










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 n.2 Pretoria Aug. 2014
SCIENTIFIC ARTICLES
Barriers and strategies to increase research involvement of South African occupational therapists
Hanlie Pitout
B OT (UP), M Occ Ther (Medunsa); Lecturer, Department of Occupational Therapy, University of Limpopo
ABSTRACT
Limited involvement in conducting and publishing research constitutes a threat to the occupational therapy profession. This article reports on the qualitative phase of a mixed methods study that aimed to explore the barriers to, and support for, South African occupational therapy research. Purposive sampling was used to identify 26 occupational therapists, with varying levels of research involvement, to participate in four focus groups. A further 12 individual, semi-structured interviews were conducted with participants with research publishing experience. Inductive reasoning identified four main themes: 1) challenges to research; 2) research education and motivation; 3) research process; and 4) research output. Factors influencing research involvement could be viewed either as a barrier or a support depending on an individual's view and circumstances. A need for both academic and clinical research, an occupational therapy research data base, scientific evidence, more knowledge and use of evidence based practice, more research skills development, streamlining the process, and more collaborative research was identified. South African occupational therapists should contribute to evidence creation through coordinated research participation and publication. A national research strategy is needed to address the identified barriers.
Key words: Research evidence based practice, research barriers
Introduction
Research evolves around the need for scientific evidence on which to base clinical practice, ownership of the knowledge base, raising the professional status, evidence - based practice (EBP) and keeping up with changes in practice1. "Competence in the role of the researcher is necessary because it contributes to the development of the individual therapist, the profession and the organisation in which the therapist functions"2:751. These developmental benefits can be derived from involvement in research through conducting a research project or using research findings for implementation of changes in clinical practice. Every occupational therapist needs to play a role in research3, whether it is applying research to practice (research consumer) or generating new knowledge through research (researcher or research leader). "Occupational Therapy is one profession where implementing research into practice to demonstrate its contribution to society is crucial for survival, yet the history of research within the profession might still be said to be in its infancy"4:253.
A review of the literature related to factors influencing research involvement, identified that lack of research involvement is a cause of concern in many professions and in many countries5-9. Studies have been conducted in the United States of America (USA)5, Australia6,7, United Kingdom8,9, Sweden10 and Canada11,12. The identified barriers in professions like medicine, psychology and nursing are similar to occupational therapy's, even though their professions are much older and the barriers included lack of time, funding and recognition8.
A national research strategy has been identified as important in support of research involvement. Countries that have played an important role in the development of the occupational therapy profession through substantial research outputs, such as the United Kingdom8,9, the USA5, Canada12 and Australia6, have national research strategies that involve occupational therapists directly. A national research strategy entails a coordinated effort to develop the infrastructure to support researchers, identify strategic priority research areas and make optimum use of the research initiatives that already exist5. Currently there is no national occupational therapy research strategy for South Africa. Although a national research strategy for health care in South Africa exists, it is more medically focussed e.g. on diseases such as HIV/AIDS and tuberculosis13. Occupational therapy has not identified its own research priorities or engaged formally with the national research strategy to determine whether occupational therapy research priorities are aligned with national priorities.
The limited research output of occupational therapists in South Africa has been highlighted14,15,16,17 but there is no empirical data about the current research involvement of occupational therapists or the barriers they experience. The quantitative first phase of the study18 revealed that only 32% (94/275) of all respondents had participated in research since qualifying. The research output was limited to 51% (48/94) that published and 64% (60/94) who gave oral presentations of their research. The majority (56%, 27/48), who had published had only published once. Fifty percent (18/36) of respondents with post graduate degrees had never published. Few undergraduate studies are published even though all final year students from the eight occupational therapy programmes (approximately 300 students per year) do a research project in their final year17. Lack of publishing undergraduate research may be due to the small sample sizes used in order to complete the research within the limited time available, students going to do community service, lack of expectations to publish, time taken to write an article, and/or lack of skills/experience in writing.
