










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versión On-line ISSN 2310-3833
versión impresa ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 no.2 Pretoria ago. 2014
SCIENTIFIC ARTICLES
The prevalence of burnout amongst therapists working in private physical rehabilitation centers in South Africa: a descriptive study
Theresa Du PlessisI; Surona VisagieII; Gubela MjiIII
IBA Social Work, MPhil Rehab; Social worker - Life, The Glynnwood Hospital, Benoni
IIB.Sc Physiotherapy, M.Sc Rehab; Extra-ordinary senior lecturer, Centre for Rehabilitation Studies, University of Stellenbosch
IIIB.Sc Physiotherapy, M.Sc Rehab (UCT), PhD; Director Centre for Rehabilitation Studies, University of Stellenbosch
ABSTRACT
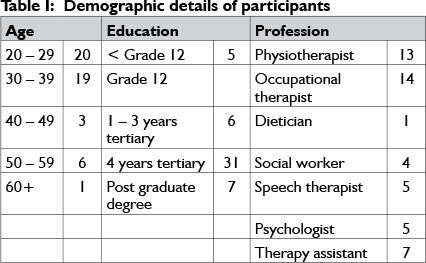
Health care service providers are at risk of burnout due to the nature of their jobs and their personalities. No research has been published on the prevalence and causes of burnout in therapists working in physical rehabilitation units in South Africa. This study aimed to determine the prevalence of burnout and identify causes in therapists working in physical rehabilitation in South Africa. A descriptive, quantitative study was done. Study participants comprised 49 therapists (14 occupational therapists, 13 physiotherapists, 7 therapy assistants, 4 social workers, 1 dietician, 5 speech therapists and 5 psychologists) from six private rehabilitation units in South Africa. No sampling was done. The prevalence of burnout was established with the Maslach Burnout Inventory Manual (MBI). Demographic and employment data were gathered through a questionnaire. MBI scores were categorised as high, moderate or low on the subscales of emotional exhaustion, depersonalisation and decreased personal accomplishment. The maximum likelihood and chi-squared tests were used for statistical analysis. A p value of <0.05 was deemed statistically significant. The prevalence of burnout was high: 57.14% suffered from emotional exhaustion, 20.40% from depersonalisation and 38.77% from decreased personal accomplishment. Not having children (p = 0.029), poor coping skills (0.031), an overwhelming workload (0.039),and poor work environment (0.021) had a statistically significant relationship with emotional exhaustion. An overwhelming patient load (0.012), seldom achievable deadlines (0.036), postponing contact with patients (0.02) and poor work environment (0.04) had a statistically significant relationship with depersonalisation. Male gender (0.023), not having children (0.038), less than four years of tertiary education (0.036), low income levels (0.022), high administration load (0.003) and postponing contact with patients (0.011) had a statistically significant relationship with personal accomplishment.Ensuring on-going support emotional support and job satisfaction of therapists is important if an institution is to provide continuing quality rehabilitation services.
Key words: Burnout, therapists, physical rehabilitation
INTRODUCTION
Due to the nature of their work health care service providers are at risk of burnout. However, research on the prevalence and causes of burnout amongst health care service providers in South Africa is scarce1. Those studies that have been done focussed on nurses practising in acute, public health care settings2,3. No South African study on burnout amongst therapists from a private or public health care setting could be found. The primary author of this article was employed as a social worker in a private physical rehabilitation facility in South Africa. She noticed that staff members often complained about stress in the workplace. She recognised some of the signs and symptoms of burnout in their complaints. Thus she embarked on the study to determine the prevalence and possible causes of burnout in private, physical rehabilitation units in South Africa.
LITERATURE REVIEW
The term 'burnout' is used to describe a state of physical and emotional exhaustion4. Burnout develops when an individual is exposed to chronic work stressors and frustration that exceed his/ her tolerance, and render his/her coping mechanisms ineffective4,5. It is encountered frequently among health care service providers, because of the chronic stress and emotionally challenging nature of their work4,5. Burnout presents a serious threat to an employee's health and working ability, with a negative impact on emotional, behavioural, physical and cognitive functioning6,7.
