










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 n.3 Pretoria Dec. 2014
SCIENTIFIC ARTICLES
Leadership: The key to person-centred care
Corne ThomasI; Sanetta Henrietta Johanna du ToitII; Susanna Maria van HeerdenIII
IBOT (UFS), MOT (UFS) Assistant Director: Occupational Therapy National District Hospital, Bloemfontein
IIB OT (UFS). M OT (UFS), M.Sc. OT (Exeter, UK), PhD (UFS), Dementia Care Mapper (Bradford, UK) Lecturer, Dept of Occupational Therapy, Faculty of Health sciences, University of Sydney, Affiliated Lecturer, Dep of Occupational Therapy, Faculty of Medicine, University of the Free State
IIIB OT (UFS), M. OT (UFS), PhD (HPE) (UFS) Senior Lecturer, Dept of Occupational Therapy, Faculty of Health Sciences, University of the Free State
ABSTRACT
Person-centred care for elders with advanced dementia living in long-term care is essential when addressing these residents' quality of life. Occupational therapists could play a facilitative role in enhancing person-centred care, but need to ensure that caregivers, as essential care partners, are collaborators in this process. Therefore, the perspectives of caregivers would be key to a process where greater understanding and joint effort pave the way for advances in care practice. A mixed methods triangulation design was used to investigate the perspectives of caregivers with regard to occupation, quality of life and activity participation. The findings of this study indicated that caregiver perspectives and behaviour are unlikely to change if the organisation as a whole does not embrace a person-centred approach towards the caregivers. The discussion highlights specific changes needed to attain a level of servant leadership that could assist the organisation to facilitate person-centred care, focussing mostly on caregiver burnout but also including feelings of boredom of residents with dementia. This article considers the potential role of servant leadership as a driving force behind person-centred care.
Key words: Quality of life, dementia, burnout, boredom, servant leadership, restorative practices
INTRODUCTION
The dignity of elderly people with dementia living in residential care facilities is honoured through person-centred care (PCC). However, the traditional model of care, focussing on care as a regimented list of tasks to complete, still dominates the care culture in South African residential care homes1. Consequently residents are institutionalised, a factor that leads to boredom and causes emotional impairments above and beyond the impact of health problems associated with old age2. Institutionalisation creates a pathological system that also impacts on staff, especially in an environment where nurturing is neglected3. Without nurturing residents cannot be recognised as individual human beings with preferences, emotions and potential, but are often treated as objects who only have physical needs2. Institutionalisation creates a pathological system that also impacts on staff, especially caregivers, who often suffer from isolation, helplessness and burnout3.
In recent years, occupational therapists working in residential care settings in South Africa have been challenged to assist with combatting resident boredom and caregiver burnout. The endeavour has involved supporting staff to move beyond a task-focussed orientation to a person-centred focus where residents direct their own care needs. Because of their constant involvement, the care-givers who provide 24-hour care to residents were key in initiating a process for addressing PCC. However, formal and informal in-house training, in addition to occupational therapy staff modelling PCC practice, did not ensure care that was resident directed.
Occupational therapists could play a facilitative role in enhancing person-centred care, but need to ensure that caregivers, as essential care partners, are collaborators in this process4. Changing the leadership approach of any organisation is a challenge in need of careful consideration2,5. Therefore, the perspectives of caregivers would be key to a process where greater understanding and joint effort pave the way for advances in care practice. As facilitators of PCC, the occupational therapists, being mostly involved on a part-time basis within the residential care facility, needed more insight into the role of leadership for combatting a pathological care setting. In this article the potential role of servant leadership as driving force behind person-centred care is considered while exploring the relationship between resident boredom and caregiver burnout. The literature review is followed by an explanation of the mixed methods triangulation study design. The results and discussion are presented simultaneously and emphasise the impact of leadership on boredom and burnout, as well as the changes needed to embrace PCC.
LITERATURE REVIEW
The role of PCC can be better understood when considering the context of the residential care and the impact of institutionalisation on caregiver burnout and resident boredom.
Institutionalisation in a residential care facility
Most residential care facilities have more in common with a hospital than with a home. Anyone who enters a residential care facility, whether to work or to visit, should do so from the perspective that they are entering someone's home, not a workplace or a medical facility4. This hospital perspective is due to society's view that ageing equals decline and therefore elderly persons are all in need of constant medical care2. In this traditional model, the residents in residential care facilities are referred to as patients and the central focus is on their medical conditions. The doctor, professional nurses and therapists are the main role players within the care plan of the residents. A top-down management approach is followed and the workload is divided between the different departments6,7.
