










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.44 no.1 Pretoria Jan. 2014
SECTION 1
Perceptions of the Traditional Health Practitioner's role in the management of mental health care users and occupation: a pilot study
Matty van NiekerkI; Abigail DladlaII; Nolwazi GumbiII; Luther MonarengII; Winston ThwalaII
IB.Occ Ther (Pret) MSc Med Bioethics & Health Law (Wits); Lecturer, Department of Occupational Therapy, School Therapeutic Sciences, University of the Witwatersrand
IIBSc OT (Wits); Final year occupational therapy students, Department of Occupational Therapy, University of the Witwatersrand at the time the study was conducted
ABSTRACT
Since 1992 discussions about the South African health care system highlighted the need for including traditional healers, because 80% of South Africans access them. Nonetheless, there is little formal collaboration between allopathic and traditional health practitioners.
The purpose of the study was to identify traditional healers' awareness of occupational therapy, their use of occupations in their interventions, the allopathic health practitioners' perception of traditional healers' role in managing patients with mental illness and whether referrals occur between the two health systems.
Convenient sampling was used to select research participants. Data for this descriptive study were gathered by means of a survey questionnaire containing open and closed-ended questions. Data were presented using descriptive statistics.
This pilot study suggests that traditional healers value occupations such as personal care and some use occupations in their practice. Results indicate, however that the traditional healers are not as familiar with occupational therapists as they are with community rehabilitation workers. The study also suggests mistrust on the part of allopathic and traditional health practitioners of each other. In the absence of research into cooperation between traditional healers and occupational therapists, this study is valuable in identifying research questions about the use and value of occupation.
Key words: occupational therapy, traditional health practitioners, occupation
INTRODUCTION
Allopathy, for the purpose of this paper, refers to "the treatment of disease by conventional means"1:36 and is used in the broadest sense of the word and includes persons who are traditionally part of the multi-disciplinary team working with mental health care users, i.e. psychiatrists, medical practitioners, psychiatric nurses, occupational therapists, psychologists and social workers. Here it is used in contrast to traditional healing carried out by practitioners of traditional African medicine in the community in which illness is thought to be the result of witchcraft, contact with impure objects or through neglect of the ancestors2. The term allopathic in reference to mainstream health care was preferred to "western", which is also found in the literature, because it was perceived to be more neutral.
The traditional health practitioners' (THPs') role in their communities in South Africa has long been acknowledged. Although the practice of traditional healing was illegal2,3 in terms of the Health Professions Act4 (HPA) prior to the democratisation of the country, there were organisations which registered THPs5 and THPs continued to practice in their communities6. It is reported that allopathic health care practitioners turned a blind eye to THPs and in some cases even collaborated with them informally2. The publication of the White Paper on the Transformation of the Health System7 in 1997 effectively decriminalised traditional health care and placed the role of THPs firmly on the health care transformation agenda2.
Despite reported informal collaboration between allopathic practitioners and THPs, there are no published studies on collaboration or even mutual points of interest between occupational therapists and THPs. Very little is known about THPs' knowledge of occupational therapy or the importance (if any) of occupation in traditional healing. In an open and democratic South Africa, greater collaboration in the interest of the patient will become increasingly necessary between occupational therapists and THPs, but this is difficult to establish in the current environment where there is no information available about practitioners' perceptions of each other, or of their knowledge of the other's profession.