Burnout is said to have three components i.e. emotional exhaustion (EE), depersonalisation (DP) and lack of a sense of personal accomplishment (PA)8. Emotional exhaustion is usually the first phase of burnout and is characterised by feelings of tension and frustration. Employees feel drained on a psychological level9 and may withdraw from patients and persons linked with the work. Emotional exhaustion is often accompanied by physical exhaustion and signs and symptoms include lacking the energy to work or to treat patients, waking up tired after a night of sleep, psychosomatic symptoms, sickness, increased conflict in marital and family life as well as increased use of drugs and alcohol10.
Depersonalisation usually occurs after emotional exhaustion. This phase of burnout is characterised by cynical and negative feelings and attitudes about one's work and patients11. A dehumanised view of others can lead employees to view their patients as deserving of their problems8. Depersonalisation can lead to poor patient care, rudeness to and disinterest in the patients12. Decreased personal accomplishment is the final phase of burnout. The person views himself/herself in a negative light, especially in relation to his/ her patients11. People suffering from burnout may be disgruntled with their work achievements, competence and with themselves9.
Literature mentions the following factors as risk factors for burnout:
- A stressful work environment
- Lack of recognition and fair competitive remuneration
- Staff shortages
- Watching patients suffer
- Demands of patients
- Impaired communication with and support from management § Racism
- Limited heed of professional value
- Non-conducive psychological and physical environments
- Long work hours
- Increased responsibility
- Increased workload/task overload
- A lack of resources 1,2,13,14,15.
Health care service provision in South Africa is plagued by staff shortages, a complicated burden of disease, an overwhelmed, demoralised health system and service providers, a protracted, complex health transition process and insufficient leadershipl6, all factors that relate to the risks mentioned above. Thus health care service providers in South Africa might be at risk for burnout. Working in a rehabilitation unit as a therapist is particularly stressful and demanding since emotionally taxing interactions with patients and families are intrinsic to the work, the cumulative effects of which can contribute to the development of burnout17. In addition, therapists tend to be empathetic, idealistic, committed and altruistic l7. These very attributes, that are desirable in human service professionals, create a level of vulnerability that makes them highly susceptible to burnoutl7.
METHODOLOGY
The purpose of the study was to establish the prevalence of burnout, who is affected and what caused it. Therefore a descriptive, quantitative study was used. This methodology was chosen since a descriptive study can provide a "snapshot view of a single sample measured once"18:148 and quantitative methods allow the researcher to quantify numbers of people involved, in this instance, numbers of persons who suffer from burn out.
Study setting
In South Africa private, physical rehabilitation facilities provide acute rehabilitation for clients suffering from a variety of disabling conditions such as stroke, spinal cord injury and head injury. One of the major private hospital groups in South Africa19 owns rehabilitation facilities in various South African provinces. The group implements uniform fee structures, which means the daily tariff includes all professional services that patients may require. This tariff structure is beneficial to the rehabilitation process since it includes services like reporting, education of patients and families and team meetings. The health care team in the units comprised of a rehabilitation doctor, rehabilitation nurses and care givers, physiotherapists, occupational therapists and their assistants, psychologists, social workers, speech therapists and dieticians. Therapists' duties, other than treating patients, included administration, education to patients and families and attending meetings. Therapy staff worked to a large extent autonomously. The therapy team reported to the therapy manager who reported to the hospital manager.
At the time of the study in 2010, the group operated six rehabilitation units: two each in Johannesburg and Pretoria, one in Bloemfontein and one in Durban. The study was carried out in these six facilities.
Study Population
The study population consisted of all 54 people. This included the physiotherapists, occupation therapists, speech therapists, social workers, dieticians, psychologists and therapy assistants permanently employed at the six rehabilitation units at the time of the study. Since this was a small number no sampling was done. However, therapy staff members in temporary and locum positions were excluded, as were therapy staff who were on leave when the data were collected, since it was too costly to travel to the different units more than once. Forty nine people participated in the study (l4 occupational therapists, l3 physiotherapists, 7 therapy assistants, 4 social workers, l dietician, 5 speech therapists and 5 psychologists). Of the five who did not participate four were on leave and one declined to participate.
Study tools
The prevalence of burnout was established by means of the Maslach Burnout Inventory (MBI)8. The MBI has been used in various parts of the world to study burnout on various populations including therapists and is deemed a sound tool to use when measuring the prevalence of burnout20. The MBI has 22 items. Scoring is done on a seven-point scale ranging from zero ('never experienced such a feeling') to six ('experience such feelings every day'). Burnout is determined across three subscales i.e. emotional exhaustion (EE), depersonalisation (DP) and decreased personal accomplishment (PA). A number of studies which used factor analysis have supported the validity of the three-dimension composition of the MBI5. Dos Santos, Alves and Rodrigues assessed the MBI's reliability by applying the alpha Cronbach coefficient and found high levels of reliability for each of the three dimensions21.