Furthermore, the traditional approach creates an environment where the residents wait for the caregivers to provide routine care that is cost-effective. In this task-oriented environment, the person-hood of the residents is neglected and not much attention is given to their individual needs6,7. The problem with this approach is that it cannot address the three most prominent problems faced by elderly people residing in care facilities, namely loneliness, helplessness and boredom. These three problems are referred to as the three plagues of the human spirit 2,5,6. Due to the progressive nature of major cognitive disorders and continuous decline in abilities, the three plagues are more severe for people with advanced dementia. A loss in occupational performance components impact activity performance and can cause people with specific debilitating conditions to become deprived in terms of occupation and prone to situations where they experience sensory deprivation8,9. Therefore, elderly persons with dementia are at risk of suffering from occupational deprivation and occupational injustice10. They are prohibited from participating in meaningful activities, which ultimately lead to a decrease in their quality of life10.
The effect of institutionalisation has an impact beyond the residents and also affects the caregivers. Horton3 compares the experiences of caregivers to those of the residents. In a pathological care setting where elderly residents are lonely, caregivers feel isolated; when elderly residents feel bored, caregivers experience burnout; and ultimately all parties experience helplessness. Therefore, the three plagues for caregivers working in a residential care facility are isolation, helplessness and burnout.3Table 1 offers a breakdown of the three plagues for both residents and caregivers, with the suggested antidote for each plague6. The impact of boredom and burnout in particular are highlighted in this article.
The negative impact of institutionalisation on both staff and caregivers could be counteracted when PCC directs care practice.
Person-centred care in residential care
In contrast to the traditional model of care, a person-centred approach aims to combat the three plagues and enhance residents' quality of life6,11,12. In this approach, the patients are referred to as residents and they are the main role players in a homelike environment where caregivers facilitate the independence and growth of the residents. In this nurturing environment, the personhood of the residents is preserved; they are free to make choices; their preferences and individuality are the main focus; and medical treatment has a predominantly supportive function, only when needed. In a nurturing care culture, caregivers know the life stories of the residents and provide residents with the opportunity to give as well as to receive care. The strict routine of the traditional care model is replaced by variety and spontaneity.
Person-centred care facilitates the building of strong relationships between leaders and caregivers within an organisation. An important part of this approach is to break down the leadership hierarchy and create a decentralised view of leadership. This enables a nurturing environment where decisions are made in conjunction with the staff and residents; where the needs of the residents are priority6. Staff members in a nurturing setting report to each other and to residents, not to the leadership of the residential care facility. Person-centred care also allows for the development and empowerment of the caregivers and the opportunity to take initiative and to be creative6,13.
The caregivers are the persons with the most potential to have a constant impact on the lives of the residents, therefore they have the greatest capacity to impact on the residents' quality of life. When a residential care facility aims to advance PCC, authoritarian leadership styles should be replaced with leadership styles that support PCC principles14. This development is key to promote a nurturing care culture at an organisational level6.
Leadership
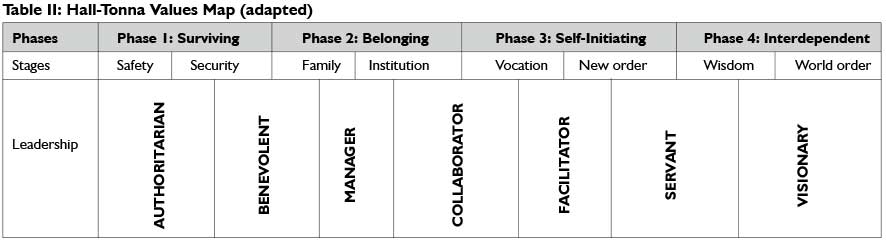
There is inadequate literature on the impact of leadership styles on person-centred care. However, the importance of motivation/ volition and values as part of life roles for growth and development is a well-documented occupational therapy perspective15. Hall and Tonna14 developed a map recognising the values of an organisation, its leadership and staff members. The map is based on theories of growth, volition and values that endeavours to link the association between leadership and nurturing environments16. See Table II.