The profession has therefore lacked evidence to inform strategies to address the limited research involvement and publication. This study aimed to explore the barriers to, support for and strategies that may increase occupational therapists' research involvement.
METHODOLOGY
This article reports the qualitative second phase of a mixed methods study in which a qualitative descriptive design was used with purposive sampling to select participants for their views and opinions across the spectrum of research involvement. Participants included those with no research experience since qualifying; those currently doing research; and experienced researchers. Data were collected using focus group discussions and individual interviews.
Four focus groups, each with different participants, were conducted with a total of 26 participants. Criteria for inclusion in the focus group discussions were participation in phase 1 of the study, residing in Gauteng, willing to participate and able to meet at the identified venue. Data were collected until saturation was reached. An interview guide was compiled based on the findings of the quantitative phase of the study in order to explore the findings in greater depth (for more detail see addendum).
Twelve semi-structured individual interviews were conducted with participants who had published in the South African Journal of Occupational Therapy (SAJOT) in the previous four years and lived and worked in Gauteng in 2009. These interviews explored how participants overcame barriers to conduct and publish research. Questions included involvement in publishing occupational therapy research, to investigate why research is conducted but not published. Suggestions for improved research participation and publication were also elicited. Data were collected until saturation was reached.
Data were transcribed verbatim and analysed systematically according to the inductive reasoning process19. Transcribed data were re-read and reflected upon to identify themes and categories that emerged from this analysis. The constant comparative method20 was used to code data as a way of indexing and sorting the data. Themes and categories were identified through iterative (thematic) analysis.
Credibility and transferability were ensured by triangulation of findings from different sources, namely results of phase one and two of the study, literature, and peer review. Reflexivity was applied by the researcher noting her own perspective, position and assumptions. Dependability was ensured by using multiple persons and different groups, across situations (questionnaires, interviews and focus groups) over a six month period in 2009. The variety of participants contributed to the credibility as a range of perspectives from research experts to those with limited research involvement was obtained. Transferability was addressed further through thick descriptions with direct quotes illustrating conclusions and trian-gulation of data sources20.
Ethical clearance was obtained from the Medunsa Research and Ethics Committee. Participation was voluntarily and informed consent was obtained. Confidentiality was ensured by keeping consent forms and identifying data separately and giving respondents' pseudonyms during the analyses and recording.
FINDINGS AND DISCUSSION
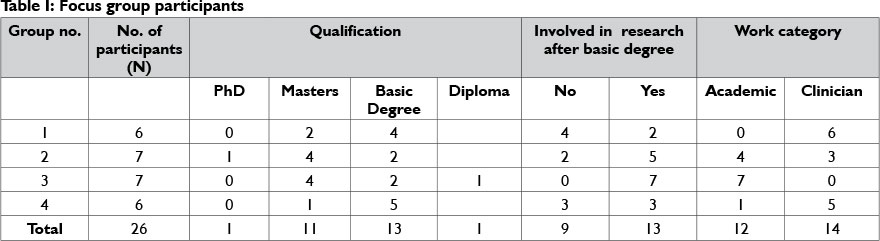
The profile of the 26 focus group participants and 12 individual participants is shown in Table I and II respectively.
Table III indicates the themes and categories that were identified. The findings are discussed in more detail under each theme and their categories, in the following section.

Theme 1: Challenges to research in the profession
Currently, research in South Africa is mainly done by academics and students (undergraduate and post graduate) and only rarely by clinicians. Although participants realised the need for research they experienced a discrepancy between research conducted by academics and clinicians' needs for evidence to inform their clinical practice. Three participants commented on the fact that academics and clinicians have a different understanding and needs with regard to research. Participants felt that
"Research done by academics lacks clinical application".
