










Services on Demand
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
Indicators

Related links
-
 Cited by Google
Cited by Google -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkSouth African Journal of Occupational Therapy
On-line version ISSN 2310-3833
Print version ISSN 0038-2337
S. Afr. j. occup. ther. vol.43 n.2 Pretoria Aug. 2013
SCIENTIFIC LETTER
Promoting person-centred care for people with advanced dementia through environmental adaptations
Sanet du ToitI; Riandi van der MerweII
IB OT, M OT, BSc OT (St Loye's UK). PhD Senior Lecturer, Department of Occupational Therapy, University of the Free State
IIB. OT Therapy (University of the Free State) Community therapist (2012). Undergraduate student at the University of the Free State at the time the research was conducted
Dear Editor:
INTRODUCTION
Dementia, a condition usually associated with age, is commonly characterised by memory loss, changes in personality, deterioration in personal care and fluctuating levels of disorientation1. In addition to these losses, many persons with dementia are eventually institutionalised due to their fulltime care needs, and social losses are often experienced in this unfamiliar environment. Institution-alisation could also negatively impact on the care experienced by a new resident as individuality is often lost within a clinical environment and set routines could potentially be monotonous and dominate daily life2. Additionally the residents' well-being is affected by dementia as their ability to spontaneously engage in meaningful tasks is diminished1.
For people with advanced dementia, memorabilia (especially objects and artefacts they valued or used often in the course of their lives) may facilitate moments during which social connectivity could be established. In such a given moment the staff member (e.g. the occupational therapist) may be privileged to share in a memory or be involved in a task that was previously meaningful. This type of shared experience, however short in duration, is precious and may become a thread woven into the creation of future opportunities for meaningful engagement3. The Bradford Dementia Group published a variety of Good Practice Guides aimed at promoting quality of life and quality of care through jargon-free, evidence-based guides and stresses the importance of understanding experiences and events signifying a resident's life2. Understanding who the resident is, what gave him/her joy and why he/she acts in a certain way is all locked up in memories and the resident's past; especially when he/she cannot successfully communicate any more2. It is therefore evident that reminiscing could provide pleasure and a sense of relatedness and connection with what has happened before3.
If an activity is meaningful for a resident and the resident participates and engages in this activity, it could/will result in the resident experiencing a blend of pleasure, productivity and restoration in his/her life4. The contextual and subjective dimensions of the environment, the required task expected to be engaged in, and the well-being of the resident are all linked to address the quality of life experienced by the resident4. Consequently, this clinical project was conducted to investigate possible adaptations to a specific environment (in this case a separate, accessible room next to the common area) with the purpose of facilitating participation in purposeful activities through reminiscence.
METHODS
The clinical project, aimed at advancing person-centred care of residents through the development of person-specific programmes for everyone living in the dementia care unit, was part of a preliminary quantitative investigation. This pilot study was designed to explore the use of the tools and to consider the potential value of the descriptive data generated5.
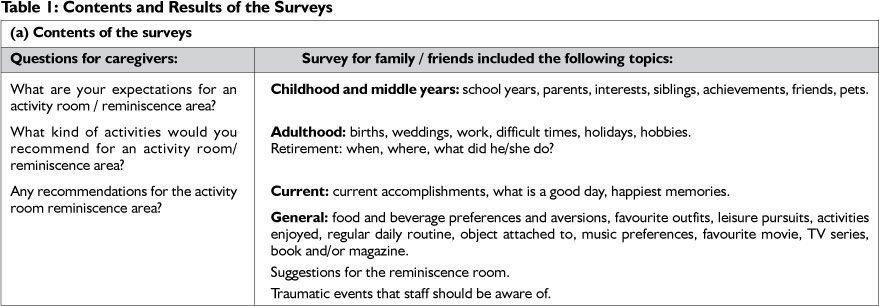
The research tools consisted of two different semi-structured questionnaires that were compiled; one for the family members of the residents and the other for the caregivers. The questionnaires were based on the person-centred approach and life story work by May, Edwards, and Brooker2 (see Table 1). The questionnaire for the family members was divided into four sections namely childhood, middle years, adulthood and current life and comprised three and a half pages. Different themes were listed and the focus of the family questionnaire was to attain information about the person's history and valuable memories.
The single page caregiver's questionnaire consisted of three questions namely what are your expectations for this room; what do you think is the goal of this room; and what activities do you think should be included in this room. The caregivers' questionnaire thus mainly focused on their expectations of how residents would respond to the suggested activities as a result of this clinical project. As effective multidisciplinary work could contribute to staff members' willingness to implement the project in the long-term, it was important to involve the caregivers from the onset in this proposed project.