The value map suggests four progressive phases of human development namely surviving, belonging, self-initiating and inter-dependence14. Surviving is seen as the most basic of the phases and interdependence as the most developed. Each phase is divided into two stages, with goals and means which represent the values of the particular phase. The phases are associated with seven leadership styles, also in progressive order: authoritarian, benevolent, manager, facilitator, collaborator, servant and visionary. The Hall-Tonna Values Map14 indicates that, in the context of residential care, the authoritarian leadership style correlates with goals and means that focus on the self, physical care and comfort. When the characteristics of PCC are compared with the values map, it is evident that the self-initiating phase aspires towards PCC. The values of this phase focus on community interaction, interpersonal relationships, working together, development, recognising individuality, and sharing responsibility. The leadership style associated mostly with the self-initiating phase is servant leadership. Therefore, servant leadership supports the principles of PCC. In order to achieve PCC, organisations should promote a servant leadership approach rather than enforcing a climate of dictatorial authority.
According to the Hall-Tonna values map, authoritarian leadership is the most basic form of leadership with a potentially rigid impact on the care culture of an organisation14. An authoritarian leadership approach implies that leaders take total control, their goals are aimed at their own instead of the organisation's benefit and that they are more focused on the task at hand than the people doing the work17. In essence, the authoritarian's motivation is aimed at the lower levels of Maslow's hierarchy of needs, namely, addressing personal physical needs of food, warmth, shelter and safety14,18.
At the other end of the leadership continuum is servant leadership14. The concept suggests that servant leaders are dedicated to the development of their followers to ensure that each follower reaches his/her full potential19,20. The impact of servant leadership on caregivers in a residential care facility implies that the leaders will be the mentors rather than managers - the servant leader persuades others rather than forcing them to do a certain task21. A mentoring relationship between the leader and the caregiver could ultimately serve as an antidote to isolation. If caregivers are included in decisions, they can take ownership of their work, because their opinions are valued21. Ownership would combat the plague of helplessness.
The servant leader could also explore the unique potential of each caregiver and assist in developing areas of strength and compensating for areas where the caregivers experience challenges21. The implementation of this principle could lead to the empowerment of caregivers19, serving as an antidote to feelings of burnout3.
The main focus of servant leadership is service to their followers; in return they expect their followers to extend this by serving others20,22,23. This implies that if the leadership of a residential care facility serves its caregivers, the caregivers will serve the residents. If the leadership practices PCC when dealing with the caregivers, the caregivers will serve the residents through PCC13.
Therefore, within the context of the Hall-Tonna Values Map14, servant leadership creates the potential for caregivers to build meaningful relationships with residents, limiting the plague of loneliness. Other potential benefits of servant leadership would be including residents in decision making, promoting resident-directed care and combating helplessness of the residents. The nurturing environment within such a care culture would discard strict routines, allowing variety and spontaneity based on real-life situations, thus eliminating feelings of boredom experienced by the residents.
METHOD
Problem statement
PCC programmes were individually designed to enhance the quality of life of residents with dementia and meant for the use by all care partners, especially caregivers, as they spent the most time with the residents.
Although most of the caregivers were perceived as dedicated to their work, PCC training attempts appeared unsuccessful to enhance quality of care.
Research question
This study explored the caregivers' pre-conceived ideas regarding person-centred care, occupational engagement and quality of life for people with dementia.
Objective
The objective of this collaborative research investigation was to describe the caregivers' pre-conceived ideas of occupational engagement, person-centred care and quality of life for people with dementia.
Research design
A mixed methods triangulation study design24 was used. The predominant focus of the study was qualitative in nature as eight staff members were interviewed at length to gain an understanding of their personal perspectives. The qualitative responses were then compared and contrasted with quantitative responses to determine the relationship between the two.
Sample
Eight (n=8) female caregivers who participated in the study were a comprehensive sample of all permanent caregivers working in the special care unit of a residential care home in the Free State. Purposive sampling ensures that all available resources are used regardless of the level of saturation and was therefore applicable to this study in order to give each of the caregivers a chance to voice their perspectives25.
The caregivers' ages ranged between 30 and 46. None had any formal training in the work expected of them. Six caregivers were Sesotho-speaking, one caregiver was Setswana-speaking and one caregiver was isiXhosa-speaking.
At the time of the study, these caregivers cared for a population that consisted of mainly Afrikaans and English-speaking residents between the ages of 40 and 96, with two Sesotho-speaking residents. There were 21 residents at the time of the study.
Data collection
Qualitative and quantitative data were collected simultaneously. The open ended questions used to collect qualitative data were posed directly after each participant's response to each closed-ended question. Two data sets were produced that were analysed separately and compared afterwards, a process true to the mixed methods triangulation design24.
