










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 no.2 Pretoria Ago. 2014
SCIENTIFIC ARTICLES
In-hand manipulation of children aged four and five-years-old: translation, rotation and shift movements, in Bloemfontein
Marieta VisserI; Mariette NelII; Juanne de VriesIII; Erina KlopperIII; Kabi OlënIII; Johanette van CollerIII
IMSc OT (Wits); Lecuturer, Department of Occupational Therapy, Faculty of Health Sciences, University of the Free State
IIM Med.Sc (UFS); Lecturer, Department of Biostatics, Faculty of Health Sciences, University of the Free State
IIIOccupational Therapy students, Department of Occupational Therapy, Faculty of Health Sciences, University of the Free State at the time the study was carried out
ABSTRACT
BACKGROUND AND AIM: Children are often referred to occupational therapy for deficits in hand function, specifically in-hand manipulation problems. There is however no standardised measurement instrument with age-related norms available that evaluates all in-hand manipulation components. The aim of the study was to describe the in-hand manipulation skills of a multicultural group of four- and five-year-old children in Bloemfontein.
METHODS: A quantitative, descriptive study that included 98 four and 97 five-year-old English-speaking children was conducted. An observation checklist was compiled from non-standardised activities and standardised tests published in the literature to cover all aspects of in-hand manipulation. Video footage of each child performing the activities was used to score the checklists
RESULTS: A total of 195 children participated in the study, with 98 (50.3%) in the four-year-old and 97 (49.7%) in the five-year-old groups. The following percentages of four-year-old children had successful task completion (without compensation): finger-to-palm translation 11.2%, simple rotation 29.6%, complex rotation 44.9%, complex rotation with stabilisation 13.3% and shift movements 68.4%. The following percentages of five-year-olds had successful completion (without compensation): finger-to-palm translation 22.7%, simple rotation 45.4%, complex rotation 46.4%, complex rotation with stabilisation 10.3% and shift movements 67.0%
CONCLUSIONS: Although the findings cannot be generalised to the SA population, they do contribute to the body of knowledge regarding the developmental trends of four and five-year-old children's in-hand manipulation, by indicating that both age groups do not have fully developed in-hand manipulation and use compensatory methods. The observation checklist developed for and used in this study does however provide a comprehensive, inexpensive and quick method to assess IHM
Keywords: in-hand manipulation; assessment instruments; rotation; shift; children; translation
INTRODUCTION
Occupational therapists play an essential role in the evaluation and treatment of children with deficits observed in everyday tasks such as writing, dressing and playing. These activities are dependent on good hand function, the components of which include the aspects of muscle strength, grips and grasps and the most complex skill, namely in-hand manipulation (IHM)1,2.
IHM is the "process of using one hand to adjust an object for more effective object placement, or release; the object remains in that hand and usually does not come in contact with a surface during IHM"3:35. If a child presents with IHM deficits, activities could be executed in a slower manner or with greater difficulty 4.
Evaluation of IHM in children has been done in terms of various observation checklists. Several researchers, such as Exner5,6, Case-Smith3,7 and Pehoski8 have conducted studies on IHM, but to date no standardised test has been developed that evaluates all aspects of IHM.1 As a result of the lack of norms regarding IHM, therapists are not aware of what can be expected of specific age groups in terms of IHM, causing difficulty with regard to accurate assessment and intervention planning. If IHM problems are not identified at an early age, further hand function deficits could develop and influence the child's function in daily activities such as in school, personal independence and play1.
The research presented here aimed to describe the IHM skills of a multicultural group of 195 four and five-year-old English speaking children in Bloemfontein. This study was conducted in 2011 by fourth year occupational therapy students. The aim of this study was not to develop a standardised assessment tool for IHM, but only to provide a foundation for further IHM related studies. The observational checklist developed for, and used in this study, did however provide a comprehensive method to assess IHM. It is inexpensive and quick to administer.
LITERATURE REVIEW
The following review of the literature gives a description of IHM and its development, its importance and finally the assessment of IHM.
Defining components of in-hand manipulation
In the literature, the components of IHM are described and grouped in different ways3,7,9. For the purpose of this research, the components of IHM are described and grouped as translation, rotation and shift movements1, and are defined below.
