










Servicios Personalizados
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkSouth African Journal of Obstetrics and Gynaecology
versión On-line ISSN 2305-8862
versión impresa ISSN 0038-2329
SAJOG vol.28 no.2 Cape Town dic. 2022
http://dx.doi.org/10.7196/sajog.2022.v28i2.2013
RESEARCH
How to care for fetuses with prenatally diagnosed severe abnormalities
C J M Stewart
MMed (O&G); Department of Obstetrics and Gynaecology, Mowbray Maternity Hospital and Faculty of Health Sciences, University of Cape Town, South Africa
ABSTRACT
Ultrasound in pregnancy has become standard of care, resulting in an increased number of antenatally diagnosed fetal anomalies. It is important to have a consistent approach to the management of these abnormalities. This may include offering termination of pregnancy, standard care or non-aggressive/palliative care. A categorisation of anomalies and management options is proposed to assist with these decisions, underpinned by an ethical framework.
Ultrasound examination in pregnancy, including screening for fetal abnormalities, is now standard care in most obstetric services. The World Health Organization and the National Institute for Health and Care Excellence guidelines in the UK both recommend that routine screening for both chromosomal and structural abnormalities be offered to all pregnant women. [1,2] Adequate counselling and informed consent are required prior to screening. Screening for chromosomal abnormalities involves nuchal translucency determination, with or without first-trimester serum biochemical tests, second-trimester biochemical tests, second-trimester ultrasound, or, more recently, non-invasive intrapartum testing.[3-5] Screening for structural abnormalities consists of a detailed ultrasound examination in the second trimester. With advances in imaging and training, more than 60% of major abnormalities can be detected antenatally.[6] Soft markers which, when detected, increase the risk for trisomies 13, 18 or 21 are also sought. A high-risk result from any of the screening tests necessitates that the patient be counselled further regarding karyotyping to confirm an aneuploidy.
Antenatal diagnosis of serious abnormalities has now become commonplace. Some of these are potentially surgically correctable, for example, congenital diaphragmatic hernia, although antenatal and postnatal mortality rates remain high.[7,8] Others, such as spina bifida and Down syndrome, may result in lifelong physical and/or mental disability. Yet others are incompatible with a meaningful life, for example anencephaly and trisomies 13 and 18. These are often referred to as lethal abnormalities, although this term has been called into question in recent times.[9] Extensive counselling of the parents is necessary to provide them with an understanding of the underlying condition, and this inevitably results in complex and emotionally difficult decision-making regarding management for the rest of the pregnancy.
Termination of pregnancy
Laws regarding abortion for serious abnormalities differ from country to country. In South Africa (SA), the Choice on Termination of Pregnancy Act 92 of 1996[10] allows termination of pregnancy for a serious abnormality up to term. It does not, however, define what constitutes a serious abnormality. Fetal medicine units have drawn up their own guidelines concerning the severity of the condition, certainty of the diagnosis, certainty of the outcome, and stratification according to gestational age at diagnosis. The South African Society for Ultrasound in Obstetrics and Gynaecology has produced a position statement to assist practitioners with these decisions in cases of late termination of pregnancy.[11] While patients may be offered the option of termination of pregnancy, in a Western Cape public sector hospital, fewer than 50% of patients accepted termination of pregnancy for serious abnormalities, including Down syndrome and the lethal trisomies (author, unpublished data, 2014). The reasons for refusal were not assessed, but were thought to be related to religious and cultural beliefs. More than 50% of patients therefore continued their pregnancies, even in the presence of serious abnormalities.