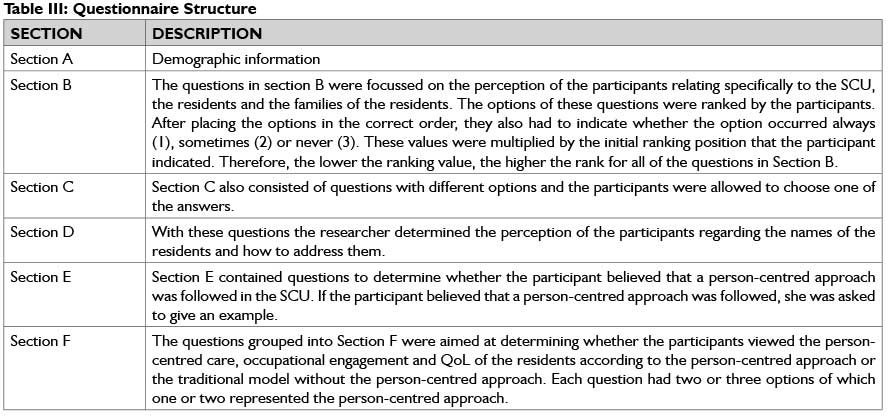
The structured interview questionnaire used for quantitative data collection contained sections focussing on demographics, perceptions of care quality and causes of aspects that enhanced or detracted from PCC. The structure of the questionnaire is summarised in Table III.
Data analysis
Qualitative
The interviews were recorded as audio-visual material, transcribed and member-checked. Observation was used to verify verbal and non-verbal messages of the caregivers24,26-27. Data were analysed and two co-coders were involved to enhance trustworthiness28.
After the data sets were read thoroughly and the coders were familiar with the content, the following process, described by Creswel129, was followed:
✥ Verbatim quotes were underlined and coded in the transcriptions.
✥ The codes were indicated on a separate diagram.
✥ The codes were clustered into categories.
✥ The categories were then clustered into themes.
✥ The coders also marked the responses of caregivers who spoke from first-hand experience to determine which pieces of data bore the most weight.
Quantitative
The quantitative data were analysed by the Department of Biosta-tistics, University of the Free State and produced frequency tables30.
Reliability and validity
Qualitative
Adequate time was spent in the interview to obtain rich data from the caregivers. A literature study was done on the situation of the caregivers, occupational engagement and quality of life to ensure that relevant questions were asked. Although all of the caregivers were fluent in Afrikaans, a translator was available to eliminate any language barriers that occurred. These measures ensured prolonged engagement during the interview.
Investigator triangulation was utilised as the two co-coders and the researcher independently analysed and interpreted the data from the interviews and observations. The process was repeated until the researcher and co-coders agreed on the results. The two co-coders were both occupational therapists who were chosen on account of their qualitative research experience, as well as their experience working with caregivers. Methodological triangulation24,31 was utilised and both qualitative and quantitative methods of study were followed. Observing and interviewing all the caregivers promoted data source triangulation.
Data were retrieved from audio-visual material and field notes. Both techniques ensured that contradictions between caregivers' verbal and non-verbal messages could be determined. An inquiry audit by a fourth expert addressed confirmability of the study. She reviewed the codes and themes established to confirm that the categorisation of the data reflected the transcript contents.28
Quantitative
To increase the reliability of the structured interviews, variables were clearly defined within the questionnaire design. Specific questions were used to measure each variable and a pilot study was done prior to the execution of the study to test the reliability of the interviews32. It was possible to determine the reliability of most of the questions on the interview schedule statistically, because of the nature of the items and the small study sample.
A thorough literature study ensured that all the aspects underlining PCC, occupational engagement and quality of life were included in the questionnaire. A pilot study contributed to the content validity. Triangulation of the data was used between Section B (relating to the perceptions of the caregivers regarding the special care unit, the residents and the family of the residents) and Section F of the structured interview questionnaire as similar themes emerged from the two sections33.
All the questions included were directly linked to PCC, occupational engagement and quality of life and/or aimed to establish a link between the two concepts. This factor enhanced face validity.
Upon completion of the interviews, the researcher engaged member checking. Each caregiver was provided with a copy of her completed questionnaire to confirm that the data was a just recording of her perceptions.
Ethical considerations
Approval to conduct this research was obtained from the Ethics Committee of the University of the Free State and the researcher obtained written consent from the managers and caregivers at both facilities for execution of the pilot and research phases of the study.