According to Versveld10, translation can be defined as the process of the thumb and index finger, or the thumb, index and middle fingers, moving in synchronicity in a certain pattern which can be either toward the palm or away from the palm. Two types of translation are recognised, namely finger-to-palm translation when an object is moved from the finger pads to the palm of the hand9 , and palm-to-finger translation which is the action of moving an object from the palm of the hand to the finger pads11.
Rotation is specifically required to shape a grasp, rotate an object positioned between the finger tips, and to turn an object over and over between the fingers12. There are two types of rotation. Simple rotation occurs when the thumb is used in opposition to the fingers to rotate an object. The object is usually rotated less than 180 degrees and the fingers act as a unit during this rotation11. Complex rotation is the process of rotating an object 180 degrees by using active thumb movements and differentiation between finger movements. Complex rotation can also be defined as the movement when an object is rotated around one or more of its axes and when isolated finger movements are required to move the object9.
Shift is the adjustment of an object in a slightly linear direction by using the finger pads11. Shift can be distinguished as simple shiftand complex shift movement. Simple shift is the movement of the thumb and all participating digits as one unit, while complex shift occurs when digits are repositioned on an object to move the object in a linear direction9.
In addition, Case-Smith1 states that all the above described components of IHM can be executed with or without stabilisation, which refers to the use of IHM skills while other objects are being stabilised in the palm of the hand.
The development of in-hand manipulation
Understanding the typical development of IHM skills is important in order to provide the occupational therapist with a foundation in the evaluation and treatment process. However, the comprehensive aspects of hand function, the development and assessment thereof, and aspects that could influence IHM (for example, motor control, the influence of environmental factors, and the contribution of extramural activities) will not be discussed since they fall outside the scope of this research.
Different variables related to the developmental trends of IHM are described in the literature, some of which were considered relevant for this study. These variables include the age at which each aspect of IHM emerges and is mastered1,5,9,13-15, the quality and control of these movements, the patterns of movement or methods used to manipulate objects5,9, the ability to use IHM skills with or without visual monitoring5, the normal inconsistencies5,9, the time required to complete the task9 and the possible gender differences5. For the purpose of this research, it was decided to focus on children aged four and five years, as these ages fall within the period of rapid IHM development7.
When reviewing IHM developmental milestones or the age at which each aspect of IHM emerges and is mastered, it was found that IHM usually develops over a period of time ranging from 12 months to seven years of age. Rapid development is usually noted between the ages of three and six years1,7. During the first six months of life, the infant lacks IHM skills13 with the development of finger-to-palm translation occurring between the ages of 12 and 15 months1. Between the ages of two and three years, the child is able to manipulate an object with one hand and stabilise the object with the other hand14, while at the age of three years complex rotation is developed15. Between three and five years of age, most children develop the requisites of rotation, shift and translation5. Finally, at the age of six years, IHM with stabilisation occurs1. The time required to complete the IHM task decreases, and the consistency and maturity of the methods used to manipulate the objects, increase9.
No statistically significant gender differences were found in the literature5,8, although it appears that boys had lower scores and seem to be more variable in their performance than girls of the same age5.
The importance of in-hand manipulation
There are functional implications if IHM does not typically develop in children. According to Case-Smith1, poor IHM skills have an impact on self-care skills in children of pre-primary school age, for example, adjusting eating utensils and finger foods in the hand4. Competence in fine motor skills such as IHM significantly influences the development of play in pre-primary children9,4,16. Impaired IHM in school children may cause difficulty with different grasps and problems with holding and manipulating a pencil and cutting with scissors thus influencing writing ability and other fine motor activities17.
The assessment of in-hand manipulation
Several IHM tests without norms2 have been published, such as the In-Hand Manipulation Test (IMT) by Miles Breslin and Exner6, the Test of In-Hand Manipulation (TIME) by Exner 3, the Test of In-Hand Manipulation (TIHM) by Case-Smith7, the Test by Pehoski et al8, and the Observation Protocol on In-Hand Manipulation and functional skill development by Humphry et al1 as well as Benbow's informal checklist2. Since not all of these have been through psychometric evaluation and none of them have published normative data, they provide only criterion related data such as that described by Case-Smith7, Exner5 and Benbow12, such as separating magazine pages using shift, picking up a crayon using complex rotation and unscrewing a bottle top using simple rotation. These observation activities do not include aspects of IHM such as stabilisation.