LITERATURE REVIEW
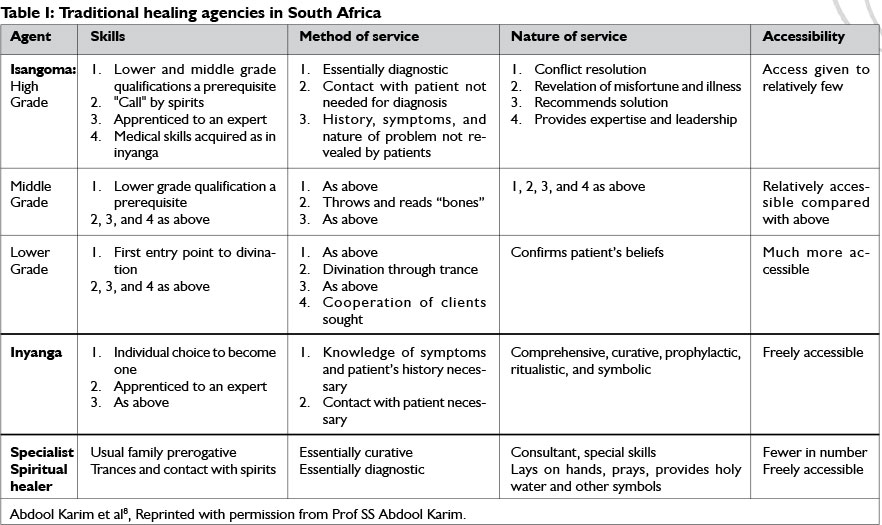
THPs are recognised as an integral part of their communities, where they are highly regarded and often shape their communities' thinking5. Ordinarily, a distinction is made in the literature between three types of THPs: the traditional doctor/herbalist or inyanga, who has an extensive knowledge of herbs and herbal treatment2,3; the diviner or sangoma who makes use of divination by consulting the ancestral spirits and the bones to diagnose and treat patients2,3, and faith healers, umprofethi or umthandazi, who mix Christian practices with traditional beliefs2,3. While some authors such as Ross3 assert that ordinarily the inyanga does not use divination and that the diviners do not use herbs3, Freeman and Motsei2 indicate that the classification of THPs is artificial. Some diviners do use herbs to treat and some traditional doctors do make use of divination2. Kale5 presented a breakdown of these three categories, as can be seen in Table I on page 21.
The Traditional Health Practitioners Act9 (THPA) as well as authors such as Ross3, Kale5 and Peltzer10 recognise two further categories of THPs, i.e. the traditional birth attendant, who must have at least two of her own children5,10 and who helps during the birthing process2,5,9, and the traditional surgeon who performs circumcision during initiation rituals2,5,10.
The literature is divided on the proportion of the population which accesses THPs. Figures as diverse as 80%3,5, 60-80%10, and 0.1% of the population10 are quoted. Pelzer, however, indicates that between 1995 and 2007 nationally representative studies show a decline in use of THPs as follows: between 1995 and 1998 3.6-12% of people accessed THPs, whereas 0.1% or fewer people accessed THPs between 2005 and 200710. However, he provides no reasons for this decline.
It should be borne in mind that THPs form part of the private health care sector and that patients have to make out-of-pocket payments to them10 (medical aid schemes do not cover THPs' services). A decline in accessing THPs could be attributed to factors such as the expense of out-of-pocket payments to THPs and/ or increased coverage of public health services and specifically primary health care services. Unfortunately there does not seem to be literature investigating reasons for this decline in accessing traditional health care services.
As early as 1992, shortly after the unbanning of political organisations including the African National Congress and the Pan Africanist Congress, scholars such as Freeman and Motsei2 discussed possible models that would allow for the integration of THPs into the health care system. Freeman and Motsei discussed three possible models: incorporation, where THPs are incorporated usually into the primary health care system where they are "first-line" practitioners; cooperation/collaboration, where the traditional and allopathic health care systems essentially remain independent and keep their individual methods of operation, but they recognise the value and contribution of the other and adopt a system of mutual referral; and total integration, which will require the development of a new health care system where traditional and allopathic health systems are intermingled and thus patients would receive treatment from both2.