Pseudonyms were used to protect the participants' and other staff members' identities. The facilities and caregivers received feedback on the results of the study.
FINDINGS AND DISCUSSION
A comparison was made between the third plague for residents (boredom) and the third plague for caregivers (burnout) as indicated in Table 1. These problems are paralleled as antidotes for them are similar.
Boredom and burnout are the consequences of a life without creativity and growth. Both caregivers and residents are in need of challenges that living offers in every stage of life18. The findings and discussion focus on burnout and boredom to illustrate the importance of a change in leadership approach. Afrikaans quotes were translated to English. The number of the caregiver (e.g. C1) is indicated after each quote. Translations are also indicated (e.g. C1t).
Burnout
Burnout, as one of the three main problems for caregivers, is combatted when empowerment, education, emotional support and creativity are facilitated2.
Empowerment
The perceptions of the caregivers were that the organisation was in control and that they were not afforded the opportunity to take initiative. Feelings of disempowerment were recorded, "I would like the professional nurse to understand that I also know something about dementia and that my ideas will also be good for the patient." (C3t)
The caregivers mentioned that surveillance cameras were used in the special care unit. They were scared of being captured on camera while attempting new methods for which they could be criticised, "Yes, if there is a problem Sr. X goes to the camera and checks on you." (C1t)
The fact that the caregivers were afraid to try new methods when working with the residents was the predominant reason indicated from a list of eight that restricted them from facilitating independence of the residents. Furthermore, the organisation appeared to discourage new ideas by reminding caregivers of the possible negative consequences, "...every time you come up with a new idea, they will ask you: 'What if the patient gets hurt? Then you will have to take the blame." (C2t)
The organisational culture guides the behaviour of the caregivers and therefore the caregivers operate within the boundaries of that culture and are unlikely to take initiative6. Power2 states that the organisational structure in a residential care home often undermines and belittles the insight of the caregivers. This is the result of an authoritarian leadership approach that aims to take all control away from the caregiversI4. Chenoweth et al. 34 emphasise the importance of facilitating the learning of the caregivers in an environment where they are respected and not criticised. In contrast, the servant leadership approachI4 encourages caregivers to undertake stewardship, to be creative and to grow. The small efforts of caregivers to take initiative cannot be sustainable against the force of the organisation, unless the leadership mentors and encourages caregivers.
Education
Five of the caregivers working in the special care unit matriculated, two completed Grade II and one caregiver completed Grade 7. None had formal tertiary training.
Although caregivers did receive in-service training, one of the caregivers very strongly questioned the feasibility of the training. However, she indicated that some training was valuable to provide new knowledge. She valued the knowledge, but did not apply this knowledge practically, "... at the Alzheimer's training we learned how to work with people with Alzheimer's." (C7t)
"We try to do it in the unit. We cannot do everything, because sometimes the book says one thing and you cannot follow the book for everything, because those people are really difficult." (C7t)
The above findings are supported by the uncertainties of the caregivers as to how to analyse an activity to make it possible for the residents to participate in - this was ranked as the sixth most important reason for not facilitating independence.
It appears that caregivers were at an educational disadvantage in performing the complex job of caregiving. None were formally trained and although some of them believed that they did apply the principles of the in-service PCC training, they chose to do everything for residents within the set routine: "So we do, we do it for them so that we can knock off." (C3t)
Research confirms that deficient knowledge and perceived inadequate training could be a source of stress for caregivers and that dementia-specific training is one of the best ways to reduce stress for caregivers working with people with dementia34-35. Stress reactions of the residents cause low morale and a burden of care for caregivers, but can be counteracted by the provision of in-depth knowledge of dementia care35-39.
When the caregivers do not view what is expected of them as feasible, it causes feelings of powerlessness which adds to work stress40 and limited job satisfaction.41 Furthermore, Zimmerman et al. 42 report that trained caregivers are more prone to provide PCC. Watts43 confirms that the application of knowledge is a process that happens over a period of time and through a combination of formal training (including effective guidance from a mentor) and learning through trial and error. According to Du Toit and Surr,I staff should experience being treated in a person-centred way so they can experience the benefit thereof and apply it.
Therefore, it can be concluded that providing PCC to a residential care facility means a move towards a servant leadership approach that focuses on enhancing the knowledge and educational level of the caregivers.I4
Emotional support
The caregivers were of the opinion that they suffered under a very high workload caused by the understaffed facility and had insufficient time to perform their daily duties: "Sometimes we cannot even finish everything" (C7t). The high work load was given quantitative preference as evidence of why the caregivers did not facilitate independence of the residents.