Demographic information (age, gender, marital status and leisure activities) and employment-related information (profession, educational status, place of employment, years of employment, responsibilities and hours spent on various responsibilities) was gathered through a separate questionnaire that was developed by the primary author.
Data collection
A pilot study was done to determine if questions were clear and easy to understand and if the data gathered through them could answer the objectives of the study. The study tools were piloted with three locum therapists at one of the study sites. None of the participants in the pilot study formed part of the population for the main study. It took approximately fifteen minutes to complete the MBI. The participants did not experience difficulty in completing it, except that it needed to be explained that "recipients" mean patients in this instance. It took approximately fifteen to 20 minutes to complete the Demographic and employment questionnaire. Some questions were rephrased after the pilot study based on feedback from the participants.
Data were collected during 2010. A 'neutral' psychologist, with no direct authority over the participants, travelled with the primary author to the venues to administer and interpret the MBI. She contributed to the minimisation of response bias by stressing the importance of giving honest answers and by reassuring participants of the confidentiality of the results. She handed out the MBI. Participants completed it. She then checked each completed form as it was handed in to make sure that all items had been answered.
The psychologist scored the MBI by hand; scores were calculated for each participant and were categorised as high, moderate or low on the subscales according to the instructions provided by the MBI manual8. MBI scores and demographic data were entered in a spread sheet for statistical analysis and presentation. The maximum likelihood and chi-squared tests were used to determine if demographic and employment variables had a statistically significant impact on burnout scores. A p value of <0.05 was deemed statistically significant. Statistical analysis was conducted by a statistician from the University of Stellenbosch, Centre for Statistical Consultation using STATISTICA, Version 8.
Ethical considerations
The study was registered with the Committee for Human Research at the University of Stellenbosch. Written permission to perform the study was obtained from the hospital group. Participation was voluntary and written consent was obtained from all participants. In order to minimise the effect of individual opinions people might have on burnout on their scoring the MBI manual requires that participants should not be sensitised to the general issue of burnout and they must not be aware that the MBI is being used to determine burnout. The researcher could not follow this advice because it would have breached the principle of informed consent and she is aware that it might have impacted on results. However, it was not possible to determine if prior knowledge of the purpose of administering the MBI did have an impact on study findings and what that impact was. All information was treated as confidential. The participants' identities would not be disclosed to anybody at any time. Data were stored on a pass-word protected computer and data collection tools contained identification numbers, not names of participants.
RESULTS
Demographic profile of participants
Demographic details of the study participants are presented in Table 1. Participants consisted of seven (14.28%) males and 42 (85.71%) females. The majority (39; 79.59%) were between the ages of 20 and 39.
Prevalence of burnout
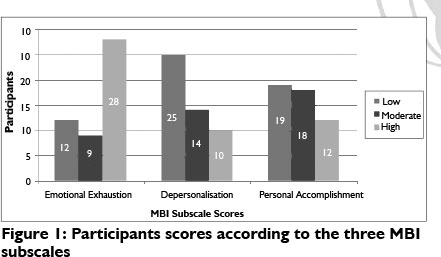
The prevalence of burnout amongst participants was high, with 57.14% (28) presenting with emotional exhaustion (EE), 20.40% (10) with depersonalisation (DP) and 38.77% (19) with decreased personal accomplishment (PA) (Figure 1).
Forty-one (83.67%) therapists had high levels of burnout in one of the three dimensions while one therapist (2.04%) had high levels of burnout in all three dimensions, and one therapist (2.04%) had low levels in all three dimensions.
Table II provides the mean, median and standard deviation for EE, DP and PA and the prevalence rate for each of the dimensions. The means and medians of DP and PA were both within average ranges, while the means and median for EE were in the high range.
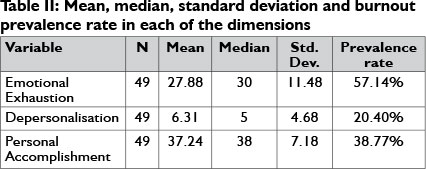
Table III provides a summary of demographic and employment variables which were found to have a statistically significant impact on the presence of burnout in one or more of the dimensions.

