










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkSouth African Journal of Occupational Therapy
versão On-line ISSN 2310-3833
versão impressa ISSN 0038-2337
S. Afr. j. occup. ther. vol.43 no.1 Pretoria Abr. 2013
SCIENTIFIC ARTICLES
Substance abusers' anger behaviour and sensory processing patterns: An occupational therapy investigation
Denisé StolsI; Rita van HeerdenII; Annamarie van JaarsveldIII; Riette NelIV
IB Occupational Therapy (UP), M Occupational Therapy (UFS) Denmar Specialist Psychiatric Hospital, Pretoria
IIPhD (UFS) Department of Occupational Therapy, Faculty of Health Sciences, University of the Free State, Bloemfontein
IIIM Occupational Therapy (UFS) Department of Occupational Therapy, Faculty of Health Sciences, University of the Free State, Bloemfontein
IVMMedSc (UFS) Department of Biostatistics, Faculty of Health Sciences, University of the Free State, Bloemfontein
ABSTRACT
BACKGROUND: Persons with a high tendency towards anger often abuse substances. When problematic anger interferes with substance abusers' ability to cope, the occupational therapist plays a vital role in providing opportunities for substance abusers to experience and practice effective ways to deal with their anger. Many substance abusers seem to also have atypical sensory processing patterns. In Occupational Therapy atypical sensory processing is recognised as a domain of concern not only in children, but adults as well. It is against this background that the question was asked whether relations exist between substance abusers' anger behaviour and their sensory processing.
METHODS: A quantitative, cross-sectional study was conducted to describe adult substance abusers' anger behaviour and sensory processing patterns. Adults with substance abuse difficulties admitted to two institutions in Pretoria between 1 October 2008 and 29 May 2009 represented the study population. The one institution specialises in substance abuse rehabilitation, while the other is an inpatient treatment facility for clients with mental health problems. A total of 84 participants met the inclusion criteria, of which 54 participants were in-patients at one institution and 30 in-patients at the other institution. Participants reported on the following anger behaviours: verbal expression, physical expression, escape, substance use, suppression, non-verbal expression, and calming strategies. Participants' sensory processing patterns were determined by completing the Adolescent/Adult Sensory Profile.
RESULTS: Anger behaviour in the majority of participants with low registration patterns more than the typical norm, was related to a style of directly expressing anger (65.5% regularly expressed anger physically and 61.5% regularly expressed anger verbally). Anger behaviour in the majority of participants with sensory-avoidance patterns more than the typical norm, was related to a style of avoiding anger (62.5% seldom expressed anger verbally, 60.8% regularly escaped from anger situations and 58.9% regularly suppressed their anger).
CONCLUSIONS: Occupational therapists should consider evaluating and if necessary address the sensory processing of their adult clients with problematic anger and/or substance abuse difficulties. Further research on the above associations is indicated in clinical and non-clinical populations. For future studies the use of a qualitative research approach and purposive or representative sampling are recommended. This will provide deeper understanding of relations found and support generalisation of results.
Key words: occupational therapy, anger behaviour; anger management style; substance abuse; sensory processing; sensory processing patterns
INTRODUCTION
Anger management problems can affect every aspect of a person's life - especially when it leads to the chronic experiencing of anger, hostility and subsequently violence1. Many persons with a high tendency to become angry also seem to often abuse substances2,3,4,5. In a study conducted by Tafrate et al6 participants with a high tendency to anger used three times more substances than persons with a low tendency to anger. It seems that rehabilitated substance dependants revert back easier to their substance abuse habits when they experience anger management problems7. Clients abusing substances often need occupational therapy for associated medical, physical or psychosocial problems8 and in these cases the occupational therapist aims at improving the clients' ability to manage a balanced lifestyle and to effectively cope with stress9. Thus, when anger interferes with the substance abusers ability to cope, the occupational therapist plays a vital role in providing opportunities to experience and practice effective ways of dealing with their anger9.
Stoffel and Meyers11 as well as Crouch9 emphasise the importance of occupational therapists following a holistic approach when treating clients who abuse substances. The research study of Quadling et al12 found that 80% of a sample of 64 adult substance abusers showed significant sensory seeking or sensory avoiding behaviour in one or more sensory systems. In occupational therapy, sensory processing difficulties are recognised as a domain of concern not only in children, but adults as well13. Brown and Dunn14 recognised the need for an adult measure of sensory processing that included all sensory modalities and which was based on a theoretical model. This led to the development of the Adolescent/ Adult Sensory Profile15. Anectodal evidence suggests that sensory processing disorders may play a large role in children and adolescents that present with emotional regulation difficulties16. Dunn's Model14 depicts sensory processing patterns as stable traits of a person across the life span indicating that there is a possibility that sensory processing difficulties can also affect the emotional regulation of adults, for example when they experience anger.
Adults with insight into the manner in which their brain processes sensory information are aware of and understand their own sensory preferences, dislikes and behaviour towards sensory stimuli and adapt their behaviour using healthy ways to satisfy their sensory needs17,18. Persons without this insight become more easily involved in high-risk behaviour such as in reckless driving, some types of sexual relationships or substance abuse19. When adults manage sensory stimuli in a way that it impedes the regulation of their nervous system's state of arousal, increased levels of anxiety, frustration or anger can occurr18. During intervention the occupational therapist and client need to become aware of which sensory stimuli cause stress and must be managed differently, as well as which sensory stimuli contribute to a calm alert state14,17. This insight can also be shared with significant people in the client's life to provide them with better understanding of the client's behaviour and therefore offer better support13,14,17.
