










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.46 n.1 Pretoria Apr. 2016
http://dx.doi.org/10.17159/2310-3833/2016/v46n1a8
SCIENTIFIC ARTICLES
The impact of the "Developmental Resource Stimulation Programme" (DRSP) on children with Down syndrome
Dorothy Charmaine RussellI; Rita van HeerdenII; Santie van VuurenIII; André VenterIV; Gina JoubertV
IMOT (UFS), PhD OT (UFS)- Senior occupational therapist / Director at Bloemfontein Child Information Centre, Faculty of Health Sciences, Department of Paediatrics and Child Health, University of the Free Sate
IIMOT (UFS), PhD (HPE) (UFS) - Senior Lecturer, Department of Occupational Therapy, University of the Free State
IIIMOT (UFS), PhD (HPE) (UFS)- Head of the School for Allied Health Professions, Faculty of Health Sciences, University of the Free State
IVMBChB (Pret), MMED (Wits), PhD (CAN), DCH (SA), FCP (SA)- Academic Head of the Department of Paediatrics and Child Health, Faculty of Health Sciences, University of the Free State
VBA, MSc (UFS) Associate Professor and Head of Department, Department of Biostatistics, Faculty of Health Sciences, University of the Free State
ABSTRACT
BACKGROUND: This study investigated the impact of an intensive early-intervention programme, the Developmental Resource Stimulation Programme (DRSP), on Down syndrome (DS) children younger than 42 months in the South African context. The DRSP is a unique, child-parent specific, one-on-one, integrated developmental programme for children with Down syndrome from birth to 42 months.
AIM: The aim of this study was to investigate the impact of the DRSP on Down syndrome children younger than 42 months in the South African context.
METHODOLOGY: A non-randomised control group pre-test-post-test design was followed. The Bayley Scales of Infant and Toddler Development, 3rd edition was used. Thirty children with the general characteristics of DS, specifically Trisomy 21, were included in the study. There were two groups, namely the intervention group (n = 16) and the control group (n = 14) which were studied over a period of six months.
RESULTS: This study showed that a specifically designed programme, with participation of a parent, has a positive impact on the development of the child with Down syndrome.
CONCLUSION: Contrary to the existing literature, there were positive changes in the fine-motor development and language of the intervention group overall and in the gross-motor development of children older than 9-months with Down syndrome.
Key words: early intervention programme, Down syndrome, younger than three years, developmental domains, occupational therapy
INTRODUCTION
Down Syndrome (DS) is a multisystem neuro-genetic (chromosomal) disorder, which has been recognised as the leading genetic cause of intellectual disability. In South Africa the incidence of DS is one in 770 births1. Children with Down Syndrome have an additional chromosome, the extra one being an additional copy of chromosome 21 called Trisomy 21. This is the most common cause of Down Syndrome2,3. An additional cause of the condition is related to chromosomal translocation. Down syndrome is typically associated with physical growth delays, characteristic facial features, and mild to moderate intellectual disability4, with speech as well as motor-developmental problems5. According to the existing literature, early intervention is a systematic programme of therapies, exercises and activities designed to address the developmental delays6 specifically experienced by children with Down syndrome. However early intervention programmes for children with developmental delays especially for children with Down Syndrome in South Africa are rare7..Fergus8 mentions only physiotherapy and speech therapy as possible early-intervention treatments. According to the Down Syndrome Association websites and support groups, occupational therapy would only play a role in promoting the independence of children with DS once the physiotherapist and speech therapist had produced the primary foundation for development8. There also appears to be no occupational therapy early intervention stimulation programme that has been specifically developed for the child with Down syndrome9,10,11,12.
The programmes currently most used for intervention in SA are as follows: "The Washington DSPI Programme" (Developmental Sequence Performance Inventory), was adopted in the Western Cape. This programme was developed by Model Programs, Experimental Education Unit, College of Education and Child Developmental and Mental Retardation Center, University of Washington, but not specifically for DS7. This programme is a developmental sequence performance inventory, which consists of age bands with developmental activities based on typical development7. The START (Strive Towards Achieving Results Together) programme was developed at the Sunshine Center in collaboration with the Memorial Instituter for Child Health and Development (CMI) in Johannesburg, SA but this programme was also not specifically for DS but for all children with developmental delays13. The acronym underwrites the importance of equipping parents to assist their own child and not always to depend on a health worker13.
