










Serviços Personalizados
Artigo
 Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
Indicadores

Links relacionados
-
 Citado por Google
Citado por Google -
 Similares em Google
Similares em Google
Compartilhar

 Permalink
PermalinkAfrican Journal of Disability (Online)
versão On-line ISSN 2226-7220
versão impressa ISSN 2223-9170
Afr. j. disabil. (Online) vol.6 Durbanville 2017
http://dx.doi.org/10.4102/ajod.v6i0.264
ORIGINAL RESEARCH
The development and evaluation of content validity of the Zambia Spina Bifida Functional Measure: Preliminary studies
Margaret M. MweshiI; Seyi L. AmosunII; Mary P. Shilalukey-NgomaIII; Esther Munalula-NkanduI; Zuhayr KafaarIV
IDepartment of Physiotherapy, School of Medicine, University of Zambia, Zambia
IIDivision of Physiotherapy, School of Health & Rehabilitation Sciences, University of Cape Town, South Africa
IIIDepartment of Paediatric & Child Health, School of Medicine, University of Zambia, Zambia
IVDepartment of Psychology, Faculty of Arts & Social Sciences, Stellenbosch University, South Africa
ABSTRACT
BACKGROUND: Very little is known on outcome measures for children with spina bifida (SB) in Zambia. If rehabilitation professionals managing children with SB in Zambia and other parts of sub-Saharan Africa are to instigate measuring outcomes routinely, a tool has to be made available. The main objective of this study was to develop an appropriate and culturally sensitive instrument for evaluating the impact of the interventions on children with SB in Zambia.
METHODS: A mixed design method was used for the study. Domains were identified retrospectively and confirmation was done through a systematic review study. Items were generated through semi-structured interviews and focus group discussions. Qualitative data were downloaded, translated into English, transcribed verbatim and presented. These were then placed into categories of the main domains of care deductively through the process of manifest content analysis. Descriptive statistics, alpha coefficient and index of content validity were calculated using SPSS.
RESULTS: Self-care, mobility and social function were identified as main domains, while participation and communication were sub-domains. A total of 100 statements were generated and 78 items were selected deductively. An alpha coefficient of 0.98 was computed and experts judged the items.
CONCLUSIONS: The new functional measure with an acceptable level of content validity titled Zambia Spina Bifida Functional Measure (ZSBFM) was developed. It was designed to evaluate effectiveness of interventions given to children with SB from the age of 6 months to 5 years. Psychometric properties of reliability and construct validity were tested and are reported in another study.
Introduction
Spina Bifida (SB) is one of the congenital malformations of the central nervous system that is a major and unrecognised expensive public health problem in much of Africa (Adeleye, Magbagbeola & Olowookere 2010; Blenchowe et al. 2010; Mweshi et al. 2015). It is the commonest of the neural tube defects, and hydrocephalus commonly occurs in association (Fabiano, Doyle & Grand 2010; Qureshi 2010; Sacko et al. 2010). The two are the most recurrent and disabling malformations in neonates in the sub-Saharan African paediatric environment which have a huge impact on the functioning of a growing child (Mweshi et al. 2010).
Children with SB need specialists who can address problems related to hydrocephalus, neurogenic bowel and bladder, mobility, learning disabilities and functional limitations. They also require generalists who can help educate caregivers and address health promotion issues, including nutrition and exercise. Thus, a multidisciplinary team comprising neurosurgeons, neurologists, orthopaedic surgeons, urologists, physiotherapists, paediatricians, neuro-nurses, rehabilitation specialists, psychologists and social workers is what is recommended for the management of children with SB (Mitchell et al. 2004). Consequently, the delivery of this complex care requires an integrated system that aligns and informs all parties involved (Adzick et al. 2011; Liptak & El Samra 2010).
Studies performed on the management of children with SB in some African countries such as Nigeria, Cameroon, Kenya, Uganda and Zambia have reported challenges encountered in the management of SB (Adeleye et al. 2010; Blenchowe et al. 2010; Mweshi et al. 2015). No outcomes have been reported on the management of children with SB in sub-Saharan Africa; hence, knowledge on instrument measures that could be used has been unavailable. Given the several studies performed in many African countries without reported evidence of the impact of management, one could probably assume that either appropriate instrument measures are inaccessible or that they do not just exist. This situation ultimately creates a gap in the provision of evidence of the impact of interventions given to such children in the regions of sub-Saharan Africa. Therefore, in order to investigate how other rehabilitation professionals outside the region manage to measure the impact of the interventions given to children with SB, a systematic review was carried out.
The search strategies used were the Cochrane, Database Specification Review, Autodesk Certified Professional Journal Club, Database of Abstract Reviews Effects, Cochrane Controlled Trial Register, Comprehensive Microbial Resource, Health Technology Assessment and National Health Service Economic Evaluation Database from 1950 to January 2010. A total of 705 (n = 705) titles and abstracts related to the topic were retrieved and reviewed. Eighty-two (n = 82) titles were deemed relevant by the researchers. Subsequently, data were extracted from all fitting methodological articles (n = 19) of which six (n = 6) were located and critiqued. Consequently, four (n = 4) studies were critically appraised and evidence was reported.
The results of the search showed that the instruments identified were the Gross Motor Function Measure (GMFM) Dimensions D and E, Pediatric Outcomes Data Collection Instrument Parent and Child versions, Gillette Functional Assessment Questionnaire Walking subscale, Functional Independence Measure for Children (WeeFIM), Pediatric Quality of Life Inventory, temporal-spatial gait parameters, O(2) cost during ambulation, Child Health Questionnaire, Functional Mobility Scale, Pediatric Evaluation of Disability Inventory (PEDI), CP QOL-Child, and QOL (KIDSCREEN), Bruininks-Osserestsky tests, Alberta Infant Motor Scale and Bayley Scale of Infant development (Harvey et al. 2008; Oeffinger et al. 2007; Sullivan et al. 2007). Subsequently, the search revealed 11 outcome measures of which two are commonly used tools for measuring interventional outcomes in children: the PEDI and the WeeFIM validated for American children (Berg et al. 2008; Sirzai et al. 2008; Sonel et al. 2009).
Based on the results of the literature search, it can be concluded that there is no empirical data showing evidence of the PEDI and WeeFIM being translated into any of the African languages and their usage in Africa. However, although the two measures have not been so easily available and perhaps applicable for Zambian children, there is a lot that could be learnt from the same measures. On the other hand, it is also extremely important to note that there has been a paradigm shift of thinking from a developmental focus to functional focus in paediatric rehabilitation. For instance, worldwide researchers and clinicians who have used the PEDI have highlighted variations in functional skill acquisition in clinical populations. Furthermore, the importance of recognising cultural differences and the value of documenting functional progress in relation to interventions must be upheld (Haley et al. 2010). It is therefore quite imperative to recognise the shift of thought from the original authors of the PEDI who at one time encouraged the idea of translating the tool into local languages while using the normative data from the USA to determine whether a deficit or delay existed with regard to functional skill development (Berg et al. 2008).
Additionally, there has been some debate over issues of culture and the importance of cultural validation of norm-referenced tests (Berg et al. 2008; Sirzai et al. 2008; Sonel et al. 2009). Despite the consensus on what appears to be the impact of culture on the functioning of children, some efforts have been made to translate the PEDI into Dutch, Norwegian, Swedish, Spanish, Turkish, Portuguese, Slovene, Icelandic, French, Hebrew, Japanese and Chinese languages (Haley et al. 2010; Jahnsen et al. 2002). A number of these international users have reported challenges applying the PEDI to their own culture. One of the issues in translating the PEDI is finding comparable words in each country's language. For example, a Norwegian team has reported difficulty finding comparable Norwegian words for 'prompting', 'fasteners' and 'item'. Cultural differences required item adaptations and additions to the PEDI, for example the Dutch team added 'bicycling' to their mobility scale.
