










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versión On-line ISSN 2310-3833
versión impresa ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 no.1 Pretoria ene. 2014
SECTION 1
Factors influencing model use in occupational therapy
Antonette OwenI; Fasloen AdamsII; Denise FranszenIII
IB. Occ. (Pret) MSc OT, (Wits); Lecturer, Department of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand
IIB.OT, MSc OT (Wits); Lecturer, Department of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand
IIIBSc OT (Wits), MSc OT (Wits); Senior lecturer, Department of Occupational Therapy, School of Therapeutic Sciences, University of the Witwatersrand
ABSTRACT
STUDY AIM: To determine which models are used by occupational therapists who attended a workshop on the Kawa Model, in their practice, the demographic factors related to the use of these models and the reasons why they use various models in their practice.
METHOD: A descriptive, single case study method was used with embedded units. The research instrument consisted of a survey questionnaire with closed and some semi-structured questions.
RESULTS: The characteristics of therapists influenced their use of models. This was determined by their educational background, their level of experience and exposure in the clinical field and their work setting. Time constraints and the nature of the presenting clients also played a role. The clinicians' overall attitude towards new theory and their habituated ways were highlighted as constant factors influencing model use. The use of models provides structure and assists occupational therapists to produce proper, profession-specific, scientifically-based intervention. Models taught during undergraduate studies need to be relevant to address clients' needs in their specific context.
Keywords: influencing factors on model use, application of models, why we use models
INTRODUCTION
The development of occupational therapy models has been influenced by the biomedical and bio-psychosocial models of health1. Reed2 and Kielhofner3 both identified four historical periods in the short history of the occupational therapy profession. The pre-formative period (1800-1899) was influenced by the Moral Treatment movement as well as the Arts and Crafts movement. The formative period (1900-1929) was influenced by the philosophy of pragmatism that was characterised by the development of foundational terms and concepts. The mechanistic period (1930-1965) was influenced by the philosophy of medicine and science using a quantitative approach. The models used by occupational therapy during the mechanistic period were borrowed from other disciplines.
During the modern period (1966-current) there has been a return to formative ideas and the acceptance of qualitative methods. According to Kielhofner4 there was a difference between the nineteen sixties and the nineteen eighties, when he proposed the emergance of a new paradigm with the introduction of the Model of Human Occupation (MOHO).There was also a view that Mary Reilly's Occupational Behaviour Framework5 and that of occupational science were the "introduction" to the models by Kielhofner and those that followed on from his model. The development of practice models reflected a deeper understanding of occupation in daily life as the focal point1 and occurred with the advent of the theories of occupational science in the 1980s1. Whiteford, Townsend and Hocking6 emphasised the return to the focus on occupation. This reaffirmation of focus is referred to as the "renaissance of occupation"6:61.
The "body-as-machine" metaphor from a biomedical understanding was integrated at this stage into an open systems theory by Kielhofner (1985) in the Model of Human Occupation (MOHO)4 by which humans were conceptualised as consisting of layers of mutually influencing systems. Their occupational performance was considered not only in relation to their impairments but also in relation to their psychosocial as well as the sociocultural external systems in which they lived. Individuals were viewed as open systems that received input from the external environment and then consciously acted on it1. However, the occupational therapy models developed during the 1980's retained the bio-psychosocial model of health, and still placed the focus on individual autonomy.
Categorisation of Models
During these four historic periods as identified by Reed2 and Kielhofner3, models for the practice of occupational therapy were grouped into three categories; generic or outcome models, programme models and specific practice/conceptual models7. These different perspectives have developed over time. Initially models aimed to simplify phenomena and provide structure, but current models aim to tie together a multitude of phenomena to make sense of the whole8.
The first generic/outcome models (1930-1975) focussed on individual adaptation and explained why occupational therapy was valuable, but did not explain how this value could be achieved in clinical practice. These models consist of a theoretical framework to describe, explain, guide and predict therapy outcomes in practice, without which occupational therapy would amount to little more than a disorganised, irrational service lacking utility and relevance7,8. Examples of generic/outcome models are that of occupational behaviour as described by Mary Reilly8 , which is based on the assumption that occupations are developmentally acquired, and the individual adaptation model as described by King9, that focuses on the relationship between the environmental demands and the individual's ability to meet those demands.
