










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAfrican Journal of Disability (Online)
versão On-line ISSN 2226-7220
versão impressa ISSN 2223-9170
Afr. j. disabil. (Online) vol.8 Durbanville 2019
http://dx.doi.org/10.4102/ajod.v8i0.582
CASE STUDY
Integrated home-based screening for people living with disabilities: A case study from rural Malawi
Elizabeth M. PetersenI; Emily B. WroeI, II; Kondwani NyanguluII; Chisomo KanyendaII; Sam NjolomoleII; Elizabeth L. DunbarIII; Chiyembekezo Z. KachimangaII
IDivision of Global Health Equity, Brigham and Women's Hospital, Boston, United States
IIPartners In Health, Neno, Malawi
IIIPartners In Health, Harper, Liberia
ABSTRACT
People living with disabilities (PLWDs) have poor access to health services compared to people without disabilities. As a result, PLWDs do not benefit from some of the services provided at health facilities; therefore, new methods need to be developed to deliver these services where PLWDs reside. This case study reports a household-based screening programme targeting PLWDs in a rural district in Malawi. Between March and November 2016, a household-based and integrated screening programme was conducted by community health workers, HIV testing counsellors and a clinic clerk. The programme provided integrated home-based screening for HIV, tuberculosis, hypertension and malnutrition for PLWDs. The programme was designed and implemented for a population of 37 000 people. A total of 449 PLWDs, with a median age of 26 years and about half of them women, were screened. Among the 404 PLWDs eligible for HIV testing, 399 (99%) agreed for HIV testing. Sixty-nine per cent of PLWDs tested for HIV had never previously been tested for HIV. Additionally, 14 patients self-reported to be HIV-positive and all but one were verified to be active in HIV care. A total of 192 of all eligible PLWDs above 18 years old were screened for hypertension, with 9% (n = 17) referred for further follow-up at the nearest facility. In addition, 274 and 371 PLWDs were screened for malnutrition and tuberculosis, respectively, with 6% (n = 18) of PLWDs referred for malnutrition, and 2% (n = 10) of PLWDs referred for tuberculosis testing. We successfully implemented an integrated home-based screening programme in rural Malawi.
Keywords: Malawi; disability; screening; task shifting; primary healthcare.
Introduction
People living with disabilities (PLWDs) constitute up to 15% of the global population, and about 80% of them live in low- and middle-income countries (Hanass-Hancock et al. 2016). It is well documented that PLWDs have poor access to healthcare, a problem that is worse in rural than urban areas (World Health Organization [WHO] 2011). For sexual and reproductive health services (SRHS), PLWDs are often not involved in planning nor targeted for routine treatment and screening. Healthcare workers are often not trained on how to provide services to PLWDs, and some deny them care as they consider PLWDs asexual (Hanass-Hancock 2009). Although the disability itself may prevent access to care, some studies also attribute access difficulties to poor socio-economic status (Eide et al. 2015; Vergunst et al. 2017). For example, in many African countries, including Malawi, the main reasons for lack of access to health services for PLWDs include lack of transport, inadequate availability of services, drugs and equipment, and high out-of-pocket costs (Eide et al. 2015). These challenges are magnified by a weak health system, poverty, illiteracy, stigma and marginalisation of PLWDs (Hanass-Hancock, Regondi & Naidoo, 2013; Vergunst et al. 2017).
Caregivers and families of PLWDs also face challenges with accessing health services. Households with PLWDs are worse off: they tend to have a high number of dependents, high unemployment, a lower income, reduced access to education and in general have higher levels of poverty (Munthali 2011).
People living with disabilities are a vulnerable population, and healthcare systems should be adapted to address their barriers to care. With the shortage of professional healthcare workers in many low-income countries, including Malawi (Malawi Government, 2017), new approaches for delivering services in the community and household need to be developed. One approach is task shifting, a process of transitioning complex responsibilities to less specialised staff. While task shifting has been successful in many SRHS, including HIV programmes (Callaghan, Ford & Schneider 2010; Dawson et al. 2014), programmes need to adapt task shifting for home-based screening, focusing on appropriate supervision, well-trained staff and appropriate allocation of responsibilities to ensure quality services (Dawson et al. 2014).