Ethical issues in the management of lethal abnormalities
In certain cases, it would be futile to provide extensive neonatal intervention - for example, when the infant is likely to die shortly after birth, or has an extremely small chance of pursuing a meaningful existence. This would apply to lethal abnormalities, such as anencephaly or trisomies 13 and 18. In the case of anencephaly, reports suggest that the majority of infants will die within the first 24 hours after birth, and only 5% will live for more than 6 days.[12] Duration of postnatal life will depend to some extent on the degree of postnatal intervention offered. Many institutions provide 'comfort care' only - keeping the baby warm, hydrated and fed - but would not offer any medical, surgical or ventilatory options. However, others offer more invasive care that would result in prolongation of life. Providing such care has become more common in developed countries, in some of which aggressive therapy is now recommended for trisomies 13 and 18, including surgical correction of cardiac abnormalities.[13-16] In SA, where resource constraints may prevent even babies with a good prognosis from accessing care in a neonatal intensive care unit, this is not feasible. The use of the word 'lethal' has recently been brought into question, because it suggests that the baby will die at birth or within minutes thereafter. As this is not always the case, parents may have incorrect expectations of the outcome. 'Futile care' and 'life-limiting conditions' have been offered as alternatives, although these are also open to interpretation.[9]
In weighing up the ethical obligations to the mother and fetus, the principles of beneficence to the fetus, beneficence to the mother and autonomy of the mother come into play and may be in conflict. Chervenak and co-authors[17,18] have stated that, in the case of an abnormality with no reasonable hope of survival or cognitive function, there is no ethical obligation to the fetus, but the ethical obligation should rather be to avoid harm to the mother by using potentially harmful interventions,[17,18] such as caesarean section. While caesarean section is commonplace and regarded as safe in the modern age, there are reports from resource-constrained countries of maternal mortality rates following caesarean section of up to 1.9%.[19] Furthermore, late complications in subsequent pregnancies, such as uterine rupture and placenta accreta spectrum disorders, need to be considered.
Perinatal palliative care is therefore important for mothers who wish to continue their pregnancies but accept that the outcome is likely to be poor.[20] This care should be provided by a multidisciplinary team, including at least a fetal medicine specialist and a neonatologist. Counselling and communication are key. The diagnosis and the management planned should be agreed upon by both medical personnel and the family, and there should be consistent and clear communication, including a clearly documented plan for delivery and the perinatal period. The delivery plan will need to consider issues such as non-aggressive intrapartum treatment, i.e. no cardiotocograph (CTG) monitoring of the fetus and no recourse to caesarean section for fetal reasons. The neonatal plan will need to make explicit the degree of resuscitation at birth and indications for any interventions, and would generally involve early discharge home to the parents.
Non-aggressive intrapartum care
Fetal monitoring is one of the mainstays of obstetric care in an attempt to optimise pregnancy outcome. CTGs are used antenatally to monitor high-risk fetuses for signs of sudden deterioration, and in labour to monitor for features of suspected fetal compromise. The general reaction to an abnormal CTG is to deliver the fetus as quickly as possible, usually by caesarean section. It can be argued that if a caesarean section is not indicated or possible, CTG monitoring is not indicated.
While the principles of non-aggressive intrapartum care are clear, there is a paucity of literature regarding which abnormalities would qualify for this. Chervenak et al.[17] proposed a classification based on the certainty of the diagnosis and the certainty of the prognosis. They divided abnormalities into three categories. Category A, where the diagnosis was certain and the prognosis of probable death or absence of cognitive developmental capacity was certain, consisted only of anencephaly. Category B consisted of two groups: where the diagnosis was certain and there was a very high probability of death or absent cognitive function, as with trisomies 13 and 18, or where there was a very high probability of a certain diagnosis as well as certainty about the lethal prognosis, such as with renal agenesis. Category C consisted of abnormalities where either the diagnosis was not certain, e.g. lissencephaly, or the prognosis was variable, e.g. hydrocephalus and achondroplasia. They allowed for non-aggressive intrapartum treatment only for category A. In category B, the choice of aggressive or non-aggressive care was made by the mother, and in category C, all fetuses had aggressive intrapartum care, with conservative management not being an option. The difference between categories A and B was based on there being no beneficence-based obligation to the fetus in category A and minimal beneficence-based obligation in category B.
Bijma et al.[21] reported their results of a survey of practice among obstetricians based on whether the abnormality was regarded as having a poor, uncertain or good prognosis. They found that the majority of cases in which the fetus was regarded as having a good prognosis had standard management, while among those in which the prognosis was poor, 25% pregnancies were terminated, 46% had non-aggressive intrapartum care and 26% had standard management. In the uncertain category, 67% had standard management and only 20% had non-aggressive intrapartum management.