Inasmuch as facilitating international comparison is extremely essential in some cases, comparing the lifestyle of an American child with a typical Zambian child in terms of function may not be easily justifiable. This is because ethno-theories of most countries in the developed world are very different from those of the developing world because of cultural diversity. For example, Zambian children start crying for food at a later stage compared with Dutch and Turkish children (Willemsen & Fons 1997). This just highlights the importance of recognising the ability of a growing Zambian child to communicate the need to eat and drink because children are breastfed for a very long time and may need to develop the survival skills after being weaned from breast milk. This is supported by the notion that breastfeeding in Zambia is on demand and when the child is no longer breastfed there is a separation from the mother physically and emotionally (Chibuye, Mwenda & Osborne 1986). Other differences in culture for instance are that the PEDI and WeeFIM include the use of fork and knife in the evaluation. The two utensils may be considered unsafe for use by Zambian parents or caregivers of children with disabilities. It is therefore clear that instruments such as the PEDI or WeeFIM that are in use in the USA and Europe may lack appropriate items essential for Zambian children and may also include tasks and materials which are not encouraged in the Zambian culture. Therefore, the two instruments may not be easily applicable on Zambian children. As a consequence, Clinicians like physiotherapists managing children with SB in Zambia, cannot effectively quantify the impact of interventions given to the children and hence cannot produce evidence (Mweshi et al. 2011:20).
As evidence-based practice (EBP) and initiatives to improve the quality of healthcare and life in children with disabilities have grown around the world, recognition of the need to measure functional outcomes in all healthcare settings has also increased. While there has been such increasing emphasis on the provision of evidence by rehabilitation professionals worldwide (Kaplan 2007), rehabilitation outcomes have been less reported in the developing world because of limited and lack of appropriate instrument measures. The inability of appropriate measures should provoke African researchers to be innovative and develop measures that are culturally sensitive to the needs of African children with disabilities.
Considering the lack of specific outcome measures developed for evaluating the impact of interventions given to children with SB and lack of appropriate and culturally sensitive tools among the ones available, it was deemed necessary that a measure be developed in order to measure the level of functioning in children with SB in Zambia. In view of such limitations and the relevance of using a psychometrically sound instrument in paediatric rehabilitation, we set out to develop a culturally appropriate, multidisciplinary and sensitive functional measure for children with SB in Zambia and subsequently tested it for psychometric properties. The purpose of this paper was to describe the processes involved in the preliminary development and content validation of the Zambia Spina Bifida Functional Measure (ZSBFM).
Methodology
The study was carried out at the University Teaching Hospital (UTH) and Beit Cure Hospital (BCH). Both the hospitals, which are the only centres providing specialised care to children with SB in Zambia, are found in Lusaka. The two hospitals were comprehensively informed of the nature of the study through letters of permission. The initial process of instrument development involved the identification of the main domains of care in children with SB through a nine-year retrospective study, while confirmation of domains was done through a systematic review of literature. Eventually, parents and caregivers of children with SB and youths with SB were recruited to participate in the process of item generation. Subsequently, expert clinicians managing children with SB validated the items, and ultimately the measure called ZSBFM was constructed. In total, four studies were carried out in the whole process of instrument development.
The methodology section comprises the mechanisms used to identify study participants, followed by the procedures that were undertaken to collect data. Eventually, methods of data analysis used in the studies will be presented.
Identification of participants for the studies
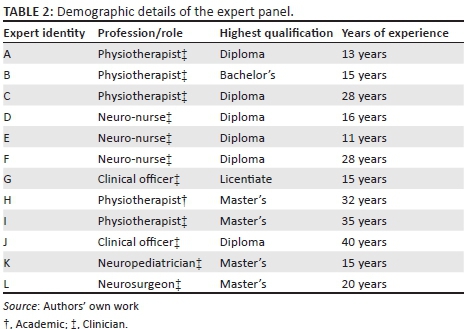
Table 1 presents samples for all the four studies involved in the initial development of the ZSBFM. Study 1 conveniently identified children with SB and hydrocephalus from whom domains of care were identified. Study 2 captured external data of the appraised studies in the systematic review process. In Study 3, purposive samples were used including participants with experience of caring for children with SB and other participants who were youths with SB. Eventually, clinicians were purposively identified for Study 4 from the UTH and BCH for the content validation exercise, and subsequently three content specialists, being two physiotherapists and one nurse, were also conveniently identified for the item-objective congruence exercise. Table 2 shows the demographic details of the expert panel.
Procedure of data collection
The procedures involved in the process of data collection and final instrument construction will be presented in four sections:
-
Domain identification
-
Domain confirmation
-
Instrument preparation
-
Item generation, content validation and item-objective congruence evaluation
Domain identification
The process of identifying the domains of care started by orientating three research assistants who are physiotherapists by profession. They were oriented on how to extract relevant information from the clinical files using a data-capturing sheet and eventually entering data into the SPSS database. Upon receiving ethical approval, permission from the hospital administrators of the two hospitals was sought. A checklist was then adapted from the assessment form routinely used for children with SB at the BCH. The viability of the checklist was tested by piloting and subsequently validated by three physiotherapists, three neuro-nurses, one orthopaedic surgeon and two neurosurgeons. Upon validating the checklist, domains were identified from the clinical files of children with SB and hydrocephalus identified from 2001 to 2010 (Mweshi et al. 2011).
Domain confirmation
To confirm the domains of care that were identified, a systematic review study was performed. The clinical question was:
What is the evidence that the functional domains of self-care, mobility, social function, participation and communication can be used to measure function in children with SB following an intervention in Zambia?
A critical appraisal of functional outcomes studies and commonly used functional outcome measures with their psychometric properties in measuring the impact of interventions was performed. This whole process was based on external data from four studies giving a sample size of 1135 participants (Table 1: Study 2).
Instrument preparation
Preparation for instrument development is essential before items are generated. Therefore, it becomes necessary to identify methods of administration, number of items testing each objective or subscale, item formats and test scoring in the preparation of instrument specifications.
Method of administration
The instrument is expected to be administered by clinicians with the help of primary caregivers, based upon their direct observations of the child's behaviour in performing functional activities. To facilitate a multidisciplinary approach which is needed for SB management, the ZSBFM has been principally designed for use by physiotherapists, occupational therapists, neuro-nurses, neurosurgeons, orthopaedic surgeons and clinical officers in Zambia. It is expected to provide an examiner's guide and a summary scoring form, with graph paper.
Number of items testing each objective
The establishment of the number of items began by a process of blueprint development. This was initiated by formulating a set of objectives reflecting the outcomes and critical areas to be assessed. Below is a list of objectives that were set:
-
to determine the levels of performance of self-care, mobility and social function in children with SB in their activities of daily living,
-
to ascertain the ability of children with SB to communicate the functional needs in performing activities of daily living,
-
to ascertain the ability of children with SB to participate in performing functional activities.
The next strategy was concerned with the total number of items that would make up the ZSBFM. Based on the numbers of items in commonly used measures such as the WeeFIM with 18 items, BDI with 61, GMFM with 88 and the PEDI with 241 items, the researchers made a resolve to develop a measure that would neither be too short nor too long.