Neno District is a southwestern district of Malawi with an estimated population of 150 800 (National Statistical Office 2008). Recent estimates showed that approximately 5000 people, or 3.5% of the population, are living with disabilities (Partners In Health 2015). This case study reports an approach to home-based screening for HIV, malnutrition, tuberculosis and hypertension for PLWDs and their families in Neno District.
Setting and approach
The PLWDs home-based screening programme was instituted in response to a 2014 survey conducted by community health workers (CHWs) to identify the number of PLWDs in Neno District. The CHWs, who are all long-term residents of Neno and have been employed since 2007, focus on education, case identification and referral for HIV and tuberculosis services. During the survey, PLWDs expressed significant challenges in accessing screening services because of lack of transport and lack of health service prioritisation for PLWDs at the facilities.
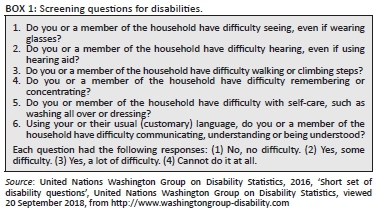
To address these challenges, in 2016, this programme was piloted in a remote area on the Mozambique border, targeting an estimated 1300 PLWDs of the population of 37 000 people (Partners In Health 2015). Neno is one of the poorest and most remote districts of Malawi, with a poverty level 15% higher than the national average (National Statistical Office 2012). The goal was to revisit households that registered PLWDs during the survey and offer screening services. Additionally, efforts were made to identify PLWDs not originally identified. As in the initial survey, PLWDs were identified based on the International Classification of Functioning, Disability and Health (ICF), which encompasses impairments, activity limitations and participation restrictions (WHO, 2018). People living with disabilities were identified by asking disability-related questions that identified functional limitations in the three domains of ICF (Box 1). Based on the screening questions, people were classified as either having a disability or not; no grading of disability was performed.
To maximise integration, several screening programmes were combined, namely HIV, tuberculosis, malnutrition and hypertension (Table 1). Because of shortage of clinical staff, task shifting for home-based screening utilised three groups of support staff: CHWs on a monthly stipend, one clerk from the HIV clinic and HIV testing counsellors. Community health workers personally knew the PLWDs and were responsible for informing community leaders and households at least a day before the screening. Additionally, as part of their routine tasks, CHWs were already trained to provide malnutrition and tuberculosis screening. For HIV screening, existing HIV counsellors provided counselling, testing and referral. These counsellors were already working in the district and received a standard 4-week training organised by Malawi Ministry of Health. The clerk who normally worked in an HIV clinic providing routine screening provided hypertension, tuberculosis and malnutrition screening and supervised the team. None of the staff were providing all four screenings as HIV screening required nationally certified HIV providers. This multidisciplinary team received a 2-day additional training on identification of PLWDs, appropriate communication to PLWDs and screening and referral procedures for different conditions. All screening was provided free of charge.
Household-based screening started in March 2016. Consent to screen households for PLWDs was obtained from the head of household. Additional informed consent was obtained from PLWDs if they were over 18 years and fit to give consent, and if not, informed consent was obtained from a legal guardian. To ensure confidentiality, all screening and communication of results was conducted in a private space within the household. If PLWDs or household members screened positive or were seen to be sick, they were counselled on-site about their condition by a team member and referred to the nearest facility. Since households with PLWDs often have barriers in accessing healthcare services, the screening was offered to all household members who were given a choice to opt out of any of the screening services, although the intervention prioritised screening PLWDs.
As the screening team was already working with patients, they were reminded on infection prevention and given materials for infection prevention. This home visit package is explained in Table 1. All results were recorded in a specially designed screening register and were transferred to Excel for cleaning and analysis.