The second type of model i.e. programme models (1970-1995) focussed on how occupational therapy concepts could be organised to address a set of problems, in a particular diagnostic group. Programme models highlighted what was needed to make occupational therapy effective, but did not consistently indicate how to apply these resources to a specific clinical case7. The programme models were identified by Weimer10 as offering promotion, protection, correction, accommodation and/or identification. For example, programme models for correction would focus on providing treatment on already identified problems in order to improve an individual's functional capacity like sensory integration and neuro-developmental techniques.
Finally the specific conceptual models for practice offered an explanation on how to apply occupational therapy in the clinical context. These models organised occupational dysfunction and addressed performance dysfunction. They exist as evidence that our knowledge base is not just common sense, practised within the context of ordinary life1. Examples of such a model are the Model of Human Occupation3 and the Kawa Model11.
This study focusses on the last two categories, namely programme and conceptual models of practice. However, Kielhof-ner3 stated that the term 'model' in occupational therapy can be associated with a variety of frameworks or perspectives. He provided criteria for defining the characteristics of a conceptual practice model. Firstly it must have a solid grounding in practice, and secondly it must provide theory that addresses unique practice circumstances and supports the development of practice resources. In his book, Conceptual Foundations of Occupational Therapy Practice,Kielhofner3 identified several previously known frames of reference as conceptual models such as sensory integration, motor control, etc., based on his definition of what constitutes a conceptual model. Therefore, the term 'conceptual model' was used for the various modalities used by therapists in this study.
A criticism of the models used in occupational therapy is that they have been mostly developed and researched by occupational therapists with a Western world view, and are therefore not always applicable in the contexts of clients from Asian, African and Eastern countries12. Their clinical and cultural relevance needs to be explored in developing countries.
The occupational therapy profession needs to continue evolving and transforming in order to maintain social relevance and it seems that the development of practice models is an important aspect in this process13,14. Duncan13 describes this evolution as being related to one's ability to match a society's needs with an appropriate response. Hence the importance of conducting research on the use of current occupational therapy models in various settings and different countries, and to establish their clinical relevance in different cultures in order to ensure that our profession stays true to its philosophy by providing clients with a unique and relevant service12.
Why do we apply Models?
Models in occupational therapy can be seen to serve practice in the following ways: models make explicit the profession's assumptions about humans and occupation, and provide a "short-cut" that guides professional and clinical reasoning. Models further help to define the profession's scope of practice by providing a focus for intervention, and making explicit its domain of concern. Thirdly, models enhance professionalism and accountability by providing a certain status to the profession and assisting in ethical decision making. Models also assist the therapist in collecting information in a systematic and organised fashion. Finally, models guide intervention, and provide the profession with solutions1.
The decision on which model to apply clinically as suggested by Creek15 can come down to selecting not just one model, for it may not fully represent the diversity and unique role of the occupational therapy profession. Kielhofner16 supported this when stating that the multiple factors involved in the occupational functioning of an individual cannot be addressed by the application of a single model due to each model's specific focus, and that a combination of two or more models should be used to address complex needs.
The application of any of the conceptual models in practice is neither simple nor based on a straight-forward formula, but rather requires a sophisticated understanding of the specific model and its application8. Davies17 feels that the complexity in models is often missed by therapists, who take the simplistic diagram as a one-dimensional presentation of the concepts without comprehending the full meaning behind these concepts. Therefore it would be important to explore how models are interpreted and used by occupational therapists.
Aim of study
The aim of this study was to explore the perceptions of occupational therapists about the occupational therapy models that they currently apply in their clinical practice. The following objectives were set:
- To identify which conceptual models South African occupational therapists apply in their clinical practice, and why.
- To establish demographic factors related to model use in clinical practice.
