










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.46 n.1 Pretoria Apr. 2016
http://dx.doi.org/10.17159/2310-3833/2016/v46n1a9
SCIENTIFIC ARTICLES
Time management guidelines for the intervention of a child with Down syndrome using the Developmental "Resource Stimulation Programme" (DRSP)
Dorothy Charmaine RussellI; Rita van HeerdenII; Santie van VuurenIII; André VenterIV; Gina JoubertV
IMOT (UFS), PhD OT (UFS)- Senior Occupational Therapist/Director at Bloemfontein Child Information Centre, Faculty of Health Sciences, Department Paediatrics and Child Health, University of the Free State
IIMOT (UFS), PhD (HPE) (UFS) - Senior Lecturer, Department of Occupational Therapy, Faculty of Health Sciences University of the Free State, Bloemfontein
IIIMOT (UFS), PHD (HPE) (UFS)- Head: School for Allied Health Professions, Faculty of Health Sciences, University of the Free State, Bloemfontein
IVMBChB (Pret), MMED (Wits), PhD (CAN), DCH (SA), FCP (SA)- Academic Head: Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Free State, Bloemfontein
VBA, MSc (UFS) Associate Professor and Head of Department, Department of Biostatistics, Faculty of Health Sciences, University of the Free State, Bloemfontein
ABSTRACT
BACKGROUND: The duration of an intervention session for an intensive early-intervention programme, the Developmental Resource Stimulation Programme (DRSP), for Down syndrome (DS) children younger than 42 months, was investigated as part of a larger research study. The DRSP is a unique, child-parent specific, one-on-one integrated developmental programme for children with Down syndrome from birth to 42 months.
AIM: The aim of this programme was to determine the required number of sessions per activity and optimal session length that enables a child younger than 42 months with DS to master the DRSP activities.
METHODOLOGY: A descriptive study design was used to organise and summarise data from the DRSP checklist score-sheets. Sixteen children with common characteristics of DS, specifically Trisomy 21, and their parents formed part of the investigation.
RESULTS: The research established a time management guideline including the specific duration and frequency of executing an occupational performance activity by a child with DS in order for the child to master the activity.
CONCLUSION: The recommendation is that individual sessions should occur fortnightly to implement the DRSP for children with DS from birth, with the suggested length of a session being 12-15 minutes for children younger than 18 months and 15-40 minutes for children older than 18 months and should be undertaken over a six month period.
Key words: intervention session duration, Down syndrome, early intervention programme, developmental domains, occupational therapy
INTRODUCTION
According to the literature there are few effective early-intervention programmes for children with developmental problems in South Africa1-4. There is a need to ascertain, not only the effectiveness of an intervention programme, but also, at what age intervention should start, what the duration of the intervention should be, and what the frequency of intervention sessions should be5. This study, investigated the impact of the Developmental Resource Stimulation Programme (DRSP) on children with Down syndrome and provided the opportunity to establish the specific duration and frequency of intervention required by children with DS to achieve an occupational performance activity.
The DRSP is a unique, child-parent-specific, one-on-one integrated programme for children with DS from birth to 42 months and spans seven age bands6,7. It was developed in order for both the parent and child to be actively involved during activity participation at home. The DRSP activities manual is easy to
understand and/or read and consists of 85 activities. The activities cover cognitive, language, fine-motor and gross-motor development. The activities also utilise occupations such as play and social participation of the child. The manual consists of detailed sketches, descriptions of occupational activities for participation and clearly stipulates the outcomes (goals) of the programme. The materials used are everyday household objects such as three plastic mugs, four teaspoons and a facecloth. These objects are durable, inexpensive and they do not exclude any socio-economic group8,9. It is a systematic programme consisting of exercises and activities designed to address developmental delays experienced by children with DS in different age bands10-12. It was developed to assist parents of children with DS in developing countries. The development of the programme is described in more detail in the article "The impact of the "Development Resource Stimulation Programme on children with Down syndrome" published in this journal13.
The aim of this study was to determine the required number of sessions per activity and the optimal session length would that would enable a child with DS to master the DRSP activities.
METHODS
Study design
A descriptive study design14 was used to organise and summarise data from the DRSP score-sheets.
