










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.43 no.2 Pretoria Ago. 2013
SCIENTIFIC ARTICLES
Current practices in the assessment of hypotonia in children
Pragashnie Naidoo
B.OccTh (UDW), M.OccTh (UKZN), CAMAG (ABIME) Senior Tutor, Discipline of Occupational Therapy, School of Health Sciences, University of Kwa-Zulu Natal
ABSTRACT
The assessment of muscle tone is a fundamental component of the neurological examination of infants and children and is often crucial in the establishment of an accurate diagnosis and appropriate management. However, the accurate identification and quantification of muscle tone, particularly in the clinical setting continues to pose a challenge for clinicians. An electronic survey was used to determine the current practices of Paediatric Occupational Therapists, Physiotherapists, Paediatric Neurologists and Paediatricians in the assessment of hypotonia. Three hundred and nineteen (319) responses were eligible for data analysis utilising SPSS 18. Results are described descriptively and indicate that practices vary. The need for more objective measures in assessment was also strongly indicated.
Key words: hypotonia, clinical characteristics, assessment methods
INTRODUCTION
This paper describes a cohort of clinician's (occupational therapists, paediatricians and physiotherapists) current practices, challenges and difficulties in the assessment of hypotonia in the paediatric population. In children with neurological or neurodevelopmental dysfunction or delays, be it mild or severe, the presence of muscle tone abnormalities is often one of the presenting deficits. Abnormality in muscle tone is commonly classified into hypertonic or hypotonic groups1. Whilst methods for the clinical assessment of hypertonia have been widely reported and critiqued, with the development of assessment scales2-8, the clinical evaluation of hypotonia is one of the aspects of the diagnostic process that often remains subjectively assessed, and thus creates a dilemma for clinicians. The scientific community is yet to gain consensus on the operational definition, diagnostic criteria used to determine hypotonia and assessment techniques for evaluation of hypotonia9,10.
Although the term "hypotonia" is utilised frequently amongst healthcare professionals, there appears to be little evidence to definitively conclude that clinicians who use the term hypotonia are indeed describing the same phenomenon9,10. Hypotonia can be a confusing clinical presentation, often leading to inaccurate evaluation and unnecessary investigations11,12. The clinical reality of examining muscle tone is that the assessment is most often subjective in nature, which is frequently indicated in the literature6,13-15.
As therapists become increasingly involved in early examination, evaluation and intervention programmes, the accuracy of early assessments becomes imperative in order to contribute to rational decisions for intervention strategies16. Accurate assessment and diagnosis is also essential in to order to predict clinical course, manifestations, complications, prognosis and provide parental counselling.
LITERATURE REVIEW
Muscle tone is described as the resistance experienced by the examiner to movement of limbs around joints1,17,18. Authors distinguish between passive19, phasic6,18 and postural muscle tone6,18.
Hypotonia is considered to be "abnormally diminished muscle tone or floppiness"17. It may be acute or chronic, progressive or static, isolated or part of a complex clinical situation affecting children of all ages. It may or may not be associated with weakness. Functionally, it may be described as diminished resistance to movement as a limb is passively moved through a range of motion about a joint17.
Hypotonia is caused by disorders that affect any level of the nervous system, viz. brain, brain stem, spinal cord, peripheral nerves, neuromuscular junction and muscle12. Despite the underlying causative factors, the clinical presentation of hypotonia is considered to be similar in most cases20. It is this initial clinical assessment that is reportedly an important aspect of the diagnostic process6,9,10.
The classification of hypotonia has been approached in various ways, with most of the literature indicating a distinction being made between hypotonia of central origin and peripheral origin11,13,18,21,22,23. This is supplemented with a list of procedures and processes that assist with a differential diagnosis, the initiation of which is often based on a clinical opinion of muscle tone and by a process of exclusion by the diagnostic clinician9,10,13. However, the clinical appearance can often present as confusing leading to inaccurate evaluation and unnecessary investigations9,10,11,13.
Some authors indicate that decreased tone, floppiness or hypotonia in infancy may be transient and resolve without future problems or may be caused by serious, permanent disease originating in the central nervous system, spinal cord, anterior horn cell, neuromuscular junction or muscle24.