One explanation for the difference of opinion of research is the so-called "theory-practice divide" because clinicians see the theory that academics value, as inappropriate to practice, while academics experience clinicians as ignorant or resistant to theory21. Clinicians often abdicate their responsibility for research because they believe that someone else will do it, for example the academics, while they only need to be concerned with the treatment of clients1. In the profession we need both theoretical research to increase the scientific knowledge base of the profession and clinical research to improve intervention.
Optimising research capacity is hindered by the lack of an accessible, centralised data base with information on completed studies, studies in process and needs for further research. A database can help aspirant researchers to identify topics that have been researched already, and help prevent unnecessary duplication of research studies, as one participant explained:
"...research is scarce and the need for evidence is vast...".
The database will further contribute to the ability to do EBP as data from South African research studies would in many instances provide the best evidence for local clinicians. EBP is still relatively unknown worldwide and not easy for all clinicians to implement22,23.
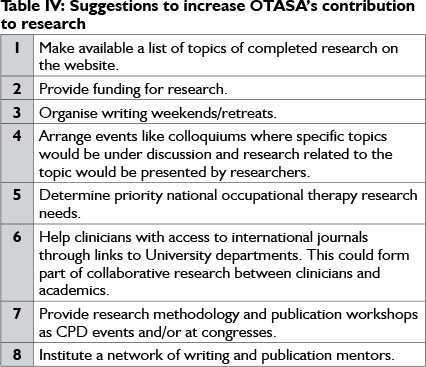
The Occupational Therapy Association of South Africa (OTASA) plays an active role in research through its publications (SAJOT and the Focus newsletter) and bi-annual congresses that provide opportunities to present research. Study participants provided suggestions to increase OTASA's contribution to research output as listed in Table IV.
Theme 2: Research education and motivation
Research education occurs mainly during undergraduate studies when students conduct their final year research project, which is a requirement stipulated in the Minimum standards of the World Federation of Occupational Therapy (WFOT)17. Effective methods of research education are widely discussed in international literature in both occupational therapy and other health disciplin es3,8,23,24,25,26,27,28,29,30. Education can include formal research short courses, mentorship, in-service training through participation in a research project.
Participants agreed that a passion for and appreciation of the importance of research needs to be fostered at an undergraduate level:
"A positive experience during the undergraduate research project will be sowing seeds for pursuing research after qualification".
Providing students with the opportunity to present their research and share their information was highlighted as a method to acknowledge, recognise and encourage students' research efforts.
Participants had conflicting opinions on the adequacy of their undergraduate research training to prepare them for conducting research after graduation. Participants who were experienced lecturers felt that knowledge was adequate, while lecturers with less experience, but who had started their own post graduate research, viewed their undergraduate level research education as 'insufficient'.Most clinician-participants expressed the view that
"Post graduate research does not come close to what you learned as undergrad. I don't think undergrad prepares you to do research properly when you get into the field. Doing post grad research is an enormous learning curve as undergraduate training did not prepare me adequately for independent research".
Although undergraduate research provides a starting point for research involvement, on-going development of research abilities need to occur after qualification through attending CPD activities and in-service training of novice researchers through collaborative research with an experienced researcher.
Participants highlighted that in previous years, very few South African occupational therapists obtained post graduate qualifications. Three participants indicated that recently there has been an increase in the number of younger therapists registering for post graduate studies e.g. at one local University they now have 90 post graduate students of whom almost half are doing research by dissertation and the others through a combination of research and coursework. This could mean as one participant explained that
"they have been successfully inducted into an academic culture".
An academic culture would include being inquisitive and knowledgeable about a subject area and interested in pursuing research. Other participants however interpreted the increase in post graduate registration as a symptom that
"Courses fail to provide sufficient training in undergraduate courses".
Participants indicated that for many occupational therapists the motive for doing post graduate degrees is to increase clinical knowledge rather than to do research. An increase in post graduate registration and qualification might increase research output. Obtaining a post graduate degree however does not translate into publishing the research as there is a tendency to 'down tools', meaning they do not continue with scholarly activities once the research study has been submitted for a degree and no publication of the study is attempted18. At some universities/institutions publication of research is not a prerequisite for obtaining a post graduate degree.