The discussion so far led to the researchers to question whether possible connections existed between substance abusers' anger behaviour and their sensory processing patterns. Although it is possible to explain these connections in theory, research shedding some light on this topic is almost non-existent. Therefore the goals for the study were to, first investigate substance abusers' behaviour that manifested when they experienced anger (anger behaviour), then to determine substance abusers' sensory processing patterns (as explained in Dunn's15 Model) and lastly to describe the possible connections between substance abusers' anger behaviour and sensory processing patterns.
Literature review
The three main concepts of this study are briefly discussed.
Substance abuse
There is still a need for studies that could lead to the effective treatment of substance abuse20,21 with the gap in knowledge existing within both the pharmaceutical and psychosocial fields22. Some authors9,22,23,24,25,26 describe occupational therapy treatment for substance abuse, but research within this field is limited.
The results of one Occupational Therapy study supported the use of arts and crafts in substance rehabilitation27. Martin et al21 investigated the changes in occupational performance, self-image and quality of life of substance abusers receiving occupational therapy, as part of their programme at a halfway house. Stoffel and Moyers11 compiled an occupational therapy perspective of interventions for persons with substance abuse disorders based on an interdisciplinary literature review. Researchers emphasise the need for time and money to support comprehensive research projects on the role that occupational therapists play in the treatment of substance abuse11,27,28.
Anger
A need still exists to differentiate between functional and dysfunctional anger behaviour29. Anger is negatively correlated to assertiveness and self-image, and is positively correlated to depression, feelings of guilt, conflict avoidance and dependency30. Assertion, direct anger expression, searching for social support, anger avoidance and diffusion of anger have been identified as different styles of anger management3 '. In their descriptive study, Tafrate et al6 described the different components of anger behaviour as being the verbal expression of anger, the physical expression of anger, resolution (assertiveness), the escape from an anger situation, the suppression of anger, the non-verbal expression of anger and substance use.
Although occupational therapists treat adult clients with poor anger management8 literature discussing this is scarce 32. Taylor8 as well as Grogan10 published articles on occupational therapy and anger management based on psychology research, especially cognitive-behavioural therapy. Tang32 studied the efficacy of an occupational therapy anger management group which used a cognitive-behavioural approach. She viewed dysfunctional anger behaviour as reactions that include verbal aggression, physical aggression and the abuse of substances. The review of the occupational therapy literature has thus revealed a need for further investigation.
Sensory Processing
Miller and Lane33 define sensory processing as the registration, modulation, integration and organisation of sensory stimuli, as well as the behavioural responses to sensory stimuli. It appears that adequate sensory processing and management of sensory stimuli also influence the functioning of adults13,14,1734. Up to now only a few research studies have focused on adults with sensory processing disorders12,35,36,37,38.
Dunn's Model of Sensory Processing
As already mentioned, Brown and Dunn14 recognised the need for an adult measure of sensory processing and developed the Adolescent / Adult Sensory Profile14. Further studies provided sufficient information for this model to be applied to people of all ages39,40. Dunn's Model15 defines sensory processing as the interaction between a person's neurological threshold and behaviour responses. The Model presents the neurological threshold on a continuum from high to low, and behaviour responses on a continuum from active to passive. Different threshold values on the neurological threshold continuum are represented when a person becomes aware of a specific sensory stimulus, reacts to it or experiences irritation. Persons with neurological threshold values higher than the typical norm tend to react more slowly to sensory stimuli than other people. On the other hand, when the neurological threshold values are lower than the typical norm, there is a tendency to react more quickly to sensory stimuli18 as well as being constantly aware of sensations and having difficulty concentrating on other tasks.
The one side of the behaviour continuum represents the use of passive behaviour strategies (such as remaining in a noisy environment in spite of the fact that it is disturbing), while the other side represents active behaviour strategies (for example, moving away from a noisy environment when it is experienced as disturbing). Where a person's behaviour patterns are more active than the typical norm, the person can be driven to the extent of performing certain behaviour rituals, which could negatively influence the completion of daily routines on the other hand, if a person's behaviour responses are more passive than the typical norm, the person can be so uninvolved in the environment that it hinders the execution of daily routines18. Dunn's Model for Sensory Processing15 represents the relationship between the two above-mentioned continuums (see Figure 1).

According to Dunn18 there are four types of sensory processing patterns. Those with low registration patterns show behaviour that is more passive in nature and they are less troubled to collect additional information from the environment whereas persons with sensory seeking patterns show active behaviour strategies and tend to find ways of enhancing their sensory experiences. Those persons demonstrating sensory sensitive patterns notice sensory stimuli quicker and tend to react to all of them whereas those with sensory avoiding patterns tend to find ways of avoiding sensory stimuli.
All four sensory processing patterns occur in every person and can be compared to the typical norm using the Sensory Profile14. A person can display typical or atypical sensory processing in respect of each of the patterns. People do not process sensory information in a uniform way, but in a complex and unique way within all four of the sensory processing patterns18.
METHODOLOGY
Study design
A quantitative study design was used to investigate the relations between participants' anger behaviour and sensory processing patterns. Quantitative research is applied among others to answer research questions on relations between measurable variables41. Furthermore a cross-sectional design was considered appropriate, as above-mentioned relationships were investigated at a certain point in time by means of statistical comparisons42.
Population and Sampling
Convenience sampling was used, which offered the opportunity to involve as many voluntary participants as possible. The study population consisted of adults with substance abuse difficulties who were admitted to two institutions in Pretoria between 1 October 2008 and 29 May 2009. The one institution specialises in substance abuse rehabilitation, while the other is an inpatient treatment facility for clients with mental health problems. A total of 84 participants met the inclusion criteria, of which 54 participants were in-patients at one institution and 30 in-patients at the other institution. The inclusion criteria were as follows:
If clients were able to respond appropriately and complete the questionnaires independently, they could participate from their second week of hospital residence. It was expected that participants' physical withdrawal symptoms would be under control by then.