The quantitative data indicated that the fact that caregivers had frequently been exposed to the death of patients meant that they did not want to become attached to the residents, and was the reason why they did not take initiative. The emotional burden caused by the death of the residents took their toll on the caregivers: .I loved that Oupa very much.the day when that Oupa.oh I was so heartbroken...I just prayed that it should pass." (C1t).
In spite of the heavy burden caused by the workload and the death of the residents, some caregivers believed that they were not allowed to experience work stress, "Now if you are working there, you are not allowed to have stress." (C5t). Therefore, it seemed that they suppressed their negative emotions in an attempt to control their stress levels at work, "Mmm, you may not say anything, you do not answer, you just keep quiet." (C1t).
Instead of being a source of emotional support for the caregivers, the organisation encouraged them to take 'mental health leave': "No, the professional nurse tells you, when you are very tired, to just phone and not come to work." (C5t).
Once again the qualitative data shows an authoritarian approach to leadership aimed at meeting physical needs as opposed to emotional needsI .Caregivers were deprived of the opportunity to share their emotions and experienced little emotional support from the organisation. If caregivers were to experience emotional support that eliminates burnout, it could enhance their relationship with the organisation and they would be more likely to provide emotional support to the residents. Emotional support is a priority of a servant leader and could eliminate the feeling of burnout14.
Creativity
The caregivers reported that the repetitive nature of care tasks led to boredom. In addition, the organisation did not afford the caregivers the opportunity to take initiative and to be creative. Quantitative evidence indicated that the lack of opportunity to be creative was an important reason why caregivers did not take initiative. The monotonous routine was a factor that caused stress and intensified burnout, "Yes, you do the work, one thing every day. You become tired of it." (C4t).
Literature supports the opinion that care can be monotonous, but also indicates how PCC could impact such situations positively. Repetitiveness of a job certainly has a negative influence on work stress40, but job satisfaction can be greatly enhanced by the application of PCC2. Therefore it is concluded that the controlling routine associated with authoritarian leadership14 should be replaced with a supportive environment that encourages creativity to prevent burnout of caregivers.
Boredom
Residents were influenced by caregiver burnout. This section of the results focusses on variety and spontaneity as the antidotes to the feeling of boredom for residents.6
Variety
Caregivers understood some of the positive benefits of activity participation. This was confirmed by the quantitative evidence that indicated that all of the caregivers recognised that meaningful participation in activities enhanced positive emotions. However, not only was activity participation not enforced by the organisation (activity participation was ranked least important on the priority list of the organisation), but the caregivers also felt that the organisation sometimes discouraged activity participation, ".because she wants it to be quiet". (C4t).
Literature confirms that the physical and psychological benefits of activity participation for residents with dementia are numerous,44 but that organisations often do not view this as a priority45. Stress reactions are reduced when each resident's individuality and life story are taken into account to meet their occupational needs46. Activities provide opportunity for success and enjoyment and decrease the development of unnecessary disability, thereby adding to general well-being47.
Organisations often neglect the right of the residents to participate in meaningful activities when they are physically cared forJ Power2 also confirms the low priority of activity participation for the caregivers and therefore states that they are prone to isolate the tasks that their job entails and perceive anything other than these tasks as an added burden. In addition to this, Anderson, Taha and Hosier48 report that the focus on tasks associated with physiological needs may be explained by the high demands on the caregivers in terms of the workload that results in the neglect of PCC, and in turn results in enhanced dependence of residents.
Spontaneity
It appeared that a strict routine was followed in the special care unit that allowed little spontaneity: "When you go to work, you get a certain, uhm, sequence to follow." (C3t). Caregivers further were of the opinion that the residents experienced fewer memory problems within a fixed routine:
"The other reason is that we do not want the residents to be exposed to different things too much, causing them to not remember." (C4t).
The actual events in the special care unit showed that the residents were bathed at 04:00 in the morning: this was not part of their routines before entering the residential care home. The caregivers reported that the strict routine that was followed was unrealistic, especially in terms of the time that the residents were expected to wake up in the morning: "Because they are woken so early, like four o' clock to wash, but then they must wait until eight o' clock to eat." (C8t).