The major content areas to be assessed included self-care, mobility and social function that appeared as column headings across the top of the table and critical areas assessed being communication and participation that appeared on the left side as row headings. At each intersection was a particular content-objective pairing and values in each cell reflecting the actual numbers of each item that were to be included in the proposed draft measuring instrument. The range of the number of items picked by the researchers was between 70 and 80. It was suggested that the total number of items for the three main domains would be between 50 and 60 items, while items on the sub-domains would be between 10 and 15 items each.
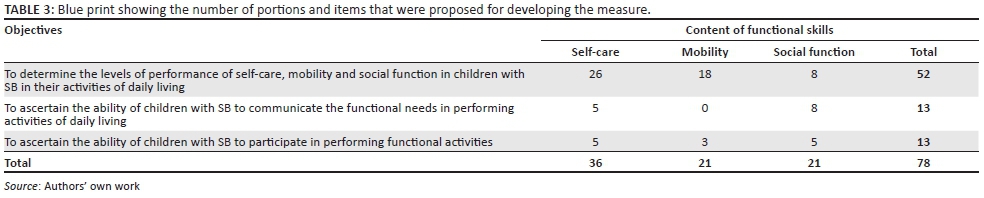
A total of 52 items were suggested to reflect the three main domains of which 26 items were earmarked for self-care, 18 items for mobility and 8 items for social function. With regard to communication, a total of 13 items were proposed, of which 5 items represented communication in self-care and 8 items communication in social function, while none was suggested for the domain of mobility. Participation was equally given a proportion of 13 items of which 5 items reflected participation in self-care, 3 items represented participation in mobility and 5 items were earmarked for participation in social function. Table 3 shows the blueprint that was ultimately constructed in the preparation of the test specifications showing the number of proportions and items that were subsequently generated.
Identification of the scoring rules and procedures
There are basically four classic scales or levels of measurement presented in literature being nominal, ordinal, interval and ratio scales. Well-renowned measures such as the GMFM 88 have utilised the scale in the use of the four-point ordinal scale (Avery et al. 2003; Russell et al. 1989). Given the potential advantages of using such a scale, the current study adopted a four-point Likert scale (1-4). The researchers adopted a model that awards scores for performing a functional task from 4 to 1, with each statement giving equal weighting as it has been suggested that differential weighting brings about potential problems of calculation (Avery et al. 2003; Bjornson et al. 1998; Russell et al. 1989). The final score is expected to be obtained by summing individual items. Nonetheless, the expected final scores for the age ranges of 6 months to less than 2 years, 2 years to less than 3 years and 3 years to less than 5 years are different because some of the functional skills are age dependent. The results of a total score of a domain can be interpreted that a child has 100% probability of having a score of 4 on every item of a domain.
General instructions for awarding scores for the performance of the task
The items of functional skills of children aged 6 months to 5 years are arranged into three sections. Section one has items on self-care, followed by the section on mobility and lastly social function. Instructions state: Please indicate by ticking (√) the statement that best describes the child's ability to perform each of the following activities taking into consideration the appropriate age category. Please note that blocked spaces in the age categories of 6 months to 2 years and 2 years to 3 years show that the child is young for the activity in question. However, the scores to be awarded are from a range of 4 to 1, with the following interpretations:
Score 4, independent of caregiver, can perform the activity with or without mechanical aids
Score 3, independent of caregiver, but needs monitoring or aid in performance of activity
Score 2, requires assistance by caregiver or mechanical aid in performance of activity
Score 1, completely dependent, needs help with activity.
Item generation process, content validity and item-objective congruence evaluation
Upon identifying and confirming the domains of care and formulating the specific instrument preparation guide, the researchers immediately went into specific item generation. This process was followed by the process of preliminary item validation and, subsequently, the congruence of the items was evaluated.
Process of item generation
The process of item generation involved the qualitative enquiry of semi-structured interviews and focus group discussions (FGDs). A summary of questions asked in the interviews and focus groups is presented in Appendix 1. For the purpose of congruent items, themes and question guides from both interviews and FGDs were generated from the blueprint and are shown in Table 3. As soon as everything was put in place, a pilot study was performed to ensure that items would be extracted from the two methods of enquiry. Semi-structured interviews were conducted before the FGDs in order to identify relatively personal views before validating the general consensus views.
-
Semi-structured interviews
■ A total of 20 semi-structured interviews were conducted in the study. Appointments with the research participants were made during the clinics at both hospitals. All the interviews were carried out at Cheshire Homes Rehabilitation Centre for children with disabilities. Before interviews started, informed consent was obtained from all participants and permission to record interviews was sought. Participants were asked what language they were comfortable with, and the main researcher identified a research assistant in instances where she was not so comfortable with the preferred language of the participant. Confidentiality was ensured and the participants were made comfortable by creating an atmosphere that facilitated freedom of expression.
■ The first five interviews were conducted with youths and the next five with parents, or caregivers, followed by five youths and then the last five parents, or caregivers, giving a total of 20 interviews. Codes were given to the participants in order to facilitate easy analysis. Codes A1-A10 were given to youths who took part in the semi-structured interviews while B1-B10 to mothers or caregivers. For the purpose of quality listening, a maximum of three interviews were conducted in a day. This was meant to create ample time for the researcher to download the recorded interviews and transcribe them with ease. On average, interviews took between 45 minutes and 1 hour 30 minutes.
-
Focus group discussions
■ Upon getting consent from parents, or caregivers, and assent from the youths with SB, dates and times for the two FGDs were set. The first FGD comprised youths with SB (n = 10) while the second was with parents or caregivers (n = 10) of children with SB. Codes C1-C10 were given to youths, while D1-D10 to mothers or caregivers in order to facilitate easy management of data. The two FGDs took place at Cheshire Homes for Children with Disabilities in Kabulonga, and confidentiality was ensured before commencing the FGDs.
Content validation and item-objective congruence evaluation
When investigating content validity, the interest is in the extent to which the measure represents the content domain (Waltz, Strickland & Lenz 2010). At least two or three experts in the area of the content to be measured can evaluate the validity of the items. When only two or three judges are employed, content validity index (CVI) is used to measure the level of agreement between the experts. When more than two or three experts rate the items on a measure, the alpha coefficient is employed as the index of content validity. Therefore, in order to be more inclusive, a resolve was made to involve 12 different clinicians who are involved in the management of children with SB and 3 for the item-objective congruence evaluation.
In order to validate the items generated from the interviews and FGDs, appointments with 12 expert clinicians were arranged in person to explain the purpose of the evaluation. Letters explaining the aim, the purpose of the questionnaire and procedure of administration were given to each research participant. Subsequently, the experts were given the objectives of the measure and a list of generated items. They were asked to independently rate the relevance of each item using a 4-point rating scale: 1 not relevant, 2 somewhat relevant, 3 quite relevant and 4 very relevant.
Methods of data analysis
Qualitative analysis
Of paramount importance to data quality is the accuracy of the transcribed interviews and FGD notes (Waltz et al. 2010). Given the purpose of the study and the type of data collected, the choice of type of analysis was manifest content analysis. Therefore, the analysis of both semi-structured interviews and FGDs involved downloading of recorded data, translation into English and transcribed verbatim data were then placed into categories of the main domains of care deductively. The results of both the interview and focus group methodologies were categorised under similar themes and finally the back and forth potential verification with some of the original information helped to strengthen the analysis.
Quantitative analysis
Descriptive statistics were used to analyse quantitative data by using SPSS version 17. The level of statistical significance was set at p ≤ 0.05 at 95% confidence interval. Internal consistency was measured by Cronbach's alpha. Validity was measured by using both Item Content Validity Indices (I-CVIs) and Scale Content Validity Indices (S-CVIs) (Waltz et al. 2010).