Adult men and women (18 years up to 64 years and 1 1 months) admitted for their first psychiatric rehabilitation treatment programme. The reason for this criterion was to exclude the possible effect of previous admissions' life skill training.
Participants had to be literate and able to complete the questionnaires independently as well as being conversant in English or Afrikaans as the questionnaires were available in these two languages.
Persons who had brain damage due to an acquired brain injury, congenital causes or birth trauma, were not included.
Measurement tools
For the purpose of this study a questionnaire was compiled to collect the following demographic information from participants': age, education level, occupations, gender, marital status, home language, previous rehabilitation programmes attended, family members' with substance abuse difficulties, future expectations about support, type of substances abused and whether problems related to a head injury were still being experienced.
The Adolescent/Adult Sensory Profile14 was used in the study as it can be administered to people up to the age of 64 years and 11 months. This is a 60-item questionnaire with a self-evaluation scale. The items are scored to classify the individual's propensity for behaviours in each sensory processing pattern as: much less than others, less than others, the same as others, more than others, much more than others. The classifications less and much less than others indicate sensory processing patterns less than the typical norm. It is possible that persons could experience problems in their daily functioning due to this manner of sensory processing. The classification same as others indicates sensory processing patterns that are the same as the typical norm. It is not expected that this manner of sensory processing would cause functional problems for a person. The classifications more and much more than others indicate sensory processing patterns that are more than the typical norm. It is possible that persons could experience problems in their daily functioning due to this manner of sensory processing.
The psychometric characteristics of the Adolescent/Adult Sensory Profile14 were investigated by Brown, Tollefson et al40 in respect of item reliability, face validity, construct validity and standardisation. The majority (92%) of the study population used for the standardising of the Adolescent/Adult Sensory Profile14 were Whites with a Western (Eurocentric) background. The majority (84%) of participants in our study were of similar ethnicity. The Adolescent/ Adult Sensory Profile14 has, however, not yet been standardised for a South African population. At the time of the study, no similar South African measuring instrument was available.
A second questionnaire was constructed based on published studies which describe participants' anger behaviour rather than administering standardised tests for this purpose6,43,44.This questionnaire collected data on how often participants experienced specific anger behaviour by using a simple scale with the following options: almost never (approximately 5% or less of the time), seldom (approximately 25% of the time), sometimes (approximately 50% of the time), often (approximately 75% of the time), and almost always (95% or more of the time). Participants, who indicated that they "sometimes", "often" or "almost always" experienced the particular anger behaviour, were requested to specify their behaviour. Participants were asked to report on verbal expression of anger, physical expression of anger, escape from an anger situation, substance abuse when angry, suppression of anger, non-verbal expression of anger, and applying calming strategies. One open question was asked at the end of the questionnaire where participants could specify any other anger behaviour that was not identified in the questionnaire. This questionnaire had been evaluated by occupational therapists and other experts working at the University of the Free State as part of project planning.
Methods and procedures
Each study participant attended a data collection session with other participants (between two and ten participants). Although participants were in the same room, they were asked to complete questionnaires independently from each other. The first author was present during the whole session and administered the questionnaires to the participants explaining the instructions and encouraging participants to indicate if they needed further explanation.
Control over external factors41 was exercised by collecting data over the same period of time, at the same time of the day ie afternoons, using the same venue. Data collection sessions did not take place during participants' treatment or visiting times. As the participants were in-patients they had already had breakfast and lunch, which limited the effect of hunger. The data collection sessions lasted approximately 40 minutes thus limiting the effect of fatigue. All participants were informed that the success of the study depended on the completeness and correctness of the information that they provided in the questionnaires. Participants were assured that the researcher would handle all information as confidential. At the end of the data collection session the first author checked the questionnaires with each participant to ensure that they were complete.
Ethics
The Ethics Committee of the Faculty of Health Sciences, University of the Free State, approved the study (ETOVS number 133/08). Right of admission to the premises and permission to inform patients of the study were received from both institutions in Pretoria. The expectations and potential risks of the study were explained to participants in a group, orally and in writing, in simple language and without the use of medical or professional terminology. Patients were informed that participation, refusal to participate, or withdrawal from participation in the study was voluntary and their choice would not imply any negative effect on their health care. Participants signed an informed consent form. Participants were informed that the data collected in this study would identify participants with possible anger problems and that it was ethical to make these participants aware of it. In these cases participants were asked for written permission to make results known to their psychologist and/or psychiatrist. Counselling was made available to participants, should they need it due to participation in the study.
Data Analysis
Descriptive statistics were used, namely medians and percen-tiles for continuous data, and frequencies and percentages for categorical data. Ninety five per cent confidence intervals were calculated to describe the prevalence of sensory processing patterns.
RESULTS
The median age of the 84 participants was 36 years and 6 months (range: 19.0 - 61.0); 64.3% were Afrikaans-speaking; 67.9% were male; 54.8% were unmarried; 83.3% had completed at least grade l2 and 90.5% were employed and 65.5% abused alcohol (see Figure 2). Seventy six (90.5%) of the participants abused depressants (calming or sedating effect caused by the use of substances like alcohol (65.5%), sleeping or pain medication (25.0%)) 27.4% abused stimulants (activating and euphoric effect caused by the use of substances like cocaine (l6.7%) and methacarhinone (l0.7%)) and 7.l% abused depressants as well as stimulants. Thirteen (l5.5%) of the participants reported having sustained a head injury. All of them reported having no long-term or permanent neurological deficits as a result of the injury and were included in the study.