METHODOLOGY
Design
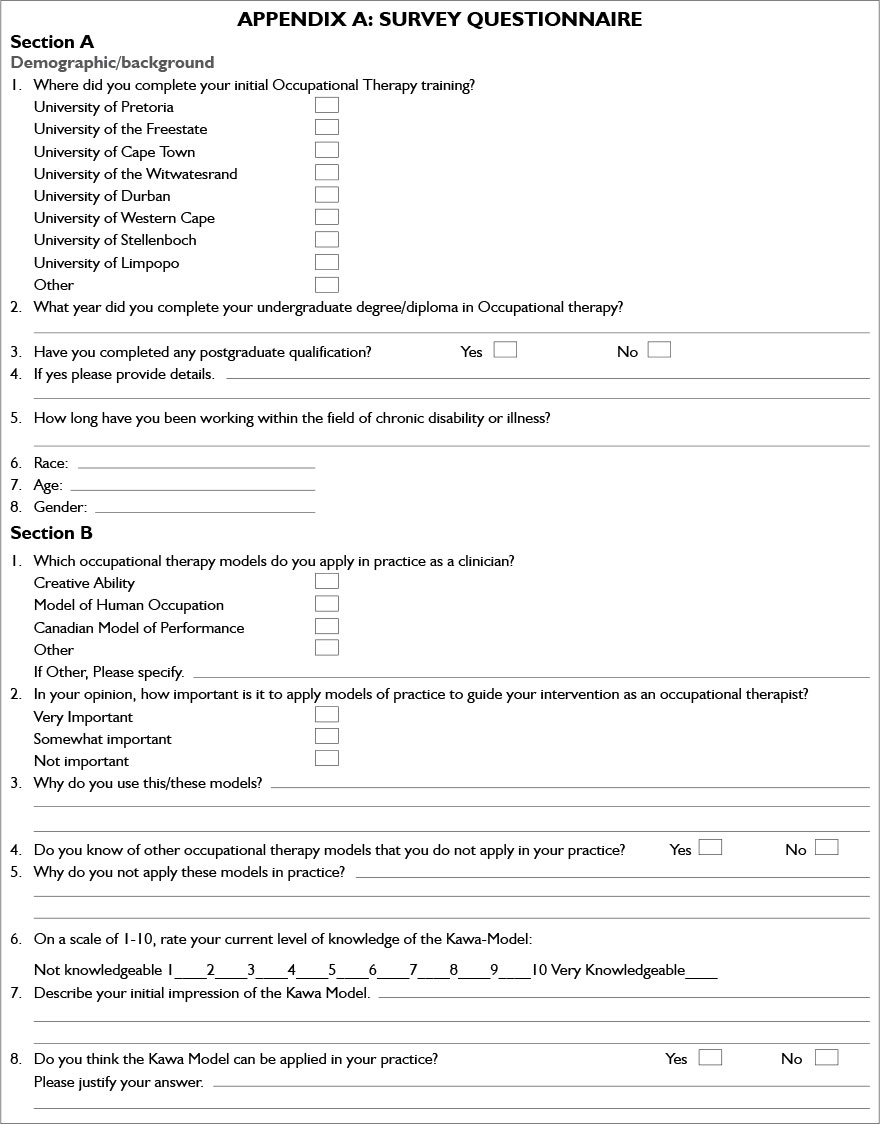
A descriptive, single case study was conducted with embedded elements using a survey method in the form of a questionnaire containing closed and semi-structured questions (Appendix A).
A preliminary phase was conducted with clinicians attending a workshop on models, while being introduced to a novel conceptual model, the Kawa Model11. Occupational therapists attending this workshop formed the population for this study. Only those who attended this preliminary phase were therefore invited to participate in the study for they all had the same view on what constitutes a conceptual model of practice.
Sample Selection
Registered occupational therapists who attended the preliminary phase workshop were invited i.e. convenient purposeful sampling was used in selecting information-rich participants18. The population consisted of a possible 35 participants. Five of these 35 were involved in the pilot study, leaving a possible sample of 30. Of this sample of 30, 27 met the inclusion criteria and 12 agreed to participate; indicating a response rate of 44,4%. The sample consisted of clinicians from both the public and private sectors.