This discussion on the integration of the THPs into the health care system remains relevant in South Africa, where there are not enough allopathic health care practitioners to render services to all South Africans11. Furthermore, an increase in health care personnel is required for service delivery in the planned National Health Insurance scheme. Peltzer10 indicates that while the National Department of Health (NDOH) supports collaboration between the allopathic health system and THPs on primary health care and HIV/AIDS prevention and education, the NDOH does not endorse referrals from the allopathic health sector to THPs. Their reasons for refusing to permit or facilitate referrals between allopathic health practitioners and THPs are that THPs and their medications are not regulated. In addition, there is no uniform system (or language) of diagnosing, treating and teaching and there is little formal evidence of the efficacy of traditional medicines9. Attempts have been made in South Africa to regulate THPs, with the promulgation of the Traditional Health Practitioners Act9 but Ross3 points out that this Act has been in abeyance because key role players cannot come to agreement.
Studies have reported that patients often view the causes of disease, especially mental illness, differently from allopathic prac-titioners6,12, viewing it to have cultural causes and not biological or genetic causes as allopathic practitioners may assert9,12. Cultural causes of mental illness may include bewitching, rape and "thinking too much"6:617 and because of the way in which this illness is viewed (i.e.as having a cultural cause), patients may rather consult THPs. Surprisingly, Petersen et al12 reported that approximately two-thirds of psychiatric patients consulted both the allopathic health care system and THPs. This suggests that there ought to be greater collaboration, or at least cooperation, between allopathic practitioners and THPs in the field of mental health.
Objectives of the study
The study aimed to investigate:
1. The perceptions of THPs regarding the importance of occupations such as work, personal care and leisure in the treatment of persons with mental illness and whether THPs use occupation-based activities in their treatment;
2. Their awareness of occupational therapy and community-based rehabilitation workers (CRWs) in the treatment of mental illness;
3. The perceptions of members of the allopathic medical team who work with mental health care patients of the role of THPs in mental health and
4. Whether referrals occur between the two health care systems.
METHOD
Study Design
A descriptive cross-sectional survey study design with a mixed method was employed. Because no prior occupational therapy research exists in this area, it was decided to conduct a pilot study to which a descriptive design was best suited as it would enable the researchers to describe findings so as to identify further research questions.
Study Sample
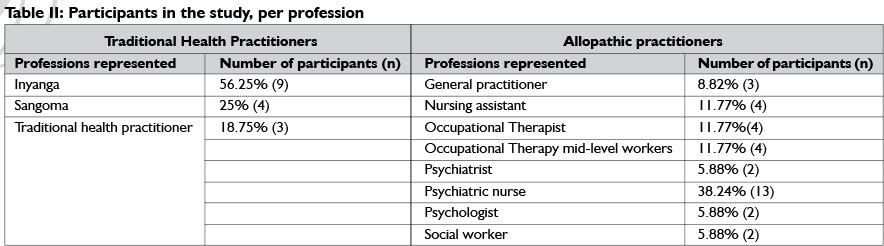
Research sites were selected based on convenience sampling, related to the places where four of the researchers were placed during fieldwork rotations in their final year of study. All health professionals who agreed to participate at those sites were included in the sample. Research participants were from Gauteng, Limpopo and Mpumalanga provinces and included both rural and urban areas. Health care practitioners who do not ordinarily work with mental health patients were excluded. Table II above illustrates the number of allopathic practitioners who participated in the study, per profession.
Traditional Health Practitioners
Originally it was thought that THPs could be identified through the Interim Traditional Health Professions Council register, but at the time of the research the Council was not yet operational. THPs were therefore identified by reference from community members living in the vicinity of the research sites; however as Table I above shows it is difficult to obtain access to some THPs. Sixteen THPs participated in the study (see Table II). .
Allopathic practitioners
In total 34 health professionals from a variety of professions at six sites were included in the sample (see Table II). Health care practitioners who did not work with mental health patients were excluded.
Data collection and analysis
Survey questionnaires containing closed and open-ended questions were used to gather data. Separate questionnaires were developed for use with the allopathic medical team and the THPs by the researchers. The surveys were checked for content and clarity by an experienced researcher in the Occupational Therapy Department of the University of the Witwatersrand. Questionnaires were initially sent to hospital-based participants by facsimile, but due to a very low return rate the questionnaires were hand-delivered to allopathic practitioners at the research sites as well as the THPs.