Relevant changes
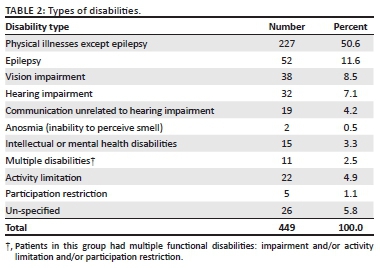
Between March and November 2016, 600 people were screened in their homes. Among the individuals screened, 75% (n = 449) were PLWDs and the remaining were their family members. The median age of PLWDs was 26 years (IQR 13-51), 48% (n = 217) were women and 70% (n = 315) were 15 years and above (Tables 2 and 3).
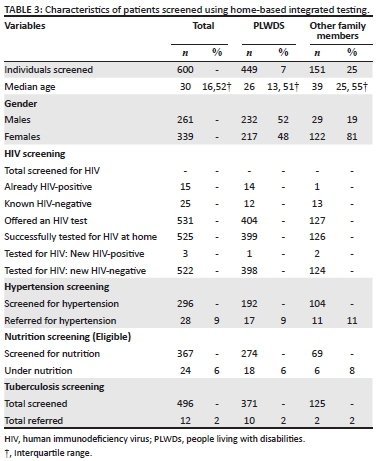
Of the 449 PLWDs screened for HIV, only 6% (n = 26) of those eligible for testing had a known HIV status (14 were HIV-positive and 12 had a negative test result within the past 3 months). Among those who were HIV-positive (n = 14), all except one individual were enrolled in HIV care.
Among all remaining PLWDs (n = 404), three people were ineligible for an HIV test as they were aged less than 2 years, and two individuals declined testing. Of those eligible for an HIV test, 99% (n = 399) accepted the HIV test. Among the 399 tested successfully, 69% (276) never had an HIV test before. At the end of the screening, one person tested HIV-positive and was successfully linked to care.
In total, 192 of the 280 eligible PLWDs above 18 years old were screened for hypertension, with 9% (n = 17) referred for follow-up for blood pressures greater than 160 mmHg systolic or 110 mmHg diastolic. An additional 274 and 371 PLWDs were screened for malnutrition and tuberculosis, respectively. Six per cent (n = 18) of those screened for malnutrition were referred to care, as were 2% (n = 10) of those screened for tuberculosis.
Lessons learnt
As Malawi is struggling with a double burden of HIV and non-communicable diseases, programmatic approaches are needed to reach key populations where they live (Malawi Government 2017). Because of a shortage of health workers, it may not be possible to use formally trained professionals to provide household-based screening. Limited information describing the use of task shifting to identify PLWDs and provide household screening exists in Malawi. Household-based studies report on disability identification and linkage to care by CHWs and/or non-clinical staff (Mulwafu et al. 2017; Tataryn et al. 2017). We could not find any programme that employed task shifting to provide integrated household screening, including hypertension screening, for PLWDs.
Secondly, the programme demonstrated the feasibility and acceptability of combining screening for HIV and other conditions, including hypertension, in a household setting: a high proportion of PLWDs accepted the services. However, few family members accepted to be screened. The screening team focused screening the PLWDs and it may be the reason that influenced lower uptake, but we were not able to collect information on why family members and some PLWDs refused some of the screening. This could be addressed in programmes similar to this case study.
Thirdly, this project provided one approach for household-based targeted disease screening, specifically for HIV, to a vulnerable population. People living with disabilities were targeted because of their limited access to services. Up to 10% of the PLWDs were referred for services. A large majority of the PLWDs had never before had an HIV test, which is striking given the considerable investments on HIV programme in Malawi. We hypothesise that this could be the result of stigma and difficulty accessing available services related to disability (Mcbain et al. 2017). Further efforts will be required to ensure that patients who tested negative remain negative; this will be addressed through continued preventive services by the CHWs. After the pilot, we could not roll out the programme to the whole district because of limited funding; however, with funding, this could be scaled up to other settings, and considering the specific needs of PLWDs is a component of ongoing exploration in Neno for the optimisation of integrated home visits.
