










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versión On-line ISSN 2310-3833
versión impresa ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 no.1 Pretoria ene. 2014
SECTION 1
Occupational performance factors perceived to influence the readmission of mental health care users diagnosed with schizophrenia
Rulaine SmithI; Patricia De WittII; Denise FranzsenIII; Michelle PillayIV; Nadine WolfeIV; Carrie DaviesIV
IB.Occ Ther (Pret), Dip Vocational Rehabilitation (Pret); Lecturer, Dept. of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand
IIDip OT (Pret), MSc OT (Wits); Adjunct Professor and Head, Dept. of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand
IIIBSc OT (Wits), MSc OT (Wits); Senior lecturer, Dept. of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand
IVStudents in the Department of Occupational Therapy University of the Witwatersrand at the time the study was carried out
ABSTRACT
Schizophrenia is a complex disorder due to the range of deficits with which mental health care users (MHCUs) present. In addition, the high rate of relapse and readmission in clients diagnosed with schizophrenia complicates the effective management of the condition. Medical factors have been evidenced to affect relapse and readmission rates however limited data exists regarding the influence of occupational performance factors. The aim of this study was therefore, to determine which occupational performance factors are perceived to affect the readmission of MHCUs diagnosed with schizophrenia. A descriptive, cross-sectional quantitative design with qualitative elements was conducted. Card sorting was implemented in two phases to a conveniently sampled population of occupational therapists and MHCUs diagnosed with schizophrenia. Data were analysed by means of descriptive statistics. It was found that social participation was perceived to be the most influential factor in the readmission of MHCUs diagnosed with schizophrenia. In conclusion, both medical and occupational performance factors affect readmission rates of MHCUs diagnosed with schizophrenia. Therefore to implement a client centred approach in occupational therapy, therapists may need to reconsider the priorities they address in treatment.
Keywords: occupational performance, readmission, schizophrenia
INTRODUCTION
The term 'schizophrenia' was coined by Eugene Bleuler in 1911 and is directly translated from Greek origins to mean skhizein: "to split" and phrên: "mind"1. Schizophrenia is viewed as a complex, debilitating disorder where symptoms in affected persons' range from altered cognitive capacity to disrupted social relationships2.
The prevalence of schizophrenia worldwide appears to be fairly common, as it is rated at 5-5.0 per 100001 according to the DSM-IV-TR. The range of symptoms present in mental health care users (MHCUs) diagnosed with schizophrenia is often difficult to manage for various reasons, but it has been said that one of the main difficulties complicating treatment is the high rate of relapse and readmission despite treatment. Limited empirical data exist in terms of the specific relapse and readmission rates within South Africa2,3. However, in a study done by Kazadi et al4, it was reported that 61% of MHCUs diagnosed with schizophrenia in Johannesburg relapse at least once, with the majority having two or more relapses.
The need for clinicians and researchers to develop the evidence for interventions that prevent early psychiatric readmission was emphasised by Vigod et al5. With the occurrence of relapse being so apparent, it is important for occupational therapists to determine and understand which occupational performance factors are associated with relapse in MHCUs diagnosed with schizophrenia.
LITERATURE REVIEW
A literature search into the factors that affect relapse and readmission of MHCUs diagnosed with schizophrenia revealed that many studies focussed on contributing medical factors. Aspects such as comorbid medical conditions, substance abuse, and non-compliance to psychotropic medications were identified4,5. Various studies allude to evidence which suggests that factors other than biomedical phenomena play a role in readmission; however they do not specify what these factors are4-6.
Jibson et al7 revealed that all areas of occupational performance and engagement in occupation for MHCUs diagnosed with schizophrenia have been impacted by the recurrence of active psychosis and readmission to hospital. One could then question whether these areas of occupational performance, which in occupational therapy include functioning in personal management, work, leisure, social participation and routine8, play any role in relapse and readmission. Odes et al9 in their study showed that the level of function of MHCUs with schizophrenia on discharge could predict long-term outcome in terms of the rate of readmission. Those MHCUs who were not readmitted during the period of this study (1999 - 2005) had a significantly higher (p < .05) comprehensive functional score when discharged from hospital in terms of cognitive, social and task related behaviour.