Questionnaires were collected from the allopathic practitioners in blank envelopes, but the THPs were found to have limited proficiency in English and therefore could not complete the questionnaires independently. Consequently, the questionnaires were used as the basis for structured interviews with the THPs in a language with which they were familiar. The researchers, who spoke a number of different South African languages, translated the questionnaires during the interviews, but did not deviate from the questions of the survey although at times they had to ask for elaboration.
Data from the closed-ended questions were analysed using descriptive statistics and is-represented in terms of percentages. Data from the open-ended questions were analysed according to the questions, by tabulating the responses using key words, as well as using descriptive statistics and percentages.
Ethical considerations
Participation was voluntary and confidential. Written consent was obtained from allopathic and THP participants to ensure voluntariness. To facilitate informed consent, the consent forms were explained verbally to THPs who could not read English. The consent forms were kept separately from the questionnaires so as to ensure confidentiality. Ethical clearance was obtained from the Wits Human Research Ethics Committee to conduct this research.
RESULTS
Results: Traditional Health Practitioners
Twenty-five per cent of THPs (n=4) indicated that they were aware of occupational therapy and 62.5% (n=I0) that they were aware of community rehabilitation workers. Following the closed ended question of whether the participants were aware of occupational therapists and community rehabilitation workers, participants were asked how they thought occupational therapists and community rehabilitation workers helped patients. While 62.5% (n=I0) participants indicated that they did not know, one participant indicated that he trains the family to care for the disabled person. A further 25% (n=4) participants said that occupational therapists and community rehabilitation workers do home visits. One of the participants said that he helped people who do not have care givers.
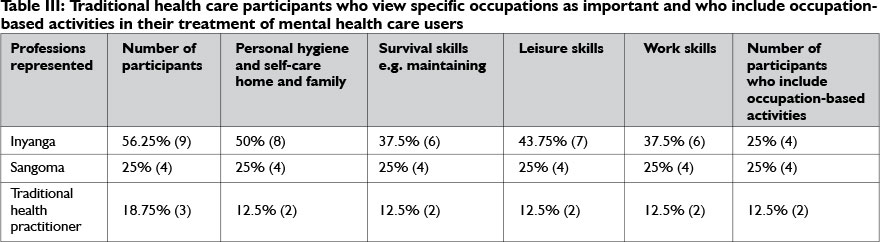
The results of this study also suggest that THPs view occupations as important. Personal hygiene and self-care were rated by 87.5% (n=I4) as important to address with patients, whereas 8I.25% (n=I3) participants viewed addressing leisure as important and 75% (n=I2) participants indicated that work and home / family maintenance respectively were important. Interestingly, one THP felt that a patient's work is a good indicator of the patient's state of mind and another thought that he knew that a patient was better if they could buy the correct goods at the spaza shop and return with the correct amount of change. However, another THP indicated that he did not use occupation-based activities, because patients needed care from others. As can be seen from Table III on page 22, fewer THPs than those who indicated that occupations are important actually incorporate occupation-based activities in their treatment.
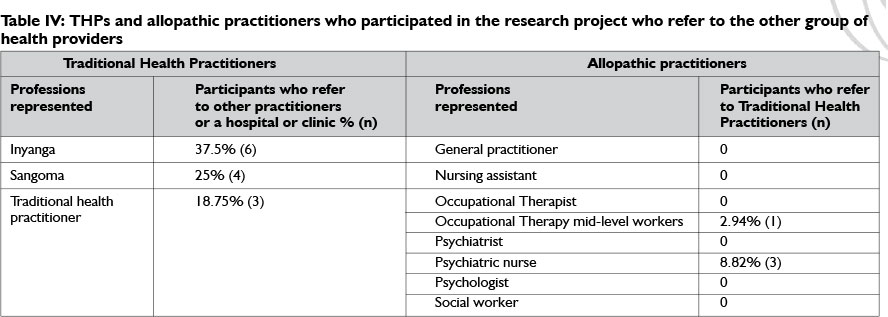
Of the THPs who participated in this study, 81.25% (n=l3) referred patients to allopathic practitioners (Table IV). On the open-ended question about the benefit patients would get from referral to clinics and hospitals, the THPs indicated that the benefits mostly related to their access to medication and medical treatment (62.5% (n=l0) participants), including sedation of aggressive patients for alleviation of pain. Two participants (12.5%) indicated that allopathic medicine helps with blood transfusions and stopping excessive bleeding.