Population and sampling
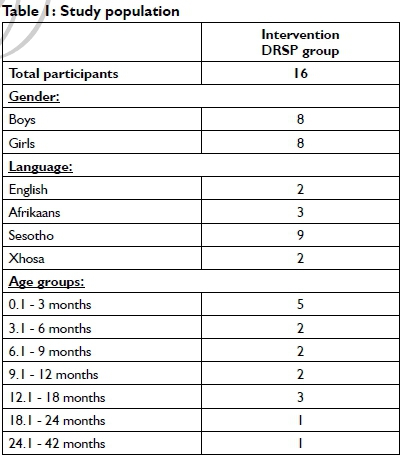
Sixteen children (8 boys and 8 girls) with common characteristics of DS, specifically Trisomy 21, and their 16 parents were included in the study. Their diagnosis was confirmed by clinicians and laboratory analyses. Their ages ranged from 25 days to 28 months. A diverse range of languages was represented, including English, Afrikaans, Sesotho and Xhosa. All parents were proficient in English. The study population selection was determined by availability and compliant parents of children with DS, who were part of a larger research study.
The study was done at the Child Information Centre, Department Paediatric and Child Health, Faculty of Health Sciences, University of the Free State in South Africa where an occupational therapist was in attendance. The children received intervention using the DRSP every fortnight for six months. There were participants in all seven age bands (birth to 3 months: n = 5; 3-6 months: n=2; 6-9 months: n=2; 9-12 months: n=2; 12-18 months: n = 3; 18-24 months: n=1; 24-42 months: n=1) as defined by the DRSP (Table I).
Data collection
The data were collected by using the DRSP during the 12 intervention sessions per child over a six-month period with active participation by the parents, which equals a total of 192 sessions for all children. A total of 85 activities within the DRSP, including the KIT with the description and outcomes of each activity used by parents during activity participation at home7.
The process used in the implementation of the DRSP session consisted of an introduction, demonstration of DRSP activities using therapeutic strategies; time allocation for practising DRSP activities by a parent/caregiver and feedback from the parent/ caregiver about issues on the intervention. During this session the DRSP intervention was done with demonstrations and repetitions with the parents' involvement. Feedback time and questions by the parents were managed at the end of the session and were not added to the intervention time. The specific time for an intervention session was recorded for each intervention session and later confirmed through the video recordings.
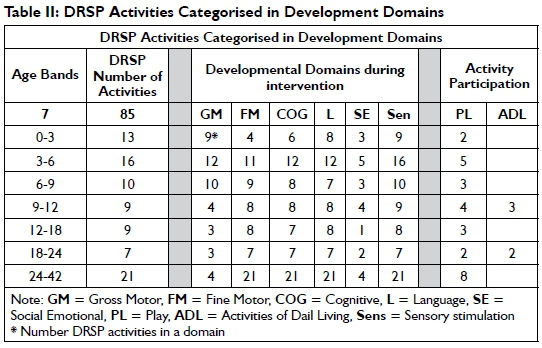
The DRSP checklists were designed ns according to the DRSP activities manual 1 (Table II)7. The scoring was done by using the rating scale of the DRSP that was guided by the rating scale of level descriptors of the International Classification of Functioning, Disability and Health Framework for Children and Youth (ICF-CY). The descriptors of each level were adapted to fit the content of the DRSP response categories6.
The DRSP checklist included subject identification in code, date of birth, specific activity in each age band, date of intervention, outcomes of intervention performed by child (measured with the ordinal scale), field notes or analytical memos and numeric recording. Participation of the child was quantified using the ordinal scale by applying the descriptors from 0-4; where 0 indicated the child "was unable" to perform the activity;
1 indicated "help required more than 50%"
2 indicated "help less than 50% required"
3 indicated "mild help required 25% of the time" and 4 indicated that the child had "no problem" performing the activity. Because of the small sample the level descriptor scores were grouped into two groups, namely "could not master items independently (level descriptors 0-2)" and "could master items independently (level descriptors 3-4)" in the five domains for interpretive purposes. The seven age bands were 0-3 months, 3-6 months, 6-9 months, 9-12 months, 12-18 months, 18-24 months and 24-42 months. These age bands were based on the stages of the Sunshine Centre Home Programme, namely the Strive Towards Achieving Results Together (START)15.
The first intervention session was determined by the child's pre-test age scores on the Bayley Scales of Infant and Toddler Development, 3rd edition16. If a child with DS had an age score of four months, intervention started in the 3-6 months age band.
Pilot study
A pilot study was conducted in order to establish how the intervention sessions could be implemented fluently. This session was video recorded to plan the correct positioning of the patient, parent and therapist.
Data analysis
A descriptive analysis was used. The data of the DRSP checklist were scored according to the level descriptors. This evaluated the intervention progress. The data were subsequently transferred to a data sheet. The data of DRSP checklists were summarised as medians17.