A proposal for South Africa
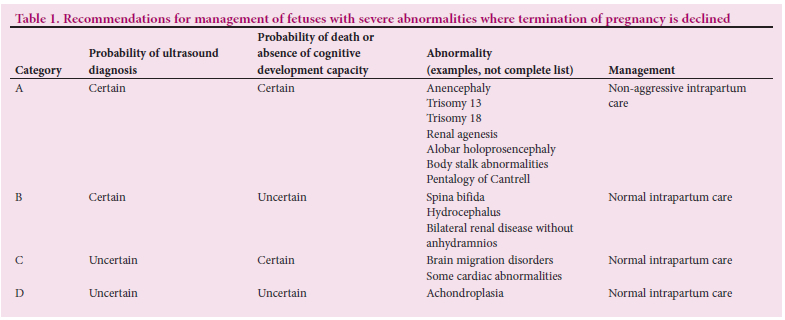
In SA, there are severe resource constraints in the public sector, where the majority of women deliver their babies. Mid-trimester fetal anomaly scans are generally performed by sonographers, who will refer to fetal medicine units if a suspected abnormality is detected. There is a longstanding shortage of trained sonographers, meaning that many women do not have a fetal anomaly scan, and abnormalities may only be detected late in pregnancy when a scan is performed for a complication, such as polyhydramnios, or for an obstetric indication. While late termination of pregnancy is legally available, there is also a shortage of fetal medicine specialists trained in the performance of feticide. In addition, the low acceptance rate for termination of pregnancy in SA results in a number of fetuses with abnormalities conferring a poor prognosis proceeding to term. It is important for there to be clear guidelines on the management of these fetuses during labour and of the neonates at and after birth. A modification of Chervenak et al.'sl171 categorisation is therefore proposed (Table 1), with the reasoning for this explained below.
Category A includes anencephaly and the lethal trisomies. Anencephaly can be diagnosed with certainty by anyone trained in ultrasound scanning for fetal abnormalities. Trisomies 13 and 18 can be confirmed with karyotyping. Although there are reported cases of children with trisomies 13 and 18 living for several months, and occasionally for years, more than 90% will die within the first week after birth.[22] There is therefore a minimal beneficence-based obligation to the fetus. There is, however, a beneficence-based obligation to the mother, as well as respect for her autonomy. In addition, in a resource-constrained environment, the principle of distributive justice is important. Termination of pregnancy should therefore be offered and, in those who decline termination, extraordinary measures should be avoided. Such measures include all medications, treatments and operations that cannot be used without incurring excessive expense, pain or other inconvenience or, if used, would not offer a reasonable hope of benefit. Management would include non-aggressive intrapartum care with no fetal monitoring and avoidance of caesarean section, and would extend to palliative neonatal care. A multidisciplinary team would be important to follow through on these decisions.
In category B, the diagnosis is certain but the prognosis is variable, for example, spina bifida. With high lesions (above L3) and cerebral signs, there is a 30% risk of moderate mental insufficiency, a 30% risk of being wheelchair-bound, a 70% risk of urinary incontinence and a 30% risk of faecal and urinary incontinence.[23] Ultrasound has been used to try to prognosticate. However, the prenatally assigned
level of the lesion underestimates the postnatal functional level used for assessment of neurological function.[24] Severe ventriculomegaly, however, is thought to have some prognostic value in terms of intellectual outcome, with measurements of >15 mm being more indicative of some degree of intellectual disability.[25] It is therefore acceptable to offer termination of pregnancy, including feticide, because of the high risk of severe physical and mental handicap. If the parents decline, however, monitoring must be carried out with awareness of the problems of raising a child with disabilities.
Category C involves conditions where the prognosis is certain but the condition is difficult to diagnose with certainty on ultrasound. An example of this is lissencephaly, where the only ultrasound feature may be mild ventriculomegaly. Magnetic resonance imaging may be helpful in the diagnosis of this condition, but is not always available. In this case, monitoring must occur to avoid jeopardy to fetuses that may be normal.
In the final category, D, both the diagnosis and the prognosis are uncertain, for example, achondroplasia. Here, the diagnosis is often made late when a decrease in the growth trajectory of the fetal limbs is detected. Genetic testing is available in some centres to confirm the diagnosis, but may not be available everywhere. Mental function and life expectancy are normal in the majority of cases. However, there is a risk of spinal compression that can cause paralysis, incontinence, hydrocephalus, and other neurological and respiratory symptoms. Given the uncertainties involved, monitoring is recommended.