In the last two decades, child neurology has experienced significant progress, especially within the fields of genetics, molecular neurobiology and neuro-imaging diagnostic techniques25. However, despite the many advances in diagnostic techniques, the importance of the clinical assessment of infants with hypotonia cannot be overstated. Differentiating the likely causes of hypotonia is important in sparing some infants and children from invasive diagnostic tests such as muscle biopsies. Some underlying causes of hypotonia relies on clinical and developmental assessments because there are no laboratory or imaging tests13. In genetic cases it is important to reach the accurate diagnosis so that counselling may be undertaken.
Most studies have accentuated the major role of the physical or clinical examination in the evaluation of hypotonia26-29, but only a few studies, most of which were retrospective, were found to confirm this statement14,22,30,31. In a retrospective analysis of clinical experience in a tertiary care facility, on a selected population of infants with hypotonia who underwent genetic/neurologic evaluation over 11 years, the results supported the value of the clinical examination. Of the 89 floppy infants included in the analysis, a definitive diagnosis was established in 60 infants, and of the 60, 40% of the cases were diagnosed purely on clinical grounds31. In another retrospective study on 144 neonates14, the authors aimed to assess the reliability of the first physical examination as well as the contribution of the main standard diagnostic tests in the diagnosis of neonatal hypotonia. Infants diagnosed between 1999 and 2005 were retrospectively included in the study. The results indicated that the initial physical examination, could correctly identify the type of hypotonia in eight out of ten eventually elucidated cases. In another 11-year retrospective cohort study, intended to describe the diagnostic profiles of neonates with hypotonia who were admitted to an intensive care unit 22, the authors concluded that the diagnostic profile of neonates is diverse and careful clinical observation is critical to the proper evaluation of these children. In a study to establish the degree of inter-rater reliability amongst paediatric physical therapists in the assessment of muscle tone in children, aged between birth to three years, eighteen children were evaluated by a group of three raters. The testing protocol included observation of each child's movements followed by use of the rater's preferred method of evaluation. A low reliability in the clinical setting was found with the author indicating that therapists should be cautious regarding clinical decisions based on an assessment of muscle tone. Inter-rater reliability was affected by, inter alia, the following the lack of a standard technique of method for assessing tone and the lack of consistent terminology to describe tonal state and severity32.
This study thus aimed to describe the current practices and challenges of clinicians in the assessment of hypotonia. The findings of this study provided the initial data required, for a move towards consensus in the assessment of hypotonia (currently in press).
METHODS
A non-experimental survey design using an electronic survey generated on SurveyMonkey was used. Non-probability, purposive (maximum variation) sampling was employed. The development of the survey is discussed followed by a description of the use of the survey in data collection.
Development of the Survey
Following an appraisal of the literature, a manual search of articles for characteristics associated with hypotonia, as well as tests and methods used in it's clinical assessment, was conducted. Consultations with two paediatric neurologists, a neurodevelopmental paediatrician, a paediatric occupational therapist and the researcher's experience within the neurodevelopmental field of paediatrics, assisted in the development of the instrument.
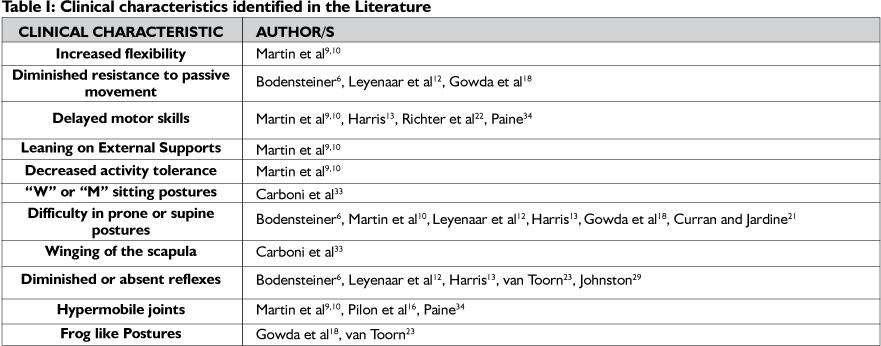
Characteristics of hypotonia compiled from the literature were collected and are highlighted in Table 1. Eleven characteristics were identified, viz. increased flexibility, diminished resistance to
passive movement, delayed motor skills, leaning on external supports, decreased activity tolerance, "W" or "M" sitting postures, difficulty in prone and supine postures, winging of the scapula, diminished or absent reflexes, hypermobile joints and frog-like postures.