Error of measurements
Two independent occupational therapists moderated the DRSP checklists from the video recordings. Weighted Kappa was a suitable approach for the calculation of the interrater reliability (IRR) in this study. Since the DRSP checklist is on an ordinal scale, a variant of Cohen's Kappa was used by assigning weights to the scores in order to obtain a different degree of disagreement between available scores18. The Weighted Kappa was 0.97 which indicated near perfect agreement19.
Ethical considerations
Ethical approval was obtained from the Ethics Committee of the Faculty of Health Sciences of the University of the Free State prior to the research (ECUFS no. 01/2011).
Since all the participants were younger than 42 months, written, informed consent was obtained from all the parents. Parents were informed that their participation was voluntary and that they had the right to withdraw at any time without prejudice.
RESULTS
Table III summarises the median number of intervention sessions required for a child with DS to master an activity in the specific domain for the different age bands. Cognitive, language, gross-motor, social-emotional and play/ ADL activities required a median of three interventions. Fine-motor activities required a median of four. Intervention for the child with DS from birth to six months requires a six-week intervention period to master an activity independently. The 6-9 month age band would require an intervention period of five weeks, whilst the 9-12 month age band would require an intervention period of eight weeks. The 12-18 months age band requires a seven week intervention period; the 18-24 months age band requires a four week intervention period, whilst the 24-42 months age band requires an intervention period of more than 24-weeks to master activities in the DRSP (Table III).
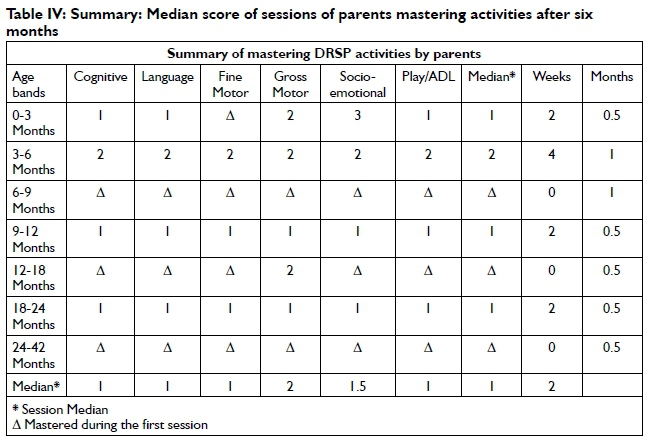
Table IV summarises the parents' mastering of activities in all the domains. The median time taken by parents to master all of the performance activities in the domains was either during or at the end of the first session (Δ/1), except for the age band 3-6 months when parents needed more assistance and mastering the activities therefore took four weeks (two sessions).
DISCUSSION
The time management guideline presented in this objective can enable an occupational therapist to plan intervention sessions for children with DS within a specific time frame. This will be more cost-effective and parents can plan their own schedules more efficiently. The results indicated that three sessions will be required to achieve pre-defined activities for all domains - three being the median number of sessions for a child with DS to master an activity in a specific domain. This implies a six-week period of intervention at two-week intervals (depending on which activity and how many different activities the occupational therapist wants the child to master). The mastering of the skills requires that the occupational therapist be part of the intervention process and that all parties be engaged20. It is important to state that the presence of an occupational therapist will help parents master the skills.
The most rewarding aspect of this study was assisting parents to be part of a process that was usually reserved for health professionals. Teaching and supporting parents with DS children to master these activities correctly and independently were the pinnacle of this study. The handling strategies in the DRSP were compiled and taught to the parents in such a way as to achieve positive outcomes in the mastering of the activities. The close involvement and accompaniment of an occupational therapist appeared to empower the parents, which was the ultimate goal.
RECOMMENDATION
The recommendation is that individual sessions should occur fortnightly to implement the DRSP for children with DS from birth, with the suggested length of a session being 12-15 minutes for children younger than 18 months and 15-40 minutes for children older than 18 months which should be undertaken over a six month period.
CONCLUSION
The observation was made that, with continuous use of the DRSP, parents could easily execute the activities at home. This resulted in excellent participation of their children during intervention sessions. As a result of the progress of the children observed by their parents, it seems reasonable to assume that parents will follow the DRSP successfully and independently as a home programme.
ACKNOWLEDGEMENTS
I would like to acknowledge Prof. H Kotzé for his invaluable assistance in writing this article and Johané Nienkemper for endless support throughout the research. I would like to thank the parents of the children with Down syndrome who participated in the research for their enthusiasm and dedication. I am grateful to the editor and other reviewers for their detailed comments and suggestions that assisted a great deal in improving this paper.