It is important to consider that conditions can change over time, influencing the prognosis. A suspected poor prognosis is not sufficient to institute non-aggressive intrapartum care. Certainty is necessary. The fact that termination of pregnancy/feticide was offered is not an indication for non-aggressive intrapartum care. It is therefore best to assign the condition to one of the categories before making a decision regarding monitoring and further management.
Conclusion
In the public sector in SA, there are resource constraints in all aspects of healthcare, including antenatal care and prenatal diagnosis. When a severe fetal anomaly is diagnosed antenatally, counselling of the parents is essential. Management decisions may include offering termination of the pregnancy, standard antenatal care, or non-aggressive intrapartum management. In order to maintain consistency and to facilitate decision-making, a model is proposed that categorises severe conditions and aligns these with ongoing care. The examples mentioned are not exhaustive, but form a framework for classification of other abnormalities. Consideration should be given in the future as to: (i) whether there is room for non-aggressive intrapartum management with graded degrees of certainty or uncertainty; and (ii) in a resource-constrained environment, whether standard intrapartum care, including caesarean section, can be accommodated for life-limiting abnormalities.
Declaration. None.
Acknowledgements. None.
Author contributions. Sole author.
Funding. None
Conflicts of interest. None.
References
1. Oladapo OT. Amniocentesis and chorionic villus sampling for prenatal diagnosis: RHL commentary (last revised 1 April 2009). The WHO Reproductive Health Library. Geneva: World Health Organization. https://srhr.org/rhl/article/amniocentesis-and-chorionic-villus-sampling-for-prenatal-diagnosis (accessed 1 November 2022). [ Links ]
2. National Institute for Health and Care Excellence (NICE). Antenatal care: NICE guideline (NG201). 19 August 2021. www.nice.org.uk/guidance/ng201 (accessed 20 March 2022). [ Links ]
3. Nicolaides KH. Screening for fetal aneuploidies at 11 to 13 weeks. Prenat Diagn 2011;31(1):7-15. https://doi.org/10.1002/pd.2637 [ Links ]
4. Evans MI, O'Brien JE, Dvorin E, Harrison H, Bui TH. Second-trimester biochemical screening. Clin Perinatol 2001;28(2):289-301. https://doi.org/10.1016/s0095-5108(05)70084-1 [ Links ]
5. Hill M, Wright D, Daley R, et al. Evaluation of non-invasive prenatal testing (NIPT) in an NHS setting: A reliable, accurate non-invasive prenatal diagnosis (RAPID) protocol. BMC Pregnancy Childbirth 2014;14:229. https://doi.org/10.1186/1471-2393-14-229 [ Links ]
6. Chen M, Leung TY, Sahota DS. Ultrasound screening for fetal structural abnormalities performed by trained midwives in the second trimester in a low-risk population - an appraisal. Acta Obstet Gynecol Scand 2009;88(6):713-719. https://doi.org/10.1080/00016340902934688 [ Links ]
7. Gallot D, Boda C, Ughetto S, et al. Prenatal detection and outcome of congenital diaphragmatic hernia: A French registry-based study. Ultrasound Obstet Gynecol 2007;29(3):276-283. https://doi.org/10.1002/uog.3863 [ Links ]
8. Colvin J, Bower C, Dickinson JE, Sokol J. Outcomes of congenital diaphragmatic hernia: A population-based study in Western Australia. Pediatrics 2005;116(3):e356-e363. https://doi.org/10.1542/peds.2004-2845 [ Links ]
9. Wilkinson D, de Crespigny L, Xafis V. Ethical language and decision-making for prenatally diagnosed lethal malformations. Semin Fetal Neonat Med 2014;19(5):306-311. https://doi.org/10.1016/j.siny.2014.08.007 [ Links ]