Research linking employment to relapse has identified a perpetuating negative cycle between these two factors as MHCUs experienced increased hospital admissions during economic slumps when they were less likely to retain their employment10-12. Engagement in work or work related activities has been shown to result in improved mental health. Furthermore, employed MCHUs show improved quality of life and report that active engagement provides them with a purpose in life10.
Provencher, et al13 found that 'profiles of recovery' related to work required an understanding of the benefits of work as perceived by MHCUs themselves. Supportive employment was found to reduce readmission14, and this was supported by the perceptions of MHCUs who felt they were more successful in obtaining and retaining a job with supported employment15. There is evidence that support should not be given by health professionals such as occupational therapists, as their belief system about the stresses of work precipitating relapse tend to make them overprotective of MHCUs16. Rinaldi et al16 found that professionals underestimated their clients' coping abilities and advised them to not engage in work at all.
Mental health care users diagnosed with schizophrenia have poor personal management skills and in the long term are less likely to perform self-care or health promotion activities, than persons without a mental illness17,18. These MHCUs were found to have a high external locus of control with regards to their health beliefs. Many were dependent on family members to complete or assist with their personal management activities however, it has been shown that if they had no family support in this regard they were more vulnerable to relapse and readmission18. There is limited research to indicate that poor personal management directly contributes to readmission.
The social support that MHCUs receive and the social activities that they participate in after discharge have been found to have a major impact on the course of the illness, as returning to live with family or carers can either positively or negatively influence the MHCUs vulnerability for relapse and readmission19. A strong social support system has been evidenced to prevent readmis-sion20. Cohen and Sokolovsky20 highlighted this in their study of a Puerto Rican man diagnosed with catatonic schizophrenia who was frequently readmitted to hospital secondary to relationship stressors. Interventions aimed at improving socialisation prevented his readmission for nine years. However, when this social intervention was discontinued, readmission to hospital followed shortly after. Enhancing skills in social abilities appear to help patients re-engage in their relationships and are instrumental in maintaining their supportive social networks21.
Another contributing occupational performance factor associated with readmission in MHCUs is a lack of routine. Chugg and Craik22 found that MHCUs diagnosed with schizophrenia had difficulty maintaining daily routines and that they spent most of the day sleeping23. The importance of constructive use of free time for MHCUs therefore needs to be emphasised12 as involvement in leisure provides opportunity for the "development of a person's identity, motivation, autonomy, self-regulating behaviour, personal enrichment and socialisation"24:304. Many MHCUs engage in disruptive behaviours such as substance abuse in their free time which has been found to contribute to relapse4.
Literature has shown that all areas of occupation are seen to be affected by schizophrenia and dysfunction in these areas may actively contribute towards readmission. However, minimal research has been done into which occupational factors are perceived to have the most influence on relapse and readmission. Identification of these factors could have implications for the prioritisation of meaningful occupational therapy intervention to prevent readmission25. However, as occupational therapy practice is based on a client centred frame of reference, obtaining evidence for practice must include the opinions of MHCUs in relation to the effects of occupational performance on the outcomes of therapy24. The objectives of the study were therefore:
- To identify the perceptions of MHCUs diagnosed with schizophrenia with regards to which occupational performance factors have the greatest influence on their readmission.
- To identify the perceptions of the occupational therapists working in the mental health field of practice with regards to which occupational performance factors have the greatest influence on the readmission of MHCUs diagnosed with schizophrenia.
METHODOLOGY
Study Design
A descriptive, cross-sectional quantitative study was implemented after obtaining ethical clearance from the Human Research Ethics Committee (HREC) of the Faculty of Health Sciences at the University of the Witwatersrand. The study aimed to determine which occupational performance factors were perceived by MHCUs diagnosed with schizophrenia and occupational therapists to affect readmission the most; therefore there were two phases.
Population and Sampling
For phase 1 of the study, sample A consisted of 30 adult clients diagnosed with schizophrenia who had been readmitted to hospital. They were conveniently selected over a period of three months in 2010 from six facilities offering services to MHCUs in Gauteng. Permission was obtained from the Gauteng Department of Health, as well as CEOs of the facilities who consented for the research to be conducted at the occupational therapy departments. The occupational therapists at the facilities identified potential participants during the prescribed time period; however, only 26 participants met the inclusion criteria of being: apsychotic, over the age of 18 years, and literate.
For phase 2 of the study, sample B consisted of 10 conveniently sampled South African occupational therapists working in the field of mental health for at least one year.
