










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versión On-line ISSN 2310-3833
versión impresa ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 no.2 Pretoria ago. 2014
SCIENTIFIC ARTICLES
Patterns of sensory integration dysfunction in children from South Africa
Annamarie van Jaarsveld
M.OT (UFS); Head, Dept of Occupational Therapy, Faculty of Health Sciences, UFS
ABSTRACT
While patterns of sensory integration (SI) function and dysfunction have been studied in the US for more than 50 years exploration of whether or not similar patterns exist in cultures and communities outside of that country has been limited, with no studies conducted in South Africa to date. The purpose of this study was to investigate and describe the similarities and differences of patterns of SI dysfunction between children in South Africa and those in the US. A quantitative, analytical study was conducted on a convenience sample of 223 children who were identified as experiencing sensory integration difficulties. The Sensory Integration and Praxis Tests (SIPT) were used as the measuring instrument and correlation and factor analyses were applied in order to describe similarities and differences. Consistencies in tests loading on patterns of Visuodyspraxia, Somatodyspraxia, Bilateral Integration and Sequencing dysfunctions and Tactile and Visual Discrimination dysfunctions were found. Therefore, this research confirmed similarities in the patterns of dysfunction in children in South Africa and confirmed the value of the SIPT in identifying sensory integration dysfunctions cross-culturally.
Key words: Sensory integration, patterns of dysfunction
INTRODUCTION
Two pertinent questions are related to sensory integration (SI) in South Africa. Firstly, how relevant is it to use a measuring instrument that was developed and standardised in a first world country on children growing up in a developing country? Secondly, how do the patterns of sensory integration (SI) dysfunction in children from a country, such as South Africa (SA) compare to those of children from a first world country? Are there similarities or differences in the types of SI dysfunctions that children experience due to the fact that they grow up in different environments, contexts, lifestyles and with diverse resources? Patterns of SI dysfunctions currently researched and described in the literature are those of children growing up in a first world country and mostly in the United States (US)1,2,3,4.
REVIEW OF THE LITERATURE
Sensory integration function and dysfunction were first described by A. Jean Ayres in the late 1950's her legacy of theory and research is still expanding. This body of knowledge, now recognised as Ayres Sensory Integration® (ASI) includes a theoretical framework, assessment methods and intervention principles5 and, as Mailloux et al.4 stated: "ASI is one of the most developed and distinctive frames of reference to emanate from the profession of occupational therapy"450. The Sensory Integration and Praxis Tests (SIPT), developed by Ayres1, are considered the "gold standard" for evaluation of sensory integrative function and dysfunction6:25.The instrument was standardised mainly on children from the US (the normative sample also includes a small sub-sample from Canada). The SIPT demonstrates an exceptional ability to discriminate between children with known learning disorders or previously identified sensory integration problems and typically developing children1. Originally published as the Southern California Sensory Integration Tests (SCSIT)7, this collection of tests was developed to provide an in-depth profile of a child's sensory integration abilities and to identify sensory integration problems that impact on the child's ability to participate meaningfully in daily occupations. Children with SI dysfunctions experience mild to severe problems related to motor skills, perception, behaviour, learning, attention, language, and social-emotional abilities.
Recent research involving the use of the SIPT on a selected sample of typically developing South African children8 revealed these children aged 6-9, performed moderately to significantly better than their US counterparts on five of the seventeen tests of the SIPT (specifically, Standing and Walking Balance, Bilateral Motor Coordination, Oral Praxis, Design Copying and Motor Accuracy). The results of this study led to a recommendation to adapt the scores when applied to South African children by half a standard deviation to the negative side for these tests. It was concluded that it would be fair to use the SIPT to identify SI dysfunctions in children from SA8 with this adjustment.