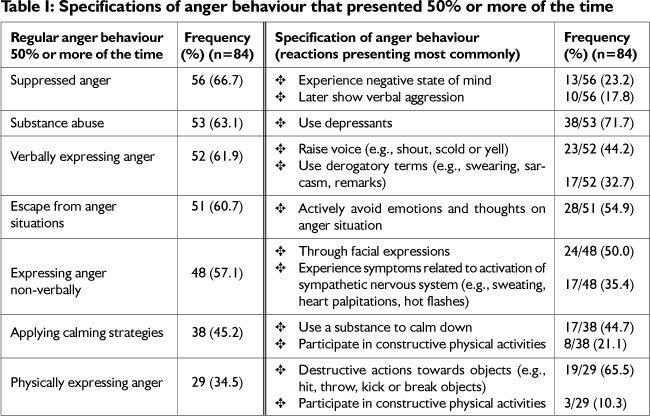
Anger behaviour that occurred regularly ie 50% or more of the time, was reported by participants as suppressing anger (66.7%), using substances (63.l%), expressing anger verbally (6l.9%), escaping from anger situations (60.7%) expressing anger non-verbally (57.l%), applying calming strategies (45.2%) and expressing anger physically (34.5%). Participants were asked to specify their anger behaviour in more detail and the most common reactions reported are illustrated in Table I.
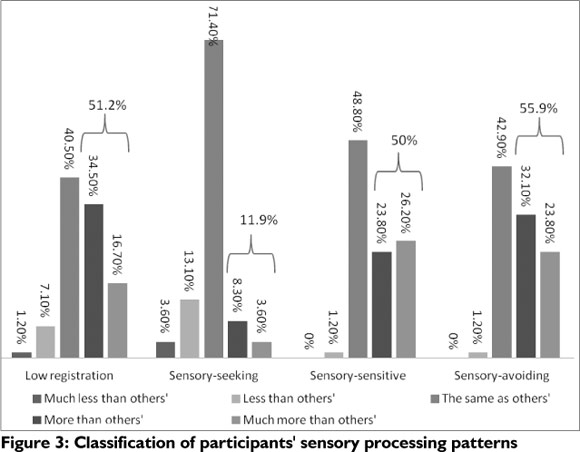
All the participants in the study could understand and complete the Adolescent/Adult Sensory Profilel4. According to the Adolescent/Adult Sensory Profile14 (see Figure 3 on page 29), 51.2% of participants' low registration patterns were classified as more or much more than that of other people, while 11.9% of participants' sensory-seeking patterns were classified as more or much more than others. The sensory-sensitive patterns of 50% of participants were classified as more or much more than that of other people, while 55.9% of participants' sensory-avoiding patterns were classified as more or much more than that of others.
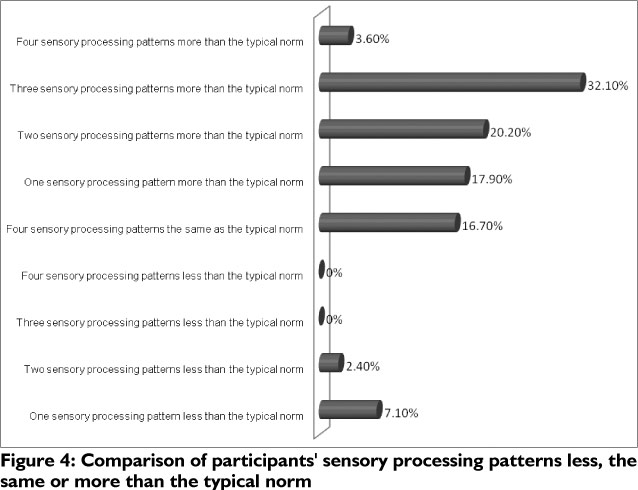
Approximately one third (32.1%) of the participants showed more than the typical norm in three sensory processing patterns (see Figure 4 on page 29). These three patterns were specified as follows: (i) 27.4% (n=23) of participants' low registration, sensory- sensitive and sensory-avoiding patterns were more than the typical norm; (ii) 3.6%(n = 3) of the participants' low registration, sensory-seeking and sensory-avoiding patterns were more than the typical norm; and (iii) l.2%(n=l) of the participants' sensory-seeking, sensory-sensitive and sensory-avoiding patterns were more than the typical norm.
Participants' seven anger behaviours experienced as seldom (25% or less of the time) or regularly (50% or more of the time) were described in terms of the four sensory processing patterns. Each anger behaviour's association with the four sensory processing patterns described as less, the same, or more than the typical norm were determined in terms of the prevalence thereof. The occurrence of the sensory processing pattern having the highest prevalence (see Table II on page 30) was the same for:
Verbal and physical anger behaviour:
⥠seldom express anger verbally and seldom express anger physically; sensory-seeking less than the typical norm, sensory-seeking the same as the typical norm and sensory-avoiding more than the typical norm
⥠regularly express anger verbally and regularly express anger physically; sensory seeking the same as the typical norm and low registration more than the typical norm
Suppressing anger and nonverbal anger behaviour:
⥠seldom suppress anger and seldom express anger non-verbally; sensory-seeking less than the typical norm, sensory-seeking the same as the typical norm
⥠regularly suppress anger and regularly express anger non-verbally; sensory seeking the same as the typical norm and sensory-avoiding more than typical norm
Escaping from anger situations and applying calming strategies when angry:
⥠seldom escape from anger situations and seldom apply calming strategies when angry; sensory-seeking less than the typical norm and sensory-seeking the same as the typical norm
⥠regularly escape from anger situations and regularly apply calming strategies when angry; sensory-seeking the same as the typical norm, sensory-avoiding more than the typical norm
Descriptions of participants' anger behaviour and sensory processing patterns were investigated further in terms of low registration more than the typical norm and sensory-avoiding more than the typical norm. In Table III on page 31 the two patterns were specified further in terms of anger behaviour.
DISCUSSION
Convenience sampling possibly led to bias in the study's results, which limited the internal validity of the study. The results were therefore interpreted circumspectly. The study's external validity also showed limitations due to the convenience sampling and because the study was not repeated in other study populations. The results can thus not be generalised outside the chosen study population.