This pilot study was executed by a final year occupational therapy student during her fieldwork placement at a residential care facility in the Free State. One week was available for project implementation and staff members directly available to the student during the day shift participated. Twenty family members and friends of the 17 residents in the unit were contacted, but the convenience sample eventually comprised six relatives of six residents who completed the family questionnaire5. Therefore the participants included six of the caregivers of the dementia unit and six family members of residents. The questionnaires were available in both Afrikaans and English as all of the participants understood both languages. The nominal data generated were tabled according to the predetermined themes that were directed by the lay-out of the questionnaires6.
The pilot phase of this proposed project considered the feasibility of a larger study and specifically assisted in identifying factors that could impact on the validity and reliability6 of the surveys utilised.
FINDINGS
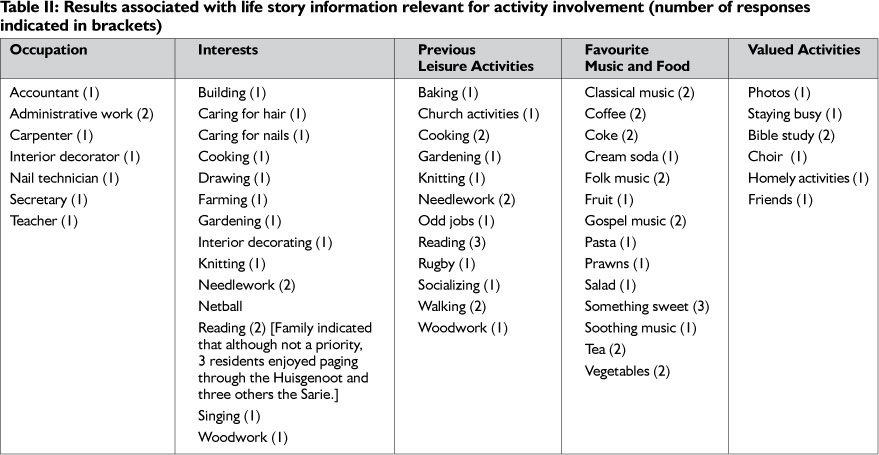
The completed family questionnaire represented the preferences of 35% of the residents (i.e. five females and a male) and assisted with identifying potential occupations, interests and leisure activities of these residents. Table II summarises the information obtained through the questionnaires.
The average age of the 1 7 residents residing in the unit at the time of implementation of the clinical project, was 76 years, which meant that they were born in the 1930s. The researcher, as a result, familiarised herself with the habits, routines and activities in which adults engaged in during the period 1920 to 1950, by consulting published literature. Findings from the family questionnaires indicated that these residents had diverse career backgrounds, (e.g. being an accountant, teacher or nail technician), were listed. Their leisure activities could be categorised into the different categories of self-care, crafts and activities with a spiritual connotation. Other activities the residents had in common and valued were needlework, cooking, reading, listening to music and gardening (Table II). The residents involved in the survey had all completed secondary schooling. No specific information was included about tertiary education and the questionnaires rather referred to positions held during their careers (e.g. the teacher being a head of department).
The factors considered were that:
Only one person was involved in compiling the questionnaires which could impact negatively on the validity of the data.
Internal validity of the pilot data was decreased by the fact that the participants (especially in the case of family members) varied and included either a spouse or one of the resident's children.
Internal validity was enhanced because the investigation was limited to the specific unit.
A single investigator could have advanced the reliability of the study as she was the only one who explained the questions to the participants.
The reliability of the study could have been affected by the fact that the residents themselves could not answer the questions and also because the caregivers did not complete the questionnaires in their mother tongue.
The results of the investigation are not generalisable as the same questions posed to different participants would not have the same outcome (staff members and different family members' knowledge of a specific resident's preferences differ).
Questionnaires completed by the caregivers enhanced insight into their expectations of this project. These questionnaires indicated that the caregivers did not understand the potential contribution that reminiscence could have on the quality of life of residents and they saw the outcome of the project as being just an activity which they could use to keep residents busy.
DISCUSSION
Activities identified by the surveys that would most likely promote engagement and diminish isolation, monotony and helplessness of some of the elderly residents in residential care and in which reminiscence would be an important component, included: needlework, gardening, cooking, administrative tasks and activities that involved children.
The results had the potential to be utilised in two different ways. Firstly, ways in which the institutional environment could be adapted to enhance a more home-like atmosphere and secondly, tasks that could facilitate the activity participation of the residents, were recommended. The main challenge was to provide ideas that would be appropriate for the majority of the residents, and as a person-centred approach was promoted in the unit, the occupational therapy staff had to attempt to address the needs of every resident.