Knowing that the SIPT can be administered on South African children (with the recommended adaptations) and striving towards ethical, just and sound research and practice, led to the question regarding the patterns of dysfunction. In planning ASI interventions, the occupational therapist (OT) depends on careful analysis of assessment data including standardised scores on tests such as the SIPT, as well as observations, interviews, other forms of assessment and clinical reasoning. This comprehensive set of information is considered within the context of a large body of research on patterns of SI dysfunction. Numerous factor analyses, and later cluster analyses, in a variety of typical and atypical samples demonstrated the presence of consistent patterns of sensory integration dysfunction including Visuopraxis, Somatopraxis, Vestibular Bilateral Integration, Somatosensory perception, and Tactile Defensiveness/Attention patterns as the most consistent patterns across multiple studies1,2,3,4,9,10,11,12,13,14. All of these studies were conducted in the United States.
Clinicians within the paediatric field of occupational therapy in SA are increasingly confronted with children experiencing sensory integration difficulties, thus highlighting the need for research on SI within the SA context. The fact that the research on the SI patterns of dysfunction has primarily been conducted in the US leaves the question as to whether South African children with identified sensory integration problems would demonstrate similar or contrasting patterns of dysfunction to those found in previous studies1,3,4 . No similar studies currently exist to establish whether patterns of SI dysfunctions of children outside of the US are similar to those that have been identified amongst children within the US1,2,3,4. In order to provide fair and just services in South Africa to children who experience SI dysfunctions (and to their families), research confirming or contrasting the existing patterns of SI dysfunctions is needed. Therefore, the following questions were addressed in this study:
1. How do the patterns of SI dysfunction in children from SA, compare to patterns in children from a first world country, such as the US?
2. Are there similarities and/or differences in the types of SI dysfunctions that children experience, possibly due to the fact that they grow up in different environments, contexts, lifestyles and with diverse resources?
The aim of this study was thus to confirm, compare and/or contrast patterns of sensory integration dysfunction identified (through the use of the SIPT) in a convenience sample of children from SA who had experienced SI difficulties, to the patterns that have already been identified in US samples.
METHODOLOGY
Based on the strong theoretical constructs of SI and the consistent patterns of dysfunction that were found in previous research the hypothesis of this study was that a factor analysis conducted on SIPT scores from a sample of South African children would reveal the presence of the following patterns, consistent with patterns that have been identified in US samples:
1. Somatopraxis/Somatodyspraxia (referred to as Somatoprax-is)-expecting high loadings on tactile and praxis tests.
2. Visuopraxis/Visuodyspraxia (referred to as Visuopraxis)-ex-pecting high loadings on visual perception and visual motor and visual praxis tests.
3. Bilateral Integration and Sequencing Pattern (referred to as BIS)-expecting high loadings on vestibular and bilateral integration and sequencing tests.
4. Multiple Sensory Perception-expecting high loadings on tests of tactile perception and possibly other sensory perception tests (i.e. visual, vestibular or proprioception).
Research design
A quantitative, analytical research design was used. Data were retrospectively extracted and analysed from SIPT reports available at a certain date, at the South African Institute of Sensory Integration (SAISI) of children identified with sensory integration difficulties.
Sample
A sample of convenience was used with data of 223 children from throughout SA who had been experiencing sensory integration difficulties and had been assessed with the SIPT. The children were between 4-0 (4 years, 0 months) to 8-II (8 years, II months). Children were assessed by members of SAISI who were trained in the use of the SIPT. The sample included 223 children of which 145 (65.03%) were boys and 78 (34.97%) were girls. The majority of the children's parents (for whom information was entered) held jobs which typically would be from middle to higher socio-economic settings (50.40% of the fathers and 55.I5% of the mothers) in a South African context. There were, however, 9.87% of fathers and 4.04% mothers that held jobs that would be associated with low socio-economic settings in SA. White children made up 78.03% of the sample. All of these children presented with functional difficulties that could be related to sensory integration difficulties. This sample, from a clinical viewpoint, is typical of a profile of children who currently have access to an occupational therapy and SI assessment and intervention in SA.
Inclusion criteria
All the children in the sample grew up in SA. The children included were experiencing difficulties that had been identified as possible sensory integration problems. They were referred to or identified by occupational therapists with knowledge of SI problems.