Research Tools
The research team consisted of three researchers who gathered data by:
- Completing a demographic questionnaire with the MHCUs diagnosed with schizophrenia,
- Implementing card sorting with both samples A and B. The same first and second card sort was used for both samples.
- Questioning the participants regarding the ranking of the cards for the first and second card sort.
The demographic questionnaire consisted of 17 items which included questions relating to personal and medical background. The questionnaire took 20 minutes to administer.
Card sort26 is a technique used to explore the way in which preselected information can be grouped by people. This technique was chosen as it was found to be an easy method of gathering information related to the specific occupational performance factors assessed in this study27. This technique allowed the participants to rank occupational performance factors as they perceived them to influence readmission. The content of the card sort was developed by the researchers by:
1. Reviewing the literature to determine the occupational performance factors influencing readmission. Six categories were identified, namely 'work', 'personal management', 'leisure', 'social ability', 'routine' and 'other'. These categories were then reworded into simple phrases for clients' ease of understanding, as follows:
- Work - 'I did not have a job'
- Personal management - 'I could not care for myself'
- Leisure - 'I did not have anything to do in my free time'
- Social ability - 'I did not have anyone to support me'
- Routine - 'I did not have a structure to my day'
- Other.
These phrases, which formed the cards for the first card sort, related directly to occupational performance8 thereby ensuring face validity of the tool.
2. The first card sort cards were then sent to a panel of six experts in the field of mental health. The experts were asked to critique the content of the cards and they found that the reworded phrases were too broad and would not yield adequate data. The researchers then drafted cards for a second card sort (see Table I) in order to yield explanations specific to the occupational performance factor ranked first in the first card sort. Thus, in the second card sort, participants were exposed only to the cards linked to the specific occupational performance factor, e.g. if a participant chose "I did not have a job" in the first card sort the only cards presented in the second card sort were: 'I could not keep a job', 'I could not find an available job', 'I did not have the skills to work' and 'I did not want to work' (see Table I).
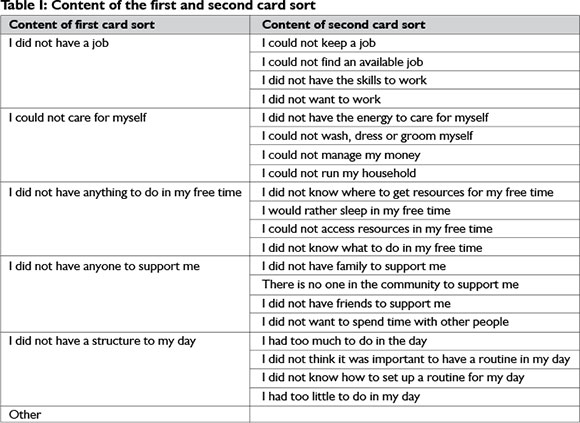
Participants were also expected to rank the cards of the second card sort according to their perceived level of importance for readmission.
Experts reviewed the content of both card sorts thereby ensuring content validity of the tool.
3. To ensure inter-rater reliability the card sort and demographic questionnaire were piloted by each of the three researchers on three clients at a facility offering services to MHCUs. Participants in the pilot study showed no difficulties when ranking the first and second card sort activities, hence the content of both card sorts was unchanged.
Data gathering procedure
For phase 1, occupational therapists working at the participating facilities identified readmitted MHCUs diagnosed with schizophrenia according to the inclusion criteria. The identified participants were approached and informed consent was obtained. The demographic questionnaire was then completed with each participant individually; after which the first and second card sort were implemented. Each participant was asked to prioritise the occupational performance factors that they perceived to have the greatest impact on their current readmission using the first card sort. The second card sort was implemented thereafter based on the ranked choice from the first card sort (see Table I). The researchers questioned participants regarding the ranking of the cards in order to understand the reasons for prioritisation.
For phase 2, the ten participating occupational therapists completed the card sort individually as administered in phase 1. The occupational therapists were asked to rank the cards of the initial card sort to indicate which occupational performance factors they perceived to have the greatest impact on readmission of MHCUs diagnosed with schizophrenia. The second card sort was implemented thereafter based on the ranked choice from the initial card sort in order to yield explanations for the initial ranking (see Table I). The researchers questioned therapists regarding the ranking of the cards in order to understand the reasons for the prioritisation.