Instrument construction process
The process of instrument construction involved compiling all the necessary components essential for the instrument measure. It involved designing the cover page presenting the title of the tool and the age limit for using the tool and the name of the instrument developer. Also found on the cover page is a provision for brief information about the interviewer, respondent and about the child concerning information on SB and services such as surgery, orthotics and physiotherapy and general instructions on the use. General instructions on awarding scores for the testing different functional skills to facilitate uniformity in assessing the levels of function in the children were also put in place. The items of functional skills of a child aged 6 months to 5 years are arranged into three sections with items on self-care, followed by the section on mobility and lastly social function. Instructions state: Please indicate by ticking (√) the statement that best describes the child's ability to perform each of the following activities taking into consideration the appropriate age category. Please note that blocked spaces in the age categories of 6 months to 2 years and 2 years to 3 years show that the child is young for the activity in question. Lastly, the summary scoring form that provides the clinician with raw scores for each sub-section and also a graph for plotting in order to monitor if there is progress or no progress in the management programme was also compiled.
Results
The results section presents the domains identified and confirmed, items generated from qualitative data, results of the content validation exercise and the item-objective congruence exercise. Subsequently, the process of instrument construction will be presented.
Domain identification and confirmation
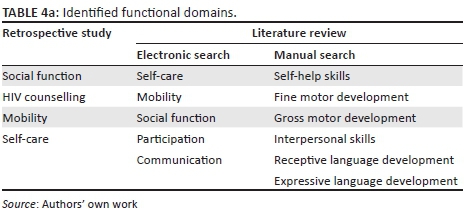
Domains of care were identified from an audit of 1400 children with SB and hydrocephalus over a period of 9 years. Categorically, social function (46%) was the highest domain of care provided, followed by HIV counselling to parents (32%), mobility (16%) and self-care (6%) (Mweshi et al. 2011) The results of the study show levels of how the domains of self-care, mobility and social function were being managed. The facility of HIV counselling to parents was used significantly and hence becomes an important aspect in the whole rehabilitation process of children with SB.
Subsequently, the results of the literature search confirmed the already known three functional domains of self-care, mobility and social function and the two new contributions, being the domains of participation and communication that were identified and included. There is evidence that functional tools have potential to evaluate the impact of clinical interventions (Adolfsson et al. 2010; Bier et al. 2005; Ettling et al. 2006; Ketelaar et al. 2001). Further, functional independence in children can be measured in three areas of self-care, mobility and social cognition using the WeeFIM, PEDI and other measures. It is highly recommended that the ICF-CY-based assessment tool measuring interventions focus on communication and child participation (Adolfsson et al. 2010; Björck-Åkesson et al. 2010; Klang 2012; Morris 2009). Table 4a and Table 4b show the domains that were identified and subsequently confirmed.

Item generated from qualitative data
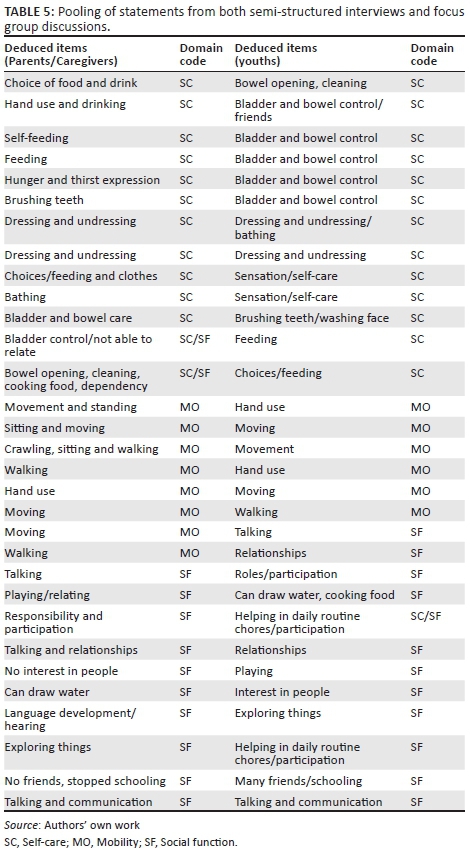
Statements generated from interviews of parents and youths were initially pooled and so were those from the focus groups of parents and youths. Eventually, the pooled data from the two different methods were combined to come up with one pool of results leading to a process known as triangulation. Methodological triangulation is the use of two or more different kinds of methods in a single line of inquiry (Risjord 2001). Combinations at the method level can be used to expand the scope of a study as researchers seek to capture method-linked dimensions of a target phenomenon (Greene, Caracelli & Graham 1989). The two methods served as invaluable tools for gathering data, and the benefits were seen from the depths of responses during interviews compared to responses from the focus group. For instance, A9, a male student, had this to share:
'I have no interest in friends because of my smell … they run away.'
Another female student, A5 shared:
'I feel the urge to pass urine, but by the time I reach the toilet, my pants are wet. This makes me always to stay at home.'
The depth of such responses involved pure honesty and such would be quite difficult to share freely for most people. Pooling of items for some researchers is performed during literature search and they just get confirmed during FGDs (Nassar-Mcmillan et al. 2010). The current study opted to pool statements after the interviews and FGD. The statements that were pooled were a homogeneous collection of functional items around the three main domains of self-care, mobility and social function.
The process of selecting items from pools of statements has been practised by several researchers (Babcock-Parziale & Williams 2006; Slaghuis et al. 2011). Selecting items for the current study began first by converting the statements into clear items. For instance, a parent coded B3 during semi-structured interviews shared this:
'My child cannot feed himself although he is 4 years.'
The deduced item was self-feeding and the functional domain identified was self-care domain. An initial pool of 150 statements enabled the key concepts to be identified and after checking for redundancy, colloquialisms and ambiguity, the number of statements was reduced to 100 statements. Table 5 presents a pooling of statements from both semi-structured interviews and FGDs. These statements were further categorised and thus reduced to 90 items and later categorised into the three main domains of function, being self-care, mobility and social function. Following the conceptual plan of the blueprint, a selection of 78 items was made. Subsequently, 36 items were grouped under self-care, mobility 21 items while social function also had 21 items, shown in Table 6. The items that were generated were subsequently subjected to content validity evaluation.