Pont et al.7 used Rasch modelling to examine the TIHM's construct validity, reliability and test-retest reliability and it was found to have evidence for adequate construct validity as well as excellent reliability7, which some of the other above-mentioned tests do not have. However, only criterion related scoring is available for the TIHM for example, time, drops, stabilisations, quality7. The results are used in several different ways to make suggestions about children's IHM skills.
While the TIHM demonstrated potential as a clinically useful assessment of IHM, critique on the test is firstly that it does not examine all aspects of IHM, but only rotation and translation with stabilisation. Secondly that it may have limited sensitivity to the performance of finger-to-palm and palm-to-finger translation and thirdly that the child is exposed to an unfamiliar task and only allowed one attempt to perform the task7,9.
The review of the literature indicated that there were no available IHM assessment instruments to evaluate all aspect of IHM. This combined with the lack of instruments with normative data present a gap in the outcome measures available for use in occupational therapy. Therapists are therefore unable to assess and determine deficits in IHM in specific age groups making intervention planning difficult. This has implications for evidence based practice as a therapist's clinical decision making processes may not be informed by research evidence as well as clinical experience.
A descriptive study of IHM can therefore be of great value in terms of the future development of age-related norms and the development of a comprehensive IHM assessment instrument.
METHODOLOGY
Study Aim
The aim of this study was to describe in-hand manipulation skills with regards to translation, rotation and shift movements to cover all aspects of in-hand manipulation in 4 and 5-year-old children, through the use of an observation checklist compiled by the researchers, from non-standardised activities and standardised tests published in the literature.
A quantitative descriptive study was conducted by using video footage and the observational checklist to describe the IHM of four-and five-year-old children in Bloemfontein, South Africa. Approval to conduct this research was obtained from the Ethics Committee of the Faculty of Health Sciences, UFS.
Study Population
The names of 63 registered pre-primary schools in the Bloemfontein area were obtained from Statistics South Africa and the Department of Education and included private and public schools from various socio-economic and cultural backgrounds.
Study sample
Of these 63 schools, 28 schools were included in the research. The remaining schools either did not fall within the inclusion criteria set for this research, did not agree to participate or had insufficient contact details. Written consent was received from the principals of the participating schools. The total number of four- and five-year-old children from each school was determined using the class lists. For the purpose of this research, the four-year-olds were defined as four years, zero months to four years, 11 months and 30 days, and the five-year-olds were defined as five years, zero months to five years 11 months and 30 days. A probability based, simple random sampling method was used to select a proportional sample (100 four and 100 five-year-old children) from these class lists. Firstly, the number of children to be sampled from each class was determined and then simple random sampling was done to identify the children needed for sampling. Schools were visited and notified regarding the names of the specific children selected for this research. An information leaflet, consent letter and a questionnaire were sent out to the 200 prospective participants' parents. A 100% return rate was ensured by doing the research in a team, excellent cooperation from the schools' personnel, parents and multiple visits to the schools.
The inclusion and exclusion criteria were based on the feedback from a parent questionnaire.
The inclusion criteria for this study were as follows:
The children had to:
1. Be aged four or five-years-old.
2. Have English as their language of education regardless of their home language and culture (a multicultural group of children).
3. Have attended a pre-primary school for at least one year.
4. Speak and understand English.
The exclusion criteria for this study were as follows:
The children:
5. Who had any physical, cognitive or emotional disabilities as a result of pathologies (e.g. autism, cerebral palsy and attention deficit disorder).
6. Whose parents had not given consent for participation in the study.
7. Who had not themselves given assent for participation in the study.
8. Who had previously received or who were currently receiving occupational therapy intervention for in-hand manipulation/ hand function difficulties.
This study was not expanded to include different language groups which would have ensured a representative sample of the South African population as the funding and allocated time to conduct this study was very limited. No funds were therefore available to be used for translators to assist in the execution of the research, which could have enabled the inclusion of different language groups.
Measurement tools
Firstly a parent questionnaire which included questions that enabled the researchers to include/exclude the appropriate sample of children for this study was compiled. The questions related to the child's pre-primary school history, language proficiency, health, development, and indications of any medical, developmental, behavioural, or scholastic concerns that could influence their performance in an IHM activity.