All ll characteristics identified in the literature were included in the questionnaire, together with four additional characteristics that were identified during the appraisal stage. These included rag-doll postures, co-contraction, postural asymmetry and postural fixation.
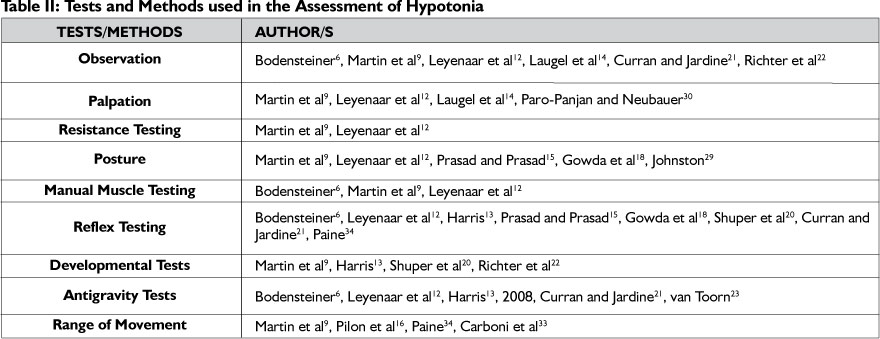
A further search to determine the tests and methods used in the assessment of hypotonia was initiated. Eight options from the literature were listed in the final questionnaire in addition to an option of "no formal testing". These tests and methods are presented in Table 2.
The final survey comprised 10 questions, using multiple choice and Likert-scale, closed-format responses. The researcher allowed for some flexibility of response by including an "other" as a possible response category in some questions.
Survey Piloting
A multi-stage testing process was undertaken in the piloting of the survey35. A review by knowledgeable experts (2 paediatricians, a paediatric neurologist and a paediatric occupational therapist) indicated question completeness, efficiency, relevancy and format appropriateness. The electronic survey was then piloted on five occupational therapists in general practice. A "think-aloud" protocol was observed in which survey language, question interpretation and the survey "look and feel" were evaluated35. The final stage involved a check for general and typographical errors that may have inadvertently been introduced during the final revision process.
Ethical considerations
Following institutional ethical clearance, informed consent from all participants was received, with participants being assured about issues of confidentiality, proper data management, scientific honestly in reporting, and the right to withdraw.
Data Collection
Data collection was done by means of the survey described above. A short introduction to the study was provided in an e-mail with a hyperlink to the survey. SurveyMonkey allowed for different collector links, therefore three hyperlinks were created to send to different participant groups so that the researcher was able to determine which groups of individuals required repeated e-mails. Participants were encouraged to click on the link and complete the survey. Attachments on the e-mail included the researcher's affiliation as well as contact details and a covering letter explaining the purpose of the research.
The three clinical disciplines included in this study were considered homogenous in their approach to hypotonia testing. The questionnaire was distributed to approximately 1500 registered professionals within the paediatric groups registered with the Occupational Therapy Association of South Africa (OTASA), the Paediatric and Neurodevelopmental Association of South Africa (PANDA), the South African Paediatric Association (SAPA), the Paediatric Management Group (PMG), hospital and clinic listings (Netcare, Mediclinic, Medicross, PrimeCure, Lifehealth Care), as well as Medpages listings of occupational therapists, physiotherapists and paediatricians. The South African Society of Physiotherapy was contacted but indicated that they did not send out group emails. A listing of paediatric physiotherapists was thus retrieved via sub-groups (viz. Physioinfo, a Physiotherapy website and the Physiotherapy Pain Management Group).
Participants were encouraged to complete the questionnaire if they met the following inclusion criteria:
They had to be currently registered with the HPCSA
They had to currently be in paediatric practice, either within the fields of occupational therapy, physiotherapy or paediatrics (including paediatric neurology).
Data Analysis
Excel spreadsheets were exported from SurveyMonkey. The Statistical Package for the Social Sciences (SPSS) version 18, was used to analyse the data. Descriptive statistics were used in order to describe and summarise data into an organised, visual representa-tion36. Cross tabulations were derived from the data that allowed the researcher to explore trends in data against professional group, age and level of experience variables.
