated with psychopathology, relationship variables, and styles of emotional regulation? Cogn Behav Ther, 2008; 37(1): 26-37. [ Links ]
11. Weinberg A, Klonsky ED. Measurement of emotion dysregulation in adolescents. Psychol Assess, 2009; 21(4): 616-21. [ Links ]
12. World Health Organization (WHO). WHO-AIMS report on Mental Health Systems in South Africa [Internet]. Cape Town; 2007 [cited 2016 Aug 25]. p. 28. Available from: http://www.who.int/men-tal_health/evidence/south_africa_who_aims_report.pdf. [ Links ]
13. Fouché L, Wegner L. Specific Occupational Therapy Intervention with Adolescents. In: R & Alers EC, editor. Occupational Therapy in Psychiatry and Mental Health. 5th ed. Oxford: Wiley Blackwell; 2014: 276-94. [ Links ]
14. Silk JS, Steinberg L, Morris AS. Adolescents' Emotion Regulation in Daily Life: Links to Depressive Symptoms and Problem Behavior. Child Dev, 2003; 74(6): 1869-80. [ Links ]
15. Cotgrove AJ, Cowers SG. Use of An Adolescent In-Patient Unit. Adv Psychiatr Treat, 1999; 5: 192-9. [ Links ]
16. Pierce DE. Occupation by Design: Building Therapeutic Power. Philadelphia. FA.Davis Company; 2013. 356 p. [ Links ]
17. Klopfer E, Sheldon J. Augmenting your own reality: student authoring of science-based augmented reality games. New Dir Youth Dev, 2010; (128): 85-94. [ Links ]
18. Rottenberg J, Gross JJ. Emotion and emotion regulation: A map for psychotherapy researchers. Clin Psychol Sci Pract, 2007; 14: 323-8. [ Links ]
19. Huysamen GK. Psychological and educational test theory. Bloemfontein: Author; 1989. [ Links ]
20. Raubenheimer JE. An item selection procedure to maximise scale reliability and validity. SA J Ind Psychol, 2004; 30(4): 59-64. [ Links ]
21. De Choudhury M, Gamon M, Counts S, Horvitz E. Predicting Depression via Social Media. In Proceedings of the Seventh International AAAI Conference on Weblogs and Social Media. Redmond Association for the Advancement of Artificial Intelligence. 2013; v2: 128-137. Available from: http://www.aaai.org/ocs/index.php/ICWSM/IC-WSM13/paper/viewFile/6124/635l. [cited 2016 Aug 25]. [ Links ]
22. Valkenburg PM, Peter J, Schouten AP. Friend Networking Sites and Their Relationship to Adolescents' Well-Being and Social Self-Esteem. CyberPsychology Behav. 2006; 9(5): 584-90. [ Links ]
23. Greenwood DN, Long CR. Mood specific media use and emotion regulation: Patterns and individual differences. Pers Individ Dif, 2009; 46(5-6): 616-211. [ Links ]
24. Tarter RE. Etiology of adolescent substance abuse: a developmental perspective. Am J Addict, 2002; 11(3): 171-91. [ Links ]
25. Macht M. How emotions affect eating: A five-way model. Appetite, 2008; 50: 1-11. [ Links ]
26. Sim L, Zeman J. The Contribution of Emotion Regulation to Body Dissatisfaction and Disordered Eating in Early Adolescent Girls. J Youth Adolesc, 2006; 35(2): 207-16. [ Links ]
27. Penedo FJ, Dahn JR. Exercise and well-being: a review of mental and physical health benefits associated with physical activity. Curr Opin Psychiatry, 2005; 18: 189-93. [ Links ]
28. Furnham A, Badmin N, Sneade I. Body image dissatisfaction: gender differences in eating attitudes, self-esteem, and reasons for exercise. J Psychol, 2002; 136(6): 581-96. [ Links ]
29. Ullrich PM, Lutgendorf SK. Journaling About Stressful Events: Effects of cognitive processing and emotional expression. Ann Behav Med, 2002; 24(3): 244-50. [ Links ]
 Correspondence:
Correspondence:
Monique Strauss
straussm@ufs.ac.za
*** Article commemorating the UFS Anniversary


{kind=link}
{kind=link}
{kind=link}