Secondly, the UFS Observation Checklist was developed as follows:
Several available IHM tests and non-standardised activities were investigated to ensure the inclusion of all the components of IHM in the measurement tool3,5,9,12. The Test of In-Hand Manipulation (TIHM) and non-standardised activities from Case-Smith7, Exner5 and Benbow12 were selected to form part of the measurement tool, which was then named the UFS IHM Observation Checklist.
The standardised test, the Test of In-Hand Manipulation (TIHM; nine-hole-peg board) by Case- Smith7 consisted of five tasks. During task 1, complex rotation was required from the children who were instructed to remove five dowels from the holes in the peg board, one at a time. Using their fingertips they then needed to turn the dowels 180°, replacing each in its original hole. Tasks 2 to 5 were finger-to-palm translation tasks that involved the children picking up as many pegs as possible within their palms and replacing them in the peg board.
Since the TIHM test does not include all the components of IHM, the following non-standardised activities from Exner5 and Benbow12 were added. These activities made use of three R2 (two rand) coins, a piggy bank and two dowels. During these activities, the children were instructed to:
(i) pick up two coins and place them one at a time into the piggy bank slot by using the thumb and index finger while holding the
other coin in the palm. This evaluated shift with stabilisation;
(ii) hold the coin horizontally and rotate the coin with the finger tips 180°, evaluating simple rotation; and
(iii) with two dowels placed on the ulnar aspect of the palm, to stabilise one dowel on the ulnar side of the palm while the other dowel was then moved to be rotated between the finger tips, to evaluate complex rotation with stabilisation. These activities were referred to as task 6 to 8 in the UFS IHM observation checklist.
The time taken for the execution of each of the eight tasks as a whole was recorded.
METHODS
Each school allocated a quiet, well-lit room equipped with a small plastic table and chairs. Two researchers were responsible for the assessment procedure at each school. One researcher was responsible for production of the video footage by means of a Sony Handy Cam DCR-SR 47 (digital zoom, 60X optical zoom) video camera, while the other researcher explained by demonstrating the test activities.
At the beginning of the evaluation session, the child was informed about the research and assessment procedures. The child agreed to participate by crossing the block on the assent form. This also gave an indication of the child's hand preference and pencil grasp, which was recorded on video footage and afterwards indicated on the observation checklist.
The assessment procedure consisted of two separate opportunities. The first opportunity was for practice purposes and to eliminate the possible variable of unfamiliarity influencing task performance7. The second opportunity was recorded on video footage for scoring purposes. The whole procedure took approximately 10 minutes per child. Afterwards, the child's execution of the tasks was scored and coded from the video footage, using the UFS IHM observation checklist.
Data Analysis
To ensure confidentiality, the checklist and video footage were matched and coded numerically. Descriptive statistics namely frequencies and percentages for categorical data and medians and percentiles for continuous data, were calculated. The data analysis for this paper was generated using SAS software (Copyright, SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC, USA). Data were analysed by the Department of Biostatistics, UFS.
RESULTS
From the 200 returned parent questionnaires, 195 children met the inclusion criteria and participated in the research. Ninety-eight (50.3%) children were four years of age, of whom 48 (49.0%) were male. Ninety-seven (49.7%) were five years of age, with 58 (59.8%) being male. With regard to hand preference, 85 (86.7%) of the four-year-old and 86 (88.7%) of the five-year-old children were right hand dominant. A functional pencil grip was observed in 67 (68.4%) of the four-year-old and 86 (88.7%) of the five-year-old children. A functional grip was defined according to Benbow12 as a pencil grip where an open web space was present, and included a tripod, quadruped and adapted grip.
Translation
Finger-to-palm translation (Tasks 2 to5)
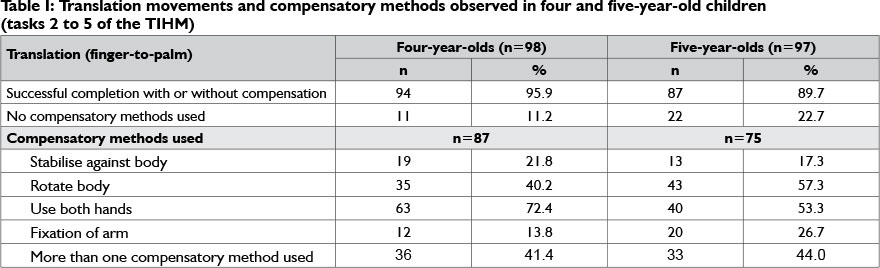
Table 1 indicates that slightly more ie 94 (95.8%) children in the four-year-old age group picked up five dowels with their fingertips than the five-year-old children (87 89.7%). More of the four-year olds (94.9%) than the five-year-old children (78.4%) were able to hold all five dowels in their palms. A similar number of the four-year-olds (50%) and five-year-olds (49.5%) dropped dowels while executing the task, with a median of one dowel stick being dropped.