The following themes appeared to have the potential of stimulating reminiscence for the majority of the residents:
an administrative area (e.g. 1920 to 1950 newspapers, books and magazines on bookshelves; a desk and study chair; old telephone and typewriter);
a self-care area (e.g. 1920 to1950 clothes, hats, scarves and jewellery, a mirror, make up, nail care, iron and ironing board, or laundry basket);
a school area (e.g. large printed idioms, desk, old school clothes, school satchel, black board and school bell); as well as
a variety of domestic activities that could be alternated (e.g. shelling peas, simple knitting that was already started like scarves);
opportunities for co-occupations (e.g. along with other residents, family or volunteers to engage in singing hymns, reading from the Bible and praying); and
planned times for enjoying music (as different music preferences were listed and by allocating specific time slots, more individual tastes would be accommodated).
When utilising the above ideas to plan reminiscence areas it would be important to ensure that these areas are easily accessible and that residents could explore tasks that were personally significant to them. Consideration should be given as to which artefacts/objects would be more decorative and which ones would actually entice residents to engage in activity, as residents' involvement should be spontaneous and they should not be coerced to participate in any activities. Resident-specific adaptations should also receive consideration, for example, one female resident might prefer to put on jewellery and make up in the self-care area, while another resident (who used to be a nail technician) might enjoy doing the nails of a staff member or fellow resident. The activity should be person-specific in order for it to be meaningful for the individual.
Potential future activities were selected in order to stimulate reminiscence as various authors emphasise the importance of creating a person-centred environment1'2,3,4. A fact that should be kept in mind is that the residents did not fill the questionnaire in for themselves. Therefore, if the family member who filled in the questionnaire did not know the resident's personal preferences very well, he/she might have concentrated on his/her own memories of the person rather than life events important to the resident.
The aim of the second questionnaire was to ensure the caregiv-ers' involvement and to promote sustainability of the project. The caregivers spend a great amount of time with the residents, and were thus potentially more aware of residents' likes and dislikes. Merely asking opinions about the proposed project, therefore, was only an initial step for involving caregivers, as it is just as important to inform and educate all staff members about the value of reminiscence for persons with dementia before activity areas can be established.
CONCLUSION AND RECOMMENDATIONS
The pilot study reflected the preferences of a limited number of residents and these suggested areas should be implemented and assessed for the impact on the residents, before involving the remainder of the residents in the project. The life stories of each resident should be considered in order to make small adaptations to the institutional environment so that the quality of life of every resident could be promoted. By creating an environment where reminiscence in meaningful activities would be facilitated, spontaneous participation could be encouraged. Therefore, the residents' history (i.e. life stories) is important to ensure that the adaptations of the environment are person-centred and create a feeling of belonging that could enable engagement. Small resident-specific adaptations could also be made in the area, for example the availability of clothes that a specific resident wore when he/ she was younger. Reminiscence boxes could be made for each resident; these boxes should contain items that have meaning for a specific resident.
Follow-up clinical projects should explore how resident-specific adaptations would encourage participation in specific activities or whether the suggested artefacts and objects included in the reminiscence areas are mostly decorative. Caregivers should also be trained in utilising components of reminiscence for promoting participation in self-care (productive activities) and leisure (pleasurable activities). It is essential that caregivers experience how various small adaptations in the environment can promote engagement of residents and thereby improve their quality of life.
REFERENCES
1. Author unknown. "Meaningful Activities in Dementia Care" Demystifying Dementia Care. May 2004. <http://www.accreditation.org.au/site/learning_packages/Dementia-meaningful.pdf> (19 June 2012) [ Links ]
2. May, H., Edwards, P, and Brooker, D. A Good Practice Guide to Delivering Person-Centred Care. London: Jessica Kingsley Publishers. 2009. [ Links ]
3. Gibson, F 2011. Reminiscence and Life Story Work - A practical Guide. London: Jessica Kingsley Publishers. [ Links ]
4. Pierce, D. Occupation by Design: Building Therapeutic Power. FA. Davis, Co.: Philadelphia. 2003 [ Links ]
5. Foster, R.L. 2013. What a pilot study is and what it is not. Journal for Specialists in Paediatric Nursing 18 (2013) 1-2 ©2013, Wiley Periodicals, Inc. http://onlinelibrary.wiley.com/doi/i0.!11/jspn.12015/pdf (5 March 2013) [ Links ]
6. Babbie, E. & Mouton, J. 2010. The practice of social research. Cape Town: Oxford University Press Southern Africa [ Links ]
 Correspondence:
Correspondence:
Sanet du Toit
dutoit@ufs.ac.za


{kind=link}
{kind=link}