RESULTS AND DISCUSSION
A total of 320 questionnaires were completed with 319 being eligible for analysis. The required amount of responses was set to 306, for results to be representative of the population, with a confidence level of 95%, therefore enough questionnaires were returned to be representative. Occupational therapists appeared to have responded to the research more positively (65.3%) as compared to the other two disciplines, physiotherapists (21.3%) and paediatricians (13.4%). The majority of the respondents fell within the 30-39 age range (36.9%). There was however representation from all ranges i.e. 20-29 years up to >59 years.
Within the sample, a high number of clinicians (48.1%) possessed greater than ten years experience within the paediatric field. Additionally, most of the respondents had engaged in some form of postgraduate study, in fields related to paediatrics.
A high number of occupational therapists possessed qualifications in sensory integration (58%), with a high number of physiotherapists demonstrating qualifications in Neurodevel-opment (59%). Paediatricians, in addition to their specialty, possessed additional qualifications in fields of Early Childhood Intervention/Development, Neurodevelopment and Paediatric Neurology.
Challenges experienced by Clinicians
The majority of respondents indicated that difficulties in assessment were experienced, with a small percentage indicating no difficulties (9%). The subjectivity of clinical assessment (70%) and difficulty in quantifying hypotonia (78%) were most frequently indicated.
Authors of papers on evaluation of hypotonia often emphasise the challenge in clinical assessment as it may be the sign of both benign and serious conditions.6,12 Confusion in terminology related to hypotonia were cited in papers almost five decades ago34,37 and results from this study still indicates challenges in the assessment.
A small percentage (16%) indicate that the exclusion process with clinical assessment was difficult. Despite the many advances in diagnostics, difficulties in the assessment of infants with hypotonia cannot be overstated. Differentiating the likely causes of hypotonia is important in sparing some infants and children from invasive diagnostic tests such as muscle biopsies. There are also a number of underlying causes of hypotonia for which there is NO definitive laboratory or imaging tests, namely idiopathic hypotonia, so the role of clinical and developmental assessments remain important13.
Age category most difficult to assess
A small percentage of respondents indicated difficulties in assessment of the older child (19.7%), probably due to their ability to co-operate with a structured neurological examination38.
More significantly, respondents in this study indicated that the zero to one year (30.3%) and two to five year (35.9%) age ranges were most difficult to assess. Assessment of the 2 to 5 year age range may be difficult for a number of reasons, viz. the continuous developmental changes of the brain during infancy and childhood can lead to a disappearance of signs of dysfunction present at an early age. The reverse is also said to occur where children can be free from signs of dysfunction with deficits becoming evident with increasing age due to the age-related complexity of neural functions39.
Clinical characteristics and methods used to assess hypotonia
Trends were interesting with respect to each of the clinical disciplines response to clinical characteristics and methods and tests that are utilised in the assessment of hypotonia.
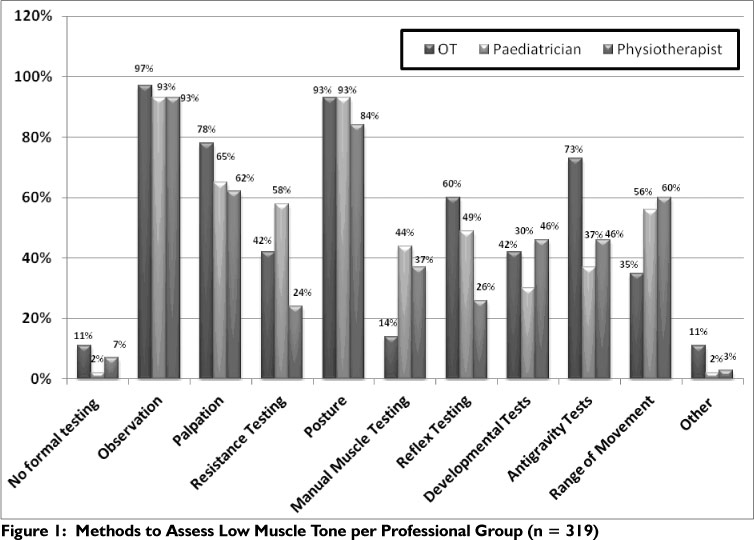
All three disciplines (Figure 1 on page 15) indicated that observation was a method of choice (96%). This was reinforced in the literature6,10,12,14,21,22. Assessment of posture was also indicated commonly amongst respondents (91%). Postural assessment was re-iterated by authors of papers on hypotonia10,12,15,18,29.