Three (42.86%) males and 25 (59.52%) females presented with high EE scores and one (l4.28%) of the males and nine (2l.43%) of the females presented with high DP scores. The majority of male therapists (5; 7l.43%) had low PA scores, whereas 14 (33.33%) of the females had low scores for PA. This difference was statistically significant (p = .02379). Gender had no statistically significant impact on EE (p =.50957) and DP (p = .67191).
Younger therapists had higher EE scores overall, with 13 therapists (65.00%) in the 20 - 29 year age group showing high levels of EE. Generally all age groups scored DP in the lower and average ranges. Older therapists experienced generally lower levels of PA with six of the seven therapists (85.71%) in the group older than 50 years scoring low in this area. Age did not have a statistically significant influence on any of the dimensions. However, a value of .05749 for PA indicated that older therapists might experience marginally lower levels of PA than their younger counterparts.
Twenty-nine (59.18%) of the therapists did not have children. A higher percentage of therapists without children (72.41%) experienced high levels of EE than therapists with children (35.00%). This difference was statistically significant (p = .02994). PA was also statistically significantly (p = .03895) impacted on by the absence of children. DP was not influenced significantly by whether therapists had children or not (p = .07413).
Lower levels of education had a statistically significant impact on burnout prevalence in PA with a p value of .03640, but not on EE (.24719) or DP (p = .75859).
In all professions, high levels of EE were found; notably for occupational therapists (9; 64.29%), speech therapists (3; 60.00%), psychologists (3; 60.00%) and physiotherapists (7; 53.85%). Reduced PA at levels indicative of burnout was experienced by 71.42% (five) of the assistants, 60.00% (three) of the psychologists and 50.00% (two) of the social workers. The majority of participants throughout all occupational groups had low DP scores. Occupation showed no statistically significant impact on the dimensions of burnout.
The majority (23; 46.93%) of therapists earned between R10 000 - Rl5 000 per month, with five (10.2%) earning less than R5 000 per month and five (10.2%) earning more than R15 000.00 per month. Fifteen (65.22%) members from the R10 001 - R15 000 income group experienced high levels of EE (although not statistically significant, with a p value of .51131). Earning less than Rl5 000 was statistically significantly associated with reduced PA (p = .02262). Income level had no significant impact on DP (p = .73019). Seventy-one per cent of participants felt that their salaries were not market-related. Although not statistically significant, more therapists who saw their salaries as not market-related scored within ranges indicative of burnout, than therapists who saw their salaries as market-related. Twenty one therapists (42.85%) were doing additional work to supplement their income. Of these 71.43% showed high levels of EE. Of the 28 therapists who were not doing additional work, 46.43% had high EE. This difference was only just not statistically significant, with a p value of .05866.
Most therapists (45; 91.83%) worked over weekends and public holidays. Weekend work had no statistically significant impact on EE (p = .4l554) or PA (p = .85497), but had statistically significant impact on DP (p = .02882). However, in this case it was the group that was not working over weekends that had the higher burnout prevalence in this category.
The majority of therapists (31; 63.26%) also worked overtime, but this showed no statistically significant impact on the three burnout dimensions. The number of hours of overtime worked showed no statistically significant impact on EE and DP, but did have a statistically significant impact on PA with a p value of .04521. Neither the number of days of leave taken nor the number of days sick leave taken had a statistically significant impact on any of the burnout dimensions.
Thirty-four therapists (34, 69.38%) viewed their coping mechanisms and skills at work as fairly good. The therapists who felt that they had either no or poor coping strategies and skills to deal with stress had the highest EE rate (100.00%) and this was statistically significant (p = .03180). Coping strategies, or a lack thereof, had no statistically significant impact on DP and PA. Most therapists (42, 86%) expressed confidence in their skills with l7(34.69%) feeling fairly confident and very competent (25; 51.02%). Job competency showed no statistically significant impact on any of the dimensions of burnout.
Workload included patient load, administration, research and meetings. On this issue the majority of therapists (35; 71.42%) felt their workload was either above average (18; 37.73%) or overwhelming (17; 34.69%). The group who felt their workload was overwhelming had the highest percentage of high DP scores (29.41%). An overwhelmingly high workload had a statistically significant impact on EE and DP, with p values of .03972 and .0l227 respectively, but not on PA (p = .15474). In addition, twenty-one (43.75%) of the therapists felt their patient load was above average and ll (22.91%) that it was overwhelming. A high patient load showed a statistically significant impact on EE (p = .02365) but not on DP (p = .09762) or PA (p = .11563).