Content validation
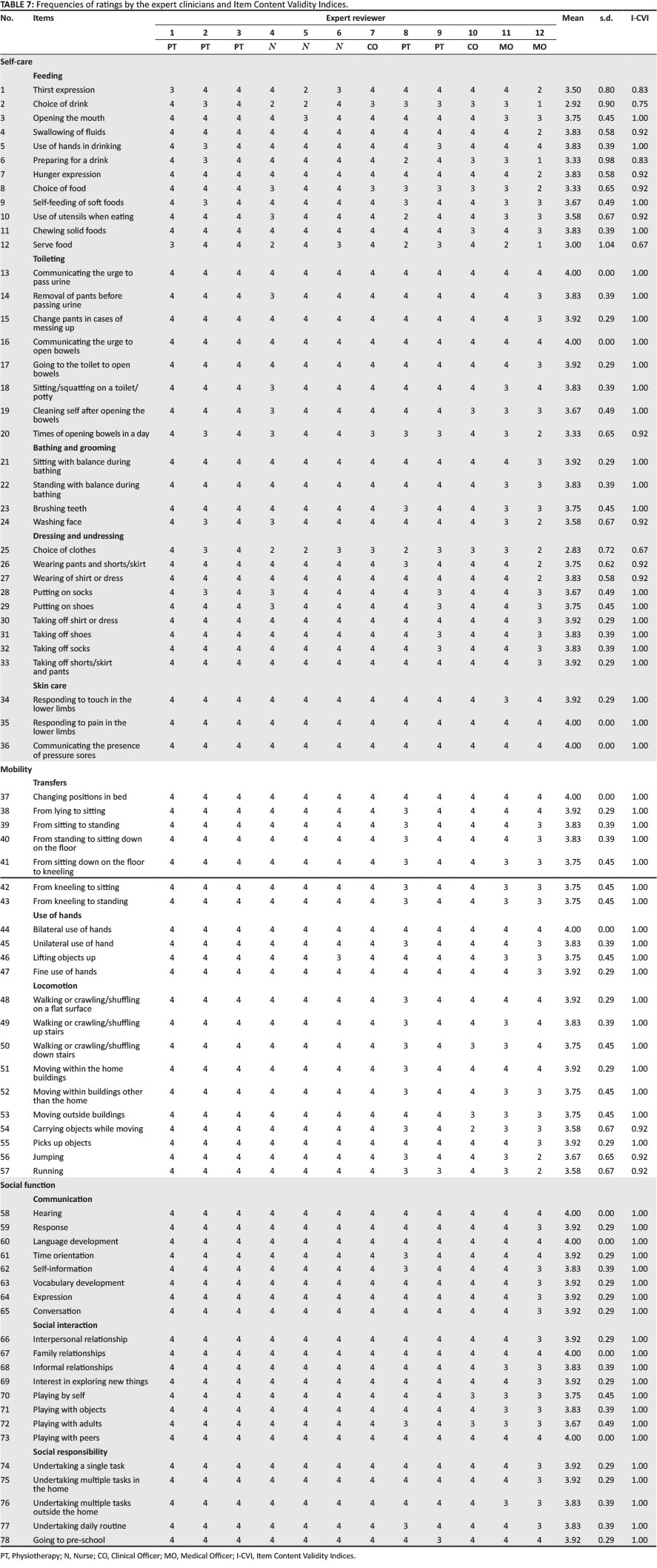
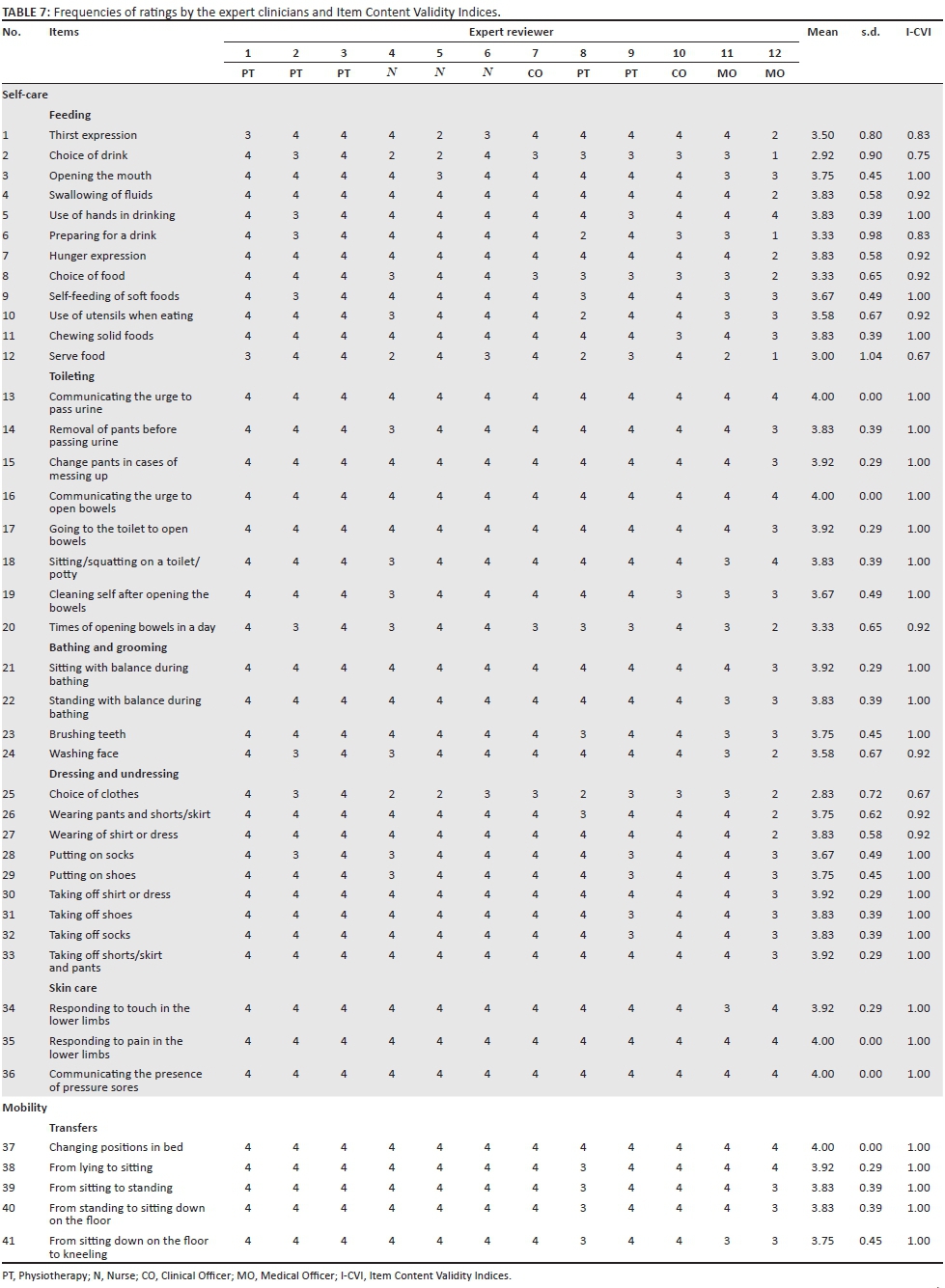
The frequencies of the ratings for the content validity results by the 12 expert specialists are evident in Table 7. Only two items had average ratings less than 3 (somewhat relevant), viz. item 2 'Choice of drink' ( = 2.92; s.d. = 0.90) and item 25 'Choice of clothes' (
= 2.92; s.d. = 0.90) and item 25 'Choice of clothes' ( = 2.83; s.d. = 0.72). All other items had average ratings from the 12 expert specialists of 3 (quite relevant) and above, while 10 items received average ratings of 4 (very relevant) indicating that all 12 expert specialists rated these items as very relevant. The average expert specialist rating for all 78 items was 3.78. Table 7 shows the frequencies of ratings by the 12 expert specialists for each item that was employed for the determination of content validity of the measure.
= 2.83; s.d. = 0.72). All other items had average ratings from the 12 expert specialists of 3 (quite relevant) and above, while 10 items received average ratings of 4 (very relevant) indicating that all 12 expert specialists rated these items as very relevant. The average expert specialist rating for all 78 items was 3.78. Table 7 shows the frequencies of ratings by the 12 expert specialists for each item that was employed for the determination of content validity of the measure.
I-CVIs were calculated for each item by counting the number of experts who rated the items as either somewhat relevant (3) or very relevant (4) and then dividing that total by the number of expert specialists (Polit & Beck 2006). As mentioned above, items 2 (Choice of drink) and 25 (Choice of clothes) had the lowest average ratings and thus the lowest I-CVI scores (0.75 and 0.67 respectively). In addition, item 12 (Serve food) also had an I-CVI of 0.67. Two items, item 1 (Thirst expression) and item 6 (Preparing for a drink) had I-CVIs of 0.83, while 11 items had I-CVIs of 0.92. The remainder of the items (62 items) had I-CVIs of 1.00 indicating that all 12 expert specialists considered these items as either somewhat relevant or very relevant. Polit and Beck (2006) argue that S-CVIs can be calculated by dividing the number of items that all experts considered either somewhat or very relevant by the total number of items. In this instance our 62 items divided by the total items (78) result in an S-CVI of 0.80, which is the standard criterion for acceptability (Polit & Beck 2006).