Exclusion criteria
The children excluded from the sample were receiving or had received therapeutic intervention for conditions related to developmental delays prior to assessment. This exclusion was instituted due to the possibility that therapeutic intervention could influence a child's sensory integrative functions and therefore influence their original patterns of sensory integrative dysfunction.
Data collection
Data was extracted from all SIPT reports available at SAISI of children who met the inclusion criteria within a designated time frame (Jan 2007-Dec 20I0).
Ethical Approval
Ethical approval was obtained from the Ethical Committee of the Faculty of Health Sciences, University of the Free State (ETOVS nr: 162/2010) and there was no risk to the health of the individuals included in the study by participating in the assessment. Parents or legal guardians of the children were informed of the use of the data for research purposes and were required to sign an informed consent form. Confidentiality and anonymity were maintained during the research process.
Data Analysis
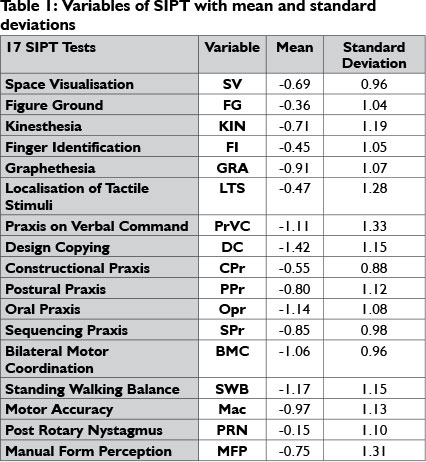
Each of the 17 tests in the SIPT battery has multiple sub-scores, and only the major test score for each test was used in the descriptive and exploratory analysis of data. Based on previous research on the use of the SIPT with children from SA8, the major scores of Standing Walking Balance, Bilateral Motor Coordination, Oral Praxis, Design Copying and Motor Accuracy were adapted with half a standard deviation to the negative side before the analysis. Pearson Correlation coefficients were calculated between all variables. Next, factor analysis was performed using all the major SIPT scores. The SAS system was used to perform maximum likelihood exploratory factor analysis with orthomax rotation. Factors were identified on the basis of scree plots, revealing patterns of dysfunctions within this sample of children. Test items were considered to load moderately on a factor when the loading was >|.35-.49| and strongly when the loading was >|.50|. This is also in line with previous factor analytic studies performed with the SIPT2,4.
RESULTS
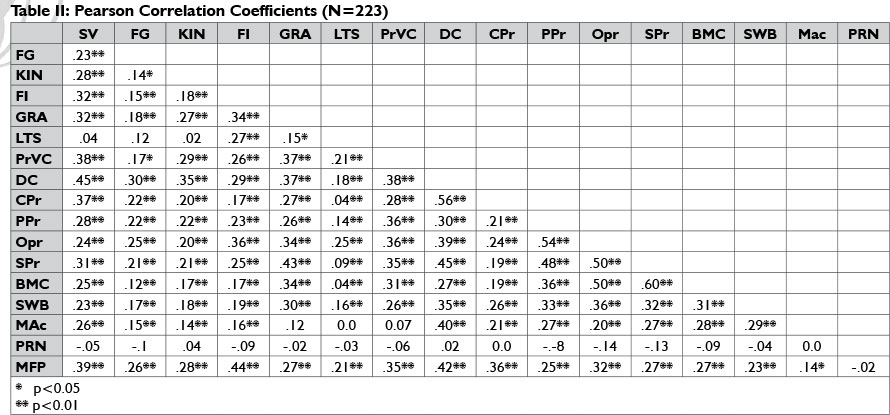
The mean and standard deviations scores (incorporating the correction to the five tests mentioned above) of the sample used in this study are displayed in Table 1. Pearson Correlation coefficients that were calculated between all variables are displayed in Table 2 and levels of significance in terms of relations are also indicated where applicable.