Those therapists who carried high administrative loads - in some cases up to 75% of their daily duties had the highest EE (66.67%) and DP (66.67%) scores. More administrative duties per day showed a statistically significant impact on PA, with a p value of .00302, but not on EE or DP with p values of .7925l and .06898 respectively.
Two therapists, who felt their work deadlines, were always unreachable scored high in EE. The highest percentage (50.00%) of the group who felt they seldom had reachable deadlines scored high in DP (50.00%), while 70.00% of the group who felt that they always had reachable deadlines scored low in PA. Deadlines which are seldom achieved showed a statistically significant impact on DP with a p value of .03693, but not on EE or PA, with p values of .12866 and .19532 respectively.
The overwhelming majority of therapists (87.75%) never or seldom postponed contact with patients. All six therapists who often delayed treatment of their patients had high EE scores, and four of them also had high DP scores. Low PA was experienced by nine (45.00%) therapists who never postponed treatment and ten (43.48%) therapists who seldom postponed treatment. Postponing contact with patients correlated statistically with DP (p= .02023) and PA (p= .01164), but not with EE (p = .08633).
The majority of therapists (42; 86%) felt that their work environment was either fair (23; 46.98%) or good (19; 38.77%). The three therapists who rated their work environment as poor had high EE scores, as did 18 of the 23 (78.26%) who rated the work environment as fair. Low DP scores were found for 16 (66.66%) of the 24 therapists who rated their work environment as good or excellent. A poor work environment rating had statistically significant impact on EE (p = .02162 (EE) and DP (p = .04034), but not on PA (p = .21708).
Thirty four therapists (69.39%) felt that they received good or excellent support from their line managers. The four therapists who felt that support from their line managers was poor had high EE scores, as did eight (72.73%) of the 11 who felt support was fair and 13 (61.90%) of the 21 who felt support was good. DP scores showed that 20 (58.82%) of the 34 therapists who rated support from line management as good or excellent had low levels of DP On the other hand, eight (61.54%) of the 13, who felt that support was excellent, had low PA scores. Although support from line management showed no statistically significant impact on any of the burnout dimensions, with p values of .05380 (EE), .06350 (DP) and .32631 (PA), both EE and DP were close to the cut-off point of being statistically significant.
DISCUSSION
The prevalence of burnout was highest in the category of emotional exhaustion (EE) and lowest in depersonalisation (DP). This leads one to infer that less than a quarter of the therapy staff allowed their exhaustion to interfere with the way they treat their patients (for example, being indifferent and insensitive). However, burnout is regarded as a developing phenomenon and Innstrand et al. maintain that DP is the final phase to develop20. If that is indeed the case the therapists (if they remain in this environment) might progress towards depersonalisation. It is not possible to comment on whether prevalence of burnout impacted on the quality of patient treatment as measuring quality of treatment was not part of the study, but a 20% prevalence of DP might indicate reason for concern in this regard.
The prevalence of burnout was much higher for the current study population than in a population of South African trauma nurses, whose scores were EE = 16.53%; DP = 8.87%; PA = 33.42%12. This could be attributable to the difference in professions, as well as to differences in the type of work. Trauma nursing involves short, intensive periods of mainly physical contact with patients while rehabilitation involves longer periods of emotionally demanding contact. In another South African study, Sardiwalle et al did not give specific scores, but indicated that they found a high degree of burnout in a population of hospice workers22. Contact with terminal, hospice patients is also emotionally demanding. However, that environment does not include the added pressure of trying to achieve improvement against time deadlines, as a physical rehabilitation environment does.
Results from international studies done with therapists, show EE prevalence rates varying from eight to 60%6,17,23,24,25,26,27,28. When aligned with other studies the EE prevalence of 57% in the current study is the second highest. Studies by Schlenz et al.17 and Donohoe et al.23 were performed in settings similar to the current one. Although lower than in the current study, both these studies found high EE rates, at 42.5% and 46% respectively. This might be an indication that the nature of rehabilitation work plays a role in the development of EE.
Scores recorded in the literature for DP range between ten percent and 39%6,17,23,24,25,26,27,28. The DP scores were relatively similar, with most in the twenties, including that of the current study. None of the variables which impacted significantly on DP in any of the studies were similar to each other or to the current findings. This means that conclusions over specific contributing factors for DP could not be drawn.