The author has been involved for the past 20 years in an occupational therapy programme as part of a holistic approach which included the therapist-implemented treatment approach with two motor-intervention models, namely Neuro-Developmental Treatment (NDT) and Developmental Skills7 as well as Parent-implemented developmental training14 for young children with DS at a resource centre in Bloemfontein, SA. The positive clinical outcomes, especially early walking (before 27 months), of these children, were encouraging. Studies that supported this finding showed that a more holistic approach to the developmental problems of children with DS can make a long-term difference in their functioning and quality of life15-19. During the course of her work in assisting parents of children with DS the author formulated the Developmental Resource Stimulation Programme (DRSP)20, an early-intervention programme specifically intended for DS children7. It was specifically developed to assist parents of children with DS in developing countries.
The DRSP is a unique, child-parent-specific, one-on-one, integrated programme for children with DS from birth to 42 months and spans seven age bands7. The DRSP was designed to stimulate the child's development and involves the active participation of the parent who carries out relevant DRSP activities at home with their child. The DRSP consists of an activities manual and an activities kit. The DRSP manual describes specific activities for specific age groups, starting from birth up to 42 months. Each of the 85 activities stipulates the outcomes and gives a detailed description, with a specific and appropriate name7. To address possible literacy problems and forgetfulness, each named activity is accompanied by a sketch to reinforce the description of the positioning, handling and presentation. These are to be used by parents during activity participation at home.
The manual is accompanied by a kit (DRSP KIT) containing household objects which are durable, cost-effective and do not exclude any socio-economic group21,22. The participation of the child with DS was quantified using an ordinal scale by applying the level descriptors from 0-4 based on the qualifiers for seven age bands, namely 0-3 months, 3-6 months, 6-9 months, 9-12 months, 12-18 months, 18-24 months and 24-42 months. Each activity in the age bands was analysed to goal specific abilities, namely; cognitive, gross-motor, fine-motor, language, socio-emotional, play and activities of daily living (ADL). The activities address the same developmental domains as the Bayley Scales namely cognitive, language, fine-motor and gross-motor development. In the age band, for example 3-6 months activity "Hands in Midline", the description is that the baby's head is on the mothers' knees and his bottom against her stomach. The mother holds the mug in midline in front of the baby and encourages the baby to reach for the mug and/or to touch. The mother constantly talks to the baby while he/she is watching her face. She should make sounds such as "ee". "aa". "uh", "k". "g"20.
There are only two known studies on intervention with children younger than six months with DS - one in the Netherlands (a problem-specific physiotherapy programme23) and the other in Italy14. In the Italian study a parent-implemented developmental training programme was compared to the therapist-implemented treatment. This intervention was based on activities that can readily be incorporated in the daily care routines of the infants. In the study the parent-implemented developmental training was found to be more effective. The majority of published studies were carried out on children older than two years10-12,18,19. These studies found that early intervention was beneficial to the child with DS, but the programmes that were described consisted of treatment methods only and no description of the way in which the programmes were implemented were given11,19.
This study aimed to assess the effectiveness of the DRSP through an intervention programme with children with DS who were younger than 42 months. This resulted in the validation of the DRSP in the SA context for children with DS where the socio-economic environment differs largely from that in developed countries.
METHODS
Study design
A quasi-experimental design was used24. Due to the small population sample a matching process was not feasible. A heterogeneous non-randomised control group pre-test-post-test design was followed25.
Population and sampling
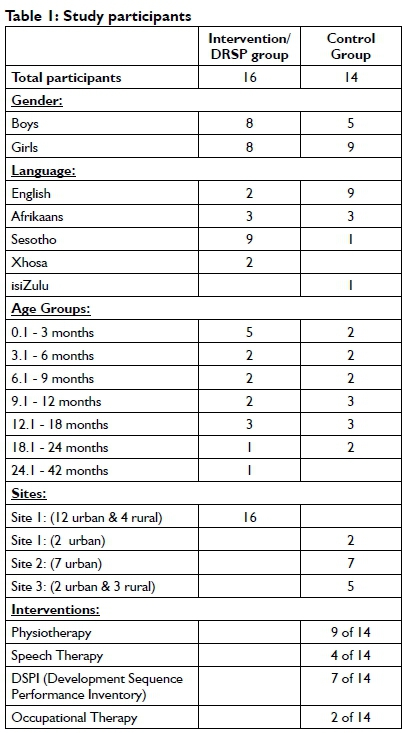
The deciding factor for the study population was the availability of participants. Thirty children with common characteristics of DS, specifically Trisomy 21, were studied. Their diagnoses having been confirmed by medical practitioners. All participants had to be younger than 42 months as the test used for evaluation purposes was standardised only on children up to 42 months. Children were excluded from the study if they suffered from adverse events such as illnesses that could negatively influence attendance at intervention sessions and their endurance; Cerebral Palsy with DS, as the physical challenges influence the development of the child; and heart disease and/or open-heart surgery at the time of the research study. A diverse range of languages was represented, including English, Afrikaans, Sesotho, Xhosa and isiZulu (see Table I).