All participants' rankings of the cards were photographed for data collection. The principles of informed consent, and confidentiality were adhered to27.
Data analysis
Descriptive statistics, in the form of percentages was used to describe the demographics of sample A. The ranking of the occupational performance factors for both card sorts was analysed using percentages and presented as a matrix. Content analysis of the participant responses was done.
RESULTS
Demographics
Of the 26 participants who met the inclusion criteria, 73% (n=l9) were male and 26% (n = 7) female. Seven percent (n=2) fell within the ages 20-25, l9% (n=5) within 26-30 years, l9 %
(n=5) within 3l-35 years, 15% (n = 4) within 36-40 years, and 38% (n=l0) over 40 years of age. Ninety two percent (n=24) of the participants reported to be single, indicating not having a life partner or being widowed or divorced. Only 7% (n=2) indicated that they were married.
In terms of the level of education, 11% (n = 3) completed grade 7, 26% (n = 7) completed grade 10, 34% (n=8) completed grade 12 and 34% (n=8) had further educational training.
100% of the participants fell within the low socioeconomic status category, i.e. earning an income of less than R2000/month if earning at all.
Card sort 1: The perceptions of MHCUs diagnosed with schizophrenia
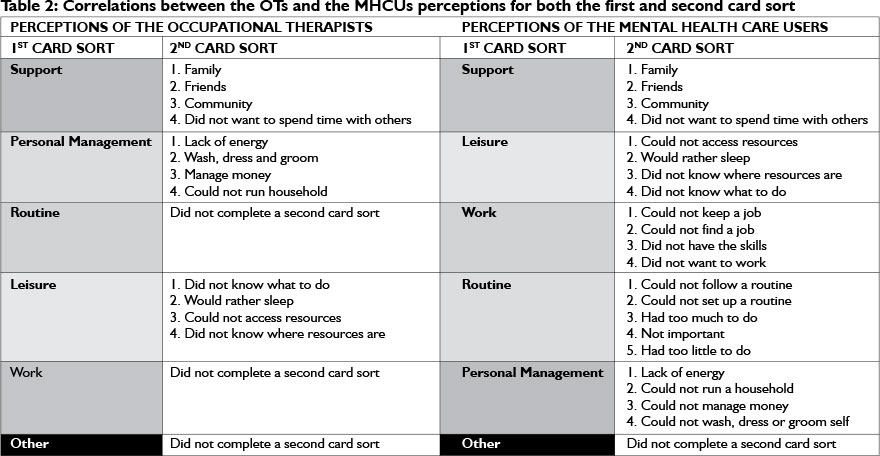
The results of the first card sort for the MHCUs diagnosed with schizophrenia indicated that the factor they perceived as most influential in contributing to readmission was in the occupational performance area of support where 30% (n=8) ranked it first. Leisure was ranked as the second most contributing factor to readmission. The highest percentage for work was ranked second at 23% (n=7), however this was lower than leisure and was then ranked as the third most influential factor. 30% (n=8) of the participants ranked routine as the fourth most influential factor. Self-care was ranked equally at fourth and fifth, but was less than routine at rank at number four, therefore overall it was rated as the fifth most influential factor. Fifty seven percent (n=15) ranked other as the least influential factor affecting readmission (See Table II).
Card Sort 1: The Perceptions of Occupational Therapists
Fifty percent (n=5) of the occupational therapists ranked support as the main contributing factor to readmission in the first card sort. For rank two, the results were equally split between a self-care, routine and work at 10% (n=1). Therefore the percentages that were higher at other rankings for each factor were taken into consideration first, and through a process of elimination, self-care was identified as the second most influential factor. Routine was ranked fourth by 50% (n=5) of the OTs, and 50% ranked work as the fifth most influential factor. Other was chosen as the least influencing factor affecting readmission, by 60% (n=6) of the OTs (See Table II).
Card Sort 2:
The findings of card sort 2 are presented in Table II. The only agreement between the perceptions of MHCUs diagnosed with schizophrenia and the occupational therapists is in the category of support. All other categories show varied rankings.