The median period of time taken by the four-year-olds to complete the task was 43 seconds (range 26-96 seconds) and 39 seconds (range 22-75 seconds) for the five-year-olds. Executing the tasks without using any compensatory methods was achieved by 11.2% of the four-year-olds and 22.7% of the five-year-old children. The most common compensatory method was using both hands (72.4%) by the four-year-olds and (53.3%) of the five-year-olds. The five-year-olds rotated their body in compensation (57.3%).
Rotation
Simple rotation (task 7 of non-standardised measurements)
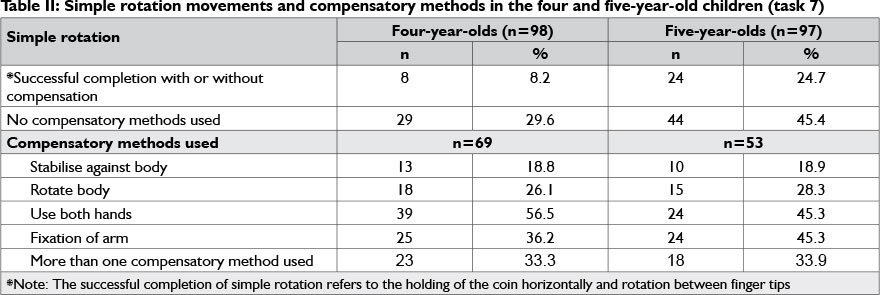
Table II shows that fewer children in the four-year-old eight (n=8 [8.2%]) than in the five-year-old group (n=24 [24.7%]) were able to hold the coin horizontally and rotate it between their fingertips. Of the children who completed the task successfully (with or without compensation), only about a third of the four-year-olds (29.6%) and slightly less than half of the five-year-old children (45.4%), did not use any compensatory methods. More than half (56.5%) of four-year-olds compensated by using both hands. This compensatory method occurred less frequently among the five- year-olds (45.3%). The five-year-olds (45.3%) also compensated by fixation of the arm.
Complex rotation (task 1)
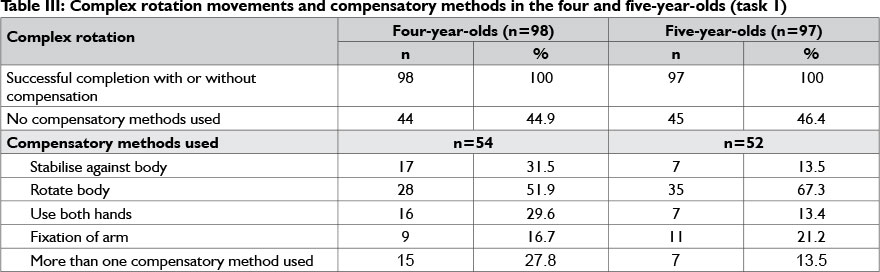
Table III shows that all the participants in both age groups could remove, turn and place the dowels successfully. Forty four (44.9%) of the four-year-old and 45 (46.4%) of the five-year-old children did not use compensatory methods. Fifteen (27.8%) of four-year-old and seven (13.5%) of the five-year-old children used more than one compensatory method to complete the task.