Intrinsic personal attributes that discern researchers include self-motivation, goal directedness, task orientation, perseverance, turning negative experiences into learning opportunities, a positive mindset and attitude towards research, ability to identify and access support, self-awareness associated with research and gratification from the research process1,2,7,22,23. Participants expressed disparate views about the compatibility of occupational therapists' personality with that of a researcher. For example, some felt that the important rigour necessary for research may be lacking. The impact of fear as a barrier5,26,27 to research should not be underestimated and it becomes important to be able to weather criticism.
Theme 3: Research process
The research process has some unique challenges including topic selection, time allocation, support and access to funding.
The difficulty in identifying an appropriate, researchable topic was highlighted. To refine an idea to a researchable topic requires, as one participant summarised:
"The topic must not be so big that you get de-motivated or overwhelmed by it and gain nothing, but also not too small that it becomes nonsensical".
There was controversy amongst participants regarding the best approach to topic selection. Some participants felt strongly that an individual must select their own topics, as
"Passion for the topic is the main drive for successful completion of the project".
One participant however indicated that in retrospect she believed
"with the funding and support embedded in receiving a topic for which funding has been allocated, I could develop passion for that topic".
Researchers often do not have sufficient knowledge and skills to understand the implications of topic selection
"One of the problems at the moment is that everyone is working on their own little research topic which does not contribute significantly to the overall progress in the profession".
Identifying and building Universities' research focus areas (niche) and informing potential researchers about it can contribute to topic selection and help to strengthen research capacity.
Lack of time could limit research output11,14,29,30. All professionals face many competing claims to their time and when there are personnel shortages and high patient workloads, personal priorities and the priorities of the employer will most likely determine where time will be spent31,32. In the Australian study of Cusick33, clinician-researchers in contrast to non- researcher clinicians, saw time for research as support and a privilege afforded to them. For occupational therapists in private practice time is directly linked to their income or as they indicated.
"I think in the private sector where people are very aware of time is money, if you don't see a client that costs money".
and
"It has been a bread and butter reality that I have had to put my time into billable hours".
Clinicians in the public sector also do research as an after-hours activity as they do not have time while handling their full workload.
The benefit of research may be promotions e.g. at Universities, or be of benefit in applying for a new job, but is rarely linked to monetary gains. Other participants though, pointed out that the doctors with whom they work,
"earn money for data collection which is paid to them over and above their salaries".
Monetary gains create a whole new perspective on research involvement and the time available for research, because with a monetary reward occupational therapists may be more amenable to become involved in research.
Often lack of funding is blamed for limiting research involvement. One participant argued that there are many research projects that can be executed with limited funding. Occupational therapists may investigate possibilities to link their research topics to a funded research project.
In the research process the availability of adequate support, research supervision and mentorship is important34,35. Research support groups have several benefits including providing mentors, peer support, accountability, provision of information and ideas, discussion about issues and problems and provision of opportunities for increased knowledge and personal development34.
Employers in clinical services tend not to be interested in research and do not provide any support or incentives for research and clinicians who pursue post graduate studies. The sad reality for a clinician trying to do research is
"...you receive almost no support from colleagues where you need support, or at least not to be negative, from management in clinical setting. Also need support from peers, and OTA's that must do work. You also need financial support, allowed time that can be used for research".
The benefits of collaboration in research were stressed by the participants and are supported by literature20,36,37,38,39. Benefits include access to resources, support34, sharing of ideas and using each collaborator's skills and strengths36. Participants mentioned their positive experiences in terms of collaboration with researchers outside the occupational therapy department. They indicated that their
"input was welcomed and they were praised for their research knowledge and skills".
One respondent cautioned that a partner for collaboration needs to be selected with care as
"a non-committed collaborator can cause loss of professional regard of those involved".