DISCUSSION
The main factor impacting on readmission, as perceived by both the readmitted MHCUs diagnosed with schizophrenia and occupational therapists was support. This is reinforced by the work of Niehaus19, as poor social support was found to have a negative impact in influencing the vulnerability for relapse and readmission. The MHCUs diagnosed with schizophrenia identified lacking support due to familial conflict as a result of psychotic behaviour as the stressor resulting in readmission, as highlighted in the statement below:
I was always fighting with my family because they thought I was trying to cause trouble... they did not understand what was happening.
A limitation to the study was that the card sort statements were chosen in order to make them unambiguous for the participants. This resulted in certain terms, such as social participation being translated into lay terms, i.e. 'support'. However, some MHCUs diagnosed with schizophrenia viewed this support as being financial support indicating ambiguity of the phrase of the card. This could be seen where 'other' was chosen as the main reason for readmission, but when asked to explain what 'other' was, the participant stated:
I was always fighting with my mother and having problems with my family, so I struggled to be around people and had no one to talk to.
The participant did not prioritise this as support even though that card best described the situation.
This skewed interpretation of support was highlighted by Marwaha and Johnson28 where MHCUs viewed support as social aspects and not financial aspects as indicators for wanting to be employed.
Besides support being the top factor perceived as influencing readmission, no other similarity in the ranking exists between the perceptions of occupational therapists and MHCUs diagnosed with schizophrenia.
Routine was identified by the occupational therapists as a necessity in order to engage in leisure and work, therefore they prioritised this above leisure and work as essential in preventing readmission. This finding is emphasised by the underlying occupational therapists' belief that routine is vital in carrying out all activities of daily living23. In contrast, the MHCUs diagnosed with schizophrenia felt that if they had something to do in their free time, or if they were employed, this would lead to a routine in their day. Therefore, leisure and work were ranked higher than routine.
This raises the question as to whether the occupational therapists are addressing routine and structure in therapy. If routine is perceived to be a highly contributing factor to mental health23 as reflected in the literature, it needs to be addressed first and foremost within intervention. Mental health care users need to understand the role that routine plays with regard to work and leisure, so that treatment efforts are focussed on achieving a balanced lifestyle, which results in improved mental health and fewer readmissions.
The prioritisation of work was influenced by additional factors and this was a limitation to the study. When asking the MHCUs diagnosed with schizophrenia about where they had placed work, the majority either said they had placed it high as they did not have work, or low because they did have work. Therefore this category was heavily influenced by their personal situations as well as their concept of the importance of work to their recovery13. Most participants did not have the insight to describe what relationship work had to relapse and readmission. These findings should however be explored in relation to the work profiles described by Provencher, et al13. They found that many MHCUs experienced the role of work in their recovery as "uncertain" or "as a challenge" due to a lack of self efficacy, social abilities and support. For the MHCUs who perceived work as "a self-empowering experience", being employed facilitated their recovery and ability to maintain themselves outside of the hospital. Thus there is a need to understand the MHCUs context and previous experience of work in relation to how they view work in influencing their readmission.
With regard to factors impacting on the constructive use of free time, especially for those participants who did not have employment, the occupational therapists felt that the lack of leisure activities was the next most important factor in readmission as MHCUs did not know what to do in their free time. The MHCUs diagnosed with schizophrenia responded differently, identifying this as the least contributing factor and reporting an inability to access resources as the main problem as highlighted in the statement below.
When I was at home, I thought about doing things for fun or with my friends, but I did not know where to go to have fun.
For those clients involved in occupational therapy programmes, many had engaged in leisure activities but within the structure of the department programme, therefore after discharge, although they may have wanted to engage in leisure activities, they felt they did not have access to resources. Thus the value placed on leisure by the MHCUs appears to be affected by the context to which they return. Inclusion of aims on how to access recreational and leisure resources in that context therefore need to be emphasised as outcomes in occupational therapy to prevent MHCUs from spending their free time unconstructively and to assist them to develop an understanding of the importance of constructive leisure in their recovery.
The MHCU participants prioritised personal management as the occupational performance factor that contributed least to readmission, whereas the occupational therapists ranked it second. This may be due to the training the occupational therapists receive, that individuals must be able to care for themselves first, before being able to engage in work, leisure or social activities. According to the Vona Du Toit Model of Creative Ability17, independence in personal management is the first area of occupation to develop.
Research has shown that unless personal management goals are prioritised with the MHCU and their family or carer the level of function in personal management was not maintained and readmission was more likely to occur29. The MHCUs themselves did not prioritise personal management and felt that the ability to care for themselves did not have a significant impact on their level of functioning. For them, the areas of work, leisure and social participation and support were more important, indicating a possible problem with insight into the importance of personal management as one of the factors identified as most affecting readmission.