Intervention group
The intervention group consisted of 16 participants, eight boys and eight girls who were located in the city where the occupational therapist, the researcher, resided and attended the same centre. The age of the group ranged from 25 days to 28 months and consisted of participants in all seven age bands as defined by the DRSP See Table I for the distribution.
Control group
The non-matched control group was made up of 14 children with DS from three cities in South Africa who could not attend two weekly intervention sessions. This group consisted of five boys and nine girls. The age distribution can be seen in Table I. After the study, training was given to these parents and other therapists to enable them to use the DRSP. This group continued with their usual interventions including physiotherapy, occupational therapy and speech therapy and the DSPI programme, during the time of the study.
Research tools
1. The Bayley Scales of Infant and Toddler Development, 3rd edition (Bayley Scales III)26-28, was used to collect the baseline data on all participants since it is the assessment tool most commonly used in numerous other studies of children with intellectual disabilities28 and children with DS17,29,30. In addition, both the Social-Emotional Scale and the Adaptive Behavior Scale's reliability scores reflect strong internal consistency31.
2. All evaluations were video recorded to obtain a true reflection of the evaluation sessions and were used in the moderating process discussed in Methods more detailed.
3. DRSP KIT was used with the intervention group. This has been described in the review of the literature.
Methods
The children were evaluated prior to the commencement of the study by an occupational therapist trained in the use of the Bayley Scales III. All the pre- and post- evaluations of the intervention- and control group were done and scored by this therapist who was blinded to this study. The pre- and post-tests were six months apart. All the assessments were video recorded on a tripod and moderated by a second OT from the video recordings to control for bias. The scores of this OT were used, as there were only seven differences throughout the evaluation process (see Data analysis).
The members of the intervention group each received 12 intervention sessions over the six month period and a total of 192 intervention sessions for the group were given, using the DRSP. These 192 intervention sessions were given by the researcher who was also the developer of the DRSP. The length of a session was 12-15 minutes for children <18 months and from 15 to 40 minutes for children >18 months. Parents were actively involved during the sessions. Another two independent occupational therapists moderated and scored 20% of the intervention sessions from video recordings using the level descriptors of the DRSP checklist.
The control group continued their regular programmes which consisted of occupational therapy, physiotherapy, speech therapy. However there were two participants in this group that received no therapy.
The same venues with pre-arranged furniture were used at the different sites for all the pre-testing and post-testing as well as the intervention sessions.
Data analysis
The assessment data from the Bayley Scales III tests were summarised using medians and quartiles25. Within-group changes were assessed using the non-parametric Wilcoxon signed-rank test, and groups were compared using Mann-Whitney tests.
The inter-rater reliability of the assessment scores given by the two occupational therapists was evaluated using Cohen's Kappa32. Since scores were classified as Nominal variables (0 and 1), all participants were rated by the same coders (fully crossed design) and two evaluators were used32. The Kappa was 0.97 which indicated high agreement between the two sets of scores33. There was no difference between the scores given by the moderators of the intervention and those of the researcher.
Ethical considerations
Ethical approval from the Ethics Committee of the Faculty of Health Sciences of the University of the Free State was obtained prior to implementing this research (ECUFS no. 01/2011).
Since all the participants were younger than 42 months of age, written informed consent was obtained from all the parents. Parents were informed that participation in the study was voluntary and that they had the right to withdraw from the programme at any time without prejudice. The control group's parents gave consent for their children to be evaluated and filmed as well being informed that they would be provided with some intervention strategies at the completion of the study.