When the 78 items were exposed to reliability analysis, the alpha coefficient of 0.98 was computed. When the items were further analysed in categories of the three main domains, the results showed that the alpha coefficient for self-care was 0.97, mobility was 0.95 and social function had an alpha of 0.95. Therefore, results for both the CVI and alpha coefficient were above 0.80, indicating an acceptable level of content validity (Waltz et al. 2010).
Based on such results, decisions had to be made on the following three items:
-
choice of drink (self-care)
-
choice of clothes (self-care)
-
serve food (self-care).
It was recommended that item 12 (Serve food) under self-care domain be removed thus reducing the number of items to 77. However, items 2 (Choice of drink) and 25 (Choice of clothes) were recommended for reliability evaluation.
Instrument construction: Zambia Spina Bifida Functional Measure
The measure with 77 items was finally assembled including the preparation of the cover page with important information, directions, scoring keys and answer sheets. Subsequent to compiling all important documents, the first draft of the tool, titled 'Zambia Spina Bifida Functional Measure' (ZSBFM), designed for evaluating the performance of functional skills in children with SB in Zambia, was developed.
The ZSBFM is aimed at measuring the impact of interventions like surgery and physiotherapy given to children with SB from the age of 6 months to 5 years. The ZSBFM draft had two sections: Section A: demographic data, while Section B: 77 items categorised in three domains of self-care, mobility and social function. From the 77 items, 37 (48%) were under the self-care domain, 19 (25%) mobility domain and 21 (27%) under the social function domain.
Discussion
Faced with the clinical problem of lack of evidence on the impact of interventions given to children with SB, the researchers set out to develop a tool expected to fill the gap that existed. The intent was to locally generate a measure with psychometric adequacy that could readily be available, affordable, appropriate and culturally sensitive in assessing the performance of functional skills in children with SB in Zambia. A retrospective study was conducted to identify domains and through a systematic review, the domains were confirmed. Subsequently, items were generated, content validation was performed, and subsequently the first draft was constructed.
Domains of care identified from the retrospective study showed that social function was the highest care provided, followed by HIV counselling to parents, mobility and self-care. Mobility performed fairly in the management of children with SB in Zambia. Although mobility performed fairly, such impairments are very common among individuals with SB (Haley et al. 2010; Jahnsen et al. 2002) and many lead sedentary lives compared to those without disabilities (Willemsen & Fons 1997). The problem of mobility can be quite overwhelming in Zambia where accessibility for Persons with Disabilities is quite a big challenge. Despite mobility limitations in some individuals with SB, a lot is expected from them by society for them to be accepted and appreciated. This can be confirmed by a study that was conducted in Zambia which revealed that boys are involved in gardening, fetching firewood, running errands and washing plates. The chores for girls include washing plates, fetching water and firewood, bathing babies, running errands, pounding food and cooking (Chibuye et al. 1986). Such demands must be taken into consideration when carrying out interventions for individuals with SB. Perhaps this should motivate clinicians to look for ways and means of rehabilitating individuals with mobility problems in order to prepare them participate in chores expected of them regardless of their physical status.
Even though self-care was rated poorly in terms of care given to children with SB in the current study, literature reveals that only about half of children with SB are able to live independently and almost a quarter of them experience both urinary and faecal incontinence in their lives (Adeleye et al. 2010; Blenchowe et al. 2010). In spite of the global problems of self-care with problems of the bladder and bowel, Zambian children may have different demands considering the cultural variations and implications. For instance, Zambian children are expected to begin eating on their own at a young age (Evans & Myer 1994) considering that most mothers just abruptly stop breastfeeding which could affect a growing child negatively if not observed carefully.
Participation and communication were identified through a systematic review as new sub-domains recommended by the ICF-CY (Klang 2012). It must be noted that the two sub-domains were not measured in earlier developed measures such as the PEDI and WeeFIM, but these have been identified as important domains. These domains may include for example, mobility, self-care, participation, communication, social relationships, leisure or play, education, domestic chores and community integration (Morris 2009). One of the critical issues rehabilitation professionals need to address is how physiotherapeutic exercises or other clinical interventions given to a child with disabilities can be measured using functional outcomes tools. The results of the clinical trial study of Ketelaar et al. (2001) show that the task-specific approach is more effective than the one that takes into account the motor function in a developmental manner. Additionally, the task-oriented approach has proven to be a systematic way of trying to solve a child's functional problems. The current knowledge that has been gained in the use of the ICF-CY has come with other measurement challenges such as the inclusion of participation and communication in new measures as presented by Adolfsson and colleagues and Morris and colleague (Adolfsson 2011; Morris 2009). The new challenge is calling on rehabilitation professionals such as physiotherapists to plan the task-oriented functional approaches in such a way that they become inclusive of participatory tasks which are also age-oriented by nature.
The process of item generation involved the use of two methods, being semi-structured interviews and FGDs. Several simultaneous steps have been reported in the process of item generation, which eventually led to a pool of items based on a thorough literature review, existing scales, expert opinion (Delamere, Wankel & Hinch 2001) and eventually leading to FGDs (Nassar-Mcmillan et al. 2010). The researchers of the current study utilised the reported several steps except that instead of involving expert opinion in the beginning, a retrospective study was performed to evaluate and identify important functional domains and eventually semi-structured interviews and FGDs were conducted. Some studies (Delamere et al. 2001; Saldana 2009) have used focus groups to confirm the items and also identify domains, whereas the current study used already confirmed domains from a systematic review study and eventually used them to generate items using semi-structured interviews and FGDs. Selecting appropriate data-recording strategies that would help organise data is recommended (Saldana 2009). Of paramount importance to data quality is the accuracy of the transcribed interviews and FGD notes (Waltz et al. 2010). Given the purpose of the study and the type of data collected, the choice of type of analysis was content analysis. Because the researchers wanted to capture the experiences and views of parents or caregivers of children with SB and youths with SB concerning functional skills, they opted to transcribe and present data in verbatim form. Data were then placed into categories of the main domains of care deductively. The results of the two methodologies were categorised under similar themes and finally the back and forth potential verification with some of the original information helped to strengthen the analysis.
The concept of validity refers to the degree to which an instrument measures what it is supposed to measure (Dekker, Dallmeyer & Lankhorst 2005). The procedures for validity evaluation of the current study focused on content. Criterion validity was not included in the plan because a gold standard is frequently not available in rehabilitation, which precludes evaluation of criterion validity (i.e. the degree to which the scores on an instrument correspond to the scores on the gold standard). The process of content-relevant evidence in the current study included the initial restricting of item selection to the test blueprint and obtaining content validity ratings from subject matter experts. Content validity is often viewed as the minimum psychometric requirement for measurement adequacy and is the first step in construct validation of a new measure. It must be built into the measure through the development of items (Waltz et al. 2010). A sample of 12 clinicians was identified comprising 5 physiotherapists, 3 neuro-nurses, 2 clinical officers, 1 neuro-pediatrician and 1 neurosurgeon. The professionals' average years of experience in child health services was 22 years (s.d. = 8.82) and had academic qualifications in their respective fields (MSc, BSc and Diploma). It is suggested that a minimum of five experts in the field are recommended to judge the content domains of an instrument (Dempsey & Dempsey 1986). The sample size identified for the study was quite adequate, and there was a good and wide representation considering the team of clinicians who manage children with SB in Zambia. The level of agreement between the 12 experts was determined via coefficient alpha in order to measure the content validity. Item as well as S-CVIs were calculated and were indicative of a validity of the measure by separately evaluating each item (Waltz et al. 2010). Additionally, the alpha coefficient computed for the scale items that were generated was between 0.95 and 0.98, showing an acceptable level of content validity (Martuza 1977). Given the good internal consistency as well as the good I-CVIs and S-CVI, we argue that the ZSBFM for children with SB in Zambia is contextually relevant and valid for use in this context.