There are a few notable limitations to this programme. Firstly, the disability identification tool we used mainly identified self-reported functional disability. Additionally, this identifies the most common disabilities and may miss 'invisible disabilities', such as mental health disorders. We also could not measure the severity of the disabilities. Secondly, the programme was carried out with a small population in a remote area of Malawi, making it difficult to generalise to Neno and other district of Malawi. Thirdly, we were not able to cost this programme that would give more information in whether scale-up would be recommended. Fourthly, we referred patients to the nearest health facilities but were not able to ascertain if all PLWDs were successfully linked to care.
Future programmes would consider the following steps to improve on our limitations: (1) expand household screening to other common chronic condition such as diabetes as they are also common in low- and middle-income countries, (2) cover a larger population to identify more PLWDs who can benefit from the screening, (3) design efforts that can be made to ensure that many family members of PLWDs are screened and document reasons of refusals for both PLWDs and family members, (4) measure costs to help other programme managers to plan and implement this programme and (5) design strategies to ensure that referred PLWDs receive the care at the facility as they may either not go to facilities or face other barriers once they arrive at the facility.
NB: The disability-associated questions were designed by United Nations Washington Group on Disability Statistics (http://www.washingtongroup-disability.com). They were translated to local language by bilingual speaker (both English and Chichewa speaker [local language of Malawi]) and were pre-tested in the initial survey conducted in 2014. The people screened were classified as either having disability (if they have a score 2 or above) or no disability if they score 1. The type of disability was also recorded.
Acknowledgements
The authors thank all the community health workers, HIV testing counsellors, Integrated Chronic Care staff, Ministry of Health and Partners In Health staff members who participated in this community-integrated screening programme.
Competing interests
The authors have declared that no competing interests exist.
Authors' contributions
E.M.P. designed and implemented the project, conceptualised the study, wrote the first draft and conducted data analysis. E.B.W. designed and implemented the project, conceptualised the study, wrote the first draft and conducted data analysis. K.N. designed and implemented the project. C.K. implemented the project. S.N. designed and implemented the project. E.L.D. designed and implemented the project and conducted data analysis. C.Z.K. conceptualised the study, wrote the first draft and conducted data analysis. E.M.P. and E.B.W. have equal contribution to the study. All authors provided input to the manuscript and approved the final draft for submission.
Ethical considerations
The project was conducted as part of a routine clinical care in Neno, and as a result, we did not obtain informed consent. The data were de-identified and retrospectively analysed. The study was approved by Malawi National Health Sciences Research Committee (protocol #1216).
Funding information
This study was funded by US PEPFAR small grants programme in Malawi.
Data availability statement
The data used in this case study belongs to the Ministry of Health in Neno District. As a result, the data cannot be shared publicly. However data can be shared upon request to the corresponding author.