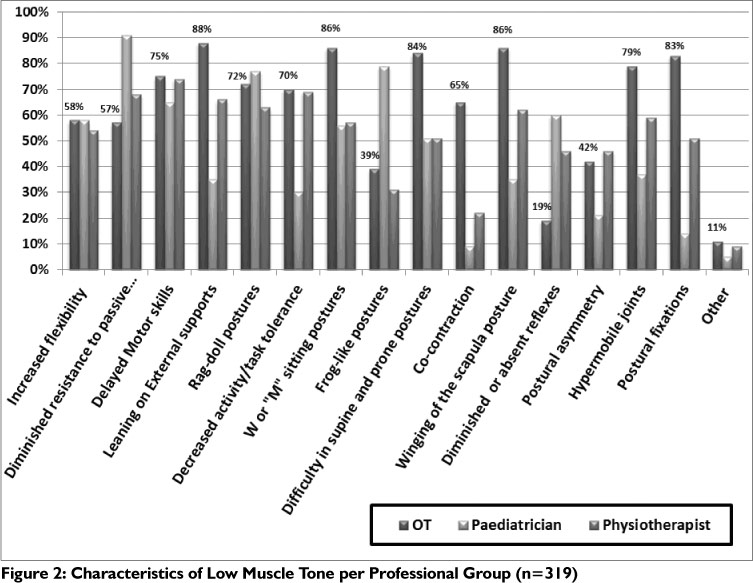
Of the 15 listed clinical characteristics (Figure 2 on page 15), those that were most frequently indicated were related to posture, viz. leaning on external supports (76.3%); "W" or "M" Sitting (75.9%); winging of the scapulae (73.8%) and rag doll postures (70.9%). Difficulty in antigravity postures such as prone extension and supine flexion was also frequently indicated (72.5%).
Palpation was also found to be commonly used by respondents in the assessment of hypotonia (73%). See Figure I. In addition, only 63.4% of respondents indicated diminished resistance to passive movement as being a characteristic (Figure 2) that is considered when assessing hypotonia. This is interesting, as hypotonia is defined as "abnormally diminished muscle tone or floppiness"17 that is determined in part by the actual palpation of musculature. Functionally it may be described as "diminished resistance to movement as a limb is passively moved through a range of motion about a joint"17. Paediatricians (91%) indicated diminished resistance to passive movement more frequently (Figure 2) as compared to physiotherapists (68%) and occupational therapists (57%), whilst occupational therapists indicated palpation (78%) more frequently as a method (Figure 1) compared to paediatricians (65%) and physiotherapists (62%). This reinforces the need for the study as confusion even in the definition of hypotonia appears to be reflected in these responses.
Increased flexibility (57.2%) and hypermobile joints (68.8%) were frequently indicated as a characteristic by the collective group (Figure 2). Occupational therapists (35%) however (Figure 1), indicated testing of range of movement less frequently as compared to the physiotherapists (60%) and paediatricians (56%). Physiotherapists (24%) indicated resistance testing less frequently (Figure 1) compared to occupational therapists (42%) and paediatricians (58%), whilst occupational therapists (14%) reported manual muscle testing less frequently than physiotherapists (37%) and paediatricians (44%). This discrepancy is interesting as the manual muscle testing grades are based on resistance testing.
The interconnection between muscle tone, strength and joint mobility is appreciated in the consideration of what muscle tone is, the resistance of passive movement around a joint18. A key distinc- tion is to determine whether a child has hypotonia with or without weakness6,l2. This is relevant as the diagnostic approach to a child with and without weakness differs and has varied implications6,23. In the younger child, muscle power is said to be best assessed by studying spontaneous movements and looking at anti-gravity movementsl8,2l, whilst the older child may be in a better position to understand instructions related to testing38.