RESULTS
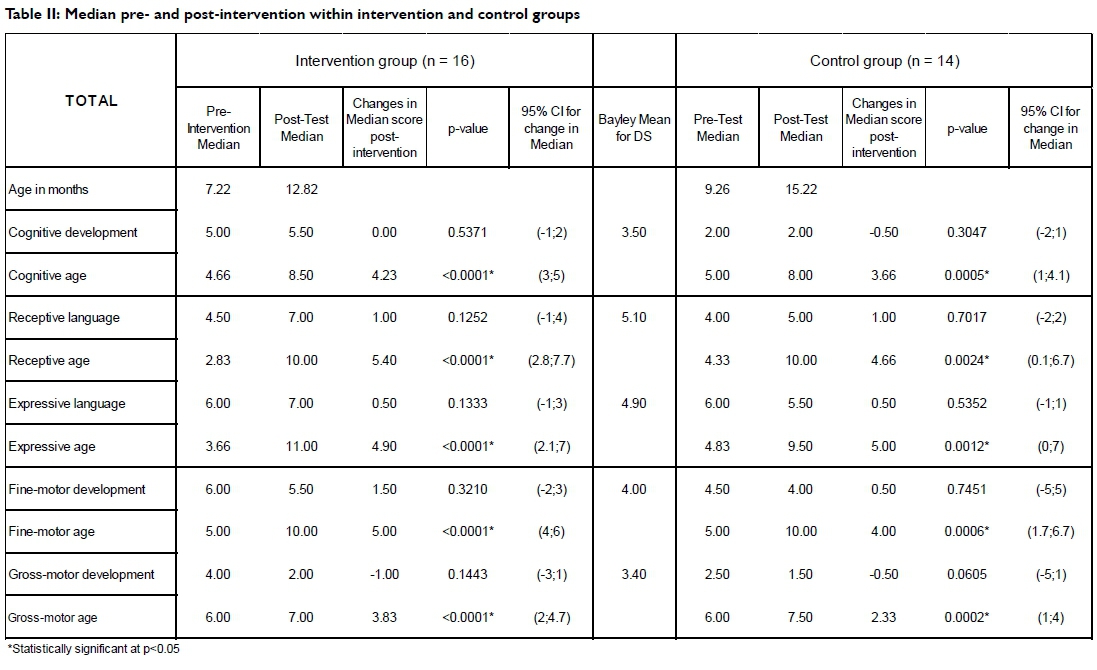
Table II on page 36 summarises the pre-intervention and post -intervention standard scores for both groups of participants as well as the Bayley Scales III mean scores that are provided for children with DS.
In general, the post-intervention median scores of the intervention group were higher than the control group and the Bayley Scales III mean scores for the DS population33, in all the domains except in the gross-motor domains.
In both groups there was a significant increase in the chronological age. The median scores increased in the expressive language domains in both groups. The fine-motor domain median of the intervention group showed an increase of 1.5 and a median decline of -1.0 in the gross-motor domain. The control group showed a median increase of 0.5 in the fine-motor domain and a median decline of -0.5 in the gross-motor domain.
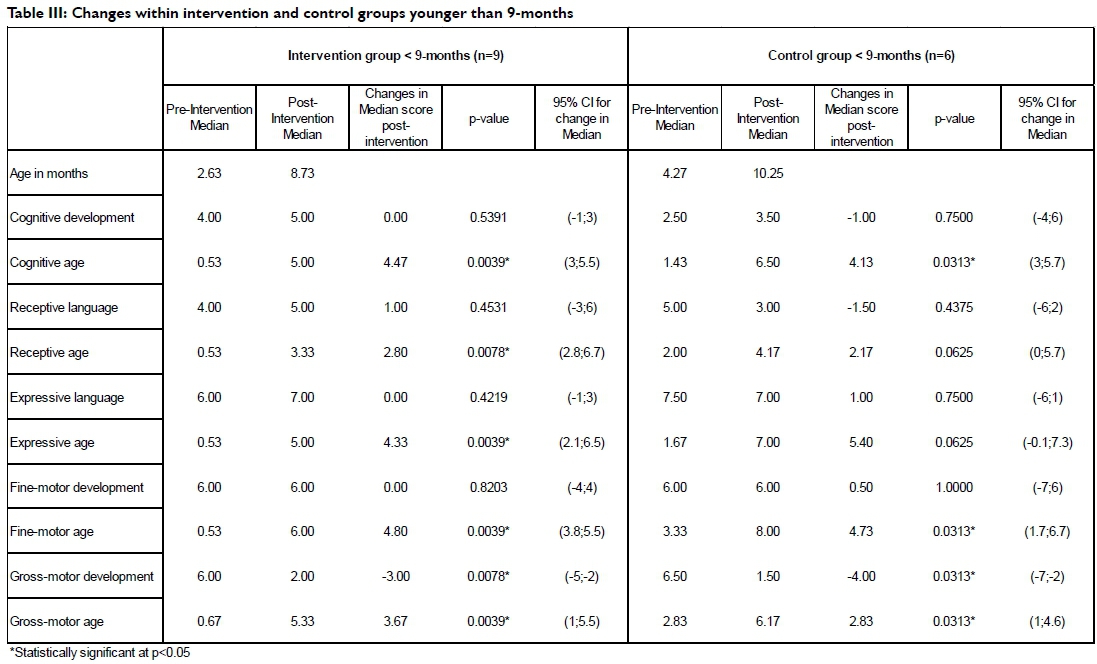
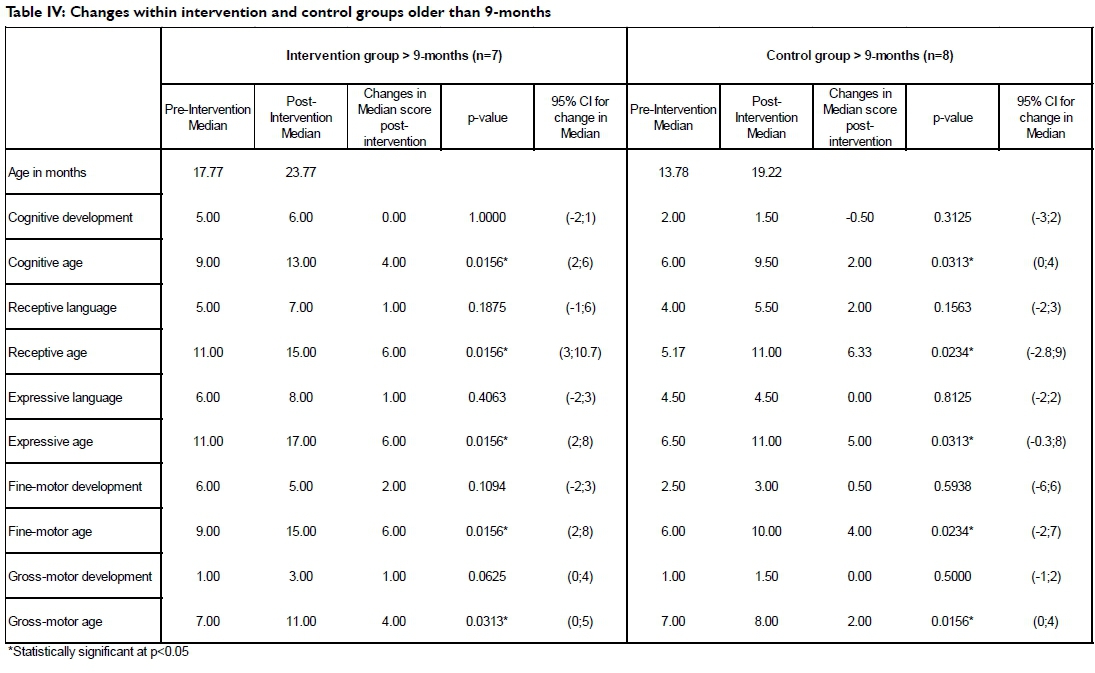
On the basis that the development of three month old infants with DS seems to be typical from birth, with delays in development only after six months19,36, exacerbated at 16 months36,37, the two groups were subdivided into those children younger than nine months and those older than nine months. The results are given in Tables III and IV on pages 37 and 38.
In both the groups younger than nine months the Bayley Scale III scores increased significantly in cognitive age, receptive age (only in the intervention group), expressive age, fine-motor age and gross-motor age. This is as expected as the participants were six months older.
The intervention group younger than nine months showed a median score increase in receptive language. Median scores in cognitive, expressive language and fine-motor domains remained the same, with a significant decrease in the gross-motor domain. The control group showed a median score increase in the expressive language and fine-motor domain, with a decrease in the cognitive, receptive language and gross-motor domain.