Disclaimer
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of any affiliated agency of the authors
References
Callaghan, M., Ford, N. & Schneider, H., 2010, 'A systematic review of task- shifting for HIV treatment and care in Africa Review', Human Resources for Health 8(8), 1-9. https://doi.org/10.1186/1478-4491-8-8 [ Links ]
Dawson, A.J., Buchan, J., Duffield, C., Homer, C.S.E. & Wijewardena, K., 2014, 'Task shifting and sharing in maternal and reproductive health in low-income countries: A narrative synthesis of current evidence', Health Policy and Planning 29(3), 396-408. https://doi.org/10.1093/heapol/czt026 [ Links ]
Eide, A.H., Mannan, H., Khogali, M., Van Rooy, G., Swartz, L., Munthali, A. et al., 2015, 'Perceived barriers for accessing health services among individuals with disability in four African countries', PLoS One 10(5), e0125915. https://doi.org/10.1371/journal.pone.0125915 [ Links ]
Hanass-Hancock, J., 2009, 'Disability and HIV/AIDS - A systematic review of literature on Africa', Journal of the International AIDS Society 12(34). https://doi.org/10.1186/1758-2652-2-9 [ Links ]
Hanass-Hancock, J., Chappell, P., Myezwa, H., Kwagala, B., Boivin, J.-M., Lloyd, J. et al., 2016, 'Committing to disability inclusion to end AIDS by 2030', The Lancet HIV 3(12), e556-e557. https://doi.org/10.1016/S2352-3018(16)30194-1 [ Links ]
Hanass-Hancock, J., Regondi, I. & Naidoo, K., 2013, 'Disability and HIV: What drives this relationship in Eastern and Southern Africa?', African Journal of Disability 2(1), 1-6. https://doi.org/10.4102/ajod.v2i1.25 [ Links ]
Malawi Government, 2017, Health sector strategic plan II 2017-2022, towards universal health coverage, viewed n.d., from http://www.nationalplanningcycles.org/sites/default/files/planning_cycle_repository/malawi/health_sector_strategic_plan_ii_030417_smt_dps.pdf.
Mcbain, R.K., Petersen, E., Tophof, N., Dunbar, E.L., Kalanga, N., Nazimera, L. et al., 2017, 'Impact and economic evaluation of a novel HIV service delivery model in rural Malawi', AIDS 31(14), 1999-2006. https://doi.org/10.1097/QAD.0000000000001578 [ Links ]
Mulwafu, W., Kuper, H., Viste, A. & Goplen, F.K., 2017, 'Feasibility and acceptability of training community health workers in ear and hearing care in Malawi: A cluster randomised controlled trial', BMJ Open 7(10), e016457. https://doi.org/10.1136/bmjopen-2017-016457 [ Links ]
Munthali, A.C., 2011, A situation analysis of persons with disabilities in Malawi, Center for Social Research, University of Malawi, Zomba.
National Statistical Office, 2008, Malawi population and housing census, National Statistical Office, Zomba, viewed 12 April 2015, from http://www.nsomalawi.mw/index.php?option=com_content&view=article&id=106:2008-population-and-housing-census&catid=8&Itemid=6.
National Statistical Office, 2012, Integrated household survey report, National Statistical Office, Zomba, viewed 01 May 2014, from http://www.nsomalawi.mw/index.php?option=com_content&view=article&id=43&Itemid=61.
Partners In Health, 2015, Neno district people with disabilities needs assessment: Key findings, Partners In Health, Neno.
Tataryn, M., Polack, S., Chokotho, L., Mulwafu, W., Kayange, P., Banks, L.M. et al., 2017, 'Childhood disability in Malawi: A population based assessment using the key informant method', BMC Pediatrics 17(1), 198. https://doi.org/10.1186/s12887-017-0948-z [ Links ]
United Nations Washington Group on Disability Statistics, 2016, 'Short set of disability questions', United Nations Washington Group on Disability Statistics, viewed 20 September 2018, from http://www.washingtongroup-disability.com
Vergunst, R., Swartz, L., Hem, K.-G., Eide, A.H., Mannan, H., MacLachlan, M. et al., 2017, 'Access to health care for persons with disabilities in rural South Africa', BMC Health Services Research 17(741), 1-8. https://doi.org/10.1186/s12913-017-2674-5. [ Links ]
World Health Organization (WHO), 2011, World report on disability, WHO Press World Health Organization, Geneva.
World Health Organization (WHO), 2018, Disabilities, World Health Organization, viewed 19 July 2018, from https://www.who.int/topics/disabilities/en/.
 Correspondence:
Correspondence:
Chiyembekezo Kachimanga
chembekachimanga@yahoo.co.uk
Received: 15 Oct. 2018
Accepted: 19 Sept. 2019
Published: 22 Nov. 2019


{kind=link}