Collaboration between academics and clinicians can be used to assist clinicians to incorporate research into practice36,37,38,39. Through collaborative research academics can assist clinicians with access to ethical committees, literature resources, statisticians and even in-service training in research while academics will benefit from researching topics that are clinically relevant and gain easier access to clients.
Theme 4: Research output
Oral presentation may be easier than publication and could even be the first step towards publication. The majority of participants found oral presentation less threatening than publication.
Participants saw the publication process as one for which few occupational therapists seem to be prepared. The participants appreciated the importance of publishing their research.
"If research is not published it is a wasted effort".
Lack of writing skills and language abilities as well as not being a first language English speaker, are barriers that may make the publication process more daunting with
"scientific writing almost another foreign language altogether".
Although occupational therapists may publish in any national or international journal, SAJOT is the only accredited (recognised by the Department of Education) journal specifically for occupational therapists in South Africa. Publishing of the journal and the various tasks leading to publication are dependent on volunteers who are 'thinly stretched'. A journal editor, one of the individual participants, indicated that often occupational therapists give up when an article is returned.
"The road to publication is long and winding.but we need to disseminate the valuable information we possess to other occupational therapists and other disciplines"16:1.
RECOMMENDATIONS FOR INDIVIDUALS, THE PROFESSION AND PRACTICE
At an individual level, occupational therapists need to be made aware of the different levels of research involvement (research consumer, researcher and research leader) and challenge themselves to reach their own highest level of functioning in this regard3,18. Should this be on the level of consumer they need to use research to incorporate best evidence into their clinical practice through EBP More workshops on EBP may equip more therapists to incorporate EBP in their day-to-day functioning. Individuals with an interest in research could be recruited by researchers to collect data as part of an in-service training in research. Researchers with experience could be recruited, perhaps through OTASA, to become national research leaders who can lead large research projects that could provide significant results for the knowledge base of the profession. Centres of research excellence could then be established where aspirant researchers could be initiated into research for example at University departments.
For the profession through OTASA, the research committee can take the lead in establishing a national occupational therapy research database containing information on undergraduate, post graduate and independent research which will improve access to research information and avoid unnecessary duplication of studies. This committee should further investigate the viability of a national research strategy. A national research strategy would include identifying priority research topics, infrastructure and capacity building through addressing the suggested actions e.g. writing retreats. Coordination of research can include fostering and informing occupational therapists on University research focus areas. Infrastructure building may include access to research funding through collaborative research projects supervised and initiated by post-doctoral candidates, to provide in service training for aspirant researchers in clinical areas and to link academics and clinicians in collaborative research.
CONCLUSION
The need for local/South African research to supply evidence that can be used in occupational therapy practice is vast. All SA occupational therapists receive research education and most have the personal attributes to be a researcher. The research process and research publication were identified as challenges and strategies by the profession to address these barriers need to be investigated.
ACKNOWLEDGEMENTS
The researcher would like to thank all the participants for their input. This research project was done as part of my Masters degree in Occupational Therapy at the University of Limpopo, Medunsa Campus. A special word of thanks to my supervisor, Prof E. Shipham for her input in the research process and to Prof. U. McIntyre for her assistance with the data analysis. Thanks to Prof E Ramani, Prof J Frantz, Dr H Buchanan for their valuable input during the writing of this article.