The intervention group older than nine months showed no changes in the cognitive domain (Table IV). There were median score increases in the receptive language, expressive language, fine-motor and gross-motor domains. The control group showed a decrease in the median score for the cognitive domain. The median score increased in the receptive language and fine-motor domain, with constant median scores for expressive language and gross-motor domain.
DISCUSSION
The results of this study suggest that the DRSP effectively improved developmental outcomes with a positive impact on the developmental domains of the child with DS. The intervention group performed better clinically than the control group in the cognitive, fine-motor and gross-motor developmental domains. The changes in median score post-intervention indicated that both groups performed similarly in the receptive and expressive language development domains (Table II).
The changes from pre- to post-intervention median scores in the intervention group were higher than those in the control group as well as when compared to the Bayley Scales III mean scores for the DS population. Both groups' post-test median showed increase in the language domains. Fine-motor developmental domains showed an increase in changes, but the control group only a small increase. This is different from what is a known consequence of DS, where the older the DS child gets without intervention the lower the level of development19'36,37.
The fine-motor development of the control group was similar to the Bayley Scales III mean scores for the DS population (Table II) whereas the cognitive, receptive language and gross-motor development post-intervention median scores were below the Bayley Scales III mean score in the control group. Possible reasons for this may be that the control group's therapists implemented only specifically targeted programmes and had less carryover by parents. However, the control group's expressive language development had higher pre- and post-intervention scores than the Bayley Scales III means score for the DS population which may be a reflection of the intervention from the speech therapists.