Literature appears to favour a relaxed regime to support a more home-like environment for residents. Kada et al.49 found that 93.I% of caregivers were of the opinion that a firm routine is very important in dementia care as it may enhance memory. Many other authors, like Harmer and Orre150 and Power2, argue that a routine caters more for the needs of the caregivers and organisation rather than those of the residents; consequently, these routines and regimes often violate residents' needs. Hung and Chaudhury51 report that an unrealistic, inflexible routine takes away residents' control over their own actions and leaves them powerless and aggressive. Verbeek et al.52actually recommend that staff working in small care facilities should experience more independence and freedom in deciding the day's schedule. They should be allowed to plan the day according to the individual preferences of the residents; this in turn leads to the work being less challenging and strenuous as caregivers can then personalise the care. A less strict routine will make way for spontaneity that is essential to turn around the residents' feelings of boredom.
The quantitative data showed that the caregivers knew residents wanted to move around. However, the caregivers were of the opinion that one of their main priorities was to keep the residents safe and comfortable at all costs, a perception that diverted care-givers from allowing spontaneity: "No, I think as I have said I should take care of them so it is my duty to see if everything is okay with that patient, that she doesn't get hurt or she is safe and clean, neat." (C6).
Ayalon et al.53have found that caregivers believe more than any other profession that supervision and seclusion are important in providing effective care to people with dementia. Harmer and Orre150 stress that safety is a very high priority for caregivers. Data from Dementia Care Mapping research in South Africa presented evidence that the caregivers used tray tables as restrictions for up to six or more hours per day, which prevented independence and residents' need to move1. Being restricted makes residents feel powerless and disrespected as human beings51. Therefore, the focus of care should be on the person as a human being where PCC preserves the personhood of people with dementia1 rather than practices that encourage helplessness. It is important to note that the safety of the resident should always be a priority for any organisation, but it should not restrict the residents' opportunity to interact with the environment. Environmental adaptations should be made to accommodate the residents' needs.
Limitations
Despite the fact that all full-time caregivers at the facility were included in the study, the small sample size limits the relevance of the findings for other long-term care institutional settings. Future research should expand the topic and include more facilities.
CONCLUSION
The research focused on the caregivers' perceptions of occupational engagement, PCC and quality of life and revealed the restrictive impact of leadership approaches on PCC. A paradigm shift towards servant leadership could support PCC in residential care facilities and serve as the driving force to combat burnout of caregivers and boredom of residents. Although the impact of leadership in residential care homes needs more intensive research, servant leadership could potentially drive PCC and restore human dignity of the caregivers and the residents. Managerial leadership might not inspire PCC, but investment in the work force would reveal that any employee could be a leader.
REFERENCES
1. Du Toit S, Surr C. Wellbeing and person-centred care of people with dementia cared for in institutional settings in South Africa. World Federation of Occupational Therapists Bulletin, 2011; 63: 48-54. [ Links ]
2. Power GA. Dementia beyond drugs: changing the culture of care. Baltimore: Health Professions Press, 2010. [ Links ]
3. Horton JA. A model leadership curriculum for managers of an Eden Alternative nursing home. Master's Thesis. New Hampshire: University of New Hampshire, 2005. [ Links ]
4. Taylor R. The intentional relationship. Occupational therapy and the use of self. Philadelphia: F.A. Davis company, 2008. [ Links ]
5. Thomas WH. Life worth living: how someone you love can still enjoy life in a nursing home. Massachusets: VanderWyk and Burnham, 1996. [ Links ]
6. Eden Alternative. Haleigh's Almanac: Eden Alternative associate training manual. Eden Alternative, 2010. [ Links ]
7. Kitwood T. Cultures of care: tradition and change. In: Kitwood T, Benson S, editors. The New Culture of Dementia Care. London: Hawker Publications, 2000: 306-313. [ Links ]