Complex rotation with stabilisation (task 8)
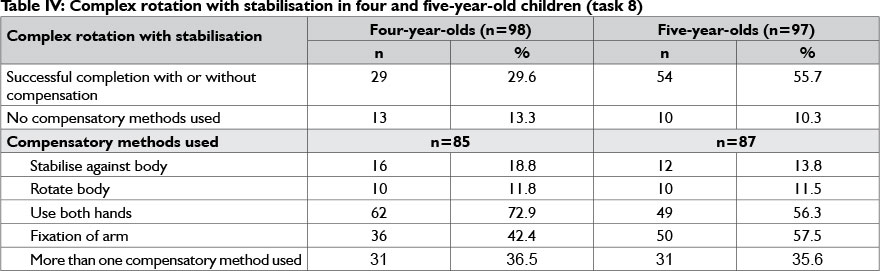
As shown in Table IV on page 26, 29 (29.6%) of the four-year-olds and 54 (55.7%) of the five-year-old children were able to rotate and stabilise the dowel. Of these successful attempts, 13.3% of four-year-old and 10.3% of five-year-old children were able to execute the task without using compensatory methods. The compensatory methods used the most were using both hands (72.9%) for four-year-olds and (56.3%) five-year-olds, while five-year-olds (57.5%) also used fixation of the arm.
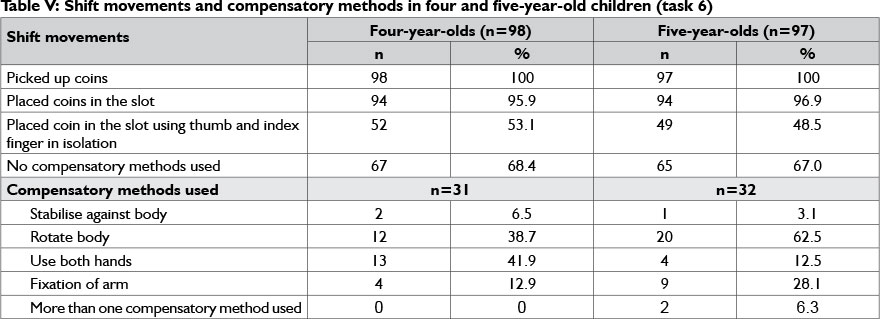
Shift with stabilisation (task 6)
Table V indicates that all the four- and five-year-old children were able to pick up the coins. Sixty-seven four-year-olds (68.4%) and 65 (67.0%) of the five-year-old children did not make use of any compensatory methods. The most common compensatory method used amongst the four-year-olds was using both hands (41.9%). The compensatory method most used amongst the five- year-olds was rotation of the body (62.5%).
Pencil grip
A functional pencil grip was observed in 67 (69.1%) of the four-year-old children and in 78 (87.6) of the five-year-old children.
DISCUSSION
To describe translation, rotation and shift movements involved in in-hand manipulation in four- and five-year-old children, it was important to observe whether the child was able to complete specific tasks4, how the child performed a task and whether any compensatory methods were used during task execution. It should also be taken in consideration that a 10 % difference in population size of males (48% males in the four-year-old group comparing to 58% of males in five-year-old group) could explain some unexpected differences between the results of the four- and five-years-old children. It could also be asked if the development of hand function in females is more advanced in this age category than males.
Translation
With regards to finger-to- palm translation, it was found that the majority (94.9%) of the four-year-old and (78.4%) of the five-year-old children, were able to successfully pick up the dowels, and hold all five in their palms. This observation indicated that finger-to-palm translation could be a skill mastered by most children in this age group, corresponding with research findings from Exner5.
A limitation of the study was that palm-to-finger translation was not recorded on the UFS IHM checklist. Palm-to-finger translation was however observed during the task of transferring the dowels to the peg board. Only a small number of children was able to execute the task without using compensatory methods. The compensatory method most commonly utilised, was the use of both hands. It was also noted that 50% of the four-year-olds and 49.5% of the five-year-olds (with or without using compensatory methods) dropped dowels while transferring them to the peg board. This could suggest that the four- and five-year-old children involved in this research had not yet fully mastered palm-to-finger translation. This corresponds with research regarding IHM developmental trends, done by Exner5 indicating that palm-to-finger translation is a more complex task than finger-to-palm translation. This greater difficulty is demonstrated by more frequent dropping of the dowels and the fact that these IHM skills are not fully developed until after 6 years.
Rotation
It was found that all of the four- and five-year-olds were able to successfully demonstrate complex rotation with 44.9% of the four-year-olds and 46.4% of the five-year-old children in this age group did not use compensatory methods. The children rotated their body when using a compensatory method. These findings do not correlate with Case-Smith1 who reported that children mostly make use of fixation of the arm as a compensatory method during rotation.