Conclusion
A draft measure titled ZSBFM for children with SB in Zambia has been developed. It is meant to help clinicians managing children with SB measure the impact of interventions such as surgery and physiotherapy given to children aged 6 months to 5 years. The measure can provide an opportunity to assess children with SB in performing distinct functional skills based on 77 items categorised into the three main domains of self-care, mobility and social function. The draft ZSBFM has an acceptable level of content validity. Psychometric properties of reliability and validity were measured through Cronbach's alpha reliability and later I-CVIs and S-CVIs.
Acknowledgements
The authors wish to thank the University of Zambia for the financial and material support towards this study. Gratitude also goes to the management and staff of BCH and UTH for allowing the study to be carried out at the hospitals and the research assistants Mr Ephron Soko, Mr Lieto and Mr Edwin Zulu. Special thanks also go to Dr Akakandelwa, University of Zambia, and Prof. Waltz, Prof. Vance of the USA and Dr Kafaar Zuhayr of Stellenbosch University in South Africa for helping in the statistical analyses. Finally, gratitude goes to my supervisors Prof. Seyi Ladele, Dele, Prof. Shalalukey Ngoma and Prof Munalula-Nkandu for guidance.
The study received partial funding from the University of Zambia as part of Staff Development.
Competing interests
The authors declare that they have no financial or personal relationships that may have inappropriately influenced them in writing this article.
Authors' contributions
M.M.M. conceptualised the study. S.L.M., M.P.S. and E.M.N. supervised the protocol development, data collection, data analysis and generation of the manuscript. Z.K. did the final statistical analysis of the data presented. All the authors participated in the internal review and finalisation of the article.
References
Adeleye, A.O., Magbagbeola, D.D. & Olowookere, K.G., 2010, 'Central nervous system congenital malformation in a developing country: Issues and challenges against their prevention', Child's Nervous System 26(7), 919-924. https://doi.org/10.1007/s00381-009-1079-0 [ Links ]
Adolfsson, M., 2011, 'Applying the ICF-CY to identify everyday life situations of children and youth with disabilities', Dissertation Series No. 14, Studies from Swedish Institute for Disability Research No. 39., Jonkoping, Sweden.
Adolfsson, M., Granlund, M., Björck-Åkesson, E., Ibragimova, N. & Pless, M., 2010, 'Exploring changes over time in habilitation professionals' perceptions and applications of the International Classification of Functioning, Disability and Health, version for Children and Youth (ICF-CY)', Journal of Rehabilitation Medicine 42(7), 670-678. [ Links ]
Adzick, M.D., Thom, E.A., Spong, C.Y., Brock, J.W., 3rd, Burrows, P.K., Johnson, M.P. et al., 2011, 'A randomized trial of prenatal versus postnatal repair of myelomeningocele', New England Journal of Medicine 364, 993-1004. https://doi.org/10.1056/NEJMoa1014379 [ Links ]
Avery, L.M., Russell, D., Raina, P.S., Walter, S.D. & Rosenbaum, P.L., 2003, 'Rasch analysis of the gross motor function measure: Validating the assumptions of the Rasch Model to create an interval-level measure', Archives of Physical Medicine and Rehabilitation 84(5), 607-705. https://doi.org/10.1016/S0003-9993(02)04896-7 [ Links ]
Babcock-Parziale, J.L. & Williams, M.D., 2006, 'Historical perspective on the development of outcomes measures for low-vision and blind rehabilitation in the Department of Veterans Affairs', Journal of Rehabilitation Research & Development 43(6), 793-808. https://doi.org/10.1682/JRRD.2005.07.0125 [ Links ]
Berg, M., Aamodt, G., Stanghelle, J., Krumlinde-Sungholm, L. & Hussain, A., 2008, 'Cross-cultural validation of the Pediatric Evaluation of Disability Inventory (PEDI) norms in a randomized Norwegian population', Scandinavian Journal of Occupational Therapy 15(3), 14352. https://doi.org/10.1080/11038120802022011 [ Links ]
Bier, J.A., Prince, A., Tremont, M. & Small, M., 2005, 'Medical functional and social determinants of health related quality of life in individuals with myelomeningocele', Developmental Medicine of Child Neurology 47(9), 609-612. https://doi.org/10.1111/j.1469-8749.2005.tb01212.x [ Links ]
Björck-Åkesson, E., Wilder, J., Grandlund, M., Pless, M., Simeonsson, R., Adolfsson, M. et al., 2010, 'The International Classification of Functioning, Disability and Health and the version for children and youth as a tool in child habilitation/early childhood interventions - Feasibility and usefulness as a common language and frame for practice', Disability and Rehabilitation 32(Suppl 1), S125-S138. https://doi.org/10.3109/09638288.2010.516787 [ Links ]
Bjornson, K.F., Graubert, C.S., Buford, V.L. & McLanhlin, J., 1998, 'Validity of the gross motor function measure', Pediatric Physical Therapy 10, 43-47. https://doi.org/10.1097/00001577-199801020-00002 [ Links ]
Blenchowe, H., Cousens, S., Modell, B. & Lawn, J., 2010, 'Folic acid to reduce neonatal mortality from neural tube disorders', International Journal of Epidemiology 39(Suppl 1), 110-121. https://doi.org/10.1093/ije/dyq028 [ Links ]
Chibuye, P.S., Mwenda, M. & Osborne, C., 1986, CRZ/UNICEF Study on Childrearing practices in Zambia, Zambia Association for Research and Development, Lusaka, Zambia.
Dekker, J., Dallmeyer, A.J. & Lankhorst, G.J., 2005, 'Clinimetrics in rehabilitation medicine: Current issues in developing and applying measurement instruments', Journal of Rehabilitation Medicine 37, 193-201. https://doi.org/10.1080/16501970510035179 [ Links ]
Delamere, T.A., Wankel, L.M. & Hinch, T.D., 2001, 'Development of a scale to measure resident attitudes towards the social impact of community festivals, Part 1: Item generation and purification of the measure', Event Management 7, 11-24. https://doi.org/10.3727/152599501108751443 [ Links ]
Dempsey, P.A. & Dempsey, A.D., 1986, The research process in nursing, 2nd edn., Jones and Bartlett Publishers, Boston, MA.
Ettling, J.T., Phiri, H.J., Msango, B., Matafwali, J., Mandyata, E., Mundaala-Simfukwe, M.O. et al., 2006, Child development assessment in Zambia, 1st edn., UNICEF, Lusaka, Zambia.
Evans, J.L., Myers, R.G, 1994, Childrearing practices in sub-Saharan Africa: An introduction to the studies, Coordinators' Notebook No. 15, The Consultative Group on ECCD, Washington, DC.