A number of participants felt that there were disadvantages in referring to allopathic practitioners. Three participants (18.75%) indicated that allopathic medicine cannot treat evil spirits and another three participants felt that allopathic practitioners' treatment is not permanent. Two participants (l2.5%) reported that allopathic medicine cannot remove bad luck or misfortune and one participant was concerned that there was no referral back to the THP. Two participants reported that allopathic practitioners advise patients not to return for traditional health consultations.
Results: Allopathic health care practitioners
Approximately l00 questionnaires were sent to allopathic practitioners (including psychiatric nurses, occupational therapists, psychiatrists and psychologists), of which 37 were returned from the allopathic medical health care practitioners. Three of these had to be discarded, because only alternate pages were transmitted when they were returned to the researchers by facsimile.
Fifty per cent (n=l7) participants indicated that THPs have a role with mental health care patients, whereas 29.4l% (n=10) participants indicated they have no role and l7.65% (n=6) participants were unsure of whether they have a role. Of those participants who indicated that THPs have a role in mental health, 26.47% (n = 9) indicated that THPs' role is cultural, 11,77% (n=4) indicated that the role is to work together with allopathic practitioners and 8.82% (n=3) indicated that it is to administer traditional medication.
Only 11.77% (n=4) participants indicated that they refer to THPs (Figure 1). Participants who do not refer to THPs gave a variety of reasons for not doing so. Three participants (8.82%) indicated that the policy environment does not allow for or facilitate referral, and two (5.88%) (n=2) participants indicated that they do not know of any THPs. Three participants (8.82%) indicated that patients have a choice as to which health care facility they access and that health care practitioners should not influence a patient's decision and another three participants (8.82%) indicated that patients relapse when they consult with THPs and therefore they do not refer. Two participants (5.88%) indicated that patients cannot benefit from THPs and another two (5.88%) indicated that they will not refer because they do not believe in traditional healing. Other reasons for not referring included the lack of scientific basis (2.94% (n=l) participants) and the danger of interaction between traditional medicine and allopathic drugs (2.94% (n=l) participants).

DISCUSSION
The results of this study show interesting, heretofore unexplored points of mutual interest between occupational therapy and traditional healing. No research has considered the THPs' view on occupations and the inclusion of activities in their assessments and understanding of the patient with a mental illness before. This provides an important opportunity for collaboration between occupational therapists and THPs. Puckree et al11 reported comparable findings in relation to the profession of physiotherapy, i.e. that traditional healers use techniques similar to steaming, hot compresses and massage as used by physiotherapists. There is, however, no research on any similarities in the treatment offered by traditional healers and occupational therapists, although both consider the psychosocial and physical outcomes for the patient, even though their beliefs about the cause of the health problems differ. Despite this, there seems to be little collaboration between rehabilitation specialists such as occupational and physiotherapists, and THPs.
Undoubtedly, the delay in regulating THPs, and the NDOH's subsequent reluctance to sanction a formal referral system between THPs and allopathic practitioners are making it difficult for any practitioners in these systems to collaborate with each other - which this study confirms. However, delays in official recognition of collaboration should not stifle informal collaboration, although referral at this stage seems more one-sided (Figure 1) with THPs recognising some benefits of allopathic health care. This research indicates willingness on the part of the THPS for patients to access both types of care, but the allopathic health care practitioners on the other hand do not appear to recognise the benefits and importance of THPs in providing health care services. Interestingly, of those allopathic practitioners who participated in this study, only professional nurses and an occupational therapy technician referred to traditional healers. This may be reflective of those practitioners' recognition of the patients' psychosocial needs.