PA scores varied between five and 60% and the current study showed the third highest PA score6,17,23,24,25,26,27,28. Low income level was the only variable found to impact significantly on PA in the current study, which was also mentioned as a cause of low PA in another study24. Additionally male gender was associated with decreased PA in the current study. It is possible that the decreased PA in this study can be attributed to the traditional role of the male being the breadwinner and the finding that six out of the seven male participants in the study felt that their salaries were not market related. In the Cypriot study by Pavlakis et al.24, 85.5% of participants felt they were underpaid and both EE and PA scores were statistically significantly associated with low salary.
A higher percentage of therapists without children experienced high levels of EE than therapists with children. Furthermore, the absence of children had a statistically significant impact on reduced PA. Parenting therefore seems to be a factor that could shield therapists against burnout. This was also found by Woodside et al.29 and Liakopoulou et al.30.
There is evidence in the literature that level of education might be associated with burnout31. In this study decreased PA was statistically significantly associated with less than four years of tertiary education. This group constituted mainly therapy assistants and because of a limited scope of practice and fewer opportunities to progress professionally they could have been frustrated in their work circumstances.
Poor coping skills and a diminished ability to deal with stress had a significant impact on EE. Sardiwalla et al.22, whose study fo-cussed on the role of coping strategies and stressors in burnout as experienced by hospice employees, found an association between poor coping strategies and EE, as well as DP.
The majority of therapists indicated that they had an above average or overwhelming work load (71.42%) and an above average or overwhelming patient load (66.66%). This was found to have a statistically significant impact on the development of EE, and, in the case of work load, there was also a significant impact on DP High workload, patient load and administrative duties are all variables which can cause time constraints. The negative impact of high workloads and time constraints on EE is also demonstrated in the literature25. A study by Girgis et al.28 that focused on Australian oncology health professionals found higher EE levels among participants who provided direct patient care. The authors felt that the emotional part of caring for critically ill patients plays a significant role in the exhaustion element but believed burnout may be related to an overload caused by high patient loads, rather than the patient contact per se. They found that time spent with patients had a positive effect on DP.
The majority of therapists (67.24%) in the current study spend up to 25% of their time on administrative duties. An increase in administrative duties was the variable with the strongest negative impact on the PA dimension of burnout. Literature agrees that burnout can be linked to a higher administrative load31,32,33. Shanafelt et al.33 found that when health care providers spent time on activities significant to them it decreases the risk of burnout. One can surmise that administrative duties are not that significant to therapists who by nature of their job choice show a need to interact with people. This supposition is further borne out by the finding that PA is the burnout dimension most negatively affected by the administration load. Another possible explanation for the administration burnout association in this study could be that participants had to do a lot of administration manually. They had no access to an electronic system which might reduce paperwork and prevent duplication. Report writing and accurate record-keeping are inherent and important functions of good clinical practice, but can be made less stressful through streamlined (e.g. electronic) procedures.
Sardiwalla et al.22 found positive correlations between EE and the physical work environment which indicated that employees who are more disgruntled with their work environment experience higher levels of burnout. These findings corroborate the current study's findings of a significant association between a poor work environment and EE. The current study also found a negative association between environment and DP which Sardiwalla et al.22 did not find. Private health care in South Africa is hailed as the flagship for health in the country34. It is also expensive and patients expect the best, given the money they pay. Crowded physiotherapy gymnasiums and outdated equipment do not live up to their expectations. Improvement in this area will decrease the risk for burnout in therapists while it can be used to advertise and boost the image of the company. It will also assist the therapy staff to provide more effective treatment.
DP was associated with not working over weekends, a finding which was the exact opposite of what was expected. Working fewer hours is normally associated with lower burnout levels4 and this finding is therefore difficult to explain. The authors could not find studies which specifically focussed on the association between weekend work and burnout. Further study is required to explore this association.