Complex rotation with stabilisation is a more difficult IHM skills6. This was confirmed in this study as only 29.6% of four-year-old and 55.7% of five-year-old children could successfully execute the task (with or without using compensatory methods). In addition, Case-Smith3 affirms that IHM tasks performed with stabilisation are more difficult than performing the same tasks without stabilisation, since tasks with stabilisation involve separate actions done simultaneously.
Simple rotation appeared to be the most difficult task as only 8% of four-year-old and 24% of five-year-old children could successfully execute the task (with or without using compensatory methods). A possible influence could have been the size and holding surface of the object being used to perform this task. Rotation of a coin with finger tips while holding it in a horizontal position is more complex than rotation of, for example, a plastic cup, which is a larger object with a larger holding surface.
Shift
According to Miles Breslin and Exner6 shift is apparently almost as difficult as complex rotation, (which is one of the most difficult skills). This was, however, was not true of this study, since 68.4% of four-year-old and 67% of five-year-old children could successfully perform the shift movement of placing the coins in the slot using thumb and index fingers in isolation without using compensatory methods.
The compensatory method most commonly occurring was rotation of the body and making use of both hands in comparison with Case-Smith1 who reported that during shift, children mostly use fixation of the arm as a compensatory method.
It could be concluded that children not using the thumb and index finger in isolation have poor shift movements. This deficit in shift movements could be as a result of poor palm-to-finger translation, as well as other hand function-related factors that have not been fully developed. It is, however, a complex skill, as stated by Miles Breslin and Exner6:44,"Shift must occur at the thumb and finger pads and requires use of intrinsic hand muscles in isolation from extrinsic hand muscles to produce well-controlled metacarpal-phalangeal flexion and inter-phalangeal extension".
Pencil grip
In a study comparing IHM skills in children with and without fine motor delays, it was found that 10% of four-year-old and 40% of five-year-old children used a dynamic tripod grasp (functional grasp)13. However in this study in the four- and five-year-old groups, functional pencil grip was observed in most of the children (while marking the assent form with an X or if able, writing their name). The task of holding the coin while placing the other coin in the slot of the piggy bank includes two different functions simultaneously. It involves stabilising on the ulnar side and movement of the radial fingers, which are components similar to those necessary for functional pencil grip. Far fewer children in both the four and five year old groups were able to complete the shift with stabilisation than had functional pencil grips.
LIMITATIONS
A limitation of this study was that palm-to-finger translation was not included in the UFS IHM observation checklist, although it was captured on video footage. However, due to time constraints it was not recorded on the checklist, analysed and included in the results.
A limitation of the observation checklist is that the tasks for simple rotation seem to be harder than the tasks for complex rotation.
Furthermore, the potential influence of recording video footage on the children's performance during the assessment and how it could have affected the results was not taken into consideration. Since the non-English speaking children in Bloemfontein were excluded from the study, the results cannot be generalised to the South African population.
RECOMMENDATIONS
The results from the study gave rise to a number of recommendations regarding future research as well as for clinical practice:
- Since rapid development of IHM skills and other related hand function components appears in young children, specifically in the four- and five-year-old age groups, it is recommended that smaller age increments of months rather than year, be used in future research
- Future research on the observation and description of children's IHM skills in a broader age range is needed in order to develop a standardised IHM assessment instrument for the South African context.
- It would be beneficial if the developed IHM assessment instrument could in future form part of a more comprehensive hand function assessment instrument.
- Critical review of the current UFS IHM observation checklist is recommended before it is used for future studies. For example, the use of various size objects (not only a coin) should be considered when assessing simple rotation.
- It is also recommended that occupational therapists using observation checklist/assessment instruments without age related norms (such as those discussed in the literature section) will use them with caution.
CONCLUSION
For children, in-hand manipulation is an important skill required for the execution of everyday activities. However, no standardised instrument has yet been developed to evaluate all aspects of IHM in South African children, making assessment and intervention planning difficult.
Findings reported in the literature outlined the different developmental trends of IHM. Some of these trends were reflected in the results of the current study, especially compensatory methods (a possible indication of the mastery level of IHM skill, method used and quality of the movements) as well as dropping of dowels (an indication of inconsistencies).