There is no question that there are not enough allopathic health care practitioners to adequately address the health care needs in South Africa2,12. With up to 80% of the population accessing THPs2,6,12 and many patients reported to access both allopathic and traditional health care services simultaneously, it is imperative that allopathic and THPs find ways to work together, to the benefit of the patient.
Occupational therapists should also capitalise on the points of mutual interest between occupational therapy and traditional healing to embark on research to improve understanding of how THPs provide treatment, so that communication and collaboration with them can be increased to ensure adequate health care for all South Africans, at least at primary health care level. The importance of providing collaborative support in the presence of limited occupational therapy services in conjunction with community rehabilitation workers and other support staff needs to be considered.
CONCLUSION
Unfortunately little progress has been made to date in regulating traditional healing in South Africa. As a result, a large barrier to creating an integrated health care system to the benefit of the patient cannot be removed. While the sample of this study is small, this study found that some THPs use occupations and occupation-based activities as an indicator of a patient's improvement. This mutual interest between occupational therapy and traditional healing should be used as an opportunity to collaborate with THPs. Further research should be conducted regarding THPs and the use of occupation, as well as possible collaboration between occupational therapists and THPs.
Limitation
Because this study is small, the results are not generalisable.
CONTRIBUTION OF AUTHORS
The second to fifth authors conducted the study as part of their final year research project and collected all the data. The first author was the study leader and re-analysed the data for this paper. The first author produced the paper.
REFERENCES
1. Pearsall, J (Ed). The concise Oxford dictionary. 10th Edition. Oxford: Oxford University Press, 1999. [ Links ]
2. Freeman M, Motsei M. Planning health care in South Africa - is there a role for traditional healers? Soc Sci Med, 1992; 34(11): 1 183-1 190. [ Links ]
3. Ross E. Inaugural lecture: African spirituality, ethics and traditional healing - implications for indigenous South African social work education and practice. SAJBL, 2010; 3(1): 44-51. Available at: http://www.ajol.info/index.php/sajbl/article/view/69949 (accessed 8 July 2013). [ Links ]
4. Health Professions Act No 56 of 1974. [ Links ]
5. Kale R. Traditional healers in South Africa: a parallel health care system. BMJ, 310: 1182-1185. [ Links ]
6. Campbell-Hall V Petersen I, Bhana A, Mjadu S, Hosegood V Flisher AJ, MHaPP Research Programme Consortium. Collaboration between traditional practitioners and primary health care staff in South Africa: developing a workable partnership for community mental health services. Transcultural Psychiatry, 2010; 47: 610-628. [ Links ]
7. Department of Health. White paper on the transformation of the health system in South Africa. Pretoria: National Department of Health. 1997. [ Links ]
8. Abdool Karim SS, Ziqubu-Page T, Arendse R for the Medical Association of South Africa. Bridging the gap. Project report. Durban: South African Medical Research Council, 1992. [ Links ]
9. Traditional Health Practitioners Act No 22 of 2007. [ Links ]
10. Pelzer K. Traditional health practitioners in South Africa. The Lancet, 2009; 374: 956-957. [ Links ]
11. Puckree T, Mkhize M, Mgobhozi Z, Lin, J. African traditional healers: what health care professionals need to know. International Journal of Rehabilitation Research, 2002; 25: 247-251. [ Links ]
12. Petersen I, Bhana A, Campbell-Hall V Mjadu S, Lund C, Kleintjes S, Hosegood V, Flisher AJ, Mental Health and Poverty Research Programme Consortium. Planning for district mental health services in South Africa: a situational analysis of a rural district site. Health Policy and Planning, 2009; 24: 140-150. [ Links ]
 Correspondence:
Correspondence:
Matty van Niekerk
matty.vanniekerk@wits.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}