Interestingly, the least indicated characteristic (Figure 2) was diminished or absent reflexes (30.3%) and collectively reflex testing (Figure 1) also yielded a low response (32%). Literature however indicates that the deep tendon reflexes are considered to be the most valuable aspect of the physical examination. Brisk reflexes indicate central nervous system dysfunction and diminished or absent reflexes point strongly to disorder of the lower motor unitll,l2,2l. Diminished reflexes and decreased antigravity limb movements are said to be suggestive of a peripheral disorder22. More paediatricians (49%), than occupational therapists (30%) and physiotherapists (26%) indicated this as a test used in their assessment (Figure 1). This significant discrepancy may be related to training of these professionals as well as the fact that occupational therapists and physiotherapists are not directly involved in diagnosis.
The use of antigravity tests (Figure 1) yielded an overall response of 62%. The occupational therapists (73%) were inclined to use this more often than physiotherapists (46%) and paediatricians (37%). This may be attributed to the fact that occupational therapists are more often involved in developmental testing with use of tests that include antigravity postures e.g. Clinical Observations of Neuro-muscular Function, based on the work by Dr Jean Ayres39. Authors of papers on assessment of the low toned infant with hypotonia however have emphasized the value of antigravity positions in the neurological assessment6,l2,l3,2l,23.
In the "other" category (Figure 1) the following were listed: specific developmental and sensory integration tests (e.g. Miller Assessment for Preschoolers40 and Clinical Observations of Neuromuscular Function39); collateral information (e.g. from teachers and parents); interviews; and functional assessments. It was interesting to note that the Modified Ashworth scale4l was also listed, although this test is used in describing hypertonia and not hypotonia.
Additional characteristics listed by respondents under the "other" category, included aspects covering posture (viz. impaired postural alignment, pronated feet, protruding abdomen, increased kypho-lordosis); reduced balance; excessive drooling; poor endurance; muscle weakness; and hypotonic facies.
Inconsistency in Assessment amongst professionals
Although the term "hypotonia" is utilised frequently amongst healthcare professionals, there is limited evidence to definitively conclude that clinicians who are using the term are describing the same phenomenon9,10. When probed about the frequency with which clinicians differ in opinion regarding assessment, on a 5-point Likert scale ranging from "never" to "always", 46.8% of all the respondents indicated some contention to a lesser or greater degree (sometimes, often, always).
This becomes significant, in that, for effective management a team approach is essential in ensuring that the child is diagnosed as early and accurately as possible, as well as in being able to access the relevant interventions. This necessitates a team that is able to communicate effectively by using the same terminology and drawing similar conclusions from their evaluations.
Parents of children that seek second opinions should also receive consistent and accurate information in order to build the professions reputation to the consumer of the service. When asked about additional challenges experienced, respondents further indicated that there were differences in the professional groups (e.g. "occupational therapists and physiotherapists differ on hypotonia") as well as having "disagreements with medical practitioner's findings". These inconsistencies are also impacted by a lack of objective measures as described below.
The need for objective measures
The majority of respondents indicated that there was a need for objective measures to assess hypotonia (87.8%). The clinical reality of examining muscle tone is the assessment which is often subjective in nature. This has been frequently indicated in the literature6,9,10,13,14,15,30. The absence of implicit and objective measures or assessment guidelines appears to compromise the ability of clinicians to adequately define and describe a child's hypotonia in a uniform and comparable manner. If this confusion persists, clinicians will continue to face the difficulty of accurately and consistently identifying children with Hypotonia as well as diagnosing the underlying cause. This may lead to a series of negative consequences which include proper management of these children as well as difficulty in conducting further research on the efficacy of intervention strategies. The response on this question further reinforced the value of the study.
CONCLUSION
This descriptive study highlighted some of the current practices and difficulties experienced by a cohort of clinicians (occupational therapists, paediatricians and physiotherapists) in the assessment of hypotonia. The use of an electronic survey assisted in accessing a sample of 319 respondents. There was adequate distribution between age of respondents and level of experience. It was positive to note that the majority of respondents had engaged in some form of postgraduate training in the field of paediatrics across all three clinical disciplines. The findings confirm the confusion highlighted in the literature with respect to difficulties experienced in the assessment of hypotonia. A large percentage of the respondents also agreed on the need for an objective measure in the assessment of hypotonia in the paediatric population.