10. Republic of South Africa. Choice on Termination of Pregnancy Act 92 of 1996. https://www.parliament.gov.za/storage/app/media/ProjectsAndEvents/womensmonth_2015/docs/Act92of1996.pdf (accessed 1 November 2022). [ Links ]
11. South African Society for Ultrasound in Obstetrics and Gynaecology (SASUOG). SASUOG position statement on the late termination of pregnancy for fetal anomalies (TOPFA). https://www.sasuog.org.za/MemberPanel/downloads/SASUOG%20Position%20statement%20on%20late%20TOP%20for%20fetal%20anomalies.pdf (accessed 5 June 2022). [ Links ]
12. Jaquier M, Klein A, Boltshauser E. Spontaneous pregnancy outcome after prenatal diagnosis of anencephaly. Int J Obstet Gynaecol 2006;113(8):951-953. https://doi.org/10.1111/j.1471-0528.2006.01014.x [ Links ]
13. Bruns D, Campbell E. Twenty-two survivors over the age of 1 year with full trisomy 18: Presenting and current medical conditions. Am J Med Genet A 2013;164A(3):610-619. https://doi.org/10.1002/ajmg.a.36318. [ Links ]
14. Subramaniam A, Jacobs AP, Tang Y, et al. Trisomy 18: A single center evaluation of management trends and experience with aggressive obstetric and neonatal intervention. Am J Med Genet A 2016;170A(4):838-846. https://doi.org/10.1002/ajmg.a.37529 [ Links ]
15. Kato E, Kitase Y, Tachibana T, et al. Factors related to survival discharge in trisomy 18: A retrospective multicenter study. Am J Med Genet A 2019;179A(7):1253-1259. https://doi.org/10.1002/ajmg.a.61146 [ Links ]
16. Kosiv KA, Long J, Lee HC, Collins RT 2nd. A validated model for prediction of survival to 6 months in patients with trisomy 13 and 18. Am J Med Genet A 2021;185A(3):806-813. https://doi.org/10.1002/ajmg.a.62044 [ Links ]
17. Chervenak FA, McCullough LB, Levene I. An ethically justified, clinically comprehensive management strategy for third-trimester pregnancies complicated by fetal anomalies. Obstet Gynaecol 1990;75(3 Part 1):311-316. [ Links ]
18. Chervenak FA, McCullough LB. Nonaggressive obstetric management: An option for some anomalies during the third trimester. JAMA 1989;261(23):3439-3440. https://doi.org/10.1001/jama.261.23.3439 [ Links ]
19. Van Roosmalen J, van den Akker T. Safety concerns for caesarean section. BJOG 2014;121(7):909- 910. https://doi.org/10.1111/1471-0528.12747 [ Links ]
20. Perinatal Palliative Care: ACOG Committee Opinion, Number 786. Obstet Gynecol 2019;134(3):e84-e89. https://doi.org/10.1097/AOG.0000000000003425 [ Links ]
21. Bijma HH, Wildschut HI, van der Heide A, van der Maas PJ, Wladimiroff JW. Obstetricians' agreement on fetal prognosis after ultrasound diagnosis of fetal anomalies. Prenat Diagn 2004;24(9):713-718. https://doi.org/10.1002/pd.972 [ Links ]
22. Lakovschek IC, Streubel B, Ulm B. Natural history of trisomy 13, trisomy 18 and triploidy after prenatal diagnosis. Am J Med Genet A 2011;155A(11):2626-2633. https://doi.org/10.1002/ajmg.a.34284 [ Links ]
23. Roach JW, Short BF, Saltzman HM. Adult consequences of spina bifida: A cohort study. Clin Orthop Relat Res 2011;469(5):1246-1252. https://doi.org/10.1007/s11999-010-1594-z [ Links ]
24. Appasamy M, Roberts D, Piling D, Buxton N. Antenatal ultrasound and magnetic resonance imaging in localising the level of the lesion in spina bifida and correlation with postnatal outcome. Ultrasound Obstet Gynecol 2005;27(5):530-536. https://doi.org/10.1002/uog.2755 [ Links ]
25. Peralta CB, Bunduki V, Plese JP, et al. Association between prenatal sonographic findings and postnatal outcome in 30 cases of spina bifida aperta. Prenat Diagn 2003;23(4):311-314. https://doi.org/10.1002/pd.584 [ Links ]
 Correspondence:
Correspondence:
C J M Stewart
chantalstewart40@gmail.com
Accepted 8 November 2022


{kind=link}