The findings for personal management could have been affected by the level of creative ability, as described by du Toit17, as the MHCU participants completing the card sort were at least on the level of passive participation and thus were already functioning fairly independently in personal management. The concern of the occupational therapists was about the ability of the MHCUs to maintain this level of functioning once they were discharged. Shimozono et al29 evidenced that MHCUs must be supported after discharge in order to maintain functioning achieved within therapy programmes.
The only other agreement between the perceptions of the two groups was that 'other' was prioritized as the least contributing factor to readmission. The card 'other' was included in the card sort to allow the MHCUs and occupational therapists an opportunity to describe any other factors that they felt had a large impact on readmission. When explaining the card sort, this card was offered as an option in the first card sort. If the participant ranked 'other' first they needed to explain, in the second card sort what 'other' was and how it impacted on readmission. Once the participants became aware of this, many of them changed their ranking and placed 'other' further down, so they would not have to describe it. This affected the ranking of the occupational performance factors and should have been omitted from the original categories.
CONCLUSION
Occupational factors and medical factors should not be viewed in isolation. There is a two-way relationship between these factors, each impacting on the other. They cannot be viewed as separate entities as they contribute together to the readmission of MHCUs diagnosed with schizophrenia.
For this study, prioritisation of the occupational performance factors was done as separate entities. It is difficult to determine which one factor in isolation has the most influence on readmission, as the factors influence one another however, in this study both samples identified support as the most influential factor affecting readmission. The perceptions of both samples differed for all other occupational performance factors indicating a need for therapists and MHCUs alike to collaborate when establishing therapeutic goals30 to prevent relapse and readmission of MHCUs diagnosed with schizophrenia.
REFERENCES
1. Sadock BJ, & Saddock VA. Schizophrenia. In: Sadock BJ, & Saddock VA. Synposis of Psychiatry. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2007: 471-504. [ Links ]
2. Tsuang M, Faraone S, Glatt S. Schizophrenia. The Facts. 3rd ed. London: Oxford University Press; 2011: 1-2. [ Links ]
3. Kazadi NJB. Schizophrenia Relapse in a Community Mental Health Setting. Unpublished Masters Dissertation, Department of Psychiatry, University of the Witwatersrand Repository; 2008. [ Links ]
4. Kazadi NJB, & Moosa MYH, & Jeenah FY Factors Associated with Relapse in Schizophrenia. South African Journal of Psychiatry, 2008; 14 (2): 52-62. [ Links ]
5. Vigod S, Kurdyak P, Dennis C, Leszcz T, Taylor V, Blumberger D, et al. Transitional interventions to reduce early psychiatric readmissions in adults: systematic review. British Journal of Psychiatry, 2013: 202 (1): 187-194. [ Links ]
6. Emsley R, Chiliza B, Asmal L, Harvey B. The nature of relapse in Schizophrenia. BioMedCentral Psychiatry, 2013; 13 (50): 1-8. [ Links ]
7. Jibson MD, Glick ID, & Tandon R. Schizophrenia and Other Psychotic Disorders. Focus, 2004; 2 (1): 17-30. [ Links ]
8. American Occupational Therapy Association. Occupational therapy practice framework: Domain and process(2nd ed.). American Journal of Occupational Therapy, 2008; 62 (6): 625-683. [ Links ]
9. Odes H, Nachum Katz N, Noter E, Shamir Y. Level of Function at Discharge as a Predictor of Readmission Among Inpatients With Schizophrenia. American Journal of Occupational Therapy, 2011; 65 (3): 314-319. [ Links ]
10. Crist PH, Davis CG, & Coffin PS. The Effects of Employment and Mental Health Status on the Balance of Work, Play, Leisure, Self Care and Rest. Occupational Therapy in Mental Health, 2000; 15 (1): 27-42. [ Links ]