The SIPT tests that had the highest inter-correlations in this sample were similar to findings of research done by AyresI on a sample of I25 children with learning or SI disorders. Examples are: Space Visualisation that also had the highest correlations with Design Copying and Constructional Praxis; Graphesthesia also had high correlations with tests of Oral Praxis and Sequencing Praxis; and Bilateral Motor Coordination with a high correlation with tests of Sequencing Praxis, Oral Praxis and Graphesthesia. The fact that correlations of similar strength between variables were found in this study, compared to previous studies done on children that were also not typically developing children, is a confirmation of the already existing underlying constructs and reliability of the SIPT.
The first round of factor analysis (maximum likelihood) yielded two eigenvalues >1, although a scree plot indicated that a three-factor solution might be preferred. In the light of this, a three factor solution was specified, with an orthomax rotation (see Table 3). The first factor that emerged had high loadings on tests that were associated with a factor of Visual Perception, Visuopraxis or Visuodyspraxia1,2 namely Design Copying, Constructional Praxis and Space Visualisation. Tests of Motor Accuracy, Manual Form Perception and Kinesthesia, also associated with this factor, had moderate loadings, comparable to the factor analyses performed by Ayres1 and Mulligan2. Tests approaching loadings of .35 on this factor (Sequencing Praxis, Praxis on Verbal Command, Standing Walking Balance and Graphesthesia) were also similar to groupings found in previous research. Ayres1 hypothesised that this combination of scores might reflect shared higher level (i.e. cortical) right and left hemisphere functions. The mentioned tests have implications regarding discriminatory abilities, form and space perception, and visual-motor abilities - all dependent on the integrity of the visual-, tactile-, vestibular- and proprioceptive systems. The one test that did not have a high loading on this factor, in contrast to previous findings, was Postural Praxis (0.24).
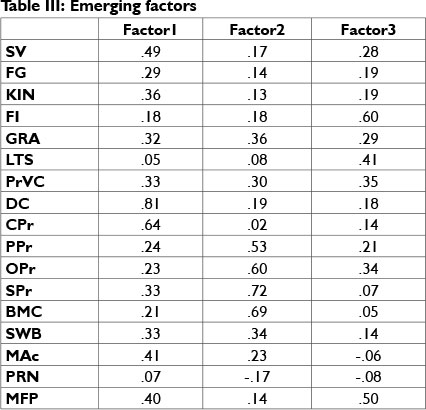
The second factor that emerged had high loadings on tests of Sequencing Praxis, Bilateral Motor Coordination and Oral Praxis, also consistent with previous research1,4 which indicated a factor of Bilateral Integration and Sequencing (BIS). Graphesthesia had a moderate loading and Standing Walking Balance, with a loading of 0.34, cannot be totally excluded in this factor, and these tests have been associated with BIS in previous research. Patterns of BIS were evident in many of the previous studies that have associated bilateral integration with functions of the vestibular- and proprioceptive systems4. Postural Praxis also had a high loading on this factor and Praxis on Verbal Command had a moderate loading on this factor, suggesting some overlap with Somatopraxis.
High loadings on Finger Identification, Manual Form Perception and Localisation of Tactile Stimuli were prominent in the third factor and all of these tests have a strong element of tactile discrimination and are dependent on the integrity of the tactile system. Finger Identification and Localisation of Tactile Stimuli have consistently been associated with a pattern characterised by multiple system sensory perception in previous research1,2,4. Praxis on Verbal Command had a moderate loading whilst Oral Praxis approached a moderate loading on this factor and is thought to be closely related with somatosensory processing. The loading on tests of praxis within this factor is similar to findings of the research of Ayres1,2,4.
A second round of confirmatory factor analyses was performed with LISREL, and specified according to the models derived by Mul-ligan2. She compared three different latent variable models, with three-, four- and five factors respectively2. The best fit for this SA sample was found for the three factor solution (see Figure 1 on page 5). The first factor that emerged during this round of analysis had high loadings on Space Visualisation, Design Copying and Constructional Praxis, again tests associated with Visuodyspraxia1,2. Manual Form Perception and Praxis on Verbal Command also had moderate loadings and have been associated with Somatodyspraxia in the past1. Postural Praxis that had loaded in patterns of somatosensory dysfunctions in previous research had a loading of 0.31 in this research which is a higher loading than in the first round of analysis, already discussed. The majority of loadings within this factor are however consistent with patterns of Visuo- and Somatodyspraxia.