The majority of participants in this study were Afrikaans speaking males with a grade 12 education, employed and rehabilitating from their alcohol abuse habits. A similar profile as mentioned above was reported in the 2006 record of South African Community Epidemiology Network on Drug Use (SACENDU)45 on the majority profile of patients admitted to substance rehabilitation clinics in South Africa. In the 2008 annual report of the South African Alcohol and Drug Abuse Research Unit factors such as affordability, awareness and location of clinics were discussed as factors that influence intake for substance rehabilitation in South Africa46. It was possible to see some similarity between these factors and our study's results. The majority of participants in this study were employed and most likely able to afford admission or had medical aid cover. Most of the participants were educated and probably more aware of the treatment options for substance abuse. The two institutions where the study took place were located in well established neighbourhoods in Pretoria, increasing the likelihood that most participants were aware of the facilities.
Despite a history of head injury in 15.5% of participants, none of them reported that they experienced any long-term neurological deficits. The inclusion of these participants in this study could be seen as a limitation, as the possibility existed that they were not aware of subtle neurological deficits as a result of the head injury. These participants were however able to give appropriate responses and complete the questionnaires independently.
Anger behaviour
Suppression of anger was selected by most of the participants (66.7%) as regular anger behaviour, with negative mood change and verbal aggression as the most prevalent reactions to anger suppression. Tafrate and colleagues6 found similar results in participants with a high tendency towards anger. They had a much larger need to suppress their anger, experienced significantly more negative thoughts about themselves, and experienced significantly more negative emotions such as depression, embarrassment and repugnance, than participants with a low tendency to anger. Mayne and Ambrosel also asserted that persons who chose to suppress their anger were more prone to withdraw socially. A large percentage (63.1%) of the participants in this study indicated substance use as anger behaviour. Again this result was also found by Tafrate and colleagues6. Persons with a high tendency towards anger were two to three times more likely to use substances during an anger episode.
Many participants (61.9%) indicated that they often expressed their anger verbally, of whom 76.9% (44.2% raised their voice and 32.7% used derogatory terms) specified verbal aggressive behaviour (see Table I on page 28). This anger behaviour reaction was also found by Tafrate and colleagues6. Their study results showed that persons with a high tendency towards anger were twice as likely to experience negative verbal anger reactions than persons with a low tendency towards anger. Many (60.7%) participants indicated withdrawal from anger situations as regular anger behaviour, of whom more than half (54.9%) described that they walked away and then consciously avoided thoughts and emotions regarding the anger situation. To withdraw from the situation and try to forget about it has been described by Linden and colleagues31 as avoidance and a less effective anger management style. Of the 57.1 % of participants who indicated that they often expressed anger non-verbally, 35.4% experienced symptoms related to the activation of the sympathetic nervous system (e.g. heart palpitations, hot flashes or sweating) and regarded it as non-verbal anger behaviour. Tafrate et al.6 found that non-verbal anger behaviour occurred regularly in persons with a high and low tendency towards anger. They6 indicated that participants with a high tendency towards anger experienced significantly more headaches and light-headedness than participants with a low tendency towards anger.
In comparison to all the anger behaviour reported, notably less (45.2%) participants indicated the use of calming strategies as regular anger behaviour. However, 44.7% of these participants specified substance use as their way of calming down. In the development of the Anger Management Scale, Stith and Hamby2 found that substance abuse correlated more strongly with behaviour and thoughts which increased the intensity of anger experiences. It was therefore possible that these participants had not yet realised the negative effect of substance abuse on their anger behaviour. What became clear in this study was participants' inability to apply healthy calming strategies during anger situations. Of the 34.5% of participants who indicated physical expression of their anger as regular anger behaviour, 55.2% acted physically aggressive towards objects, 6.9% towards other people and 3.4% towards themselves (total of 65.5% reporting physical aggression). Based on these findings, it would be valuable to further investigate the relation between anger and physical aggression in clinical populations. Generally research has shown a low correlation between aggression and anger in non-clinical populations29.
Participants who withdraw from anger situations or suppress their anger would benefit from treatment that focused on the promotion of social and cognitive skills47. To address verbal and physical aggression, or management of physical symptoms related to anger episodes, cognitive behavioural therapy, the learning of relaxation techniques and applicable leisure time activities were recommended47,48,49. For the participants who used substances to manage their anger, the above mentioned intervention would also offer support in the prevention of substance abuse relapse7.
Sensory processing patterns
It has been proposed that substance abusers could present with sensory-seeking patterns of behaviour more than the typical norm12,17. It was noticed though in this study that 71.4% of participants' sensory-seeking patterns were in accordance with the typical norm (see Figure 3 on page 29). This finding was similar to what has been reported previously on persons with schizophrenia and bipolar disorder, in which the majority of participants' sensory-seeking patterns were also the same as the typical norm50.
Figure 3 furthermore shows that 5 1.2% of the participants' low registration patterns were more than the typical norm. These participants probably missed clues from the environment and indicated a stronger need for activities that supplied them with additional sensory stimuli18. Half (50%) of the participants' sensory-sensitive patterns were more than the typical norm. They were probably very aware of their surroundings and indicated a need to decrease the intensity and amount of sensory stimuli in their environment18. Finally, 55.9% of the participants' sensory-avoiding patterns were more than the typical norm, and probably these participants had found ways to limit their sensory stimuli and indicate a need for quiet environments and clear expectations18.