Future studies should aim towards determining more objective measures for the assessment of hypotonia in the paediatric population. This initial survey could form the basis of clinical criteria to assist in the overall accurate assessment and interpretation of hypotonia.
ACKNOWLEDGEMENT
The authors would like to thank Prof Robin Joubert for her supervision of the project and Mr Sathiesh Govender, data scientist, for his assistance in data analysis.
REFERENCES
1. Sanger TD, Delgado MR, Gaebler-Spira D, Hallet M. & Mink JW. Classification and Definition of Disorders Causing Hypertonia in Childhood. Pediatrics, 2003; 111. [ Links ]
2. Burridge JH, Wood DE, Hermens HJ, Voerman GE, Johnson GR, Van Wijck FM, Platz T, Gregorie M, Hitchcock R & Pandyan AD. Theoretical and methodological considerations in the measurement of spasticity. Disability Rehabilitation, 2005; 27, 69-80. [ Links ]
3. Haugh AB, Pandyan AD & Johnson GR. A systematic review of the Tardieu Scale for the measurement of spasticity. Disability Rehabilitation, 2006; 28, 899-907. [ Links ]
4. Nakhostin-Ansari N, Naghdi S, Moammeri H & Jalaie S. A Comparative Study on the Inter-Rater Reliability of the Ashworth Scales in Assessment of Spasticity. Acta Medica Iranica, 2006; 44, 246-250. [ Links ]
5. Pandyan AD, Van Wijck FM, Stark S, Vuadens P Johnson GR & Barnes MP. The construct validity of a spasticity measurement device for clinical practice: an alternative to the Ashworth scales. Disability Rehabilitation, 2006; 28, 579-585. [ Links ]
6. Bodensteiner JB. The Evaluation of the Hypotonic Infant. Seminars in Paediatric Neurology, 2008; 15, 10-20. [ Links ]
7. Platz T, Vuadens P Eickhof C, Arnold P Van Kaick S & Heise K. REPAS, a summary rating scale for resistance to passive movement:item selection, reliability and validity. Disability Rehabilitation, 2008; 30, 44-53. [ Links ]
8. Jethwa A, Mink J, Macarthur C, Knights S, Fehlings T & Fehlings D. Development of the Hypertonia Assessment Tool (HAT): a discriminative tool for hypertonia in children. Developmental Medicine and Child Neurology [Online], 2010; 52. [ Links ]
9. Martin K, Kaltenmark T, Lewallen A, Smith C & Yoshida A. Clinical Characteristics of Hypotonia: A Survey of Pediatric Physical and Occupational Therapists. Pediatric Physical Therapy, 2007; 19, 217-226. [ Links ]
10. Martin K, Kirschner A, Deming K, Gumbel R & Voelker L. Characteristics of Hypotonia in Children: A Consensus Opinion of Pediatric Occupational and Physical Therapists. Pediatric Physical Therapy, 2005; 17, 275-282. [ Links ]
11. Jan MS. The hypotonic infant: Clinical approach. Journal of Pediatric Neurology, 2007; 5, 181-187. [ Links ]
12. Leyenaar J, Camfield P & Camfield C. A schematic approach to hypotonia in infancy. Paediatric Child Health, 2005; 10, 397-400. [ Links ]
13. Harris SR. Congenital hypotonia: clinical and developmental assessment. Developmental Medicine and Child Neurology, 2008; 50, 889-892. [ Links ]
14. Laugel V Cosse'e M, Matis J, De Saint-Martin A, Echaniz-Laguna A,Mandel J, Astruc D, Fischbach M & Messer J. Diagnostic approach to neonatal hypotonia: retrospective study on 144 neonates. European Journal of Pediatrics, 2008; 167, 517-523. [ Links ]
15. Prasad AN & Prasad C. Genetic evaluation of the floppy infant. Seminars in Fetal & Neonatal Medicine, 2011; 16, 99-108. [ Links ]
16. Pilon JM, Sadler GT & Bartlett DJ. Relationship of Hypotonia and Joint Laxity to Motor Development During Infancy. Pediatric Physical Therapy, 2000; 10-15. [ Links ]