Data gathering method and procedure
A questionnaire consisting of two sections was developed by the researcher. The first section gathered information on the demographics of the participants. The rest of the questionnaire focused on the perceptions and use of occupational therapy models. In order to ensure that questions were not ambiguous and that were interpreted in the same way by all participants, the questionnaire was piloted and changes made. Changes were mainly aesthetic; however, these changes did clarify the various sections of the questionnaire, ensuring that the right information was obtained under each section. Attendance at the preliminary phase course work allowed all respondents to have a similar view of what an occupational therapy model was18.
A questionnaire, an information letter and an informed consent form were e-mailed to participants. Two weeks after the initial date, research information was sent out again as a reminder. Questionnaires were returned via e-mail to the researcher's address or via fax to the university occupational therapy department, marked clearly for the attention of the researcher. On receipt of the completed questionnaires, codes were assigned and used from then onwards to ensure confidentiality and anonymity.
Data Analysis
Closed-ended answers on the questionnaire were analysed using percentage or the number of participants and frequency distributions. On the semi-structured questions, answers were analysed using percentages and descriptive content analysis to determine trends in the answers.
Ethics
An ethical clearance certificate was obtained from the University's Committee for Research of human subjects. The research-generated documentation was dealt with in strict confidence and the purpose of the study made clear, to enable participants to make an informed decision about their participation19. On the information letter it was made clear that completion of the questionnaires implies consent for information to be used. All research participants could withdraw from the research at any time without negative consequences.
RESULTS
The sample
The majority of the participants (n=7/12) worked within the private sector in the psychiatric field of practice. The data obtained may therefore be influenced by the fact that fewer data were obtained from the public service sector (see Table 1).
Application of models
Participants were questioned on their perception of the importance of applying models in practice. Half of participants (n=6/12) indicated that it was very important, with nearly the same amount of the participants (n=5/12) viewing it as somewhat important and only one participant (n=1/12) thinking it was not important at all.
A variety of occupational therapy practice models are currently used by the participants in their clinical practice (Figure 1). All of the participants identified using more than one model. Depending on the clients they treat; they select the most appropriate model.


Data obtained from semi-structured questions were analysed to determine the participants' perceptions of how they apply models clinically. Results indicated that there are several reasons why therapists use models in practice.
The responses from research participants made it evident that they felt that the application of models in clinical practice supported the philosophy that underpins and is inherent in occupational therapy. Four participants stated that they based their actual practice of assessment and treatment and deciding on outcomes on models of occupational therapy. This meant that the therapy was consistent with the values and beliefs about occupation and client centred practice that forms the basis of the profession. The following quote focuses on the philosophy of client centred practice within occupational therapy;
It is a tool that can be used to gain a better understanding of the client and thus guide treatment at the appropriate level, taking the client's needs into account. Participant B
One participant clarified this concept when commenting on the application of MOHO in staying true to the professions' focus.
(MOHO) helps to structure client's roles and responsibilities within their environment. Participant H
Participants also commented that models provide the theoretical concepts and structure on which they can reflect in order to enhance patient care. Fifty percent (n=6/12) of the participants felt that these selected models guide the occupational therapy process, by providing them with a foundation to work from. A participant from a private setting commented as follow:
I don't like to stick to boundaries, but it (models) gives you a basis to work from. Participant E
The use of models therefore assists in ensuring that treatment is not only appropriate in terms of scope and philosophy of occupational therapy but also supported the therapists' need to show evidence for the practice of the profession. Two participants were of the opinion that the application of models in practice supports their provision of occupation and evidence based therapy.
Two participants commented that the use of models when planning intervention facilitates their thinking process and helps them to select the appropriate intervention. Therefore using models in practice focusses their thinking and "doing". Models were considered the cornerstone of the "doing" in that they provide therapists with a framework for both assessment and/or treatment to guide intervention.