Participants with insight into their own unique sensory processing, meet their sensory processing needs by adapting their daily activities in a healthy way33. Their choice of daily activities supports the regulating process of their nervous sytem18. For persons whose sensory processing patterns are more or less than the typical norms, this process - to make sense of their sensory processing needs and adapting their daily activities accordingly - could be even more complicated. However, it is not assumed that all persons with sensory processing patterns more or less than the typical norm will definitely experience subsequent problems14. What is of clinical importance, is to be aware of, assess and treat sensory processing difficulties in adult patients. Possibly, some of the participants would benefit from treatment regarding their sensory processing patterns, which could include14,l7:
promotion of insight into the influence of unique sensory processing on their functioning, such as productivity at work, concentration, reaction to others' verbal and non-verbal communication, social interaction with others in various environments, sensory stimuli serving as stressors and sensory stimuli that promote stress relief;
analyses, in collaboration with the occupational therapist, the relevant situations, circumstances or environments, in order to develop methods to support their way of sensory processing and thus improve functioning; and
learning relevant life skills, including assertion of themselves, other people and their environment, in order to improve compliance with their own sensory processing needs.
Description of between anger behaviour in terms of sensory processing patterns
In processing the results, it became clear that a notably larger sample size would be necessary to determine statistically significant associations. The results were, however, indicative of the participants' sensory processing and the prevalence of their anger behaviour.
Similarities were noted in participants' sensory processing patterns in relation to the other six anger behaviours. Participants' sensory processing patterns were much the same for their verbal and physical anger behaviour, anger suppression and non-verbal anger behaviour, and anger behaviour to escape and apply calming strategies (see Table II on page 30). These results showed similarities with those of Linden and colleagues31. Behavioural Anger Response Questionnaire (BARQ) Model on anger management styles. The BARQ Model describes direct expression of anger to include verbally and physically aggressive behaviour; avoidance of anger to include conscious efforts to avoid the anger situation, emotions and thoughts about it; and diffusing of anger to include participation in various activities to channel anger3l.
Anger management styles are seen as stable behaviour charac-teristics5l. Dunn and Brownl4 found strong correlations between people's sensory processing patterns and behaviour characteristics. The results of participants' anger behaviour and low registration patterns more than the typical norm and sensory-avoiding patterns more than the typical norm support these correlations. With regard to these sensory processing patterns, it would seem that the various anger behaviour reactions indicated specific patterns of anger behaviour, thus anger management styles. Participants' low registration patterns more than the typical norm and anger behaviours indicated a style of direct anger expression (regular verbal and physical expression of anger, but seldom non-verbal expression of anger, and seldom suppression of anger). Participants' sensory-avoiding patterns more than the typical norm and anger behaviours indicated a style of avoiding anger (regularly withdrawing from anger situations, often suppressing anger, often expressing anger non-verbally, often using substances to manage anger, seldom expressing anger verbally or physically).
Low registration patterns more than the typical norm and direct expression of anger
According to Lombaardl7, it appears that people with low registration patterns more than the typical norm, are less aware of their level of excitement and take long to realise that they are in sensory-overload. It is also applicable to the control of a person's anger. Some people become aware of the intensity of their anger only when it is very high52. In this case, self-control is notably more difficult to apply and an anger outburst with aggressive behaviour can more easily occur. Participants with low registration patterns more than the typical norm indicated poorer self-control (regularly became verbally or physically aggressive), possibly because they became aware of their anger experience only after its intensity drastically increased. Furthermore, the majority of participants with low registration patterns more than the typical norm, used depressants in anger situations, probably to lower their nervous system's level of excitement53. A small number of these participants used stimulants and that would also influence their nervous system's level of excitement, as the abuse of stimulants in general incite euphoric experiences54.
Sensory-avoiding patterns more than the typical norm and avoidance of anger
According to Brown and Dunn, 14 persons with sensory-avoiding patterns more than the typical norm, easily experience sensory stimuli as too intense or overwhelming. In Dunn's Model15, sensory-avoiding patterns occur on the side of the behaviour response continuum that represents the use of active behaviour strategies. Dunnl8 found that people with active behaviour strategies were prone to act proactively, in order to control the amount and type of sensory stimuli at their disposal. It was possible that the majority of participants with sensory-avoiding patterns more than the typical norm, who regularly escape from anger situations or suppressed their anger, could have experienced sensory stimuli paired with anger situations as too intense or overwhelming. To withdraw from anger situations and then apply calming strategies were possibly furthermore connected to these participants' ways of sensory processing, in that they wanted to control the type and amount of sensory stimuli that they are exposed to. The majority of these participants cognitively avoided their anger or used depressants. In this case, the use of substances could be linked to the need to lower their level of excitement53. Functional anger behaviour that was most prevalent was diffusion of anger through participation in a constructive physical activity or a relaxing passive activity. It could also be that these participants regularly expressed their anger non-verbally, because they reacted quicker to the sensory stimuli from an anger situation and more easily experienced it as intense or overwhelming.
The researchers' have hoped that the study's results on sensory processing patterns can first of all contribute to the existing knowledge of anger behaviour in substance abusers. Secondly encourage occupational therapists to consider including the assessment and treatment of sensory processing patterns as part of their anger management and/or substance rehabilitation programme. Lastely to encourage research on the relationships between senory processing patterns and life skills in adult clinical populations.
CONCLUSION AND RECOMMENDATIONS
Anger suppression, substance use and verbal aggression were anger behaviours that occurred regularly in most participants in this study. Very few participants applied calming strategies during anger situations.
The majority of participants in this study displayed low registration, sensory-sensitive and sensory-avoiding patterns more than the typical norm, and sensory-seeking patterns in accordance to the typical norm. The majority of participants with low registration patterns more than the typical norm regularly expressed their anger by becoming verbally or physically aggressive and used substances in anger situations. With regard to participants with sensory-avoiding patterns more than the typical norm, the majority regularly escaped from anger situations, often suppressed their anger, regularly expressed their anger non-verbally and regularly used substances during the experience of anger.