REFERENCES
1. Seale J, Barnard S. Therapy Research: process and practicalities. Oxford: Butterworth Heinemann, 1998. [ Links ]
2. Abreu BC, Peloquin SM, Ottenbacher K. Competence in scientific enquiry and research. Am J Occup Ther, 1998; 52 (9): 751-759. [ Links ]
3. Eakin P Ballinger C, Nicol M, Walker M, Alsop A, Ilott I. College of occupational therapists; research and development strategy. Br J Occup Ther, 1997; 60 (11): 484-486. [ Links ]
4. Alsop A. Enhancing potential through Lifelong learning and Research, Chapter 17. In Practice and service learning in Occupational Therapy. Enhancing potential in context. Edited by Lorenzo, T., Duncan, M., Buchanan, H. & Alsop, A. West Sussex: Whurr, 2006. [ Links ]
5. Frontera WR, Fuhrer MJ, Jette AM, Chan L, Cooper RA, Duncan PW, Kemp JD, Ottenbacher KJ, Peckham PH, Roth EJ & Tate DG. Rehabilitation medicine summit: Building research capacity: Executive summary. Am J Occup Ther, 2006; 60(2): 165-176. [ Links ]
6. Thomas, Y Research: Do we know how well we are doing? Aust Occup Ther J, 2007; 54: 87. [ Links ]
7. Sturgess J, Fleming J. A survey about completing an honours degree and future occupational therapy career paths. Aust Occup Ther J, 1994; 41: 65-72. [ Links ]
8. Bannigan K, Boniface G., Dohert P., Nicol M. Porter-Armstrong A, Scudds R Priorities for Occupational Therapy Research in the United Kingdom: Executive summary of the POTTER Project. Br J Occup Ther, 2008; 71(1): 13-16. [ Links ]
9. Roxburgh M. An exploration of factors which constrain nurses from research participation. J Clin Nurs, 2006; 15(5): 535-545. [ Links ]
10. Kamwendo K, Tõrnquist K. Do occupational therapy and physiotherapy students' care about research? A survey of perceptions and attitudes to research. Scand J Caring Science, 2001; 15(4): 295-302. [ Links ]
11. Pain K, Hagler PWarren S. Development of an instrument to evaluate the research orientation of clinical professionals. Can J Rehab, 1996; 9: 93-100. [ Links ]
12. CAOT Position Statement: Research in Occupational Therapy, 2009. <http://www.caot.ca/default.asp?pageid=2348> (13 June 2013). [ Links ]
13. Department of Science and Technology. "SA National Research and Development strategy'. 2002. <http://www/SANational Research and Development Strategy> (10 Dec 2012). [ Links ]
14. Joubert R. Evidence-based practice: a critique based on occupational therapy within the SA context. SAJOT 2005; Sep, 35(2): 8-12. [ Links ]
15. Watson R, Buchanan H. Making our practice evidence-based. SAJOT 2005; 35(3): 14-19. [ Links ]
16. Leishman A. The long winding road to publication. SAJOT, 2003; 33(2): 1. [ Links ]
17. Du Toit S, Wilkinson A. Publish or perish: A practical solution for research and publication challenges of occupational therapists in SA. SAJOT, 2009; 39(1): 2-7. [ Links ]
18. Pitout, H. Research orientation of SA occupational therapist. SAJOT 2013; 43(2): 5-11. [ Links ]
19. Babbie, E. The practice of social research, 1 1th ed. Belmont: Thomson Wadsworth, 2007. [ Links ]
20. Corbin J, Strauss A. Basics of Qualitative Research: Techniques and Procedures for developing Grounded theory, 3rd edition. Los Angeles: Sage, 2008. [ Links ]
21. Steward B. The theory-practice divide: Bridging the gap in OT. Br J Occup Ther, 1996; 59(6): 264-268. [ Links ]
22. Dawes M, Summerskill W, Glasziou P Cartabellotta A, Martin J, Hopayian K, Porzsolt F, Burls A, Osborne J. 2005 "Sicily statement on EBP". http://www.biomedcentral.com/content/pdf/l472-6920-5-1.pdf (12 December 2012) [ Links ]
23. Corcoran, M. A busy practitioner's approach to evidence-based practice. Am J Occup Ther, 2006; 60(2): 127-128. [ Links ]
24. Rappolt S,& Tassone M. How rehabilitation therapists gather, evaluate, and implement new knowledge. J Contin Educ Health Prof, 2002; 22(3): 170-180. [ Links ]
25. Watson, R. & Buchanan, H. Making our practice evidence-based. SAJOT, 2005; 35(3): 14-19. [ Links ]