Although the intervention group's pre- and post-intervention scores increased, the median change in the cognitive domain remained the same (Table II). The performance of the control group showed a slight decline in cognitive median scores and confirms the findings in the literature37-39.
The developmental trajectories of the intervention and control groups, when divided into the two age subgroups, younger than nine months (n=9 intervention and n = 6 control) and older than nine months (n = 7 intervention and n=8 control) the positive outcomes are more evident. The pre-and post-intervention cognitive median scores increased (from 4 median to 5 median) in the younger than 9-months intervention group, but the median score in the cognitive developmental domain did not change (Table III). There was a slight decrease in the cognitive developmental domain in the control group of children younger than 9-months. This decrease may be due to the small number (2) in the control group 0-3-months age band as opposed to the five participants in the intervention group. Learning delays36 are evident in children with DS from ages 0-2 years. Our results suggest that the DRSP may have accomplished a positive impact on the cognitive abilities, not only for infants with DS younger than nine months, but may even increase the cognitive abilities for the child with DS in the older than 9-months group (post-intervention median scores) (Table IV). The intervention group of children older than 9-months (Table IV) scored higher than the control group of the same age, with a median post test score of six, which implies that the IQ standard score is expected to be 8039. This may confirm that early referrals for intervention are beneficial to the development of children with DS. The median score in the control group older than 9-months decreased from moderate to profound (Table IV). It is feasible to assume that the median score changes of the intervention group are due to the cognitive activities in the DRSP
The median score changes of the intervention group for receptive language and expressive language increased after the six-month DRSP intervention period, even though it was not statistically significant (Table II). The median post-intervention receptive language score increased from 4.5 to 7.0 and the expressive language score increased from 6.0 to 7.0 presumably as a result of intervention. This is what would be expected in a typically developing child of similar age31. This suggests that the activities allocated to the language developmental domain of the DRSP were effective. These results contradict published findings of language deficits12. They were also superior to those of the control. The change in the control group was disappointing, since therapist-implemented programmes, which included speech therapy, were followed. However, the limited increase in the scores of the control group reflected the findings in published literature7,40. According to Fewell and Glick35 Intensive early intervention does not have a statistically significant positive effect on the development of receptive and expressive language of children with DS35. The current study did not show statistical significance, but the intervention group showed almost typical development, as opposed to the decreased scores of the control group.
It was anticipated that the DRSP may positively influence the motor developmental domain through the balanced activities. Both intervention and control groups had increased median changes in the fine-motor developmental domain, but the intervention group (1.5) performed better than the control group (0.5) (Table II). The younger than 9-months old intervention group achieved constant median scores, with no decline (Table III). The change in the median score of the control group increased slightly (0.5). This increase is contrary to published results where decreased scores were observed in the fine-motor developmental domain7. It is likely that their therapist-implemented programmes and parental involvement explain these findings7. Motor development in infants with DS up to three months old is entirely normal from birth, with delays in development only later on7,10,12,16, this may also explain the discrepancies. The decreased median score in the gross-motor developmental domain for both groups of younger than 9-months (Table III) is probably due to inflated pre-intervention median scores since this subgroup included five participants younger than three months. The decrease in the gross-motor development scores for both groups (Table II) may have been due to the underlying neuropathology and phenotype of DS. It is also possible that the decrease could be attributed to the difficulty which the parents experienced in mastering some of the gross-motor activities that had to be done at home. In the older than 9-months group the intervention group improved during the six-months and performed better than the median score for the control-group, which remained the same (Table IV). This contradicts the notion that children with DS develop typically during the initial months and, after 16 months, delays in development are present12. The evidential decrease in scores for the gross-motor developmental domain adds to the accumulating evidence that the treatment methods and approaches currently used in early motor intervention are inadequate and fall short of expectations41.
It must be stressed that interpretation of the results must take into account the small sample size.
RECOMMENDATIONS
The DRSP activities manual consists of a balanced number of activities allocated for all developmental domains and may be implemented in its present format and context as a valuable therapeutic tool. We recommend that this programme, specifically developed to assist parents and children diagnosed with DS in the South African context, should be implemented at least up to the age of 42 months. This could address the lack of a specific holistic early-intervention programme. The early enrolment of children with DS into this programme may enable parents to help their children to develop to their full potential at an early age.
CONCLUSION
In conclusion, no significant increases were measured for the median scores in the domains measured within each age-band. However, a clinical significance was indicated through the results of the intervention with DRSP, since increases in the median scores were observed which was beneficial to children with DS.
This was observed specially in the cognitive, fine-motor and gross-motor developmental domains. It is possible that significant conclusions could have been reached if the sample size was larger. Our results therefore strongly suggest that a larger, multicultural study must be done in order to find definitive answers regarding the benefits of intervention programmes.