Occupational therapists should consider assessing the sensory processing of their adult patients, such as substance abusers and patients with problematic anger. Adults whose way of sensory processing affects their functioning possibly experience problems with, for example, organising daily tasks, maintaining relationships and being satisfied with their work or life roles. During Occupational Therapy, the relevant situations and environments should be analysed to identify which life skills should be taught during intervention to support the person's sensory processing and thus improve functioning.
The study results indicated that further research on the association between adults' sensory processing and behaviour characteristics, such as anger behaviour, would be worthwhile in clinical and non-clinical populations. The use of a qualitative research approach and purposive or representative sampling are recommended for future studies. This can provide a deeper understanding of the behaviour of clients' who experience specific sensory processing difficulties. It may provide confirmation for quantitative results and support the generalisation of findings.
REFERENCES
1. Mayne TJ, Ambrose TK. Research review on anger in psychotherapy. Journal of Clinical Psychology, 1999; 55: 353-363. [ Links ]
2. Stith SM, Hamby SL. The anger management scale: development and preliminary psychometric properties. Violence and Victims, 2002; 17: 383-402. [ Links ]
3. Deffenbacher JL, Oetting ER Thwaites GA, Lynch RS, Baker DA, Stark RS, Eiswerth-Cox L. State-trait anger theory and the utility of the trait anger scale. Journal of Counselling Psychology, 1996; 43:131-148. [ Links ]
4. Foley PF, Hartman BW, Dunn AB, Smith JE, Goldberg DM. The utility of the stait-trait anger expression inventory with offenders. International Journal of Offender Therapy and Comparitve Criminology, 2002; 46:364-378. [ Links ]
5. Howells K, Day A. 2003. Readiness for anger management: clinical and theoretical issues. Clinical Psychology Review, 2003; 23:319337. [ Links ]
6. Tafrate RC, Kassinove H, Dundin L. Anger episodes in high- and low-trait-anger community adults. Journal of Clinical Psychology, 2002; 58: 1573-1590. [ Links ]
7. Reilly PM, Shopshire MS. Anger management group treatment for cocaine dependence: preliminary outcomes. American Journal of Drug and Alcohol Abuse, 2000; 26: 161-177. [ Links ]
8. Taylor A. Anger intervention. American Journal of Occupational Therapy 1988; 42:147-155. [ Links ]
9. Crouch R. The recovering alcoholic and occupational therapy intervention. In: Crouch R, Alers V editors. Occupational therapy in psychiatry and mental health. 4th ed. London: Whurr Publishers Ltd, 2005:519-536. [ Links ]
10. Grogan MS. Anger Management: clinical applications for occupational therapy (Part 2). Occupational Therapy in Mental Health, 1991; 11: 149-171. [ Links ]
11. Stoffel VC, Moyers PA. An evidence-based and occupational perspective: interventions for persons with substance-use disorders. American Journal of Occupational Therapy, 2004; 58: 570-586. [ Links ]
12. Quadling A, Maree K, Mountjoy L, Bosch G, Kotkin Z. An investigation into a relationship between sensory modulation disorder and substance abuse. South African Journal of Occupational Therapy, 1999; 29: 10-13. [ Links ]
13. Watling R, Bodison T, Henry DA, Miller-Kuhaneck H. Sensory integration: it's not just for children. Sensory Integration Special Interest Section Quarterly, 2006; 29: 1-4. [ Links ]
14. Brown C, Dunn W. Adolescent/adult sensory profile: user's manual. USA: The Psychological Corporation, 2002. [ Links ]
15. Dunn W. The impact of sensory processing abilities on the daily lives of young children and their families: a conceptual model. Infants and Young Children, 1997; 9:23-25 [ Links ]
16. Cheng M, Boggett-Carsjens J. Consider sensory processing disorders in the explosive child: case report and review. The Canadian Child and Adolescent Psychiatry Research, 2005; 14:44-48. [ Links ]
17. Lombaard A. Sensoriese intelligensie: hoekom dit meer saakmaak as IK en emosionele intelligensie [Sensory intelligence: why it matters more than IQ and emotional intelligence]. South Africa: Metz Press, 2007. [ Links ]
18. Dunn W. The sensations of everyday life: empirical, theoretical and pragmatic considerations. American Journal of Occupational Therapy, 2001; 55: 608-620. [ Links ]
19. Desrichard O, Denarié V Sensation seeking and negative affectiv-ity as predictors of risky behaviors: a distinction between occasional versus frequent risk-taking. Addictive Behaviors, 2005; 30: 1449-1453. [ Links ]
20. Wong CC, Schumann G. Review: Genetics of addictions: strategies for addressing heterogeneity and polygenicity of substance abuse disorders. Philosophical Transactions of the Royal Society: Biological Sciences, 2008; 363:3213 [ Links ]
21. Martin LM, Bliven M, Boisvert R. Occupational performance, self-esteem and quality of life in substance addictions recovery. The Occupational Therapy Journal of Research, 2008; 28:81-88. [ Links ]
22. Gutman SA. 2006. Why addiction has a chronic relapsing course. The neurobiology of addiction: implications for occupational therapy practice. Occupational Therapy in Mental Health, 2006; 22:1-26. [ Links ]
23. Buijsse N, Caan W, Davis SF 1999. Occupational therapy in the treatment of addictive behaviours. British Journal of Therapy and Rehabilitation, 1999; 6:300-307. [ Links ]