CONCLUSION AND RECOMMENDATIONS
The study provided information on the prevalence of burnout amongst therapist working in private rehabilitation in South Africa; a group for whom this type of information was not previously available. This study highlighted high burnout prevalence figures amongst therapy staff in a group of physical rehabilitation units in South Africa. These findings correlate with findings from other parts of the world and suggest that South African therapists working in physical rehabilitation units might be at high risk for burnout. However, findings cannot summarily be extrapolated to all therapists working in physical rehabilitation units and services since units and services differ. Recommendations for further research thus include the need to perform a similar study in government physical rehabilitation institutions. However, the authors want to postulate that figures would be similar - or even higher - as a comparative study in South African nurses indicated that nurses in government service experienced more frustrations and job challenges than those in the private sector35. This might be true for therapists as well, since govern- ment health care in South Africa is under more pressure than private health care due to staff shortages, managerial challenges and health care reform16. A further recommendation is the need to explore the impact of burnout, and depersonalisation specifically, on the quality of patient care in the rehabilitation context.
Therapists play a pivotal role in rehabilitation of clients with physical disabilities. Ensuring on-going support of their emotional health and job satisfaction is of utmost importance if an institution is to continue to provide rehabilitation services of quality. It is essential that employers, managers, and employees work together to address modifiable causes such as educational levels, income, coping skills, size of workload, time constraints and the work environment, through proactive implementation of policy and strategies to prevent and manage burnout. The workload of therapists must be evaluated and aligned to manageable proportions. A formula to calculate workload objectively and weight patient contact time, administration time, research and personal development will assist with equitable distribution of workload. Opportunities and support for continuing professional and personal development must be provided. Such an investment in human resources is likely to bear future fruit for employers and clients.
REFERENCES
1. Cohen M, Gagin R. Can Skill-Development Training Alleviate Burnout in Hospital Social Workers? Social Work Health Care, 2005; 40(4): 83-97. [ Links ]
2. Van Wijk C. Factors Influencing Burnout and Job Stress among Military Nurses. Military Medicine,1997; 162: 707-710. [ Links ]
3. Spies J. The relationship between occupational stressors, occupational stress and burnout among trauma unit nursing staff. Masters thesis. University of Pretoria, Faculty of Health Sciences; 2004. [ Links ]
4. Mandy A, Sacter M, Lucas K. Burnout and self-efficacy in Norwegian physiotherapists.International Journal of Therapy and Rehabilitation, 2004; 11(6): 51-258. [ Links ]
5. Flaherty M. Battling burnout: Health Professionals are at high risk. [http//www.sandyewing.com/Press-Room/Monster-Interview.html]. (1 Aug 2011) [ Links ]
6. Scutter S, Goold M. Burnout in recently qualified physiotherapists in South Australia. Australian Journal of Physiotherapy, 1995; 41(2): 115-118. [ Links ]
7. Hãtinen M, Kinnunen U, Pekkonen M, Aro A. Burnout Patterns in Rehabilitation. Short-Term Changes in Job Conditions, Personal Resources, and Health. Journal of Occupational Health Psychology, 2004; 9(3): 220-237. [ Links ]
8. Maslach C, Jackson SE, Leiter MP Maslach Burnout Inventory Manual, Third Edition. Mountain View, California: CCP; 1996. [ Links ]
9. Muscatello MRA, Bruno A, Carroccio C, Cedro C, Torre DL, De Rosa AE, Zoccali R 2006. Associations between burnout and anger in oncology versus ophthalmology health care professionals. Psychological Reports, 2006; 99: 641-650. [ Links ]
10. Lloyd C, King R. A survey of burnout among Australian mental health occupational therapists and social workers. Soc Psychiatry Psychiatr Epidemiol, 2004; 39: 752-757. [ Links ]
11. Schaufeli WB. Burnout in health care, in Carayon, P (ed). Handbook of human factors and ergonomics in health care and patient safety. Mahway: New Jersey: Lawrence Erlbaum Associates. 217-232; 2007 [ Links ]