8. Christiansen CH, Baum CM. Occupational Therapy: performance, participation, and well-being. Thorofare: Slack Incorporated, 2005. [ Links ]
9. Cutler CJ, Kane RA. Towards better quality of life: manual. Louis J Cutler & Rosalie A Kane, 2004. [ Links ]
10. Wilcock AAA. Occupation for health. British Journal of Occupational Therapy, 1998; 6I (8): 340-348. [ Links ]
11. Baldwin C, Capstick A. Tom Kitwood on dementia: a reader and critical commentary. New York: Open University Press, McGraw Hill Education. 2007. [ Links ]
12. Innes A, Macpherson S, McCabe L. Promoting person-centred care at the front line. Joseph Rowntree Foundation, 2006. [ Links ]
13. Yancer DA. Betrayed Trust Healing a Broken Hospital Through Servant Leadership. Nursing Administration Quarterly, 2012; 36 (1): 63-80. [ Links ]
14. Hall BP, Tonna B. "Hall-Tonna Values Map." 2004. England. < http://www.google.co.za/url?sa=t&rct=j&q=&esrc=s&frm=I&source=web&cd=I&ved=0CCsQFjAA&url=http%3A%2F%2Fwww.newcommglobal.com%2Fupload%2FVTHallTonna%2520Values %2520Map.DOC&ei=mKdeUsP5K4WSgfj0oCQDw&usg=AFQjCNEKE4iEbH7qy5KCSrESgAODuYadag&sig2-m-f3zUh6gYSrE-jaIXz7h4g > (16 October 2013) [ Links ]
15. Kielhofner G. Model of Human Occupation: Theory and Application. Philadelphia: Lippincott Williams & Wilkins, 2008. [ Links ]
16. Lewis-Shaw CP The Hall-Tonna Framework for Values Analysis: Aligning Individual and Organisational Values. Workshop conducted by for the Vocational Education and Training Research Conference. Melbourne 8-11 July 1997. [ Links ]
17. Warrick DD. Leadership styles and their consequences. Journal of experiential learning and stimulation, 1981; 3-4: 155-172. [ Links ]
18. Maslow AH. Motivation and personality. New York: Harper & Row Publishers, 1954. [ Links ]
19. Sendjaja S, Sarros JC. Servant leadership: It's origin, development, and application in organizations. Journal of Leadership & Organizational Studies, 2002; 2 (9): 57-64. [ Links ]
20. Whetstone TJ. Personalism and moral leadership: the servant leader with a transforming vision. Business Ethics: A European Review, 2002; 11 (4): 385-392. [ Links ]
21. Spears L. Reflections on Leadership. John Wiley & Sons: USA, 1995. [ Links ]
22. Neill M, Hayward KS, Peterson T. Students' perceptions of the interprofessional team in practice through the application of servant leadership principles. USA Journal of Interprofessional Care, 2007; 21 (4): 425- 432. [ Links ]
23. Stone AG, Russel FR Patterson K. Transformational versus Servant Leadership: A Difference in Leader Focus. Servant Leadership Research Roundtable. 2003; August: 1-10. [ Links ]
24. Ivankova NV, Creswell JW, Plano Clark VL. Foundations and approaches to mixed methods research. In: Maree K. editor. First Steps in Research. South Africa: Van Schaik Publishers, 2007: 253-282. [ Links ]
25. Strydom H. Sampling in the quantitative paradigm. In: De Vos AS, Strydom H, Fouche CB. and Delport CSL, editors. Research at Grass Roots. Pretoria: Van Schaik Publishers, 2011: 222-235. [ Links ]
26. Greeff M. Information collection: interviewing. In: De Vos AS, Strydom H, Fouche CB, Delport CSL, editors. Research at Grass Roots. Pretoria: Van Schaik Publishers, 2011:341-375. [ Links ]
27. Rubin HJ, Rubin IS. Qualitative interviewing: The Art of Hearing Data. Thousand Oaks: SAGE Publications, 1995. [ Links ]
28. Polit DF Beck CT. Essentials of nursing research: methods, appraisal, and utilization. Philadelphia: Lippencott Williams and Wilkins, 2006. [ Links ]
29. Creswell JW. Educational research planning, conducting and evaluating quantitative and qualitative research. Boston: Pearson, 2012. [ Links ]
30. Raubenheimer J. (2012). (Biostatistician at the University of the Free State). Personal communication regarding quantitative data. 26 April. Bloemfontein. [ Links ]
31. Padgett DK. Qualitative methods in social work research:challenges and rewards. Thousand Oaks: Sage Publications, 1998. [ Links ]
32. Neuman WL, Kreuger LW. Social work research methods: qualitative and quantitative approaches. Boston: Allyn and Bacon, 2003. [ Links ]
33. Delport CSL, Roestenburg WJH. Quantitative data-collection methods: questionnaires, checklists, structured observation and structured interview schedules. In: De Vos AS, Strydom H, Fouche CB and Delport CSL, editors. Research at Grass Roots. Pretoria: Van Schaik Publishers, 2011:171-205. [ Links ]
34. Chenoweth L, Jeon Y, Merlyn T, Brodaty H. A systematic review of what factors attract and retain nurses in aged and dementia care. Journal of Clinical Nursing, 2010; 19: 156-167. [ Links ]


{kind=link}
{kind=link}
{kind=link}