Five of the participants felt that the use of models actually enhanced the clients' participation and allowed their clients' needs to be met more effectively. By applying the models they had a better understanding of the clients' functioning from the client's perspectives, as seen from the quote below.
This ensures therapists has understanding of clients' values and priorities and can use these to guide treatment, thereby ensuring clients' participation and compliance. Participant H
On the other hand, seven of the participants highlighted the importance of applying clinical reasoning to each individual client in practice and not relying completely on the models chosen as a background guide to therapy as is indicated in this quote:
(I) think it's important to use some guidelines but not to get completely bogged down in models and forget to use clinical reasoning. Participant E
This point also relates to the importance of having an "open mind" when applying the models in practice. This was emphasised by three of the participants. In order to meet their clients' complex needs they sometimes have to extend their intervention to use more than one model, referred to as an eclectic approach. The following quote speaks to this:
It gives you a structure to work around..., but I like to keep my eyes open for other needs of the patient or parents and will then work outside the model... Be open minded. Participant K
Overall the participants indicate that models provide therapists with a collective voice, making it easier to explain what we do, for they are based on scientific, theoretical concepts. An experienced participant from the private sector stated the following:
OTs have difficulty to say what they do- models assist with this aspect. Participant C
Models are scientifically researched and build credibility to your treatment. Participant C
Model application related to employment sector, experience and type of qualification
Employment Sector
The use of occupational therapy models by participants in the public sector and those working in the private sector was considered. Participants working in the private sector apply a greater variety of models than those in the public sector who only use the Vona duToit Model of Creative Ability (VdTMCA) and the MOHO.
Participants working within the public sector were usually less experienced and had been qualified for a period varying from three to six years. The participants working in the private sector had a greater variety of experience and had been qualified for a period varying from four to over 20 years.
In the semi-structured questions four of the participants indicated that the setting in which they work as well the type of client has an influence on their use of models and they apply those that work in the setting. A participant working in a private setting motivated why she applies certain models in her paediatric practice.
It works for my type of patients. I understand the logic in the models and it is also logic to the parents of the children I am working with. Participant K
In contrast, a participant from the public sector felt that certain models were difficult to apply within her work setting in which patients often had little education and spoke languages different to that the therapist understood.
Difficult to apply to our patients and setting. Participant G
However, in some more reductionist settings, where the focus is on the presenting diagnosis mainly, participants indicated that the models might not be used to their full potential. A therapist working in a private hand therapy setting felt the models provided too much information, which might not be acted on as the clients are not viewed as comprehensively.
(These approaches are) most appropriate and quickest to apply to hand therapy clients in an environment where time with clients is limited. Participant B
Availability of time particularly in the private sector, was another factor that influenced the application of practice models as identified by two participants who reported using models to guide specific aspects that are assessed. They felt that in settings where there is time for taking a holistic view, other models may work well.
Experience and type of qualification
The number of occupational therapy models used by therapists was also described according to the number of years they have been qualified. Participants qualified for less than 10 years reported using four models in clinical practice, predominantly the VdTMCA and the MOHO.
Those participants that had been qualified for between ten and twenty years also still applied the MOHO most often; however the number of models they used increased from four to seven. Two of the therapists used the Kawa Model in their clinical practice. The number of models used increased from seven to eight for participants qualified for over 20 years. Therapists qualified for longer than 20 years used mostly the VdTMCA and three of these therapists were already using the Kawa Model regularly in their practice. It is evident that the variety of occupational therapy models applied in clinical practice increase in relation to the number of years a therapist has been qualified.
This was confirmed by the analysis of the semi-structured questions in terms of experience, where participants revealed that the more experienced therapists often also used models in combination with each other. Three experienced therapists reported that they prefer to apply an eclectic, "open" approach using different models together for their assessments and treatments, rather than focusing on one particular model / treatment technique.
There was also a difference between participants with under-graduate versus post-graduate degrees. These differences related to the type, variety and distribution of models applied by the two groups. Although both groups reported using six models in their clinical practice, the MOHO was more commonly applied by participants with an under-graduate degree. The VdTMCA was favoured by all participants, particularly by those with a post-graduate qualification and this model was used along with the Kawa Model by all of the participants with a post-graduate qualification. Therefore it appeared that post-graduate training is influential in therapists using the Kawa Model.