11. Mueser KT Salyers MP & Mueser PR. A Prospective Analysis of Work in Schizophrenia. Schizophrenia Bulletin, 2001; 27 (2): 281-296. [ Links ]
12. Lloyd C, King R, McCarthy M, & Scanlan M. The Association between Leisure Motivation and Recovery: A Pilot Study. Australian Occupational Therapy Journal, 2007; 54: 33-41. [ Links ]
13. Provencher H, Shery Mead R & Mueser K. The Role of Work in the Recovery of Persons with Psychiatric Disabilities. Psychiatric Rehabilitation Journal, 2002; 26 (2): 132-144. [ Links ]
14. Oka M, Otsuka K, Yokoyama N, Mintz J, Hoshino K, Niwa S, et al. An evaluation of a hybrid occupational therapy and supported employment program in Japan for persons with schizophrenia. American Journal of Occupational Therapy, 2004; 58 (4): 466-475. [ Links ]
15. Johnson R, Floyd M, Pilling D, Boyce M, Grove B, Secker J, et al. Service users' perceptions of the effective ingredients in supported employment. Journal of Mental Health, 2009; 18 (2): 121-128. [ Links ]
16. Rinaldi M, Perkins R Glynn E, Montibeller T, Clenaghan M, Rutherford J. Individual placement and support: from research to practice. Advances in Psychiatric Treatment, 2008; 14 (1):50-60. [ Links ]
17. Crouch R & Alers V Occupational Therapy in Psychiatric and Mental Health. 4th ed. England: Whurr Publishers Ltd; 2005. [ Links ]
18. Dangdomyouth P, Stern P, Oumtanee A, & Yunibhand J. Tactful Monitoring: How Thai Caregivers Manage their Relative with Schizophrenia at Home. Issues in Mental Health Nursing, 2008; 29 (1): 37-50. [ Links ]
19. Niehaus DJH, Koen L, Galal U, Dhansay K, Oosthuizen PP Emsley RA, et al. Crisis discharges and readmission risk in acute psychiatric male inpatients. BioMedCentral Psychiatry, 2008; 8 (44): 1-6. [ Links ]
20. Cohen CI, & Sokolovsky J. Schizophrenia and Social Networks: Ex-clients in the Inner City. Schizophrenia Bulletin, 1978; 4: 546-560. [ Links ]
21. Horan W, Ventura J, Nuechterlein K, Subotnik K, Hwang S, Mintz J. Stressful life events in recent-onset schizophrenia:reduced frequencies and altered subjective appraisals. Schizophrenia Research, 2005; 75 (3): 363- 374. [ Links ]
22. Chugg A, Craik C. Some Factors Influencing Occupational Engagement for People with Schizophrenia Living in the Community. British Journal of Occupational Therapy, 2002; 65 (2): 67-74. [ Links ]
23. Ludwig FM. How Routine Facilitates Wellbeing in Older Women. Occupational Therapy International, 1997; 4 (3): 215-230. [ Links ]
24. Sumsion T. A Revised Occupational Therapy Definition of Client Centred Practice. British Journal of Occupational Therapy, 2000; 63 (7): 304-309. [ Links ]
25. Eklund M, Erlandsson L, & Persson D. Occupational value among individuals with long-term mental illness. Canadian Journal of Occupational Therapy, 2003; 70 (5): 276-284. [ Links ]
26. Rugg G, McGeorge P. The sorting technique:a tutorial on card sorts,picture sorts and item sorts. Expert Systems, 1997; 14 (2): 80-93. [ Links ]
27. Kielhofner G. Research in Occupational Therapy: Methods of Inquiry for Enhancing Practice; Developing and Evaluating Quantitative Data Collection Instruments. Philadelphia: FA Davis Co; 2006. [ Links ]
28. Marwaha S, Johnson S. Schizophrenia and employment: a review. Social Psychiatry and Psychiatric Epidemiology, 2004; 39: 337-349. [ Links ]
29. Shimozono N, Usami S, Nakayama Y, Nozue K, Yano C. The Characteristics of Self-care Ability and Self-care support for Successful Community Living among Schizophrenic Patients Readmitted within 3 months of Discharge, or with Continued Hospitalization of more than 3 months in M-CBCM. Departmental Bulletin Paper, 2012; 8 (1): 31-45. [ Links ]
30. Charles C, Gafni A, Whelan T. Shared decision making in the medical encounter: what does it mean? (Or, it takes at least two to tango). Social Science and Medicine, 1997; 44 (5): 681-692. [ Links ]
 Correspondence:
Correspondence:
Rulaine Smith
Rulaine.Smith@wits.ac.za


{kind=link}