The research results contribute to the body of knowledge regarding the developmental trends of four- and five-years-old children's in-hand manipulation, by indicating that both age groups do not have fully developed in-hand manipulation and use compensatory methods. The four-year-old age group performed well in tasks of finger-to-palm translation and complex rotation movements. However, they had difficulty in tasks involving complex rotation with stabilisation and simple rotation, as well as shift movements. The five-year-old group performed well in tasks of finger-to-palm translation and complex rotation. Performance in tasks with complex rotation with stabilisation was noted to be average, and difficulty was experienced with tasks involving simple rotation and shift movements.
Although the findings cannot be generalised to the South African population, it is hoped that the results of this study will form a basis for further research as part of generating broader norms for hand-function amongst four- and five-years-old children and to develop a standardised instrument for assessment.
ACKNOWLEDGEMENTS
Dr. Daleen Struwig, medical writer, Faculty of Health Sciences, UFS, is acknowledged for technical and editorial preparation of the manuscript.
REFERENCES
1. Case-Smith J, O'Brien JC. Occupational Therapy for Children. 6th ed. Maryland Heights: Mosby Inc, 2010. [ Links ]
2. Occupational Therapy, Kids health information: In-hand manipulation. Available at www.rch.org.au/emplibrabry/ot/InfoSheet_D.pdf (Accessed 21 October 2010). [ Links ]
3. Case-Smith J, Pehoski C. Development of Hand Skills in the Child. Bethesda. The American Occupational Therapy Association, Inc, 1992. [ Links ]
4. Buckner KM. Fine Motor: In-hand Manipulation. 2006. Available at www.therapystreetforkids.com/fm-inhandmanip.html (Accessed 20 October 2010). [ Links ]
5. Exner CE. Clinical interpretation of in hand manipulation in young children: translation of movements. American Journal of Occupational Therapy, 1997 51: 729-732. [ Links ]
6. Miles Breslin DM, Exner CE. Construct validity of the In-Hand Manipulation Test: a discriminant analysis with children without disability and children with spastic diplegia. American Journal of Occupational Therapy, 1999; 53: 381-386. [ Links ]
7. Pont K, Wallen M, Bundy A, Case-Smith J. Reliability and validity of the Test of In-Hand Manipulation in children ages 5 to 6 years. American Journal of Occupational Therapy, 2008; 62: 384-392. [ Links ]
8. Pehoski C, Henderson A, Tickle-Degnen L. In-hand manipulation in young children: rotation of objects in the fingers. American Journal of Occupational Therapy, 1997; 51: 544-552. [ Links ]
9. Pont K, Wallen M, Bundy A. Conceptualising a modified system for classification of in-hand manipulation. Australian Occupational Therapy Journal, 2009; 56: 2-15. [ Links ]
10. Versfeld P Difficulties Children Experience with Hand Function. 2008. Available at www.ejbjs.org/cgi/content/abstract/90/11/2408 (Accessed 15 October 2010). [ Links ]
11. Murray-Slutsky C, Paris BA. Exploring the Spectrum of Autism and Pervasive Developmental Disorders. San Antonio: Therapy Skill Builders; 2000. [ Links ]
12. Benbow M. Neurokinesthetic Approach to Hand Function and Handwriting. Albuquerque: International Association for Continuing Education Training; 1995. [ Links ]
13. Bly L. Motor Skills Acquisition in the First Year. An Illustrated Guide to Normal Development. 1st ed. San Antonio: Therapy Skill Builders; 1994. [ Links ]
14. Mulligan SE. Occupational Therapy Evaluation for Children: A Pocket Guide. Philadelphia: Lippincott Williams & Wilkins; 2003. [ Links ]
15. Case-Smith J. Comparison of in-hand manipulation skills in children with and without fine motor delays. Occupational Therapy Journal of Research, 1993; 13: 87-100. [ Links ]
16. Kramer P Hinojosa J. Frames of Reference for Paediatric Occupational Therapy. 3rd ed. Baltimore: Lippincott Williams Wilkins; 2010. [ Links ]
17. Cornhill H, Case-Smith J. Factors that relate to good and poor handwriting. American Journal of Occupational Therapy, 1996; 50: 732-739. [ Links ]
18. Steyn C, Yerxa EJ. Test of fine finger dexterity. American Journal of Occupational Therapy, 1990; 44: 499-504. Q [ Links ]
 Correspondence:
Correspondence:
Marieta Visser
vissserMM@ufs.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}