When the semi-structured questions were analysed it was found that the use of models was dependent on the educational background of those who apply them and the experience they have as occupational therapists.
Half of the participants (n = 6/12) trained at the University of the Witwatersrand. They reported that they had continued to use the two models taught during their under-graduate training ie the VdTMCA and MOHO and five of them, irrespective of whether they had a post-graduate qualification or not, reported this was because they tended to stay within the zone with which they were comfortable. There were no comments from graduates from the other universities.
The models that the participants reported using appear to be dependent on their exposure and knowledge of practice models and this determined the application in their practice. In this study participants within the public sector had less experience and therefore had had less post-graduate educational opportunities and exposure to new concepts. They lack knowledge about or experience of a variety of models and rely on those models and theories that were taught during their under-graduate studies as confirmed in a study by Crow and Kenny20 or do not use models at all as indicated by one participant in the following quote.
Don't know them well enough or haven't been exposed to them in practice, and as stated above, was never taught models as an under-graduate, so have been inclined to continue practising the way I always have, without using models specifically. Participant A
Thus both the participants' educational background and experience level determined their knowledge level and confidence in the use of models as seen in this quote:
I haven't had much experience or knowledge about the models to use them with confidence. Participant B
These aspects pertaining to the individual therapist need to be considered when applying models in practice.
DISCUSSION AND IMPLICATIONS
Influences on Model use
Participants in this study value the use of models in guiding them through the occupational therapy process, in providing evidence for practice, and in supporting the relevance of their interventions. This is in line with Kielhofner who stated that conceptual practice models offer theory to "guide practice and research in the field"14:3.
Although participants value the use of models, there are many factors that influence how they select and use models, such as those pertaining to the individual therapist applying the model. These factors include the value they placed on model use, their educational backgrounds, whether they had a post-graduate qualification, and how long they have been qualified for.
The initial receptive attitude from participants to new theory was positive, but it needs to be acted on. Kielhofner stated that a model of practice should be a way of thinking about and conducting practice, and must be constantly critiquedl6,2l. Therefore it is important for participants to have an open attitude when applying models, constantly review their application, and to explore alternative models to ensure that their interventions maintain relevance to the client group they serve.
Participants tend to apply models taught to them during their under-graduate studies. These results are in line with the literature that indicates that therapists tend to continue the application of models that were taught during their under-graduate training as there is an association between knowledge of theory and application of theory, resulting in the use of theories or models in clinical practice based on the therapists' educational backgrounds22,23.
It is important to note that post-graduate training appears to have made no difference to the use of models that were predominantly applied, with the MOHO and the VdTMCA still being used most frequently, irrespective of whether or not the participants have had further training.
The number and variety of models used increased with the number of years that participants were qualified. This gradual increase in theoretical knowledge and use was also evident in a study by Elliott, Velde and Wittman24 with participants stating that theory was learned at different stages in their professional development.
The choice and use of models also seems to be influenced by the therapists clinical reasoning skills which develop with experience. Interacting with theory contributes to the development of clinical reasoning skills23, leading to experienced participants' ability to critique a model and to identify strengths and weaknesses and apply that which suits them.
Therefore, experienced participants, apart from using more models, use a combination of models to substantiate their clinical reasoning. According to Boyt Schell and Schell25, therapists with five years' experience become proficient in clinical reasoning. All of the participants in the current study, working within the private service sector, had five or more years of experience and were therefore probably more confident in trying various models. The majority of participants in the public sector have less experience, so their clinical reasoning is still developing. It is therefore more difficult for them to do the same.
Apart from factors pertaining to the therapist, factors pertaining to the work setting influence the use of models, such as the focus of therapy, the phase of treatment of the presenting client, time constraints and opportunities to acquire and explore new knowledge.