12. Jeanneau M, Armelius K. Self-image and burnout in psychiatric staff. journal of Psychiatric and Mental Health Nursing, 2000; 7: 399-406. [ Links ]
13. Hall EJ. Nursing attrition and the work environment in South Africa health facilities. Curationis, 2004; 28-36. [ Links ]
14. Rothmann S, Van der Colff JJ, Rothmann JC. Occupational stress of nurses in South Africa. Curationis, 2006; 29(2): 22-33. [ Links ]
15. Rouleau D, Fournier P Philibert A, Mbengue B, Dumont A. The effects of midwives job satisfaction on burnout, intention to quit and turnover: A longitudinal study in Senegal. Human Resources for Health, 2012; 10:9. [ Links ]
16. Kautzky K, Tollman SM. A perspective on Primary Health Care in South Africa. South Africa Health Review. Health Systems Trust. 2008. [ Links ]
17. Schlenz KC, Guthrie MR, Dudgeon B. Burnout in Occupational Therapists and Physical Therapists Working in Head Injury Rehabilitation. The American Journal of Occupational Therapy, 1995; 49(10): 986-993. [ Links ]
18. Domholdt, E. Rehabilitation research: Principles and applications. 3rd ed. Missouri: Elsevier Saunders. 2005. [ Links ]
19. Matsebula T, Willie M. Private Hospitals. Health Systems Trust, South African Health Review. 2007. [ Links ]
20. Innstrand ST, Espnes GA, Mykletun R. Burnout among people working with intellectually disabled persons: a theory update and example. Scand J. Caring Sci, 2002; 16: 272-279. [ Links ]
21. Dos Santos FE, Alves JA, Rodrigues AB. Burnout syndrome in nurses in an Intensive Care Unit. Einstein, 2009; 7(1) 58-63. [ Links ]
22. Sardiwalla N, Van den Berg H, Esterhuyse KGF. The role of Stress-ors and Coping Strategies in the Burnout Experienced by Hospice Workers. Cancer Nursing, 2007; 30(6): 488-497. [ Links ]
23. Donohoe E, Nawawl A, Walker L, Schindler T, Jette DU. Factors Associated With Burnout of Physical Therapists in Massachusetts Rehabilitation Hospitals. Physical Therapy, 1993; 73(11): 750-756. [ Links ]
24. Pavlakis A, Raftopoulos V, Theodorou M.Burnout syndrome in Cypriot physiotherapists: A national survey. BMC Health Services Research, 2010; 10(63): 1-8. [ Links ]
25. Kowalski C, Driller E, Ernstmann N, Alich S, Karbach U, Ommen O, Schulz-Nieswandt F, Pfaff H. Associations between emotional exhaustion, social capital, workload, and latitude in decision-making among professionals working with people with disabilities. Research in Developmental Disabilities, 2010; 31: 470-479. [ Links ]
26. Ogiwara S, Hayashi H. Burnout amongst Physiotherapists in Ishikawa Prefecture. J.Phys.Ther.Sel, 2002; 14(1): 7-13. [ Links ]
27. Gulalp B, Karcioglu O, Sari A, Koseoglu Z.Burnout: Need help? Journal of Occupational Medicine and Toxicology, 2008; 3: 32 -37 [ Links ]
28. Girgis A, Hansen V, Goldstein D. Are Australian oncology health professionals burning out? A view from the trenches. European Journal of Cancer, 2009; 45: 393-399. [ Links ]
29. Woodside JR, Miller MN, Floyd MR, McGowen KR, Pfortmiller DT. Observations on Burnout in Family Medicine and Psychiatry Residents. Academic Psychiatry, 2008; 32(1): 13-19. [ Links ]
30. Liakopoulou M, Panaretaki I, Papadakis V Katsika A, Sarafidou J, Las-kari H, Anastasopoulos I, Vessalas G, Bouhoutsou D, Papaevangelou V Polychronopoulou S, Haidas S. Burnout, staff support, and coping in Paediatric Oncology. Support Care Cancer, 2008;16: 143-150. [ Links ]
31. Gutiérrez JLG, Rodriguez RM, Puente CF? Costa NA, Recio LA, Cerro P, Cuadros JA. Burnout in occupational therapy: an analysis focused on the level of individual and organisational consequences. Psychology in Spain, 2004; 8(1): 98-105. [ Links ]
32. Lee FJ, Stewart M, Brown JB. Stress, burnout, and strategies for reducing them: What's the situation among Canadian family physicians? Canadian Family Physician, 2008; 54: 234-235. [ Links ]
33. Shanafelt TD, West CP Sloan JA, Novotny PJ, Poland GA, Menaker R, Rummans TA, Dyrbye LN. Career Fit and Burnout Among Academic Faculty. Arch Intern Med, 2009; 169(10): 990-995. [ Links ]
34. Harrison S, Bhana R, Ntuli A. South African Health Review. Health Systems Trust, 2007. [ Links ]
35. Pillay, R. Work satisfaction of professional nurses in South Africa: a comparative analysis of the public and private sectors. Human Resources for Health, 2009; 7: 15. [ Links ]
 Correspondence:
Correspondence:
Theresa du Plessis
mjduplessis@mweb.co.za