Fabiano, A.J., Doyle, K. & Grand, W., 2010, 'Delayed stoma failure in adult communicating hydrocephalus after initial successful treatment of endoscopic third ventriculostomy: Case report', Neurosurgery 66, 1201-1211. https://doi.org/10.1227/01.NEU.0000369191.27291.2F [ Links ]
Greene, J.C., Caracelli, V.J. & Graham, W.F., 1989, 'Toward a conceptual framework for mixed-method evaluation designs', Educational Evaluation and Policy Analysis 11(3), 255-274. https://doi.org/10.3102/01623737011003255 [ Links ]
Haley, S.M., Coster, W.I., Kao, Y.C., Dumas, H.M., Fragala-Pinkham, M.A., Kramer, J.M. et al., 2010, 'Lessons from use of the pediatric evaluation of disability inventory: Where do we go from here?', Physical & Occupational Therapy of Pediatrics 22(1), 69-75. https://doi.org/10.1097/PEP.0b013e3181cbfbf6 [ Links ]
Harvey, A., Robin, J., Morris, M.E. & Graham, H.K., 2008, 'A systematic review of measures of activity limitation for children with cerebral palsy', Developmental Medicine & Child Neurology 50, 190-198. https://doi.org/10.1111/j.1469-8749.2008.02027.x [ Links ]
Jahnsen, R., Villien, L., Stanghelle, J.K. & Holm, I., 2002, 'Coping potential and disability sense of coherence in adults with cerebral palsy', Disability and Rehabilitation 24(10), 511-518. https://doi.org/10.1080/09638280110108805 [ Links ]
Kaplan, S.L., 2007, Outcome measurement management: First steps for the practicing clinician, FA Davies Company, Philadelphia, PA.
Ketelaar, M., Vermeer, A., Hart, H., Petegem-van, B.E. & Helders, P.J.M., 2001, 'Effects of a functional therapy program on motor abilities of children with cerebral palsy', Physical Therapy 81(9), 1534-1545. https://doi.org/10.1093/ptj/81.9.1534 [ Links ]
Klang, N., 2012, 'Applicability of the ICF-CY to describe functioning and environment of children with disabilities', Studies from the Swedish Institute for Disability Research 41, Orebro, Sweden.
Liptak, G. & El Samra, A., 2010, 'Optimizing health care for children with spina bifida', Developmental Disability Research Review 16, 66-75. https://doi.org/10.1002/ddrr.91 [ Links ]
Martuza, V.R., 1977, Applying norm-referenced and criterion referenced measurement in education, Allyn and Bacon, Boston, MA.
Mitchell, L.E., Adzick, N.S., Melchionne, J., Pasquariello, P.S., Sutton, L.N. & Whitehead, A.S., 2004, 'Spina bifida', Lancet 364, 1885-1895. https://doi.org/10.1016/S0140-6736(04)17445-X [ Links ]
Morris, C., 2009, 'Measuring participation in childhood disability: How does the capability approach improve our understanding?', Developmental Medicine & Child Neurology 51(2), 92-94. https://doi.org/10.1111/j.1469-8749.2008.03248.x [ Links ]
Mweshi, M.M., Amosun, S.L., Ngoma, M.S. & Nkandu, E.M., 2011, 'Managing children with spina bifida in sub-Saharan Africa: The Zambian experience?', Medical Journal of Zambia 38(1), 13-23. [ Links ]
Mweshi, M.M., Amosun, S.L., Ngoma, M.S., Nkandu, E.M., Sichizya, K., Chikoya, L. et al., 2010, 'Endoscopic third ventriculostomy and choroid plexus cauterization in childhood hydrocephalus in Zambia', Medical Journal of Zambia 37(4), 246-252. [ Links ]
Mweshi, M.M., Amosun, S.L., Shilalukey-Ngoma, M.P. & Munalula-Nkandu, E., 2015, 'Ethnic pattern of origin of children with spina bifida managed at the University Teaching Hospital and Beit Cure Hospital, Lusaka, Zambia 2001-2010', Science Journal of Public Health 3(6), 857-861. https://doi.org/10.11648/j.sjph.20150306.19 [ Links ]
Nassar-Mcmillan, S.C., Wyer, M., Oliver-Hoyo, M. & Ryder-Burge, A., 2010, 'Using focus groups in preliminary instrument development: Expected and unexpected lessons learned', The Qualitative Report 15, 1621-1634. [ Links ]
Oeffinger, D., Gorton, G., Bagley, A., Nicholson, D., Barnes, D., Calmes, J. et al., 2007, 'Outcome assessments in children with cerebral palsy, Part I: Descriptive characteristics of GMFCS Levels I to III', Developmental Medicine & Child Neurology 49, 172-180. https://doi.org/10.1111/j.1469-8749.2007.00172.x [ Links ]
Polit, D.F. & Beck, C.T., 2006, 'The content validity index: Are you sure you know what's being reported? Critique and recommendations', Research in Nursing & Health 29, 489-497. https://doi.org/10.1002/nur.20147 [ Links ]
Qureshi, A.M., 2010, 'Neural tube defects in the developing world: Achieving closure a hope for the use of folic acid fortification in the reduction of the high incidence spina bifida and associated hydrocephalus worldwide', Journal of Hydrocephalus 2, 2. [ Links ]
Risjord, M., 2001, 'Methodological triangulation in nursing research', Philosophy of the Social Sciences 31, 40-59. https://doi.org/10.1177/004839310103100103 [ Links ]
Russell, D.J., Rosenbaum, P.L., Cadman, D.T., Gowland, C., Hardy, S. & Jarvis, S., 1989, 'The gross motor function measure: A means to evaluate the effects of physical therapy', Developmental Medicine and Child Neurology 31, 341-352. https://doi.org/10.1111/j.1469-8749.1989.tb04003.x [ Links ]
Sacko, O., Boetto, S., Lauwers-Cances, V., Dupuy, M. & Roux, F., 2010, 'Endoscopic third ventriculostomy: Outcome analysis in 368 procedures', Journal of Neurosurgery in Pediatrics 5, 68-74. https://doi.org/10.3171/2009.8.PEDS08108 [ Links ]
Saldana, J., 2009, The coding manual for qualitative researchers, Sage, Thousand Oaks, CA.
Sirzai, H., Erkin, G., Culha, C. & Ozel, S., 2008, 'Measuring functional change in Turkish children with cerebral palsy using the paediatric evaluation of disability inventory (PEDI)', Turkish Journal of Medical Sciences 38(6), 555-560. [ Links ]
Slaghuis, S.S., Mathilde, M.H., Bal, R.N. & Anna, P., 2011, 'A framework and a measurement instrument for sustainability of work practices in long-term care', BMC Health Services Research 11, 314. https://doi.org/10.1186/1472-6963-11-314 [ Links ]
Sonel, T.B., Kucukde, V.A., Kutlay, S., Yavuzer, G. & Elhan, A.H., 2009, 'Psychometric properties of WeeFim in children with cerebral palsy in Turkey', Developmental Medicine & Child Neurology 51, 732-738. https://doi.org/10.1111/j.1469-8749.2008.03255.x [ Links ]
Sullivan, E., Barnes, D., Linton, J.L., Calmes, J., Damiano, D., Oeffinger, D. et al., 2007, 'Relationships among functional outcome measures used for assessing children with ambulatory CP', Developmental Medicine & Child Neurology 49, 338-344. https://doi.org/10.1111/j.1469-8749.2007.00338.x [ Links ]
Waltz, C.F., Strickland, O.L. & Lenz, E.R., 2010, Measurement in nursing and health research, 3rd edn., Springer, New York.
Willemsen, M.E. & Fons, J.R., 1997, 'Developmental expectations of Dutch, Turkish-Dutch, and Zambian mothers: Towards an explanation of cross-cultural differences', International Journal of Behavioral Development 21(4), 837-854. https://doi.org/10.1080/016502597384695 [ Links ]
 Correspondence:
Correspondence:
Margaret Mweshi
srmmweshi@gmail.com
Received: 03 Feb. 2016
Accepted: 15 Feb. 2017
Published: 24 July 2017



{kind=link}
{kind=link}
{kind=link}
{kind=link}