Participants working in the public service sector experienced difficulty in using models consistently mainly due to the public practice context which is still bio-medical in nature. When operating within a bio-medical context, the presenting medical condition and the treatment of such is the main focus. The underlying, contributing factor to the client's current conditions seldom gets explored, for there is only enough time to tend to the specific reason for referral.
This treatment approach is not holistic, but rather reductionist in nature and contrary to the philosophy of the occupational therapy profession. The majority of participants working within the private service sector did not express the same concerns as they worked within a more bio-psychosocial health context.
In summary, a variety of factors influenced what value the participants placed on theory, the choice of models used by them, and their ability to use these models. These included, but were not limited to their educational backgrounds, their level of exposure and experience in the clinical field and their ability to apply clinical reasoning. Apart from these influencing factors on the use of models, two particular influences affected the above, namely their receptive/ open attitude towards models and their theoretical concepts, and their habituated ways when applying models.
Limited time for intervention, opportunity to acquire new knowledge and explore it, sector context and presenting clients were identified as influencing factors relating to the participants ability in applying models.
Influence of Models on 'doing'
The factors that influenced participants' choice and use of models had a further influence on how these models impacted on them 'doing' occupational therapy.
The level of experience of the participants was highlighted. The less experienced participants felt that models helped them to think more clearly and provided structure that they could follow in understanding the client and planning interventions. This need for a structure is an indication of the level of clinical reasoning obtained by this group of participants. They therefore use a particular model to guide them step by step.
These initial interactions with theory and models are vital in developing skills specific interventions and should be encouraged, as they guide participants in their practice and helps in the development of clinical reasoning25.
As skills and knowledge of model use develop and become more integrated, we can start to rely more on clinical reasoning and working outside of the model, as was seen from the results obtained from the more experienced participants within this study. Many of the experienced participants reported using an eclectic approach to models an approach supported by Kielhofner3.
Participants in this study were asked to articulate their use of practice models, but had more difficulty in explaining how these models affected their way of doing. This is attributed to the earlier findings that the use of models becomes habituated when used often, but it is difficult to explain exactly how they are applied. Participants, who were of the opinion that they do not use models, usually did when probed by the researcher. However, they did not think of it consciously, for the use of the model learned during under-graduate training had become habituated over time. According to Davies, models are internalised and they guide what we do to evaluate intervention. They are what we "carry with us and it manifests in a more subtle internalised fashion"17:56.
In summary, the use of models influenced the participants' way of doing occupational therapy by making overt the specific contribution of the profession. Model use provides structure to the intervention, which was especially important for the 'novice' therapists. The use of models provided participants with an understanding of their client, and their interaction with the model through clinical reasoning assisted them in their intervention. Experienced therapists expressed a need to work 'outside' of the model at times, and it is important to have an open mind when using models. The use of models becomes less overt and more habituated over time.
CONCLUSIONS
The aim of the study was to explore the perceptions of clinicians about the occupational therapy models that they currently apply in their clinical practice.
The factors that influence the selection and use of models were identified and fell into two groups. Firstly those that influenced "who they were" such as the value they placed on theory, their educational backgrounds, exposure to information, experience in practice and ability to apply clinical reasoning.
The second group of influencing factors pertained to where they worked. Limited time for intervention, lack of opportunities, the sector context and presenting clients were identified as having an impact on the choice of models used by clinicians. The impact of model use clinically was discussed and found to provide structure, and assists in profession specific, scientifically based intervention.
Limitations of the study
- Sample was limited to the number of therapists who attended the workshop on the Kawa Model.
- Quantitative data were limited by the small sample size.
- This study was only a first phase to a larger study.
- Attendance at a workshop on models with a focus on the Kawa Model might have influenced the results.