ACKNOWLEDGEMENTS
We would like to acknowledge Prof H Kotzé, Dean's office, Faculty of Health Science, UFS for invaluable assistance in writing this article and Johané Nienkemper for endless support throughout the research. We are grateful to the reviewers for their comments and suggestions which assisted a great deal in improving this paper.
REFERENCES
1. Naidoo H, Aldous C, Ramdhani H, Winship W, Henriques N & Kormuth E. Down syndrome in paediatric outpatient wards at Durban hospitals. South African Medical Journal, 2011; 101(1):27-28, January. [ Links ]
2. Alexander K. Intellectual disabilities. In Brown C & Stoffel VC (eds). Occupational Therapy in Mental Health. A Vision for Participation. Philadelphia: FA. Davis Company. pp. 111-122. 2011. [ Links ]
3. Roizen NJ. Down syndrome (Trisomy 21). In Batshaw ML, Roizen NJ & Lotrecchiano GR (eds). Children with disabilities. 7th ed. Baltemore, Maryland, US: Paul Brookes Publishing Co. pp. 307-318. 2013. [ Links ]
4. Weijerman, ME; de Winter, JP (Dec 2010). "Clinical practice. The care of children with Down syndrome. European Journal of Pediatrics, 169(12): 1445-52. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2962780/pdf/431_2010_Article_1253.pdf (9 October 2015) [ Links ]
5. Hernandez-Reif M, Field T, Largie S, Mora D, Bornstein J & Waldman R. Children with Down syndrome improved in motor functioning and muscle tone following massage therapy. Early Child Development and Care, 2006; 176(3, 4): 395-410. [ Links ]
6. Moeschler JB, Shevel lM & Committee on Genetics. Clinical genetic evaluation of the child with mental retardation or developmental delays. Pediatrics, 2006; 117(6): 2304-2316. [ Links ]
7. Russell DC. The impact of the Developmental Resource Stimulation Programme on children with Down syndrome. Doctoral thesis, UFS. 2013. [ Links ]
8. Majnemer A. Benefits of early intervention for children with developmental disabilities. Seminars in Pediatric Neurology, 1998; 5(1) :62-69, March. [ Links ]
9. Fergus L. 2009. Treatment of Down syndrome. About.com. Down Syndrome. Available at http://downsyndrome.about.com/od/downsyndrometreatments/a/Treatmentess_ro.htm (20 February 2012). [ Links ]
10. Capone GT. Down syndrome: genetics, insights and thoughts on early intervention. Infants and Young Children, 2004; 17:45-58. [ Links ]
11. Castillo DL. Children with Complex Medical Issues in Schools: Neuropsychological Descriptions and Interventions. US: Springer Publishing Company, LLC. 2008. [ Links ]
12. Fidler DJ, Hepburn SL & Rogers SJ. Early learning and adaptive behavior in toddlers with Down syndrome: evidence for an emerging behavioural phenotype? Down Syndrome Research and Practice, 2006; 9(3): 37-44. [ Links ]
13. Solarsh B, Katz B & Goodman M. 1990. START Teacher-Counsellor's Guide Volume I. Johannesburg: The Sunshine Centre. [ Links ]
14. Del Giudice E, Titomanlio L, Brogna G, Bonaccorso A, Romano A, Mansi G, Paludetto R, Di Mita O, Toscano E & Andria G. Early intervention for children with Down syndrome in Southern Italy: the role of parent-implemented developmental training. Infants & Young Children, 2006; 19(1): 50-58. [ Links ]
15. Villamonte R. Reliability of Sixteen Balance Tests in Individuals with Down syndrome. A dissertation submitted to the Faculty of Brigham Young University for the degree Doctor of Philosophy. August. 2009. Available at http://contentdm.lib.byu.edu/ETD/image/etd2059.pdf (20 February 2012). [ Links ]
16. Karimi H, Nazi S, Sajedi F Akbar-Fahimi N & Karimloo M. Comparison of the effect of simultaneous sensory stimulation and current occupational therapy approaches on motor development of the infants with Down syndrome. Iranian Journal of Child Neurology, 2010; 4(3): 39-44. [ Links ]
17. Nilholm C. Early intervention with children with Down syndrome - past and future issues. Down Syndrome Research and Practice, 1996; 4(2): 51-58. [ Links ]
18. Kubo M & Ulrich B. Coordination of pelvis-HAT (head, arms and trunk) in anterior-posterior and medio-lateral directions during treadmill gait in preadolescents with/without Down syndrome. Gait & Posture, 2006; 23: 512-518. [ Links ]