The second factor with loadings on Kinesthesia, Graphestesia, Oral Praxis, Sequencing Praxis, Bilateral Motor Coordination, Standing Walking Balance and Motor Accuracy were once again consistent with BIS patterns that are well described in previous research1,2,4. The only test that did not load within this factor as was seen in previous research was PRN, likely due to the averaging effect of the prolonged and depressed scores, since more than 20% of the children within this sample had PRN scores higher than +1.0 SD. Both Mulligan2 and Mailloux, et al.4 have already commented on the difficulties involved in the scoring of the PRN factor, as both high and low scores are indicative of dysfunction. The proportion of children with dysfunctional PRN scores was, furthermore, much greater than the approximately 8% reported by Mailloux, et al.8 A factor of BIS dysfunction similar to previous studies has thus once again been confirmed with this research.
The third and last factor had loadings on tests associated with tactile and visual discrimination. Previous research1,2,4 has also indicated that associations exist between tests measuring tactile functions and other sensory systems. The two tests that loaded the highest within this factor (Manual Form Perception and Finger Identification) are largely dependent on discriminatory functions1. A third test, Localisation of Tactile Stimuli, had a loading of 0.31 and is also dependent on tactile discrimination. A factor of Tactile and Visual Discrimination thus emerged from this research.
DISCUSSION
This research, utilising both exploratory and confirmatory factor analysis, confirmed that similar patterns of sensory integration dysfunction (i.e. Visuopraxis, Bilateral Integration and Sequencing, and Multiple Sensory Perception) identified in previous research1,2,4 were present in this sample of children from South Africa. These findings are consistent with previous studies by Ayres1,10,11,12,13,14 that employed measures prior to the SIPT. In this study, elements of a pattern commonly found in previous studies, i.e., Somatopraxis, was seen in combination with both Visuopraxis and with BIS, as was the case in some of the previous studies1,4. One other common pattern found in previous studies was tactile defensiveness and hyperactivity4,9,10,11,12,13. However, measures of these functions were not available for the children in this study, therefore it was not possible to either verify or refute the presence of that pattern in this sample. One other pattern found by Ayres1-Dyspraxia on Verbal Command-was also not found in this sample.
Limited differences were found in this study. For example, the fact that Postural Praxis did not have a high loading within the factor of Somatodyspraxia as in previous studies, does not have a clear explanation, but the fact that the other praxis tests (Constructional Praxis, Design Copying) had strong loadings and Praxis on Verbal Command (0.33) and Sequencing Praxis (0.33) approached moderate loadings do support the importance of praxis within this factor.
This research also confirms that children in SA do experience difficulties with sensory integration functions that require discriminatory and perceptual abilities, such as the spatial and temporal aspects of navigating oneself in three dimensional space, as well as more refined sensory-motor functions such as motor skills and praxis. The fact that the majority of children in this study came from middle- to high socio-economic settings now leaves the challenge of performing similar studies on children from low socio economic settings, as previous research has indicated that these children do experience SI difficulties, although the patterns of dysfunctions still need to be confirmed. The argument can also be made that if all the research has shown consistency in patterns of dysfunctions, including even this research 'on the other side of the world', in a developing context, is further costly research still needed? Can we as researchers not use the existing body of knowledge and rather invest time and money in more cost effective and appropriate assessments and interventions for the thousands of children from developing countries that may never be able to access expensive services?
Implications for Occupational Therapy Practice
- The Sensory Integration and Praxis Tests (SIPT) identify patterns of dysfunction similar to those found in the US, thus these tests can be used to guide intervention planning for children in SA, consistent with OT intervention planning in the US.