24. Clarey L, Felstead B. The contribution of occupational therapy to alcohol and drug rehabilitation: a descriptive review. Australian Occupational Therapy lourna, 1990; 37:85-88. [ Links ]
25. Wegner L. Occupational therapy interventions for drug-related disorders. In: Crouch R, Alers V editors. Occupational therapy in psychiatry and mental health, 4th ed. London: Whurr Publishers Ltd, 2005 p. 537-551. [ Links ]
26. Davies R. Accroding to the models of care for the treatment of drug misusers, does occupational therapy have a role in the treatment of drug misuse? British Journal of Occupational Therapy, 2006; 69:575-577. [ Links ]
27. Stensrud MK, Lushbough RS. The implementation of an occupational therapy program in an alcohol and drug dependency treatment center. Occupational Therapy in Mental Health, 1988; 8:1-15. [ Links ]
28. McQueen J, Allan L, Mains D. Brief motivational counselling for alcohol abusers admitted to medical wards. British Journal of Occupational Therapy, 2006, 69:327-333. [ Links ]
30. Kopper BA, Epperson DL. I he experience and expression of anger: relationships with gender, gender role socialization, depression, and mental health functioning. Journal of Counseling Psychology, 1996; 43: 158-165. [ Links ]
31. Linden W, Hogan BE, Rutledge T, Chawla A, Lenz JW, Leung D. There is more to anger coping than "in" or "out". Emotion, 2003; 3: 12-29. [ Links ]
32. Tang, M. Clinical outcome and client satisfaction of an anger management group program. Canadian Journal of Occupational Therapy, 2001; 68:228-236. [ Links ]
33. Miller LJ, Lane SJ. Towards a consensus in terminology in sensory integration theory and practice. Part l: taxonomy of neurophysi-ological processes. Sensory Integration Special Interest Section Quarterly, 2000; 23:1-4. [ Links ]
34. Parham LD. Sensory integration in occupation. In: Bundy AC, Lane SJ, Murray EA, editors. Sensory integration: theory and practice, 2nd ed. Philadelphia: FA Davis Company, 2002: 413-434. [ Links ]
35. Kinnealey M, Oliver B, Wilbarger P A phenomenological study of sensory defensiveness in adults. American Journal of Occupational Therapy, 1994; 49:444-451. [ Links ]
36. Urwin R, Ballinger C. The effectiveness of sensory integration therapy to improve functional behaviour in adults with learning disabilities: five single-case experimental designs. British Journal of Occupational Therapy, 2005; 68:56-66. [ Links ]
37. Mullen B, Champagne T, Krishnamurty S, Dickson D, Gao RX. Exploring the safety and therapeutic effects of deep pressure stimulation using a weighted blanket. Occupational Therapy in Mental Health, 2008; 24:65-89. [ Links ]
38. Lai JS, Parham DL, Johnson-Ecker C. Sensory dormancy and sensory defensiveness: two sides of the same coin? Sensory Integration Special Interest Section Quarterly, 1999; 22:1-4. [ Links ]
39. Pohl PS, Dunn W, Brown C. The role of sensory processing in everyday lives of older adults, Occupational Therapy Journal of Research, 2003;23:99-106. [ Links ]
40. Brown C, Tollefson N, Dunn W, Cromwell R, Filion D. The Adult Sensory Profile: measuring patterns of sensory processing. American Journal of Occupational Therapy, 2001; 55:75-82. [ Links ]
41. Polit DF Beck CT. Essentials of nursing research: methods, appraisals and utilization. Philadelphia: Lippincott Williams & Wilkins, 2006. [ Links ]
42. Joubert G, Ehrlich R. Epidemiology: a research manual for South Africa. 2nd ed. Cape Town: Oxford University Press Southern Africa (Pty) Ltd., 2007. [ Links ]
43. Averill JR. Studies on anger and aggression. Implications for theories of emotion. American Psychologist, 1983; 38: 1145-1160. [ Links ]
and Personality, 1997; 12: 301-324. [ Links ]
45. Parry CD. "Report to parliament 2008: alcohol and drug abuse research unit selected highlights 2007-8." Alcohol and Drug Abuse Research Unit: Parliamentary reports. 2008. <www.mrc.ac.za/ home.htm> (3 December 2008). [ Links ]
46. "About SA: health: alcohol and substance abuse." South Africa Government Information. 2008. <www.info.gov.za/aboutsa/health.htm> (14 November 2008). [ Links ]
47. Del Vecchio T, O'Leary KD. Effectiveness of anger treatments for specific anger problems: a meta-analytic review. Clinical Psychology Review, 2004; 24:15-34. [ Links ]
48. Glancy G, Saini MA. An evidenced-based review of psychological treatments of anger and aggression. Brief Treatments and Crisis Intervention, 2005; 5: 229-248. [ Links ]
49. Holloway JD. Advances in anger management. Monitor, 2003; 34:54. [ Links ]
50. Brown C, Cromwell RL, Filion D, Dunn W, Tollefson N. Sensory processing in schizophrenia: missing and avoiding information. Schizophrenia Research, 2002; 55: 187-195. [ Links ]
51. Eckhardt C, Norlander B, Deffenbacher J. The assessment of anger and hostility: a critical review. Aggression and Violent Behaviour, 2004; 9: 17-43. [ Links ]
52. Potter-Efron RT, Potter-Efron PS. Letting go of anger: the eleven most common anger styles and what to do about them. 2nd ed. Oakland: New Harbinger Publications Inc., 2006. [ Links ]
53. "Central nervous system stimulants." Health A TO Z. 2006. <www. healthatoz.com/healthatoz/Atoz/common/standard/transform. jsp?requestURI=healthatoz/Atoz/ency/central nervous system stimulants.jsp> (29 September 2007). [ Links ]
54. "Central nervous system depressants." Health A TO Z. 2006 <www,healthatoz/Atoz/common/standard/transform. jsp?requestURI=/healthatoz/Atoz/ency/central nervous systemd depressants.jsp> (29 September 2007). [ Links ]
 Correspondence:
Correspondence:
Denisé Stols
ot@denmar.co.za


{kind=link}
{kind=link}
{kind=link}
{kind=link}