REFERENCES
1. Turpin M, Iwama MK. Using Occupational Therapy Models in Practice - A Field Guide. 1st ed. Toronto: Elsevier; 2011. [ Links ]
2. Reed KL. An annotated history of the concepts used in occupational therapy. In: Christiansen C, Bass-Haugen J, editors. Occupational therapy: Performance, participation and well-being. 3rd ed. Thorofare, NJ: Slack; 2005. 567-626. [ Links ]
3. Kielhofner G. Conceptual foundations of occupational therapy. Fourth ed. Philadelphia: FA. Davis; 2009. [ Links ]
4. Kielhofner, G. A model of human occupation: Theory and application. Baltimor: Williams & Wilkins; 1985 [ Links ]
5. Reilly M. Occupational therapy can be one of the great ideas of the 20th century medicine. American Journal of Occupational Therapy, 1962; 16: 1-9. [ Links ]
6. Whiteford G, Townsend E, Hocking C. Reflections on a renaissance of occupation. Canadian Journal of Occupational Therapy, 2000; 67(1): 61-69. [ Links ]
7. Reed KL, Sanderson SN editors. Concepts of Occupational Therapy. 3rd ed. United States of America: Williams & Wilkins; 1992. [ Links ]
8. Duncan EAS editor. Foundations for practice in Occupational Therapy. 4th ed. London: Elsevier Churchill Livingstone; 2006. [ Links ]
9. King LJ. Towards a science of adaptive responses. American Journal of Occupational Therapy, 1978; 32: 429-437. [ Links ]
10. Weimer RB. Some concepts of prevention as an aspect of community health. American Journal of Occupational Therapy, 1972; 26: 1-9. [ Links ]
11. Iwama M. The Kawa Model- Culturally Relevant Occupational Therapy. Irst ed. United States of America: Churchill Livingstone Elsevier; 2006. [ Links ]
12. Iwama M. Towards culturally relevant epistemologies in occupational therapy. American Journal of Occupational Therapy, 2003; 57(5): 582-588. [ Links ]
13. Duncan M. Our bit in the calabash: Thoughts on occupational therapy transformation in South Africa. South African Journal of Occupational Therapy, 1999; 29 (2): 3-9. [ Links ]
14. Kielhofner G, editor. Challenges and directions for the future of occupational therapy.Keynote address at the fourteenth congress of the World Federation of Occupational Therapists, Stockholm, Sweden; 2002. [ Links ]
15. Creek J. Occupational therapy defined as a complex intervention. London: College of Occupational Therapists; 2003. [ Links ]
16. Kielhofner G. Research in Occupational therapy: Method of inquiry for enhancing practice. Philadelphia, USA: F.A. Davies; 2006. [ Links ]
17. Davies S. Models and Theories. In: Reel K, Feaver S, editors. Rehabilitation the use of theories and models in practice. London: Elsevier; 2006. [ Links ]
18. Wood P Qualitative Research. 2006; Available at: http://www.edu.plymouth.ac.uk/resined/qualitative%20methods%202/qualrshm.htm. Accessed 11/29, 2012. [ Links ]
19. Occupational Therapy Association of South Africa. Code of Ethics and Professional Conduct. July 2005: Section A-Section E. [ Links ]
20. Crowe TK, Kenny EM. Occupational therapy practice in school systems: A survey of northwest therapists. Physical & Occupational Therapy in Paediatrics, 1990; 10 (3): 69-83. [ Links ]
21. Salminen A, Harra T, Lautamo T. Conducting case study research in Occupational therapy. Australian Occupational Therapy Journal, 2006; 53: 3-8. [ Links ]
22. Storch BA, Eskow KG. Theory application by school-based occupational therapists.American journal of Occupational Therapy, 1996; 50 (8): 662-668. [ Links ]
23. Rappolt S, Tassone M. How rehabilitation therapists gather and apply new knowledge. journal of Continuing Education in the Health Professions. 2002; 22 (3): 170-180. [ Links ]
24. Elliott SJ, Velde BF? Wittman PF? The use of Theory in everyday practice: An Explorative study. Occupational Therapy in Health Care 2002;l6(l):45-62. [ Links ]
25. Boyt Schell B, Schell, JW. Clinically and professional reasoning in occupational therapy. 1st edit, United State of America:Lippincott Williams and Wilkins, 2007 [ Links ]
 Correspondence:
Correspondence:
Antonette Owen
Antonette.Owen@wits.ac.za



{kind=link}