26. Love KM, Bahner AD, Jones LN & Nilsson JE. An investigation of early research experience and research self-efficacy. Professional Psychology-Research and practice, 2007; 38(3): 314-320. [ Links ]
27. Craik J & Rappolt S. Enhancing research utilization capacity through multifaceted professional development. Am J Occup Ther, 2006; 60(2): 155-164. [ Links ]
28. Ilott, I. The research assessment exercise: a personal SWOT analysis. Br J Occup Ther, 1997; 60(4): 167-168. [ Links ]
29. Stern P. Occupational Therapists and research: Lessons learned from a qualitative research course. Am J Occup Ther, 2001; 55(1): 102-105. [ Links ]
30. Ilott I. Challenges and strategic solutions for a research emergent profession. Am J Occup Ther, 2004; 58(3): 347-352. [ Links ]
31. Cusick, A. The experience of clinician researchers in occupational therapy. Am J Occup Ther, 2001; Jun, 55 (1):9-18. [ Links ]
32. Ballinger C, Pomeroy V, Melville H. Networking between therapists interested in research: How to set up a support group. Br J Occup Ther, 1994; 57(5), 185-187. [ Links ]
33. Grossmann, E. S. Research mentorship: remedial action required. SAJOT, 2002; 32(2):1. [ Links ]
34. Cusick A. Collaborative research: rhetoric or reality? Aust Occup Ther J, 1994; 41: 49-54. [ Links ]
35. Tse S, Lloyd C, Penman M, King R Bassett H. Evidence-based practice and rehabilitation: occupational therapy in Australia and New Zealand experiences. Int J Rehabil Res, 2004; 27(4): 269-274. [ Links ]
36. Brown GT. Collaborative research between clinicians and academics: Necessary conditions, advantages and potential difficulties. Aust Occup Ther J, 1994; 41: 19-26. [ Links ]
37. Lloyd C, King R, Basset H. Occupational Therapy and clinical research in mental health rehabilitation., Br J Occup Ther, 2005; 68(4): 172-176. Q [ Links ]
 Correspondence:
Correspondence:
Hanlie Pitout
Hanlie.Pitout@ul.ac.za
Appendix I
Interview schedule for focus groups
1. Introduction to research topic and preliminary results.
2. Focus group members share their own experiences of research: These serve as an ice breaker and also yield information on the crucial aspects that influence research orientation. This may also serve as a link to the following questions.
3. There seems to be a difference between what OT's belief about research and what they do. Most agree that research is important yet only a few do it. What is your explanation for this?
4. What do you see as the value of research for occupational therapists?
5. Can occupational therapists in South Africa do evidence-based practice? The participants are asked to make a list of barriers to and support for research.
They are asked to compare their own list to the list of barriers and support that was identified in Phase l and to try and arrange it in priority order.
6. Discuss the barriers to research that you identified and how you experience it
7. What support is available for research and how do you experience it?
8. Conclusion and wrap up.
Interview schedule for individual interviews
1. Can you please explain to me how you have been involved in publishing OT research?
2. Can you please explain to me over what period you have been involved in publishing OT research?
3. In my analysis of the results of the first part of the study I found that 80% of respondents have not published research even though 73% participated in research. Do you think that it is a common occurrence that research is conducted but not published?
4. What can be the reasons for the above mentioned?
5. The respondents indicated that they prefer to publish in the SAJOT. Is this also your experience?
6. Most of the respondents indicated that they did the research in collaboration. Would you say that this is also true from your experience?
7. Most of the respondents seem to have published only once. What do you think is the reason for this?
8. Do you have any suggestions for improving research participation amongst OT's in South Africa?
9. Do you have any suggestions for improving publication amongst OT in South Africa?


{kind=link}
{kind=link}