17. Malik SI. & Painter MJ. Hypotonia and Weakness. In: Kliegman RM, Greenbaum, LA & Lye PS, editors. Practical Strategies in Pediatric Diagnosis and Therapy. 2nd ed, Elsevier, 2004. [ Links ]
18. Gowda V, Parr J & Jayawant S. Evaluation of the Floppy Infant. Paediatrics and Child Health, 2007; 18. [ Links ]
19. Hadders-Algra M. The Neuromotor Examination of the Preschool Child and its Prognostic Significance. Mental Retardation and Developmental Disabilities Research Reviews, 2005; 11, 180-188. [ Links ]
20. Shuper A, Weitz R, Varsano I & Mimouni M. Benign congenital hypotonia: A clinical study in 43 children. European Journal of Paediatrics, 1987; 146, 360-364. [ Links ]
21. Curran A. & Jardine P The floppy infant. Current Paediatrics,1998; 8, 37-42. [ Links ]
22. Richter LP, Shevell MI & Miller SP. Diagnostic Profile of Neonatal Hypotonia: An 1 1-Year Study. Pediatric Neurology, 2001; 25, 32-37. [ Links ]
23. Van Toorn R. Clinical Approach to the Floppy Child. CME, 2004; 22, 449-455. [ Links ]
24. Kliegman RM. Fetal and Neonatal Medicine. In: Behrman RE & Kliegman RM, editors, Nelson Essentials of Pediatrics. 4th ed. Philadelphia: Saunders, 2002. [ Links ]
25. Ashwal S & Rust R. Child Neurology in the 20th century. Pediatr Res, 2003; 53, 345-436. [ Links ]
26. Zellweger H. The floppy infant: a practical approach. Helv Paediatr Acta, 1983; 38, 301-306. [ Links ]
27. Crawford TO. Clinical evaluation of the floppy infant. Pediatric Annals, 1992; 21, 348-354. [ Links ]
28. Miller VS, Degado M & Iannaccone ST. Neonatal hypotonia. Seminars in Neurology, 1993; 13, 73-83. [ Links ]
29. Johnston HM. Editorial: The floppy weak infant revisited. Brain and Development, 2003; 25, 155-158. [ Links ]
30. Paro-Panjan D & Neubauer D. Congenital Hypotonia: Is there an Algorithm? Journal of Child Neurology, 2004; 19, 439-442. [ Links ]
31. Birdi K, Prasad AN. & Prasad C. The Floppy Infant: Retrospective Analysis of Clinical Experience (1990-2000) in a Tertiary Care Facility. Journal of Child Neurology, 2005; 20, 803-808. [ Links ]
32. Kathrein JE. Interrater Reliability in the Assessment of Muscle Tone of Infants and Children. Physical and Occupational Therapy in Pediatrics, 1990; 10, 27-41. [ Links ]
33. Carboni P. et al. Congenital Hypotonia with favourable outcome. Paediatric Neurology, 2002; 26, 383-386. [ Links ]
34. Paine RS. The Future of the Floppy Infant: A Follow-up Study of 133 Patients. Developmental Medicine and Child Neurology, 1963; 5, 115-124. [ Links ]
35. Andrews D, Nonnecke B & Preece J. Electronic Survey Methodology: A Case Study in Reaching Hard-to-Involve Internet Users. International Journal of Human-Computer Interaction, 2003; 16, 185-210. [ Links ]
36. Brink HI. Fundamentals of Research Methodology for Health care Professionals, Kenwyn, Juta & Company Ltd, 2000. [ Links ]
37. Walton jn. The Floppy Infant. Cerebral Palsy Bulletin, 1960; 2, 10-18. [ Links ]
38. Maw A. Paediatric Neurology - History and Examination. ACNR, 2009; 9, 34-36. [ Links ]
39. Ayres AJ. Sensory Integration and Learning Disorders. Los Angeles: Western Psychological Services, 1972. [ Links ]
40. Miller Assessment for Preschoolers (MAPÂ). Pearson. <http://www.pearsonassessments.com> [ Links ]
41. Bohannon RW, & Smith MB. Inter-rater reliability of a modified Ashworth scale of muscle spasticity. Physical therapy, 1987; 67, 206-207. [ Links ]
 Correspondence:
Correspondence:
Pragashnie Naidoo
naidoopg@ukzn.ac.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}