REFERENCES
1. Capone GT. Down syndrome: genetics, insights and thoughts on early intervention. Infants and Young Children, 2004; 17: 45-58. [ Links ]
2. Castillo DL. Children with Complex Medical Issues in Schools: Neuropsychological Descriptions and Interventions. US: Springer Publishing Company, LLC. 2008. [ Links ]
3. Fidler DJ, Hepburn SL & Rogers SJ. Early learning and adaptive behavior in toddlers with Down syndrome: evidence for an emerging behavioural phenotype? Down Syndrome Research and Practice, 2006; 9(3): 37-44. [ Links ]
4. Villamonte R. Reliability of Sixteen Balance Tests in Individuals with Down syndrome. A dissertation submitted to the Faculty of Brigham Young University for the degree Doctor of Philosophy. August. 2009. Available at http://contentdm.lib.byu.edu/ETD/image/etd2059.pdf (20 February 2012). [ Links ]
5. Dunst DJ, Meter D & Hamby DW. Influences of sign and oral language interventions on the speech and oral language production of young children with disabilities. Center for Early Literacy Learning, 2011; 4(4)1-20. Available at http://www.earlyliteracylearning.org/cellreviews/cellreviews_v4_n4.pdf (Accessed 16 April 2012). [ Links ]
6. Russell DC. The impact of the Developmental Resource Stimulation Programme on children with Down syndrome. Doctoral thesis, UFS. 2013. [ Links ]
7. Russell DC. The Development Resource Stimulation Programme. ISBN 978-0-86886-807-3. Bloemfontein: Published. 2010. [ Links ]
8. Russell DC & Van Wyk AC. Speel-Pret Stimulasie Program, 0-3 jaar. ISBN 0-86886-654-7. Bloemfontein. 2003. [ Links ]
9. Russell DC. Play-Fun Stimulation Programme, 0-3 years. ISBN 0-86886-720-9. Bloemfontein. 2006. [ Links ]
10. Fergus L. Treatment of Down syndrome. About.com. Down Syndrome. 2009. < http://downsyndrome.about.com/od/downsyndrometreatments/a/Treatmentess_ro.htm> (20 February 2012). [ Links ]
11. Down Syndrome South Africa. Down Syndrome South Africa website. Johannesburg: South Africa. 2010. < http://www.down-syndrome.org.za/> (11 January 2010). [ Links ]
12. New York State Department of Health. New York State Department of Health (NYSDOH), Division of family health, bureau of early intervention. n.d. Clinical Practice Guideline: Report of the Recommendations: Down Syndrome Assessment and Intervention For Young Children (Age 0-3 Years). <http://www.nyhelth.ogv/community/infants_children/erarly_intervention/index.htm> (2 February 2012). [ Links ]
13. Russell D, van Heerden R van Vuuren S, Venter A, Joubert G. The impact of the "Developmental Resource Stimulation Programme" on children with Down syndrome. SAJOT, April 2016, 46;l: in this edition, 34-41. [ Links ]
14. Leedy PD & Ormrod JE. Practical Research Planning and Design. 9th ed. New Jersey, US: Pearson Education, Inc. 2010. [ Links ]
15. Solarsh B, Katz B & Goodman M. START Teacher-Counsellor's Guide Volume 1. Johannesburg: The Sunshine Centre. 1990. [ Links ]
16. Bayley C. Bayley Scales of Infant and Toddler Development. 3rd ed. Administration Manual. US: Harcourt Assessment, Inc. 2006. [ Links ]
17. Joubert G & Katzenellenbogen J. Population and sampling. In Joubert G & Ehrlich R (eds). Epidemiology: A Research Manual for South Africa. 2nd ed. Cape Town: Oxford University Press, Southern Africa (Pty) Ltd. pp. 94-104. 2007. [ Links ]
18. Cohen J. Weighted Kappa: nominal scale agreement with provision for scaled disagreement or partial credit. Psychological Bulletin, 1968; 70(4): 213-220. [ Links ]
19. Viera AJ & Garret JM. Understanding Interobserver AAgreement: The Kappa Statistic. Family Medicine. 2005; 37(5): 360-363 [ Links ]
20. Pierce D. Occupation by design: dimensions, therapeutic power, and creative process. The American Journal of Occupational Therapy, 2001; May/June 55(3): 249-259. [ Links ]
 Correspondence:
Correspondence:
Dorothy Russell
russeldc@ufs.ac.za


{kind=link}
{kind=link}