19. Uyanik M, Bumin G & Kayihan H. Comparison of different therapy approaches in children with Down syndrome. Pediatrics International, 2003; 45(1): 68-73. [ Links ]
20. Russell DC. The Development Resource Stimulation Programme. ISBN 978-0-86886-807-3. Bloemfontein: Published. 2010. [ Links ]
21. Russell DC & Van Wyk AC. Speel-Pret Stimulasie Program, 0-3 jaar. ISBN 0-86886-654-7. Bloemfontein. 2003. [ Links ]
22. Russell DC. Play-Fun Stimulation Programme, 0-3 years. ISBN 0-86886-720-9. Bloemfontein. 2006. [ Links ]
23. Lauteslager PEM. Children with Down's syndrome, motor development and intervention. PhD Thesis. The Netherlands: University Utrecht. 2000. [ Links ]
24. Leedy PD & Ormrod JE. Practical Research Planning and Design. 9th ed. New Jersey, US: Pearson Education, Inc. 2010. [ Links ]
25. Joubert G & Katzenellenbogen J. Population and sampling. In Joubert G & Ehrlich R (eds). Epidemiology: A Research Manual for South Africa. 2nd ed. Cape Town: Oxford University Press, Southern Africa (Pty) Ltd. pp. 94-104. 2007. [ Links ]
26. Bayley C. Bayley Scales of Infant and Toddler Development. 3rd ed. Administration Manual. US: Harcourt Assessment, Inc. 2006. [ Links ]
27. Rademeyer VKM. A study to evaluate the performance of black South African urban infants on the Bayley scales of infant development III. Master of Science in Medicine in Child Development and Community Paediatrics. Johannesburg, South Africa. 2010. [ Links ]
28. Shapiro BK & Batshaw ML. Developmental delay and intellectual disability. In Batshaw ML, Roizen NJ & Lotrecchiano GR (eds). Children with disabilities. 7th ed. Baltemore, Maryland, US: Paul Brookes Publishing Co. pp. 291-306. 2013. [ Links ]
29. Blauw-Hospers CH & Haddlers-Algra M. A systematic review of the effects of early intervention on motor development. Developmental Medicine &Child Neurology, 2005; 47: 421-132. [ Links ]
30. Harris SR. Comparative performance levels of female and male infants with Down syndrome. Physical & Occupational Therapy in Pediatrics, 1983; 3(2): 15-21. [ Links ]
31. Bayley C. Bayley Scales of Infant and Toddler Development. 3rd ed. Technical Manual. US: Harcourt Assessment, Inc. 2006. [ Links ]
32. Hallgren KA. 2012. Computing Inter-Rater Reliability for Observational Data: An Overview and Tutorial. Tutor Quant Methods Psychology, 2012; 8(1): 23-34. [ Links ]
33. Viera AJ & Garret JM. Understanding Interobserver AAgreement: The Kappa Statistic. Family Medicine, 2005; 37(5): 360-363. [ Links ]
34. Fidler DJ & Nadel L. Education and children with Down syndrome: neuroscience, development, and intervention. Mental Retardation and Developmental disabilities Research Reviews, 2007; 13: 262-271. [ Links ]
35. Fewell RR & Glick MP. Program evaluation findings of an intensive early intervention program. American Journal of Mental Retardation, 1996; 101(3): 233-243. [ Links ]
36. Chapman RS & Hesketh LJ. Behavioral phenotype of individuals with Down Syndrome. Mental Retardation and Developmental Disabilities Research Reviews, 2000; 6: 84-95. [ Links ]
37. Patterson T, Rapsey CM & Glue P. Systematic review of cognitive development across childhood in Down syndrome: implications for treatment interventions. Journal of Intellectual Disability Research, 2012; 1-13. [ Links ]
38. Tsao R & Kindelberger C. Variability of cognitive development in children with Down syndrome: relevance of good reasons for using the cluster procedure. Research in Developmental Disabilities, 2009; 30:426-432. [ Links ]
39. Psychometric Conversion Table. n.d. <http://faculty.pepperdine.edu/shimels/Courses/Files/ConvTable.pdf> (26 March 2012). [ Links ]
40. Burgoyne K. Reading interventions for children with Down syndrome. Down Syndrome Research and Practice Online, 2009; 1-6. <http://www.down-syndrome.org/reviews/2128/reviews-2128.pdf> (16 April 2012). [ Links ]
41. Mahoney G, Robinson C & Perales FF Early motor intervention: the need for new treatment paradigms. Infants and Young Children, 2004; 17(4): 291-300. [ Links ]
 Correspondence:
Correspondence:
Dorothy Russel
russeldc@ufs.ac.za


{kind=link}
{kind=link}
{kind=link}