- Consideration of SI dysfunction for children who are not represented in the US SIPT norms is important for identifying and ameliorating participation challenges for all children.
LIMITATIONS
The sample of children in this study was a convenience sample. Therefore, the sample may not be representative of all children in South Africa experiencing difficulties in sensory integration and especially not the children from low- to very low socio-economic settings. In addition, the study was retrospective, thus limited to the measures available in the existing records.
CONCLUSION
This study revealed relative consistency of patterns of sensory integration dysfunction between South African children and children assessed on similar measures in the US. No widely contrasting patterns of dysfunction emerged from this research. This research also demonstrates the existence of patterns of sensory integrative dysfunction in a current sample of children from South Africa, consistent with patterns identified through research over the past 50 years. It also confirms that children from South Africa do experience SI dysfunctions that interfere with their participation in activities of daily living, well-being, and quality of life irrespective of where in the world they grow up. Understanding the variations in types of deficits in sensory integration and praxis informs occupational therapy practice. It refines the analysis of assessment data from the SIPT and related measures, and guides clinical reasoning to plan intervention with confidence in order to support engagement in occupation and participation in daily life.
REFERENCES
1. Ayres, A. J. Sensory Integration and Praxis Tests Manual. Los Angeles, CA: Western Psychological Services, 1989. [ Links ]
2. Mulligan, S. Patterns of Sensory Integration Dysfunction: A Confirmatory Factor Analysis. American journal of Occupational Therapy, 1998; 52: 819-828. [ Links ]
3. Mulligan, S. Cluster analysis of scores of children on the Sensory Integration and Praxis Tests. OTIR: Occupation, Participation and Health, 2000; 20: 256-270. [ Links ]
4. Mailloux, Z., Mulligan, S., Smith Roley, S., Blanche, E., Cermak, S., Coleman, G., & Lane, C. Verification and clarification of patterns of sensory integrative dysfunction. American Journal of Occupational Therapy, 2011 ;65 (2): 143-151. [ Links ]
5. Smith Roley, S., Mailloux, Z. Miller-Kuhanek, H. & Glennon, T. Understanding Ayres Sensory Integration®. OT Practice, 2007; 12(17): CEI-CE-8. [ Links ]
6. Smith Roley, S. Evaluating sensory integration function and dysfunction. In R.C. Schaaf. & S. Smith Roley (Eds.). Sensory Integration: Applying Clinical Reasoning to Practise with Diverse Populations, 2006; (15 - 36). Austin, TX: Pro-Ed. [ Links ]
7. Ayres, A. J. Southern California Sensory Integration Tests. Los Angeles, CA: Western Psychological Services, 1972a. [ Links ]
8. Van Jaarsveld, A., Mailloux, Z. & Herzberg, D. S. The use of the Sensory Integration and Praxis tests with South African children. The South African Journal of Occupational Therapy, 2012; 42(3): 13-18. [ Links ]
9. Ayres, A. J. Patterns of perceptual-motor dysfunction in children: A factor analytic study. Perceptual and Motor Skills, 1965; 20: 335-368. [ Links ]
10. Ayres, A. J. Interrelations among perceptual-motor abilities in a group of normal children. American Journal of Occupational Therapy, 1966a; 20(6): 288-292. [ Links ]
11. Ayres, A. J. Interrelationships among perceptual-motor functions in children. American Journal of Occupational Therapy, 1966b; 20(2): 68-71. [ Links ]
12. Ayres, A. J. Deficits in sensory integration in educationally handicapped children. Journal of Learning Disabilities, 1969; 2(3): 44-52. [ Links ]
13. Ayres, A. J. Types of sensory integrative dysfunction among disabled learners. American Journal of Occupational Therapy, 1972b; 26(1): 13-18. [ Links ]
14. Ayres, A. J. Cluster analyses of measures of sensory integration. American Journal of Occupational Therapy, 1977; 31(6): 362-366. [ Links ]
 Correspondence:
Correspondence:
Anne-Marie van Jaarsveld
Gnatavj.md@ufos.ac.za


{kind=link}